matematyka w kardiologii

of 155
-
Upload
sylwia-wojdan -
Category
Documents
-
view
224 -
download
0
Transcript of matematyka w kardiologii
-
8/7/2019 matematyka w kardiologii
1/155
Mathematical modeling and spectral simulation of genetic diseases in the human heart
Ph.D. Dissertation
Alfonso Bueno OrovioDepartment of Mathematics
University of Castilla-La Mancha
Ciudad Real, May 2007
-
8/7/2019 matematyka w kardiologii
2/155
Ph.D. Advisors:Prof. Dr. Vctor M. Perez GarcaDepartment of MathematicsUniversity of Castilla-La Mancha, Spain
Dr. Flavio H. FentonDepartment of Biomedical EngineeringCornell University, U.S.A.
The studies described in this thesis were performed at the department of Mathematicsat the University of Castilla-La Mancha within the framework of the FisyMat Ph.D.program on Physics and Mathematics. The investigations were nancially supportedby the Consejera de Eduacion y Ciencia of the Junta de Comunidades de Castilla-LaMancha under Ph.D. grant 03-056.
-
8/7/2019 matematyka w kardiologii
3/155
To Alvaro,because you drive my heart.
-
8/7/2019 matematyka w kardiologii
4/155
-
8/7/2019 matematyka w kardiologii
5/155
Contents
1 Basics of cardiac electrical activity modeling 1
1.1 Thesis objectives . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11.2 Why modeling in cardiac electrophysiology . . . . . . . . . . . . . . . 11.3 Electrical function of the heart . . . . . . . . . . . . . . . . . . . . . . 3
1.3.1 Macroscopic description of the cardiac cycle . . . . . . . . . . 31.3.2 Cardiac tissue as a model of excitable media . . . . . . . . . . 41.3.3 The cardiac action potential . . . . . . . . . . . . . . . . . . . 5
1.4 Modeling cardiac electrical activity . . . . . . . . . . . . . . . . . . . 81.4.1 Equivalent electric circuit of the cell membrane . . . . . . . . 81.4.2 The Hodgkin and Huxley formalism . . . . . . . . . . . . . . . 91.4.3 Biophysically-based cardiac ionic models . . . . . . . . . . . . 10
1.4.4 Simplied models of cardiac electrical activity . . . . . . . . . 131.5 Propagation of cardiac electrical activity . . . . . . . . . . . . . . . . 181.5.1 The monodomain equations . . . . . . . . . . . . . . . . . . . 181.5.2 Planar and spiral waves in cardiac tissue . . . . . . . . . . . . 20
1.6 Numerical solution of cardiac tissue models . . . . . . . . . . . . . . . 221.7 Spectrally accurate methods . . . . . . . . . . . . . . . . . . . . . . . 231.8 Thesis summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
I Simplied mathematical modeling of human ventricularaction potentials 29
2 Minimal model for human ventricular action potentials 312.1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 312.2 Materials and methods . . . . . . . . . . . . . . . . . . . . . . . . . . 32
2.2.1 Mathematical model . . . . . . . . . . . . . . . . . . . . . . . 322.2.2 Other models of human ventricular action potentials . . . . . 352.2.3 Diffusion coefficient calculation . . . . . . . . . . . . . . . . . 352.2.4 Computational methods . . . . . . . . . . . . . . . . . . . . . 35
2.3 Results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 362.3.1 Minimal model properties . . . . . . . . . . . . . . . . . . . . 36
2.3.2 Comparison of human ventricular action potentials . . . . . . 372.3.3 Restitution of APD and CV . . . . . . . . . . . . . . . . . . . 38
v
-
8/7/2019 matematyka w kardiologii
6/155
vi CONTENTS
2.3.4 Reentry stability . . . . . . . . . . . . . . . . . . . . . . . . . 402.3.5 Transmural heterogeneity and pseudo-ECG . . . . . . . . . . . 422.3.6 Parameter ttings to other models . . . . . . . . . . . . . . . 42
2.4 Discussion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 442.4.1 Reentry stability . . . . . . . . . . . . . . . . . . . . . . . . . 442.4.2 Model complexity, efficiency and numerical resolution . . . . . 442.4.3 Transmural heterogeneity . . . . . . . . . . . . . . . . . . . . 452.4.4 Minimal model to reproduce experimental and numerical data 452.4.5 Limitations of the study . . . . . . . . . . . . . . . . . . . . . 46
2.5 Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 46
3 The Brugada syndrome: Insights from computer simulations 473.1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 473.2 Materials and methods . . . . . . . . . . . . . . . . . . . . . . . . . . 48
3.2.1 Mathematical model . . . . . . . . . . . . . . . . . . . . . . . 483.2.2 Previous mathematical models of Brugada syndrome . . . . . 503.2.3 Computational methods . . . . . . . . . . . . . . . . . . . . . 51
3.3 Results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 513.3.1 Model validation: Brugada syndrome action potentials . . . . 513.3.2 Model validation: ECG manifestations of Brugada syndrome . 533.3.3 Possible mechanisms for generation of phase 2 reentry . . . . . 55
3.4 Discussion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 613.4.1 Comparison with previous simulation studies . . . . . . . . . . 613.4.2 Factors in the generation of phase 2 reentry . . . . . . . . . . 63
3.4.3 Limitations of the model . . . . . . . . . . . . . . . . . . . . . 653.5 Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 65
II Spectral simulation schemes in electrophysiology andirregular domains 67
4 Low and high order methods in cardiac tissue simulations 694.1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 694.2 Materials and methods . . . . . . . . . . . . . . . . . . . . . . . . . . 70
4.2.1 Time integration of the reaction and diffusion terms . . . . . . 70
4.2.2 Numerical approximation of spatial derivatives . . . . . . . . . 734.2.3 Ionic cellular models in study . . . . . . . . . . . . . . . . . . 774.2.4 Criteria for time and space step selection . . . . . . . . . . . . 78
4.3 Results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 784.3.1 Numerical convergence of the wavefront speed . . . . . . . . . 784.3.2 Effects of time integration on wavefront speed convergence . . 794.3.3 Inuence of ionic models on numerical convergence . . . . . . 824.3.4 Efficiency of the numerical schemes . . . . . . . . . . . . . . . 834.3.5 Spatial accuracy of spiral wave trajectories . . . . . . . . . . . 85
4.4 Discussion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 85
4.4.1 Mesh size reduction by the use of spectral methods . . . . . . 854.4.2 Remarks on spatial adaptation . . . . . . . . . . . . . . . . . . 86
-
8/7/2019 matematyka w kardiologii
7/155
CONTENTS vii
4.4.3 Time integration of spectral schemes . . . . . . . . . . . . . . 874.4.4 Use of ionic models without stiff calcium dynamics . . . . . . 87
4.5 Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 88
5 The spectral smoothed boundary method 895.1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 895.2 The smoothed boundary method . . . . . . . . . . . . . . . . . . . . 905.3 Spectral implementation . . . . . . . . . . . . . . . . . . . . . . . . . 925.4 Examples of the methodology . . . . . . . . . . . . . . . . . . . . . . 95
5.4.1 The heat equation . . . . . . . . . . . . . . . . . . . . . . . . 955.4.2 The AllenCahn equation . . . . . . . . . . . . . . . . . . . . 985.4.3 Reaction-diffusion equations and excitable media . . . . . . . 99
