Or IGINAL PAPE r S - advances.umed.wroc.pl · CT is rap-idly broken down by serum proteases, which...
10
Krzysztof Kaczka 1 , Sławomir Mikosiński 2 , Wojciech Fendler 3 , Agnieszka Celnik 1 , Lech Pomorski 1 Calcitonin and Procalcitonin in Patients with Medullary Thyroid Cancer or Bacterial Infection* Kalcytonina i prokalcytonina u pacjentów z rakiem rdzeniastym tarczycy lub infekcją bakteryjną 1 Department of General and Oncological Surgery, Medical University of Łódź, Poland 2 Department of Nuclear Medicine and Oncological Endocrinology, Maria Skłodowska-Curie Memorial Hospital, Zgierz, Poland 3 Department of Pediatrics, Oncology, Hematology and Diabetology, Medical University of Łódź, Poland Abstract Objectives. To evaluate procalcitonin (PCT) utility as a marker of medullary thyroid cancer (MTC). Material and Methods. Calcitonin (CT) and PCT levels were measured in MTC patients and patients with seri- ous bacterial infections. 70 patients were enrolled in the study: 6 MTC active patients: 4 with disseminated, unre- operable disease and 2 re-operated patients, in whom markers were checked before and after surgery; 23 MTC patients in remission after radical surgery; 11 non-toxic nodular goiter (NTNG) patients; 30 patients with severe, bacterial infection or sepsis. Results. All MTC active patients had greatly elevated CT and PCT levels. In two re-operated patients, marker levels decreased but were still above the reference range. In 15 MTC patients in remission, the levels of either marker were not increased. Both markers were slightly increased in 3 patients in this group, while CT was elevated in 5 patients. In all but 1 patient in the NTNG group, both marker levels were not elevated. Among patients with bacterial infection, PCT and CT levels showed no increase in 8 patients, both markers were elevated in 10 patients, and an increase of PCT levels was seen in 10 patients while of CT only in 2 patients. Correlations between CT and PCT values were very strong in MTC patients (r = 0.95; p = 0.004 for active MTC, r = 0.60; p = 0.002 for MTC patients in remission) and in patients with NTNG (r = 0.77; p = 0.02). In patients with infection, both parameters were completely independent (r = 0.002; p = 0.99). Conclusions. PCT measurement could be an alternative to CT measurement for evaluation of MTC status (Adv Clin Exp Med 2012, 21, 2, 169–178). Key words: procalcitonin, calcitonin, medullary thyroid cancer. Streszczenie Cel pracy. Ocena przydatności prokalcytoniny jako markera raka rdzeniastego tarczycy. Materiał i metody. Stężenia kalcytoniny i prokalcytoniny zmierzono u pacjentów z rakiem rdzeniastym tarczycy lub ciężką infekcją bakteryjną. Do badania włączono 70 pacjentów: 6 pacjentów z aktywną postacią raka rdzeniaste- go tarczycy: 4 z rozsianą, nieresekcyjną postacią nowotworu; u 2 pozostałych chorych stężenia markerów zmierzo- no przed i po operacji; 23 pacjentów z rakiem rdzeniastym tarczycy w remisji po radykalnym zabiegu operacyjnym; 11 pacjentów z wolem guzowatym obojętnym; 30 pacjentów z ciężką infekcją bakteryjną lub posocznicą. Wyniki. Wszyscy pacjenci z aktywną postacią raka rdzeniastego tarczycy mieli znacznie zwiększone stężenia kal- cytoniny i prokalcytoniny. U dwóch reoperowanych chorych stężenia obu markerów zmniejszyły się, ale wciąż pozostawały powyżej normy. U 15 pacjentów w remisji raka rdzeniastego tarczycy nie odnotowano zwiększe- nia stężenia żadnego z markerów. Stężenia obu markerów były nieznacznie zwiększone u 3 chorych z tej grupy. U 5 pacjentów odnotowano jedynie nieznacznie zwiększone stężenie kalcytoniny. U wszystkich oprócz jednego Adv Clin Exp Med 2012, 21, 2, 169–178 ISSN 1899–5276 ORIGINAL PAPERS © Copyright by Wroclaw Medical University * This work was supported by the Dr. Magdalena Bartos Foundation. Wojciech Fendler received financial support from the project “Polish Registry for Pediatric and Adolescent Diabetes – nationwide genetic screening for monogenic diabetes” financed by the Innovative Economy Operational Program.
Transcript of Or IGINAL PAPE r S - advances.umed.wroc.pl · CT is rap-idly broken down by serum proteases, which...