5.5 Role of external boundaries conditions . . . . . . . . . . . . . . . . . 1035.6 Discussion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 106
6 Applications to mixed spectral/boundary elements methods 1096.1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1096.2 Mixed spectral/boundary element methods . . . . . . . . . . . . . . . 1106.3 The error-function-like extension . . . . . . . . . . . . . . . . . . . . 1116.4 Extension via convolution with Gaussian kernels . . . . . . . . . . . . 1126.5 Comparison between explicit extensions . . . . . . . . . . . . . . . . . 1146.6 Mixed spectral/BEM: A numerical example . . . . . . . . . . . . . . 1156.7 Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 116
7 Thesis discussion 1197.1 Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1197.2 Future extensions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 121
A Equations of detailed ionic models 123A.1 Hodgkin and Huxley model (1952) . . . . . . . . . . . . . . . . . . . 123A.2 Beeler-Reuter model (1977) . . . . . . . . . . . . . . . . . . . . . . . 124A.3 Luo-Rudy I model (1991) . . . . . . . . . . . . . . . . . . . . . . . . . 126
Honors and publications 129
Acknowledgments 131
Bibliography 133
-
8/7/2019 matematyka w kardiologii
8/155
-
8/7/2019 matematyka w kardiologii
9/155
Chapter 1Basics of cardiac electrical activitymodeling
1.1 T HESIS OBJECTIVES
The objectives of the present thesis can be summarized in three main cat-egories: (i) the creation of new cellular ionic models, computationally effi-cient but exible enough as to accurately reproduce the electrical propertiesof cardiac myocytes, both in healthy and pathological conditions; (ii) the
development and implementation of high order computational methods for the nu-merical simulation of the electrical activity of the heart, trying also to incorporate tosuch methods the irregular geometry of the cardiac muscle, aspect of great importancein the degeneration of certain arrhythmias into lethal ventricular brillation; and (iii)practical electrophysiological applications, such as the modeling and characterizationof genetic diseases able to produce sudden cardiac death.
Therefore, this thesis only covers electrophysiological aspects regarding the elec-trical activity of the human heart. Other related aspects to the cardiac cycle, such
as muscle contraction or blood ow, are thus not considered here.
1.2 W HY MODELING IN CARDIAC ELECTROPHYSIOLOGY
Cardiovascular diseases are the leading cause of death in the industrialized world. Inthe United States, they are responsible of the 32.5% of total deaths in males, whilstthe rate is of 26.6% in women. In Spain, although the incidence is lower, it is still amajor worry, representing the 25.2% of total deaths in men and the 23.7% in women(source: The World Health Organization Web page, who.int/whosis ). Within thishigh mortality rates, sudden cardiac death, primarily caused by ventricular arrhyth-mias, is a serious public health problem, resulting in more than 500 000 deaths eachyear in the United States (Thom et al., 2006). Despite intense research efforts in
1
-
8/7/2019 matematyka w kardiologii
10/155
2 1.2 Why modeling in cardiac electrophysiology
the past decades, the mechanisms involved in the initiation and maintenance of thesearrhythmias remain largely unknown.
In recent years, the study of the hearts electrical activity (called cardiac elec-
trophysiology) has evolved from a discipline of interest primarily to physicians andphysiologists to one that has caught the attention of physicists, mathematicians, andengineers. Such scientists have come to realize that cardiac dynamics are character-ized by many of the same principles that underlie the physical systems with whichthey are intimately familiar. In this context, mathematical modeling has proved to bethe perfect framework where to combine the quantitative data coming from researchand experiments with a qualitative understanding in order to produce an explanatoryand predictive tool. This type of biophysical modeling from a physical and mathe-matical point of view has made possible that many basic concepts involved in cardiacarrhythmias were formulated rst based on simple, generalized models of excitable
media. Examples include the multiple wavelet hypothesis for brillation (Moe et al.,1964; Krinsky, 1966), spiral waves as the dynamics underlying tachycardia, with spi-ral breakup being the force driving brillation (Winfree, 1989; Panlov and Holden,1990), the formation and anchoring of spiral waves produced by inexcitable obstacles(Agladze et al., 1994), or the vulnerability window of excitable media as a conditionfor spiral wave formation (Krinsky, 1966; Winfree, 1989).
Another reason for using models are the practical and ethical limitations inherentto clinical and experimental investigation. It seems plausible than in a near futureethical committees will start requiring computational evidences of research interestprior to approve in-vivo experimentation. In this way, computer-based models seem
to be the only conceivable alternative to follow up on animal experimentation. Ethicallimitations are even bigger when they concern to clinical research with human hearts,where data obtaining is limited to noninvasive measurements such as electrocardio-graphic recordings and body surface mappings, low risk invasive measurements suchas catheter mapping and multi-electrode array mapping on hearts of people undergo-ing cardiac surgery, or in vitro experiments on the small number of explanted humanhearts available for research. Mathematical models therefore represent the perfectplatform where safely testing multiple hypothesis without incurring in any cardiacrisk for the patient, or to test conditions not easily reproducible in experiments.
One argument that is often placed against the mathematical models of the cardiacprocesses is that they cannot be predictive, in the sense that they are capable onlyof reproducing the experimental results that were used to create them. However,evidence already exists that shows how models can provide insight into the underly-ing mechanisms of cardiac electrical activity, as proved in Rudy (2000), work whichallowed the mechanism of early after depolarizations to be elucidated. This and otherexamples provide strong evidence that even now models of the cardiac processes arealready being used in a predictive manner, not just to reproduce experimental data. Itis therefore not unlikely that mathematical models will start being used in the clinicalpractice in a near future, using geometrical tri-dimensional models of patient-specichearts reconstructed from ultrasounds or magnetic resonance images, in combinationwith ionic models tted to reproduce patient conditions measured for instance bycatheterism. This might require, however, an appropriate education of the medical
-
8/7/2019 matematyka w kardiologii
11/155
CHAPTER 1. Basics of cardiac electrical activity modeling 3
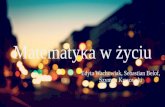
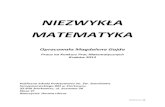
Figure 1.1: Anterior view of the opened heart. Arrows indicate normal blood ow.
profession in order to allow such a tool to be widely adopted in clinical practice bothfor prediction and prevention.
1.3 E LECTRICAL FUNCTION OF THE HEART
1.3.1 MACROSCOPIC DESCRIPTION OF THE CARDIAC CYCLE
The heart is situated slightly to the left of the middle of the thorax, underneath thesternum, between the lungs. It is supported inside a membranous structure known asthe pericardial sac , a double membrane structure containing a serous uid to reducefriction during heart contractions. There are four major chambers in the heart: thelarger, lower, thicker walled chambers are the ventricles , while the smaller, upper,thinner chambers are the atria . The bottom of the ventricles is called the apex andtheir top part is known as the base.
Both the atria and the ventricles are separated into independent left and righthalves by the septal wall . The function of the right atrium is to collect deoxygenatedblood from the body. After contraction of the atria, this blood is passed to theright ventricle and pumped into the lungs (pulmonary circulation) to produce thegas exchange between carbon dioxide and oxygen. The reoxygenated blood from thelungs is then collected in the left atrium, from where it moves to the left ventricle
-
8/7/2019 matematyka w kardiologii
12/155
4 1.3.2 Cardiac tissue as a model of excitable media
which pumps it out to the body. Since the right ventricle only pumps blood throughthe pulmonary circulation system of the lungs, whilst the left ventricle pumps bloodto the rest of the body, the left ventricle is considerably thicker than the right asappreciated in Fig. 1.1.
Mechanical contraction of the heart is caused by the electrical activation of my-ocardial cells. The electrical activation sequence (Fig. 1.2) of the human heart startsat the sinoatrial node , located in the right atrium at the superior vena cava. Thisnode consists of specialized muscle cells which are self-excitatory, pacemaker cells,able to generate an electrical impulse at a rate of about 70 per minute. From thesinoatrial node, the wave of electrical activation propagates throughout the atria, butcannot propagate directly across the annulus of separation between the atria and theventricles. The atrioventricular node , located at the boundary between the atria andventricles, is the only conducting path from the atria to the ventricles in a normalheart. Conduction velocity through the atrioventricular node is considerably delayedin order to supply enough time to the atria to ll the ventricles with blood beforethe beginning of their contraction. Propagation then proceeds through a specializedconduction system, called the bundle of His. After a short distance, it separatesinto two bundle branches propagating along each side of the septum, constitutingthe left and right bundle brunches. Both branches then continue to subdivide intoa complex network of bres called the Purkinje bre network , which spreads acrossthe endocardial surface and into the subendocardial region of both ventricles. Thefast conduction through the bundle branches and Purkinje bres causes the entireendocardium to be excited almost simultaneously, although apical regions contractrst and the basal regions are usually the latest to be excited.
1.3.2 CARDIAC TISSUE AS A MODEL OF EXCITABLE MEDIA
Excitable media are spatially distributed systems which have the ability to propagatesignals without damping. This is in contrast to passive wave propagation, which ischaracterized by a gradual damping of signal amplitude due to friction. Althoughit could be challenging to nd an exact denition, excitable media can be dened ingeneral as systems composed of elementary segments or cells, each of which possessesthe following properties: (i) a well-dened rest state; (ii) a threshold for excitation;(iii) a refractory period in which the system can not be re-excited; and (iv) a diffusive-type coupling to its neighbors. Examples of excitable media may include from a forestre, which travels as a wave from its initiation point, regenerating with every treeit ignites, to the aggregation to slime mold amoebas (Foerster et al., 1990), certainchemical reactions (Zaikin and Zhabotinsky, 1970), signal transmission in nerves(Hodgkin and Huxley, 1952) or cortical tissue (Huang et al., 2004), or propagationof electrical activity in cardiac tissue (Moe et al., 1964; Winfree, 1980).
By a threshold of excitation , we mean that any external stimulus applied to acell that keeps the cell below this threshold produces a qualitatively different resultthan a stimulus that raises the cell above threshold. Stimuli below the threshold aredamped out and produce no persistent change in the system, which simply returns tothe rest state . However, stimuli above the threshold induce the cell to change from itsrest state to an excited state. This change produces a pulse in time whose shape andnature are determined by the nonlinear properties of the medium and do not depend
-
8/7/2019 matematyka w kardiologii
13/155
CHAPTER 1. Basics of cardiac electrical activity modeling 5
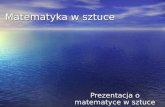
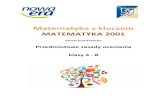
Figure 1.2: Electrophysiology of the heart. The different action potentials for eachof the specialized cells found in the heart, and their contribution to the total electro-
cardiogram waveform, are shown (modied from Malmivuo and Plonsey, 1995).
on the form of the external excitation. In spatially-extended excitable systems, theexcitation pulse may be carried over from one elementary segment to the next bymeans of a diffusive coupling . As each element undergoes an excursion from restingstate, it causes its neighbors to move over excitation threshold and re their activeresponse. The excitability of the system and the coupling strength between neighborsdetermines the minimum size of tissue required for a pulse to expand and propagateas a traveling wave front.
All the above mentioned properties can be found and characterized in the study of cardiac muscle. In consequence, the following section provides a detailed descriptionon how cardiac cells and tissue qualify as excitable media.
1.3.3 THE CARDIAC ACTION POTENTIAL
Cardiac muscle cells or myocytes are approximately attened tubes, about 80-100 mlong in human ventricular tissue, with elliptic cross sections with a major axis of 10-20 m. They are arranged in discrete layers of bres called sheets, roughly parallelto the heart surfaces (epicardium and endocardium), with the ber axis continuouslyrotating counterclockwise from epicardium to endocardium in a range of 100 o-120o
as viewed from the top of epicardium.Each cardiac muscle cell is bounded by a thin (5-7 nm) phospholipic membrane
-
8/7/2019 matematyka w kardiologii
14/155
6 1.3.3 The cardiac action potential
or sarcolemma . This membrane encapsulates a small volume that is known as theintracellular space , whereas the extracellular or interstitial space is therefore denedas the space that lies outside the sarcolemma. The membrane is heterogeneous, withnumerous large, complex proteins embedded within it, that combine to form smallpores in the cell membrane. Under most circumstances these pores are selectivelypermeable, allowing the pass of only specic ions through the membrane and onlyunder certain conditions, reason why they are commonly called ion channels .