Krzysztof Kaczka1, Sławomir Mikosiński2, Wojciech Fendler3, Agnieszka Celnik1, Lech Pomorski1
Calcitonin and Procalcitonin in Patients with Medullary Thyroid Cancer or Bacterial Infection*Kalcytonina i prokalcytonina u pacjentów z rakiem rdzeniastym tarczycy lub infekcją bakteryjną1 Department of General and Oncological Surgery, Medical University of Łódź, Poland 2 Department of Nuclear Medicine and Oncological Endocrinology, Maria Skłodowska-Curie Memorial Hospital, Zgierz, Poland 3 Department of Pediatrics, Oncology, Hematology and Diabetology, Medical University of Łódź, Poland
Abstract Objectives. To evaluate procalcitonin (PCT) utility as a marker of medullary thyroid cancer (MTC). Material and Methods. Calcitonin (CT) and PCT levels were measured in MTC patients and patients with seri-ous bacterial infections. 70 patients were enrolled in the study: 6 MTC active patients: 4 with disseminated, unre-operable disease and 2 re-operated patients, in whom markers were checked before and after surgery; 23 MTC patients in remission after radical surgery; 11 non-toxic nodular goiter (NTNG) patients; 30 patients with severe, bacterial infection or sepsis.Results. All MTC active patients had greatly elevated CT and PCT levels. In two re-operated patients, marker levels decreased but were still above the reference range. In 15 MTC patients in remission, the levels of either marker were not increased. Both markers were slightly increased in 3 patients in this group, while CT was elevated in 5 patients. In all but 1 patient in the NTNG group, both marker levels were not elevated. Among patients with bacterial infection, PCT and CT levels showed no increase in 8 patients, both markers were elevated in 10 patients, and an increase of PCT levels was seen in 10 patients while of CT only in 2 patients. Correlations between CT and PCT values were very strong in MTC patients (r = 0.95; p = 0.004 for active MTC, r = 0.60; p = 0.002 for MTC patients in remission) and in patients with NTNG (r = 0.77; p = 0.02). In patients with infection, both parameters were completely independent (r = 0.002; p = 0.99).Conclusions. PCT measurement could be an alternative to CT measurement for evaluation of MTC status (Adv Clin Exp Med 2012, 21, 2, 169–178).
Key words: procalcitonin, calcitonin, medullary thyroid cancer.
StreszczenieCel pracy. Ocena przydatności prokalcytoniny jako markera raka rdzeniastego tarczycy. Materiał i metody. Stężenia kalcytoniny i prokalcytoniny zmierzono u pacjentów z rakiem rdzeniastym tarczycy lub ciężką infekcją bakteryjną. Do badania włączono 70 pacjentów: 6 pacjentów z aktywną postacią raka rdzeniaste-go tarczycy: 4 z rozsianą, nieresekcyjną postacią nowotworu; u 2 pozostałych chorych stężenia markerów zmierzo-no przed i po operacji; 23 pacjentów z rakiem rdzeniastym tarczycy w remisji po radykalnym zabiegu operacyjnym; 11 pacjentów z wolem guzowatym obojętnym; 30 pacjentów z ciężką infekcją bakteryjną lub posocznicą.Wyniki. Wszyscy pacjenci z aktywną postacią raka rdzeniastego tarczycy mieli znacznie zwiększone stężenia kal-cytoniny i prokalcytoniny. U dwóch reoperowanych chorych stężenia obu markerów zmniejszyły się, ale wciąż pozostawały powyżej normy. U 15 pacjentów w remisji raka rdzeniastego tarczycy nie odnotowano zwiększe-nia stężenia żadnego z markerów. Stężenia obu markerów były nieznacznie zwiększone u 3 chorych z tej grupy. U 5 pacjentów odnotowano jedynie nieznacznie zwiększone stężenie kalcytoniny. U wszystkich oprócz jednego
Adv Clin Exp Med 2012, 21, 2, 169–178 ISSN 1899–5276
OrIGINAL PAPErS© Copyright by Wroclaw Medical University
* This work was supported by the Dr. Magdalena Bartos Foundation. Wojciech Fendler received financial support from the project “Polish registry for Pediatric and Adolescent Diabetes – nationwide genetic screening for monogenic diabetes” financed by the Innovative Economy Operational Program.