The main ions that are of interest in cardiac electrophysiology are Na + , K+ , Ca2+
and Cl. At rest, the intracellular and extracellular concentrations of each ion aresubstantially different. In principle, this difference on concentrations would producea chemical force that would make ions to ow down their concentration gradient tocreate a uniform distribution at both sides of the membrane. Nevertheless, differentionic concentrations also imply a net electrical charge difference between both sidesof the membrane, what causes the establishment of an electrical gradient that acts tooppose the chemical gradient, thus allowing intra- and extracellular concentrationsto be different. Consequently, at rest the cell membrane maintains a net membranepotential, which for cardiac muscle cells generally is between -90 and -80 mV, andthe cell membrane is said to be in polarized state.
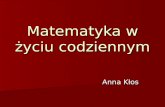
However, under electrical excitation of the cell this electrochemical equilibrium isbroken, what allows ions to ow through those ion channels to which they are perme-able, if opened. Any positive increase of the transmembrane potential towards zero istherefore known as depolarization , while the term repolarization refers to the returningof the cell to its negative resting state. Small perturbations in the potential differenceacross the cell membrane produce only a passive, linear response of the cardiac cell,followed by the returning of the transmembrane potential towards its resting state.On the contrary, if a sufficiently large stimulus able to rise the transmembrane poten-tial above the threshold potential is applied, an active, non-linear response, knownas the action potential , will be elicited, as illustrated in Fig 1.3. The sharp upstroke(phase 0 ) at the start of the action potential after the supra-threshold stimulus isdue to a rapid inux of sodium ions, creating the sodium current I Na . Throughoutthe whole action potential duration there are potassium-based currents I K that tendto bring the transmembrane potential back to the resting potential, as is for instancethe case of the rapid outward potassium current acting during phase 1. However, inphase 2 the inux of calcium ions in the form of slower inward currents I Ca is able
to compensate potassium currents, creating a relatively at plateau in the actionpotential. In phase 3 the calcium currents cease to hold the membrane potential ina depolarized state and the potassium currents return the cell to the resting state,also known as phase 4.
As it can be also observed in Fig. 1.3, one of the main characteristics of cardiaccells is the beat-to-beat variability in action potential properties, as is for instancethe case of the action potential duration (APD). The inter-beat variation of theseproperties is related to the time needed by the ion channels of the cell membraneto fully recover their resting properties prior to the next excitation. If the diastolicinterval (DI), also known as recovery time and dened as the time between the end of repolarization and the start of the next depolarization of the membrane (see Fig. 1.3),is sufficiently long for the membrane to have fully recovered, it will be followed by
-
8/7/2019 matematyka w kardiologii
15/155
CHAPTER 1. Basics of cardiac electrical activity modeling 7
01530
( A / c m
2 )
0 100 200 300 400 500 600 700 800 900
-80
-60
-40
-20
0
20
V m (
m V )
Istim
time (ms)0 1 2 3 44AP phase
INa ICa
IK
DI APD
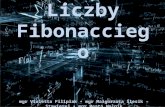
Figure 1.3: Sequence of activations in a model of guinea pig ventricular myocytes.First stimulus illustrates the different phases present in a cardiac action potential,while the second is used to show the dependence of action potential properties, suchas the action potential duration (APD), with respect to the previous diastolic interval(DI). Due to its application during the refractory period of the cell membrane, lastactivation of the sequence fails to elicit a third action potential.
a long APD that is independent of the DI. In contrast, a short DI that only allowspartial recovery will be followed by a short APD. This dependence of the APD onthe DI can be represented in the form of the APD restitution curve , which relatesthe APD at a given point in the tissue with the previous diastolic interval DI at thesame point. Since determining the end of the repolarization is often hard, APDs andDIs are usually measured at a given potential threshold (typically between 80% and95% of repolarization of the transmembrane potential). Other important propertiesof cardiac tissue are also usually presented in the form of restitution curves, as theso-called dispersion or conduction velocity curve, which relates the instantaneousconduction velocity of a plane wave train to the previous DI at the point where thevelocity is measured. See, for instance, Figs. 2.4 or 3.2 for examples of this type of restitution curves.
The existence of an effective refractory period is also of vital importance in thepropagation of cardiac electrical activity. If an action potential is elicited, then a pe-riod ensues during which the membrane cannot be re-excited, the so-called absoluterefractory state . After an interval it becomes possible to raise a new action poten-tial, but it requires an abnormally high stimulus, which characterizes the relativerefractory condition . An illustration of this cellular behavior is shown in Fig. 1.3,where the third stimulus, though equal in amplitude and duration to the previoustwo, fails to elicit an action potential. Refractory periods are hence translated in therestitution curves as the presence of a minimum diastolic interval, DI min , below whichpropagation fails.
-
8/7/2019 matematyka w kardiologii
16/155
8 1.4 Modeling cardiac electrical activity
gKgNa
EKENa
Cm Vm
f o
f i
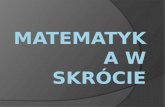
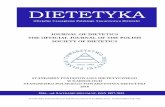
Figure 1.4: Left: Structure of a cellular membrane (taken from Malmivuo and Plon-sey, 1995). The main constituents are two lipid layers, with the hydrophobic tailspointing inside the membrane. The macromolecular pores in the cell membrane formthe ion channels through which ions may ow generating the action potential. Right:Equivalent electric circuit of the cell membrane.
1.4 M ODELING CARDIAC ELECTRICAL ACTIVITY
1.4.1 EQUIVALENT ELECTRIC CIRCUIT OF THE CELL MEMBRANE
The action potential represents changes in the transmembrane potential over timethat are the result of currents owing across the membrane via the movement of ions. Consequently, this type of behavior can be reproduced using a model of the cellmembrane in the form of an equivalent electric circuit.
The cell is enclosed by a cell membrane whose thickness is about 7.5 - 10.0 nm,and is primarily constituted by phosphoglycerides. The head of this molecule ishydrophilic (attracted to water), while the tail consisting of hydrocarbon chains ishydrophobic (repelled by water). When placed in an aqueous medium, the phos-phoglycerides orient themselves conforming a bilayer structure, with the electricallycharged heads in the aqueous solution and the electrically neutral tails lling thespace between, as shown in Fig. 1.4. Thus, the cell membrane behaves like a di-electric, with a measured value of capacitance of about C m = 1 F/ cm2. However,the ion channels allow the ow of current through the cell membrane under certainconditions. Therefore, from an electrical perspective, the cell membrane acts as acapacitance in parallel with a series of resistors representing the ion channels in themembrane. The right panel of Fig. 1.4 illustrates this equivalent circuit.
The total current ow I m through the membrane can be therefore decomposedinto its capacitive I c and ionic I ion components
I m = I c + I ion = C mV mt
+ I ion (1.1)
where the currents through each of the ion channels are summed up to give thenonlinear term I ion which represents the total current owing through the ion channels
I ion =i
I i, (1.2)
-
8/7/2019 matematyka w kardiologii
17/155
CHAPTER 1. Basics of cardiac electrical activity modeling 9
being V m the membrane potential or transmembrane voltage , dened as the potentialat the inner surface ( i) relative to that at the outer surface ( o) of the membrane,i.e., V m = i o. The action potential from a single cell can be then reconstructedby solving the differential equation
V mt
= I ion + I s
C m(1.3)
where I s represents an external stimulus current that may be required for the cell toreach its threshold potential. Consequently, the mission of the modeler is to supplycorrect approximations through the whole range of admissible voltages to each of theionic currents that conform the term I ion .
1.4.2 THE HODGKIN AND HUXLEY FORMALISM
In 1952, Sir Alan Lloyd Hodgkin and Sir Andrew Fielding Huxley presented a paperincluding a quantitative model of membrane currents on giant nerve axons of thesquid (Hodgkin and Huxley, 1952), which constitutes one of the major contributionsof the work for which authors were laureated in 1963 with the Nobel Prize in Physi-ology/Medicine. Although their model describes electrical activity in neural and notcardiac tissue, it elegantly established the basis for mathematically describing ioniccurrents through cell membranes and still forms the cornerstone of our understandingof the electrophysiology and ionic regulation of cells in a multitude of tissue types.
Hodgkin and Huxley performed a series of voltage clamp experiments on giantnerve axons from the squid over a range of voltages, holding constant the voltageand measuring the current ow across the membrane as a function of time. Givenboth the transmembrane potential and the current, Ohms law could be used todeduce the conductance of the cell membrane to certain ions. Not surprisingly, theseconductances turned out to be functions of both the transmembrane potential andtime, and were modeled by the authors in terms of a maximal conductance andvoltage-dependent gating mechanisms, where necessary.
The Hodgkin and Huxley model separates the total ionic current into three com-ponents: a current carried by sodium ions, I Na , a current carried by potassium ions,I K , and a leakage or background current, I L, that is carried by unspecied ions
I ion = I Na + I K + I L (1.4)
each of them given by the following expressions
I Na = gNa m3h(V m E Na ) (1.5a)I K = gK n
4(V m E K) (1.5b)I L = gL(V m E L) (1.5c)
Here, gNa = 120, gK = 36 and gL = 0.3 (mS / cm2) are the maximal conductancesassociated with the sodium, potassium and leakage currents, respectively, while E Na =115, E K = 12 and E L = 10 .613 (mV) are the reversal or equilibrium potentials of each of the ions. Gating variables m, h and n describe the probability that a gate
-
8/7/2019 matematyka w kardiologii
18/155
10 1.4.3 Biophysically-based cardiac ionic models
0 10 20 30 40 50time (ms)
-25
0
25
5075
100
125
P o
t e n
t i a
l ( m V )
0 10 20 30 40 50time (ms)
0
0.2
0.4
0.6
0.8
1
V a
l u e
mhn
Figure 1.5: Left: Transmembrane potential generated by the Hodgkin and Huxley
model. Right: Evolution of gate variables of the model.
will be open to allow the ow of ions under different conditions. For a given gatingvariable y, its time dependence is described in the model as
dydt
= y(1 y) yy (1.6)where y and y variables are known as rate constants and in general are voltage-dependent. Since it represents a probability, the gating variable operates in the [0,1]range, so when y = 0 the gate is completely close and no current will ow, whereasy = 1 the gate is completely open.
The and variables of each gate were appropriately dened as functions of volt-age, and tted in order to obtain as good approximations as possible to experimentallyrecorded data. The same applies to the number of activation and inactivation gatesrequired per ion current. For completeness, the full set of equations of the Hodgkinand Huxley model is given in Appendix A.1. Fig. 1.5 shows the action potentialgenerated by the model, as well as traces in time of its three gate variables.
1.4.3 BIOPHYSICALLY-BASED CARDIAC IONIC MODELS
The Beeler-Reuter model
The rst electrophysiological model for cardiac myocytes using the Hodgkin andHuxley formalism was the one of Noble in 1962 for Purkinje bres in mammals (Noble,1962). However, this model only introduced minor modications to the previouslypresented Hodgkin and Huxley model. In order to show increasing complexity in themodeling of cardiac electrical activity, we choose to mention here instead the 1977Beeler-Reuter model for canine ventricular cells (Beeler and Reuter, 1977).
The total current owing across the membrane was separated in this model infour independent components
I ion = I Na + I s + I K1 + I x1 (1.7)
-
8/7/2019 matematyka w kardiologii
19/155
CHAPTER 1. Basics of cardiac electrical activity modeling 11
0 100 200 300 400time (ms)
-80
-60
-40
-20
0
20
40
P o
t e n
t i a
l ( m V )
0 100 200 300 400time (ms)
0
0.2
0.4
0.6
0.8
1
V a
l u e m
hdf
Figure 1.6: Left: Transmembrane potential generated by the Beeler-Reuter model.
Right: Evolution of selected gate variables of the model.
where the fast inward current I Na is responsible for the quick upstroke of the actionpotential, while the slow inward current I s accounts for the duration of the plateauphase. The other two currents, the time-independent outward potassium current I K1and the time-dependent outward current I x1 , are responsible for the repolarisation of the cell membrane. Expressions of ionic currents, as well as gating rate constants,dened similarly to the Hodgkin and Huxley model, are listed in Appendix A.2.
By the time of publication, it had been already discovered that the intracellular
calcium concentration changed signicantly during the course of an action potential,and therefore it was included in the model as an additional dynamical variable, drivenby the following differential equation
d[Ca2+ ]idt
= 1 107I s + 0 .07(1 107 [Ca2+ ]i), (1.8)
whereas the reversal potential of the slow inward current also depends on the con-centration of calcium ions within the cell
E s = 82.3 13.0287 log [Ca2+ ]i . (1.9)Hence, the Beeler-Reuter model constitutes the rst biophysically-based model which,apart from describing time evolution of the transmembrane potential, also incorpo-rates descriptions for intracellular ion concentrations. This contributes to includedifferent time scales in the solution of the resulting system of differential equations,therefore making models stiffer and computationally more demanding to solve.