K. Kaczka et al.170
Calcitonin (CT) is a 32-amino acid peptide physiologically generated mainly from the thyroid C-cells [1]. It is formed by the proteolytic cleavage of a larger prepropeptide, which is the product of the CALC1 gene. The CALC1 gene belongs to a su-perfamily of related protein hormone precursors including islet amyloid precursor protein, calcito-nin gene-related peptide, and the precursor of ad-renomedullin. Calcitonin has a mild and transient hypocalcemic effect, and it was originally thought to play an important role in skeletal homeostasis. This effect is mediated by the interaction of cal-citonin with a specific receptor on the osteoclast. In almost all of the in vitro and in vivo studies conducted during the past 40 years, researchers concluded that CT is a basic inhibitor of bone re-sorption and its activity is modulated by several activators of osteoclastic function including para-thyroid hormone (PTH). Calcitonin is considered to be a sensitive and specific marker for medullary thyroid cancer (MTC). MTC is a relatively rare dis-ease, accounting for 3–5% of thyroid cancers, but MTC mortality is higher than that of differentiated thyroid cancer. Baseline or stimulated CT levels of more than 100 ng/ml are observed in almost all cases of MTC [2]. As a general rule, patients who reach undetectable serum CT levels soon after sur-gery are those with the best prognosis [3]. routine calcitonin measurement has therefore been rec-ommended in the diagnostic evaluation of patients with nodular thyroid disease by some authors to exclude MTC [4, 5]. CT as a laboratory marker has some limitations. Modest increases in serum CT concentrations might be revealed in other diseases such as: C cell hyperplasia, other neuroendocrine tumors, certain leukemias, systemic mastocytosis, small cell carcinoma of the lung, breast or pan-creatic cancer, renal failure, hyperparathyroidism, autoimmune thyroiditis, pregnancy, lactation, and during the neonatal period [5–8]. CT has a con-centration-dependent and biphasic half-life of 15 and 40 min at physiological concentrations; and 3 and 30 h at increased concentrations. CT is rap-idly broken down by serum proteases, which may lead to error – false low or false negative results, if samples are not processed expeditiously after
a blood draw. Patients who reach undetectable se-rum CT levels soon after surgery are those with the best prognosis, however normalization of serum CT after surgery is not an index of definitive cure in MTC [3]. The pattern of serum heterogeneity of patients with medullary thyroid cancer is char-acterized by the presence of at least seven different fractions of immunoreactive calcitonin. Further-more, dual site antibody-based immunoassays are commonly used in clinical laboratories to quan-tify the CT serum concentrations, as a specific and sensitive marker of MTC. Heterophilic antibodies can interfere with these assays and cause errone-ous results [9]. A high-dose hook effect may give falsely low results for several tumor markers, such as PSA, CA 19-9, CA 125 and others (10). This ef-fect has also been described in CT measurements, and it could lead to falsely low results [11, 12]. On the contrary, high levels of some substances: vita-min C, urea and creatine could cause falsely high levels of CT measured by rIA [13].
Procalcitonin (PCT), a 116-amino acid peptide, is also produced by C-cells in the thyroid and its con-centration in the serum of healthy individuals is very low (< 0.1 ng/mL) [14]). It is a product of the CALC-I gene [15]. Physiologically, the extrathyroid transcrip-tion of the CALC-I gene is blocked. Microbial infec-tions increase CALC-I gene expression, thus leading to a release of PCT. During microbial infection, there is an increase of CALC-I gene expression which causes a release of PCT from all parenchymal tissues and differentiated cell types throughout the body, in-cluding the liver and peripheral blood mononuclear cells [16]. The inflammatory release of PCT can be induced in two main ways: by toxins released by mi-crobes (endotoxin); or through proinflammatory cy-tokines released in a cell-mediated host response (e.g. interleukins 1b and 6, tumor necrosis factor-alpha) [16]. Nowadays, PCT is known as a biomarker of bacterial or fungal infection and sepsis.
In contrast to CT, PCT has a concentration-independent half-life and excellent in vitro stabil-ity in serum or plasma [17]. renal secretion is not a major pathway of PCT elimination, therefore renal failure does not affect the PCT levels signifi-cantly.
pacjenta z wolem guzowatym obojętnym stężenia obu markerów nie były zwiększone. Wśród pacjentów z infekcją bakteryjną nie zaobserwowano wzrostu stężenia prokalcytoniny i kalcytoniny u 8 pacjentów. Stężenia obu marke-rów były zwiększone u 10 chorych. Wzrost stężenia jedynie prokalcytoniny odnotowano u 10 chorych, podczas gdy wzrost stężenia kalcytoniny tylko u 2 pacjentów. Stwierdzono silną korelację stężeń kalcytoniny i prokalcytoniny u pacjentów z rakiem rdzeniastym tarczycy (r = 0,95; p = 0,004 dla aktywnej postaci raka rdzeniastego tarczycy, r = 0,60; p = 0,002 dla pacjentów z rakiem rdzeniastym tarczycy w stadium remisji). U pacjentów z ciężką infekcją oba wskaźniki były całkowicie niezależne (r = 0,002; p = 0,99).Wnioski. Prokalcytonina może być alternatywnym w stosunku do kalcytoniny markerem w ocenie stopnia zaawan-sowania raka rdzeniastego tarczycy (Adv Clin Exp Med 2012, 21, 2, 169–178).
Słowa kluczowe: prokalcytonina, kalcytonina, rak rdzeniasty tarczycy.

CT and PCT 171
PCT measurement is more available and af-fordable than CT measurement in many hospital laboratories [18].
Considering all these facts, the authors would like to assess PCT utility as a potential marker for MTC. To do this, they measured CT and PCT levels in four groups of patients: 1) MTC patients with active disease; 2) MTC patients in remission; 3) non-toxic nodular goiter (NTNG) patients; 4) patients with clinically- and laboratory-con-firmed bacterial infection.
Material and MethodsBlood samples were taken aseptically by veni-
puncture and serum was separated from the clot as soon as possible. The samples were stored frozen at –20°C.
Seventy-three serum samples were obtained from seventy patients.
The patients enrolled in the study were divid-ed into four groups.
Group 1 6 MTC patients with active disease (Table 1),
mean age 48.2, 5 females, 1 male. PCT and CT were measured once in 4 patients.
They had disseminated disease that made re-oper-ation impossible. In one patient (PU) (Table 1), CT and PCT levels were measured twice: first, one day before the second operation and next, three weeks after re-operation. She was re-operated on due to local neck recurrence. Liver metastases were excised in the last patient (MA), who unlike the others had disseminated MTC (Table 1). This patient’s blood was examined three times: first, the day before surgery and then twice, two weeks and three months following the resection of liver me-tastases.
Group 2 There were 23 MTC patients in remission
(Table 2), mean age 56.1, 17 females and 6 males. These patients underwent radical surgery (resec-tion r0) – total thyroidectomy and lymphadenec-tomy. Lymph node dissection was performed in four compartments – central, both lateral and upper mediastinal. This approach was consistent with the guidelines of the Association of Polish Surgeons and the Polish Society of Oncological Surgery. The final diagnosis was established by histopathology supported by immunohistochem-istry (to detect the presence of CT). The patients were disease-free in clinical and imaging exami-
nations. Their last CT level was measured in an out-patient department and it remained within the reference range. Post-operatively, all MTC patients received substitutive doses of levothyroxine to re-main euthyroid and were followed up in authors’ out-patient department.
Group 3There were 11 NTNG patients (Table 3), mean
age 49.5, 10 females and 1 male, whose diagnosis was confirmed by histopathology. All NTNG pa-tients underwent total thyroidectomy without lymphadenectomy.
The patients from groups 1–3 had no bacterial or fungal infection, renal failure or other carcino-mas.
Group 4There were 30 patients (Table 4) with severe,
bacterial infection or sepsis, mean age 59.5, 11 fe-males and 19 males.
Laboratory ExaminationThe frozen sera (–20°C) were taken to the lab-
oratory unit and assayed for CT and PCT levels.
CT MeasurementThe CT level was measured using the DiaSorin
LIAISON® Calcitonin Assay (DiaSorin Inc., USA).
This assay is a one-step sandwich chemilumines-cence immunoassay (CLIA) intended for the quan-titative determination of CT in human serum. An affinity-purified mouse antibody to the synthetic human CT is coated to a solid phase. A second affinity-purified mouse antibody is conjugated to an isoluminol derivative. During incubation, CT binds to the solid phase, and is subsequently bound by the isoluminol conjugated antibody. Following incubation, the unbound material is removed in a wash cycle. The starter reagents are then added and a flash chemiluminescent reaction is initiated. The light signal is measured by a photomultiplier as relative light units (rLU) and is proportional to the concentration of CT present in calibrators – controls or samples. The CT reference range is 0–5.5 pg/ml for women and 0–18.9 pg/ml for men.
PCT MeasurementThe PCT level was measured using the Liaison
Brahms PCT Assay (DiaSorin S.p.A., Italy). This as-say is a sandwich chemiluminescence immunoassay. A specific mouse monoclonal antibody is coated on magnetic particles (solid phase); another monoclo-nal antibody is linked to an isoluminol derivative

K. Kaczka et al.172
(isoluminol-antibody conjugate). During incuba-tion, the PCT present in the calibrators – samples or controls, binds to the monoclonal antibody in the solid phase and subsequently the antibody con-jugate reacts with PCT already bound to the solid phase. After incubation, the unbound material is removed in a wash cycle. Subsequently, the starter reagents are added and a flash chemiluminescence reaction is thus induced. The light signal and hence the amount of isoluminol-antibody conjugate is measured by a photomultiplier as relative light units (rLU) and is indicative of PCT concentration present in calibrators – samples or controls.
The PCT reference range is below 0.1 ng/ml.
Statistical AnalysisContinuous variables are presented as medians
and quartiles. A nonparametric Kruskall-Wallis analysis of variance was used for inter-group com-parisons with a Bonferroni-corrected Mann-Whit-ney U test used for post-hoc evaluation. A Spear-man rank correlation test was used for correlation assessment. A p value of < 0.05 was chosen as the statistical significance threshold.
ResultsThe four groups did not differ significantly
with respect to age, but showed marked differ-ences in both CT and PCT levels.
PCT and CT levels were higher in all active MTC patients – mean PCT 3.5 ng/ml and mean CT 973 pg/ml (Tables 1 and 2).
In patient (PU) (Table 1), PCT and CT levels were markedly increased (PCT 10.16 ng/ml and CT 1708 pg/ml). She was re-operated due to the local neck relapse. Cervical exploration and four-compartment lymphadenectomy was performed. Three weeks after re-operation, PCT and CT lev-els had decreased to 0.32 ng/ml and 63.2 pg/ml, respectively (Table 1).
In patient (MA) (Table 1), the PCT level was 6.67 ng/ml and the CT level was 2456 pg/ml. The patient had resectable liver metastases. Two weeks after radical surgical excision (resection r1), PCT and CT levels were much lower but still above the reference range. PCT was 2.92 ng/ml and CT was 995 pg/ml (Table 1). Three months after the opera-tion, clinical and imaging signs of relapse were ob-served. relapse was confirmed by markedly elevated levels of both markers – the PCT level was 4.1 ng/ml, and the CT level was 1441pg/ml (Table 1). In four other patients with active disseminated disease, both markers were significantly elevated (Table 1).