Fig. 1.6 shows the transmembrane potential generated by the Beeler-Reuter modelunder a 2 ms excitation of 25 A/ cm2, and the time evolution of a number of its gates.Note how the action potential duration is much longer than in the case of the Hodgkinand Huxley model for the squid axon, and how the four different phases of the cardiacdepolarization and repolarization cycle are present in the voltage trace.
-
8/7/2019 matematyka w kardiologii
20/155
12 1.4.3 Biophysically-based cardiac ionic models
The Luo-Rudy I model
The model introduced in 1991 by Luo and Rudy (Luo and Rudy, 1991), and itsconsecutive actualizations, probably constitutes the most extensively used model in
the eld of computational cardiac electrophysiology. The model, built on the Beeler-Reuter, adjusts parameters and includes additional currents in order to reproducemore accurately recent experimental results, especially on potassium ion dynamics.A total of six individual currents describe the cellular processes
I ion = I Na + I si + I K + I K1 + I Kp + I b (1.10)
where I Na newly accounts for the fast inward sodium current responsible for theaction potential depolarization, I si is a slow inward-calcium related current denedas in the Beeler-Reuter model, whereas I K , I K1 , I Kp and I b respectively representtime-dependent, time-independent, plateau and background potassium currents.
Apart from the number of currents and gating variables (we remind that an or-dinary differential equation in the form of Eq. (1.6) has to be integrated for everyadditional gate), some other factors contribute to make this model slightly more com-plex than the previously mentioned ones. The denition of rate constants for gatevariables constitutes one of these factors. Although we refer to Appendix A.3 for thecomplete set of equations, instead of a single expression being used for the wholerange of admissible voltages, some of the rate constants are approximated in thismodel through piecewise functions dened over different voltage ranges, as it can beobserved here from formulas for the fast inactivation sodium gate h
h = 00.135exp[(80 V m )/ 6.8]
if V m 40 mVif V m < 40 mV(1.11a)
h =1/ (0.13 (1 + exp[(V m + 10 .66)/ 11.1]))3.56 exp[0.079V m ] + 3.1 105 exp[0.35V m ]
if V m 40 mVif V m < 40 mV.
(1.11b)
In addition, the model also introduces the use of new direct voltage gates, whichare direct expressions of voltage that do not follow the standard Hodgkin-Huxleyformalism, such as X i or K p
X i =1.0 if V m 100 mV2.837 exp[0.04(V m + 77)] 1(V m + 77)exp[0.04(V m + 35)] otherwise .
(1.12)
Together with the modications in the denition of gate variables, none of the intra-cellular ion concentrations are kept xed within the sarcolemma 1 . Reversal potentials
1 However, and as already mentioned, it was the Beeler-Reuter the rst model incorporat-ing a description for intracellular concentrations (calcium). The 1985 DiFrancesco-Noble model(DiFrancesco and Noble, 1985) also tracked sodium, calcium and potassium concentration changes.It also incorporated a mechanism for calcium-induced calcium-realease, including in the formulationof the intracellular calcium concentration the concept of additional intracellular compartments, inparticular the sarcoplasmic reticulum which is a store of calcium ions. Ion pumps and exchangeswere also included for the rst time in an ionic model.
-
8/7/2019 matematyka w kardiologii
21/155
CHAPTER 1. Basics of cardiac electrical activity modeling 13
0 100 200 300 400 500time (ms)
-80
-60
-40
-200
20
40
P o
t e n
t i a
l ( m V )
0 100 200 300 400 500time (ms)
0
0.2
0.4
0.6
0.8
1
V a
l u e m
hdf
Figure 1.7: Left: Transmembrane potential generated by the Luo-Rudy I model.
Right: Evolution of selected gate variables of the model.
therefore need to be computed in each iteration depending on the time evolution of these ion concentrations. Several maximal potassium conductances are also expressedas functions of the extracellular concentration of this ion. Fig 1.7 illustrates the actionpotential generated by the Luo-Rudy I model. See Appendix A.3 for the completeset of equations of the model.
Other detailed ionic models
For each of the different cell types existing in the heart, including the sinoatrial node,Purkinje bers, ventricles and atria, new ionic models are continuously appearingadding additional currents and increasing complexity as more is understood aboutthe dynamics of cardiac processes. For instance, the Noble et al. (1998) model in-corporates features such as cellular mechanics, metabolism, pH dependence or drugreceptor interactions. Although not described in detail here (we refer the reader tothe original publications), some of these biophysically-based detailed ionic models areused in forthcoming chapters of the present work (Luo and Rudy, 1994; Nygren et al. ,1998; Priebe and Beuckelmann, 1998; Miyoshi et al., 2003; Ten Tusscher et al. , 2004;Iyer et al. , 2004), even incorporating descriptions of cellular processes at the proteinlevel (Clancy and Rudy, 2002). See Pullan et al. (2005) for a list of cardiac cellularmodels gathered from the literature.
1.4.4 SIMPLIFIED MODELS OF CARDIAC ELECTRICAL ACTIVITY
Despite the fact that detailed biophysically-based models denitely provide very goodapproximations to the experimental data sets they are based on, a number of openquestions still remain unanswered about their validation. This might be for instancethe case of assessing which are the actual effects of temperature on the experimentaldata sets that are used to build the models. Although it is known that some ionicmechanisms responsible for certain diseases are temperature dependent and may notmanifest at low temperatures (Dumaine et al., 1999), most ionic currents are usu-
-
8/7/2019 matematyka w kardiologii
22/155
14 1.4.4 Simplied models of cardiac electrical activity
ally measured in experiments at room temperature. These temperature differencesbetween nominal room temperature, normal body temperature, and temperaturesreported for various experimental circumstances, can be therefore sufficient to pro-duce noticeable and sometimes pronounced differences in the ionic currents that themodel tries to replicate. The same applies to gender or age considerations, since forexample it is known that some ionic currents are considerably different in male andfemale individuals of the same specie (Di Diego et al., 2002; Kimura et al. , 2004).
Other issue that should be taken into account is the use of channel and ion block-ers. In order to separate the different ionic currents owing through the cell mem-brane, often the cell preparations involve the use of chemical or pharmacologicalagents to control or block the effect of a particular channel or ion so that anothercan be studied. The use of such blockers can have in principle multiple side effectswhich can be difficult to evaluate, since under normal physiological conditions noneof these channels is blocked and different types of interactions between ions mightbe therefore masked and not considered throughout the modeling process. It is alsoof importance to note that another limitation of channel-by-channel model construc-tion is that the relative contributions of the channels generally are not assessed bymeasuring channel densities. So each current is reproduced as well as possible, butthe channel densities are varied at will in a non-quantitative process to balance thecurrents and reproduce the desired action potential shape.
Another relevant point concerning detailed ionic models is the role of intracellularcalcium handling, a regulatory process of high complexity and with important effectson cellular dynamics since it constitutes the link between electrical activation andmuscle contraction. Much is still not known about intracellular calcium processes,constituting an area of vigorous debate and resulting in a variety of detailed ionicmodels which use completely different formulations for the intracellular calcium cy-cle (DiFrancesco and Noble, 1985; Luo and Rudy, 1994; Noble et al., 1998; Shiferawet al., 2003). Besides, there are a lot of largely uncharacterized differences in cal-cium handling among atrial, ventricular, and Purkinje cells, and also among differentspecies. Because calcium can have such a huge effect in cell dynamics, this unknownis highly signicant. In addition, it is not hard to nd models whose componentsare derived from data coming from a wide variety of different species, or which usedescriptions of ionic currents and cellular compartments formulated for other typesof cells, even with different embryological development. Besides, and despite these
models claim to be detailed, in some situations the available data sets are so reducedthat the selection of mathematical interpolants to t the data is absolutely arbitrary.
The aim of the previous comments is not in absolute to try to rise doubts onthe utility of mathematical modeling as a practical tool in cardiac electrophysiology,but just to expose that, primarily for the own nature of the process under modeling,models are necessarily imperfect and none can be trusted as absolutely correct. In-deed, an increase on model complexity is not always reected into an improvementin its predictive accuracy. As more and more ionic currents, cellular compartmentsand features of the cardiac beat are incorporated into the models, more factors even-tually become susceptible to failure and the models themselves become increasinglymore difficult to implement, understand, and use. At present, this is for instance thecase of baseline drift in several last-generation models, where transmembrane voltage
-
8/7/2019 matematyka w kardiologii
23/155
CHAPTER 1. Basics of cardiac electrical activity modeling 15
0 200 400 600 800time (ms)
-0.2
0
0.2
0.4
0.6
0.8
1
P o
t e n
t i a l
0 200 400 600 800time (ms)
0
0.2
0.4
0.6
0.8
1
V a
l u e
v
Figure 1.8: Left: Transmembrane potential generated by the FitzHugh-Nagumo
model. Model parameters are c1 = 0 .175, c2 = 0 .03, = 0 .1, b = 0 .011, andd = 0 .55. Right: Evolution of the gate variable of the model.
and/or some ionic concentrations slowly drift until they are out of the physiologicalrange if the model is left running for a long period of time.
Since it seems highly plausible that detailed models will continue incorporatingdata from even smaller time and space scales, cell equations will unequivocally becomeeven more difficult, stiffer, and time-consuming to solve. This complexity inherentto detailed ionic models makes their analytical treatment impossible and simulations
highly costly, actually currently impossible in three dimensions if the most sophisti-cated models want to be used. In some situations however, and depending on theproblem under study, it is not necessary to model all sub-cellular processes of the car-diac myocyte. For this reason, and with a view placed on investigating phenomenaon larger spatial and temporal scales, several simplied models have been developedwith the intention of providing an action potential at a minimal computational cost.
The FitzHugh-Nagumo model
The simplied model most extensively used in the literature, both theoretically andcomputationally, is probably the FitzHugh-Nagumo model (FitzHugh, 1961; Nagumoet al. , 1962). Despite the model simplicity, which has just two variables and a cubicnonlinearity
dudt
= c1u(u )(u 1) c2v (1.13a)dvdt
= b(u dv) (1.13b)where u is a normalized potential and , b, d, c1 and c2 are model parameters, it isable to capture the most basic features of excitable media, such as the generation andpropagation of action potentials (see Fig. 1.8). However, the model fails to reproducethe form of action potentials in real cardiac tissue, where the time scales of depolar-ization and repolarization are signicantly different. Furthermore, the propagation of
-
8/7/2019 matematyka w kardiologii
24/155
16 1.4.4 Simplied models of cardiac electrical activity
wave trains in the FitzHugh-Nagumo model is qualitatively contradictory with whatis found in cardiac tissue, where restitution phenomena are strong promoting instabil-ity at small diastolic intervals, and where conduction velocity dispersion is weak, withwave speed practically insensitive to the postrepolarization state of the medium. Inaddition, the FitzHugh-Nagumo action potential shows a nal hyperpolarizing phase,something observed in neural but not in cardiac tissue.
In an attempt to overcome these limitations without having to resort to a fullphysiological modeling perspective, some modications have been proposed to theFitzHugh-Nagumo equations. The hyperpolarizing phase of the FitzHugh-Nagumoaction potential can be easily eliminated making use of slightly different equations 2(Rogers and McCulloch, 1994), and the model can be also modied to capture therestitution and dispersion properties of cardiac tissue, as shown in Aliev and Panlov(1996). There also exists a wide bibliography on FitzHugh-Nagumo-based models,which include for instance the Van Capelle and Durrer (1980), Barkley (1991) orKarma (1994) models, to cite some.
Even though the great efforts placed on the improvement of this type of models,and the numerous advancements obtained thanks to their use in the understandingof excitable media, FitzHugh-Nagumo-like models are still mere caricatures of realcardiac tissue. This has motivated the development of other simplied models, as theone presented next, which explicitly try to reproduce some basic ionic properties of cardiac tissue.
The three-variables simplied ionic model
The three-variables (3V) simplied ionic model was introduced in 1998 by Fentonand Karma (Fenton and Karma, 1998). The model can be seen as a simplicationof the Luo-Rudy I model of the cardiac membrane, but it is still complex enough toexhibit many of the characteristics of heart cells. It only includes three currents
I ion = I + I so + I si (1.14)
that represent the ows of total sodium, total potassium and total calcium ionsthrough the cell membrane, but that have been deliberately called the fast inward,I , slow outward, I so , and slow inward, I si , currents, respectively, to emphasize thelack of a physiological basis for these currents
I = pv d
(1 u)(u uc) (1.15a)I so = (1 p)
u 0
+ p1 r
(1.15b)
I si = w
2 si1 + tanh k(u usic ) . (1.15c)
As in the FitzHugh-Nagumo model, u is a normalized potential, while the gates
2 Just by multiplying the term c2 v of Eq. (1.13a) by the normalized transmembrane potential,i.e., dudt = c1 u(u )(u 1) c2 uv.