In MTC patients in remission, the mean PCT level was 0.06 ng/ml and the mean CT level was 3.12 ng/ml (Table 2). In 15 patients from this group, neither of the markers was elevated (Table 3). Five patients from this group (GB, BJ, WB, TL and BM) only had elevated CT levels (Table 3), while in three (KA, AW and WJ) (Table 3), the levels of both markers were slightly increased (Table 3).
In the NTNG group, PCT and CT levels were not elevated in all but one patient (DE) (Table 4).
In the group of patients with bacterial infection, the mean PCT level was 0.4 ng/ml and the mean CT level was 4.1 pg/ml (Table 2). The PCT and CT lev-
Table 1. The MTC active patients involved in the study, CT and PCT levels, clinical diagnosis
Tabela 1. Pacjenci chorzy na raka rdzeniastego tarczycy włączeni do badań, stężenie CT i PCT, rozpoznanie
Patient(Pacjent)
Age – years(Wiek – lata)
Gender(Płeć)
PCT level (ng/ml)(Stężenie PCT)
CT level (pg/ml)(Stężenie CT)
Clinical diagnosis(rozpoznanie)
PU 47 female 10.16 1708 MTC with lymph node metastases before operation
0.32 63.2 MTC with lymph node metastases after operation
MA 28 female 6.67 2456 MTC before resection of liver metastases
2.92 995 MTC following resection of liver metastases: 2 weeks later
4.1 1441 MTC following resection of liver metastases: 3 months later
PB 49 female 0.63 236 active MTC
MA 37 female 5.52 2010 active MTC
CB 65 female 0.76 159 active MTC
SZ 63 male 1.48 238 active MTC

CT and PCT 173
els were not increased in 8 patients from this group (Table 5). Both markers were elevated in 10 patients. While an increase in only PCT or CT levels were seen in 10 and 2 patients respectively (Table 5).
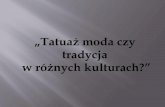
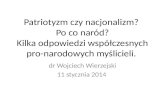
Levels of CT and PCT are shown in the Fig-ures 1 and 2, respectively.
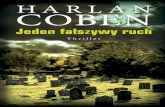
The statistical analysis shows that correlations between CT and PCT values were very strong and significant in individuals without infection – r = 0.95; p = 0.004 in patients with active MTC, r = 0.60; p = 0.002 in MTC patients in remission, r = 0.77; p = 0.02 in patients with NTNG. In indi-viduals with inflammation, both parameters were completely independent – r = 0.002; p = 0.99.
The authors concluded that PCT shows a similar distribution of values to CT and strongly correlates with CT levels in the patients without infection. Greatly elevated PCT levels in patients with active MTC or infection in contrast to both individuals in remission and NTNG offers poten-tial for using PCT as a diagnostic marker of either condition, while CT values can only be used to as-certain active MTC status.
Table 2. Levels of analyzed markers within the studied groups
Tabela 2. Stężenia badanych wskaźników w grupach
MTC active patients(Pacjenci chorzy na raka rdzeniastego tarczycy w fazie aktywnej)
MTC patients in remission(Pacjenci chorzy na raka rdzeniastego tarczycy w remisji)
NTNG patients(Pacjenci z wolem guzowatym obojętnym)
Patients with inflammation(Pacjenci z zakażeniem)
P
Age(Wiek)
48 (IQr 37–63) (min-max 28–65)
59 (IQr 44–69) (min-max 19–79)
46 (IQr 42–63) (min-max 29–66)
59 (IQr 47–70) (min-max 28–88)
0.2656
CT 973 (IQr 236–2010) (min-max 159–2456)
3.12 (IQr 1.27–7.70) (min-max 0.04–40.60)
2.66 (IQr 1.56–4.59) (min-max 0.12–10.10)
4.10 (IQr 0.87–7.50) (min-max 0.06–19.80)
0.0000
PCT 3.50 (IQr 0.76–6.67) (min-max 0.63–10.16)
0.06 (IQr 0.03–0.08) (min-max 0.01–0.27)
0.06 (IQr 0.01–0.10) (min-max 0.00–0.28)
0.40 (IQr 0.10–0.51) (min-max 0–42. 19)
0.0006
Table 3. The MTC patients in remission involved in the study, CT and PCT levels, clinical diagnosis
Tabela 3. Pacjenci chorzy na raka rdzeniastego tarczycy w remisji włączeni do badań, stężenie CT i PCT, rozpoznanie
Patient(Pacjent)
Age – years(Wiek – lata)
Gender(Płeć)
PCT level (ng/ml)(Stężenie PCT)
CT level (pg/ml)(Stężenie CT)
Clinical diagnosis(rozpoznanie)
GBKJBJGBSJKBSSMMSAOBOArUWBTL BBBMKJKAAWNrSM WJKK
7975676274577429443919764565466263365937565769
femalemalefemalemalefemalemalemalefemalefemalefemalefemalefemalefemalefemalefemalefemalemalefemalemalefemalefemalefemalefemale
< 0.1< 0.1< 0.1< 0.1< 0.1< 0.1< 0.1< 0.1< 0.1< 0.1< 0.1< 0.1< 0.1< 0.1< 0.1< 0.1< 0.1 0.15 0.16< 0.1< 0.1 0.27< 0.1
7.7< 5 13.3< 5< 5< 5< 5< 5< 5< 5< 5< 5 6.6 6.8< 5 11< 5 9.62 40.6< 5< 5 21.9< 5
MTC in remissionMTC in remissionMTC in remissionMTC in remissionMTC in remissionMTC in remissionMTC in remissionMTC in remissionMTC in remissionMTC in remissionMTC in remissionMTC in remissionMTC in remissionMTC in remissionMTC in remissionMTC in remissionMTC in remissionMTC in remissionMTC in remissionMTC in remissionMTC in remissionMTC in remissionMTC in remission

K. Kaczka et al.174
Discussion Although the prevalence of hypercalcitonin-
emia unrelated to MTC varies from 0.3% to 4.5% [19, 20], routine measurement of serum calcitonin level has been advocated by some authors as a pos-
sible marker of MTC among patients with nodular thyroid diseases [21, 22]. The assay’s high cost and lack of specificity [23] has dissuaded US health au-thorities from adopting systematic testing [23].
After surgery, patients with MTC were followed up with CT measurements. A strong correlation be-
Table 4. The NTNG patients involved in the study, CT and PCT levels, clinical diagnosis
Tabela 4. Pacjenci z wolem guzowatym obojętnym włączeni do badań, stężenie CT i PCT, rozpoznanie
Patient(Pacjent)
Age – years(Wiek – lata)
Gender(Płeć)
PCT level (ng/ml)(Stężenie PCT)
CT level (pg/ml)(Stężenie CT)
Clinical diagnosis(rozpoznanie)
WJMGDKMIŁWKWDEHCNZDANZ
4239295566634765464646
femalefemalefemalefemalefemalemalefemalefemalefemalefemalefemale
< 0.1< 0.1 0.12< 0.1< 0.1< 0.1 0.28< 0.1< 0.1< 0.1< 0.1
< 5< 5< 5< 5< 5< 5 10.1< 5< 5< 5< 5
NTNGNTNGNTNGNTNGNTNGNTNGNTNGNTNGNTNGNTNGNTNG
Table 5. The patients with bacterial infection involved in the study, CT and PCT levels, clinical diagnosis
Tabela 5. Pacjenci z zakażeniem bakteryjnym włączeni do badań, stężenie CT i PCT, rozpoznanie
Patient(Pacjent)
Age – years(Wiek – lata)
Gender(Płeć)
PCT level (ng/ml) < 0.1(Stężenie PCT)
CT level (pg/ml) < 5(Stężenie CT)
Clinical diagnosis(rozpoznanie)
GMJDEKWMrWKS SHKPSWrAPG SAGMrWZAKJZWWZSSDPFFMTKJSMWCZAAMJSMPTr
884329416065598380455784566057594674602861387550604783705670
femalemalemalemalefemalemalemalemalefemalefemalemalefemalefemalefemalemalemalemalefemalemalemalefemalemalemalefemalefemalemalefemalemalemalemale
4.65 0.51 0.12< 0.1 0.48 0.45 42.19 0.51 1.05< 0.1< 0.1< 0.1 0.34 5.55< 0.1< 0.1 0.38 1.54 11.13< 0.1 15.8 0.11 0.42< 0.1 0.41 0.46< 0.1< 0.1 0.41 0.23
< 5 6.9< 5< 5< 5< 5< 5< 5< 5< 5< 5 8.81< 5< 5< 5< 5 9.72 7.83 19.84< 5< 5 9.25 7.56< 5 5.67 8.38< 5 7.32 5.89 10.710
acute cholecystitisacute pancreatitisacute pancreatitisacute cholecystitisleft calf phlegmonright foot phlegmonperineum phlegmonright stump purulencesevere pneumoniasevere pneumoniaacute cholecystitissevere pneumoniabuttock abscesspleural empyemaright stumppurulenceacute pancreatitisacute pancreatitissevere pneumoniasepsisacute appendicitisacute cholecystitisacute pancreatitissepsisacute cholecystitisacute pancreatitissevere pneumoniaurosepsissevere pneumoniasepsissepsis

CT and PCT 175
Fig. 1. Comparisons of CT levels in the studied groups
Ryc. 1. Porównanie stężenia CT w grupach
Fig. 2. Comparisons of PCT levels in the studied groups
Ryc. 2. Porównanie stężenia PCT w grupach
Ca active ca remis Goiter Inflammation
0
200
400
1600
1800
2000
2200
2400
2600
CT
[ng/
ml]
Ca active Ca remission Goiter Inflammation
0
5
10
15
2040
45
PC
T [n
g/m
l]

K. Kaczka et al.176
tween clinical stage and CT level was observed in MTC patients. However, a minimal to moderate in-crease of serum calcitonin level has frequently been observed in diseases other than MTC [7, 8]. Addi-tionally, as was mentioned earlier, measuring the CT level has some laboratory inadequacies. Still, its advantages include: a constant and predictable half-life, absence of isoforms, excellent in-vitro stability and analytical consistency between assays [24]. For these reasons, there is a need to find an alternative for CT measurement in MTC. Perhaps PCT could be a better marker than CT. PCT assays are com-monly used in many laboratories which do not per-form CT estimations. Physiologically, PCT level is low. It is increased in bacterial and fungal infections and is considered an inflammatory marker. More-over, it has recently been shown that PCT is a valu-able tool to guide antibiotic treatment in patients with serious bacterial infections [25, 26]. Some stud-ies suggest that a PCT-based algorithm significantly shortens the length of antibiotic therapy without af-fecting the treatment and outcome [25, 26]. Beyond shortening the time of antibiotic treatment, it also has a favorable effect on the time of hospitalization in the intensive care department [27].
In this study, the authors would like to assess
PCT utility as a potential marker for MTC. To do this, they measured CT and PCT levels in four groups of patients.
PCT and CT levels were higher in all active MTC patients. In the re-operated patients from this group, the levels of both markers decreased post-operatively. The statistical analysis shows very strong and significant correlations between CT and PCT values in patients with active MTC. The results are similar to those obtained in other studies [27, 28].
In the group of patients in remission, both markers were not increased in 15 patients, 3 pa-tients had both markers slightly elevated, while 5 only showed increased CT levels.
Also in this group of patients, correlations be-tween CT and PCT values were very strong and significant. This suggests that PCT could be used as a marker in the follow-up of MTC patients.
Eleven patients with histopathologically con-firmed NTNG were included in the study as a con-trol group. PCT and CT levels in these patients were not elevated, except in one patient (DE), before routine thyroidectomy, in whom slightly elevated PCT and CT levels were observed. The fact that the PCT level is not increased in NTNG
Fig. 3. Correlation of log-transformed values of PCT and CT levels
Ryc. 3. Korelacja przekształconych logarytmicznie wartości PCT I CT

CT and PCT 177
patients and that it is increased in all active MTC patients is very hopeful. It allows authors to use PCT measurement as a screening test for MTC. Additionally, PCT measurement is cheaper and more available in many hospital laboratories.
PCT and CT levels were also checked in 30 patients with serious bacterial infections or sepsis. Only two patients, who had normal PCT levels, had slightly elevated CT levels, suggesting that CT is not a specific marker for infection or sepsis.
In the statistical analysis of this group, both parameters were completely independent.
In summary, this study showed that PCT has a similar distribution of values to calcitonin in MTC. A significant correlation was observed be-tween these two markers in MTC patients while no correlation was seen in individuals with infec-tion. These facts and PCT’s analytical advantages allow one to use PCT together with CT for the evaluation of MTC status. Additional prospective studies should be performed to check if PCT mea-surement could be an alternative to CT measure-ment. Present results encourage the performance of further studies.
References Zhong Y, Armbrecht HJ, Christakos S: [1] Calcitonin, a regulator of the 25-Hydroxyvitamin D3 1α-Hydroxylase Gene. J Biol Chem 2009, 284, 11059–11069.Constante G, Merongolo D, Durante C, Bianchi D, Nocera M, Tumino S et al.: [2] Predictive value of serum calci-tonin levels for preoperative diagnosis of medullary in a cohort of 5817 consecutive patients with thyroid nodules. J Clin Endocrinol Metab 2007, 92, 450–455.Pomorski L, Cywiński J, Kołomecki K, Pasieka Z, Bartos M, Kuzdak K: [3] recurrences of thyroid cancer after radi-cal surgery and complementary treatment: are macroscopic, microscopic, scintigraphic, and biochemical criteria sufficient in the evaluation of radicality of primary treatment? recent results Cancer res 2003, 162, 203–207.Niccoli P, Wion-Barbot N, Caron P, Henry JF, de Micco C, Saint Andre JP et al.: [4] Interest of routine measure-ment of serum calcitonin: study in a large series of thyroidectomized patients. The French Medullary Study Group. J Clin Endocrinol Metab 1997, 82, 338–341.Lew-Bohbot N, Patey M, Larbre M, Hecart AC, Caron J, Delemer B: [5] How to interprete hypercalcitonemia. rev Med Intern 2006, 27, 610–615.Iacobone M, Niccoli-Sire P, Sebag F De Micco C, Henry JF: [6] Can sporadic medullary thyroid carcinoma be bio-chemically predicted? Prospective analysis of 66 operated patients with elevated serum calcitonin levels. World J Surg 2002, 26, 886–890.Algecitras-Schimnich A, Preissner C, Theobald P, Finseth MS, Grebe SK: [7] Procalcitonin: a marker for the diag-nosis and follow-up of patients with medullary thyroid carcinoma. J Clin Endocrin Metab 2008, 94, 861–868.Akan B, Böhmig G, Sunder-Plassmann G, Borchhardt KA: [8] Prevalence of hypercalcitoninemia in patients on maintenance dialysis referred to kidney transplantation. Clin Nephrol 2009, 71, 538–542.Tomamsi M, Brocchi A, Cappellini A, Raspanti S, Mannelli M: [9] False serum calcitonin high levels using a non-competitive two-site IrMA. J Endocrinol Invest 2001, 24, 356–360.Cole TG, Johnson D, Eveland BJ, Nahm MH:[10] Cost-effective method for detection of ’’hook effect’’ in tumor marker immunometric assays. Clin Chem 1993, 39, 695–696.Leboeuf R, Langlois MF, Martin M, Ahnadi CE, Fink GD:[11] “Hook Effect” in calcitonin immunoradiometric assay in patients with metastatic medullary thyroid carcinoma: case report and review of the literature. J Clin Endocrin Metab 2006, 91, 361–364.Leboulleux S, Baudin E, Travagli JP, Schlumberger M:[12] Medullary thyroid carcinoma 2004, 61, 299–310.Morimoto S, Onishi T, Takamoto S, Imanaka S, Fukuo K, Tsuchiya H et al.:[13] Interference in radioimmunoassay of human calcitonin by vitamin C and urea. Med J Osaka Univ 1985, 35, 77–82.Summah H, Qu JM:[14] Biomarkers: a definite plus in pneumonia. Mediators Inflamm 2009, 2009, 675–753.Bihan H, Becker KL, Snider RH, Nylen E, Vittaz L, Lauret C et al.:[15] Calcitonin precursor levels in human medul-lary thyroid carcinoma. Thyroid 2003, 13, 819–822.Chastre J, Luyt CE, Trouillet JL, Combes A:[16] New diagnostic and prognostic markers of ventilator-associated pneumonia. Curr Opin Crit Care 2006, 12, 446–451Meisner M, Schmidt J, Hüttner H, Tschaikowski K:[17] The natural elimination rate of procalcitonin in patients with normal and impaired renal function. Intensive Care Med 2000, 26 Suppl 2, S21 12–16.Shehabi Y, Seppelt I:[18] Pro/Con debate: is procalcitonin useful for guiding antibiotic decision making in critically ill patients? Crit Care 2008, 12, 211.Vierhapper H, Niederle B, Bieglmayer C, Kaserer K, Baumgartner-Parzer S:[19] Early diagnosis and curative ther-apy of medullary thyroid carcinoma by routine measurement of serum calcitonin in patients with thyroid disor-ders. Thyroid 2005, 15, 1267–1272. Vantyghem MC, Pigny P, Leteurtre E, Leclerc L, Bauters C, Douillard C et al.:[20] Thyroid carcinomas involving follicular and parafollicular C cells: seventeen cases with characterization of rET oncogenic activation. Thyroid 2004, 14, 842–847. Hasselgren M, Hegedüs L, Godballe C, Bonnema SJ:[21] Benefit of measuring basal serum calcitonin to detect med-ullary thyroid carcinoma in a Danish population with a high prevalence of thyroid nodules. Head Neck 2010, 32, 612–618.

K. Kaczka et al.178
Papi G, Corsello SM, Cioni K, Pizzini AM, Corrado S, Carapezzi C et al.:[22] Value of routine measurement of serum calcitonin concentrations in patients with nodular thyroid disease: A multicenter study. J Endocrinol Invest 2006, 29, 427–437.Borget I, De Pouvourville G, Schlumberger M:[23] Editorial: calcitonin determination in patients with nodular thy-roid disease. J Clin Endocrinol Metab 2007, 92, 425–427.Martinetti A, Seregni E, Ferrari L, Pallotti F, Aliberti G, Coliva A et al.:[24] Evaluation of circulating calcitonin analytical aspects. Tumori 2003, 89, 566–568.Christ-Crain M, Stolz D, Bingisser R, Müller C, Miedinger D, Huber PR et al.:[25] Procalcitonin guidance of anti-biotic therapy in community-acquired pneumonia: a randomized trial. Am J respir Crit Care Med 2006, 174, 84–93.Nobre V, Harbarth S, Graf JD, Rohner P, Pugin J:[26] Use of procalcitonin to shorten antibiotic treatment duration in septic patients. A randomized trial. Am J respir Crit Care Med 2008, 177, 498–505.Matzaraki V, Alexandraki KI, Venetsanou K et al.:[27] Evaluation of serum procalcitonin and interleukin-6 levels markers of liver metastasis. Clin Biochem 2007, 40, 336–342.Algeciras-Schimnich A, Preissner CM, Theobald JP, Finseth MS, Grebe SK:[28] Procalcitonin: a marker for the diagnosis and follow-up of patients with medullary thyroid carcinoma. J Clin Endocrinol Metab 2009, 94, 861–868.
Address for correspondence:Krzysztof KaczkaDepartment of General and Oncological SurgeryMedical University of ŁódźMaria Skłodowska-Curie Memorial HospitalParzęczewska 3595-100 ZgierzPolandE-mail: [email protected]. +48 503 068 786
Conflict of interest: None declared
received: 2.05.2011revised: 21.06.2011Accepted: 29.03.2012