-
8/7/2019 matematyka w kardiologii
25/155
CHAPTER 1. Basics of cardiac electrical activity modeling 17
0 100 200 300 400 500time (ms)
0
0.4
0.8
1.2
P o
t e n
t i a l
0 100 200 300 400 500time (ms)
0
0.2
0.4
0.6
0.8
1
V a
l u e v
w
Figure 1.9: Left: Transmembrane potential generated by the 3V model. Model
parameters according to set BR of Fenton and Karma (1998). Right: Evolution of gate variables of the model.
v and w, which control the inward currents, are driven by the differential equations
dvdt
= (1 p)1 v
v pv
+v(1.16a)
dwdt
= (1 p)1 w
w pw +w
(1.16b)
where p and q are step (Heaviside) functions depending on voltage
p =0, u < u c1, u uc
q =0, u < u v1, u uv
(1.17)
All model parameters are constants, with the only exception of v , which is denedpiecewise as
v = q v1 + (1 q) v2 (1.18)in order to better approximate the minimum diastolic interval of the tissue. Theset of model parameters can be tted to replicate accurately the properties anddynamics of other complex ionic models, including action potential duration andconduction velocity restitution curves, thresholds for excitation, upstroke velocities,and minimum APDs and DIs for propagation, as well as experimental data (Fentonand Karma, 1998; Fenton et al., 2002). Fig. 1.9 shows the 3V model reproducingthe dynamics of the Beeler-Reuter model, according to model parameters taken from(Fenton and Karma, 1998). As it can be observed from comparison with Fig. 1.6,the duration of the electrical activation is the same in both models. However, thesimplied model fails to approximate correctly the shape of the action potential,which is actually a highly important electrophysiological factor in many problems of interest, such as the accurate reconstruction of the electrocardiogram waveform orthe clinical explanation of many life-threatening pathologies. Another disadvantage
-
8/7/2019 matematyka w kardiologii
26/155
18 1.5 Propagation of cardiac electrical activity
Im
Ia
r
l dx
Ia(x) Ia(x+dx)
Im
Figure 1.10: Schematic representation of a cylindrical cell in order to study voltagepropagation in excitable tissue.
of the 3V model versus detailed models is that it is more complicated to assess effectsof specic channel blockade. Nevertheless both limitations can be overcome, and
most of this thesis results are based on the use of an improved version of this model.
1.5 P ROPAGATION OF CARDIAC ELECTRICAL ACTIVITY
The cardiac myocardium is in essence a discontinuous tissue, where cardiac cells joinend-to-end with other cells through intercalated disks. Electrical connection betweencells is only given through specialized gap junctions , that are located in these disks.Despite this non-uniform structure, the approach used here to modeling the propaga-tion of electrical activity in the heart is that of continuum-based modeling, where themedium is treated as continuous using volume-averaged quantities. These volumes
are small compared to the lengths that we are interested in, but large enough toencapsulate a statistically representative region of the medium. One of the featuresof this continuum-based modeling is that it allows the application of different mathe-matical operators to the eld variables, such as spatial differentiation, something notreadily applicable at the atomic or molecular scales.
1.5.1 THE MONODOMAIN EQUATIONS
To study electrical propagation in cardiac tissue, we consider a tissue cable madeup of cylindrical cells where current may ow along and across the membrane (seeFig. 1.10). The cable is excited on its left side, and we examine electrical propagation
across the differential of volume shown in the right panel of the same gure. By ap-plication of conservation of charge, variation in the axial current along the differentialof volume has to equal the current ow across the membrane
[I a (x + dx) I a (x)] r 2i ax
dx r 2 = I m 2rdx (1.19)According to Ohms law, the ow of current along the cable is proportional to thevoltage gradient
V mx
= ia (1.20)where is the resistivity of the cardiac ber and the negative sign ensures that thecurrent is owing in the direction specied in Fig. 1.10. If we recover the previous
-
8/7/2019 matematyka w kardiologii
27/155
CHAPTER 1. Basics of cardiac electrical activity modeling 19
results presented in Sec. 1.4.1, the total current owing across the membrane can bedecomposed into the currents produced by the ux of ions through the ion channels,I ion , and the capacitive current I c arising from the dielectric behavior of the membrane
I m = C m V mt+ I ion (1.21)
Finally, combining Eqs. (1.19)-(1.21), we obtain the so-called cable equation , used todescribe voltage propagation along a one-dimensional cable
V mt
=1
C m 2V mx 2
I ionC m
= D 2V mx 2
I ionC m
(1.22)
where is the membrane surface to volume ratio of the cell, which in the simplest caseof a cylindrical myocyte is given by = (2 rl )/ (r 2l) = 2 /r , and D = 1 / (C m ) 1 cm2/ s is known as the diffusion coefficient of the tissue. In multiple dimensions,the diffusive term is replaced by (D (x)V m ), where is the gradient operator,and D (x) is the diffusion tensor, which encapsulates the diffusion coefficients in eachof the spatial directions and that may depend indeed on the spatial coordinates. Thisleads to write Eq. (1.22) in the form
t V m = (D (x)V m ) I ion (V m , y)/C m (1.23a) t y = g(V m , y ) (1.23b)
where it has been explicitly indicated that the equation of voltage propagation has
to be solved in conjunction with the ionic model which gives description for the termI ion , being y a vector containing the whole set of gating variables used to describethe dynamics of the cellular membrane.
Boundary conditions have to be specied for the solution of Eq. (1.23a). It isobvious that in the real heart a fraction of the total electrical current has to leavethe organ and propagate through the thorax, since it can be registered on the bodysurface in the usual form of a clinical electrocardiogram. However, this fraction of current is considerably small when compared to the total current sustained by theheart. If we are only interested on electrical propagation within the cardiac muscle,a good approximation to the total picture is to neglect this outgoing fraction of current and consider the organ as electrically insulated, therefore imposing zero-ux(homogeneous Neumann) boundary conditions to the problem. In fact, many clinicalexperiments are done indeed using insulated pieces of cardiac tissue.
If different conduction properties had been assumed for both the intracellular andextracellular spaces, a more challenging model consisting of a system of two coupledpartial differential equations, and known as the bidomain model , is obtained to de-scribe the evolution of the intracellular and extracellular potential elds. Althoughsuch a bidomain model is required in some situations of study, such as debrillation,its use is not necessary for the achievement of the results exposed in the present dis-sertation. Eqs. (1.23) can be also derived from the bidomain model assuming equalconductivity tensors for both the intracellular and extracellular media, reason whythey are also widely known as the monodomain model or monodomain equations of cardiac electrical activity propagation.
-
8/7/2019 matematyka w kardiologii
28/155
20 1.5.2 Planar and spiral waves in cardiac tissue
Cable Length
Time
Cable Length
Time
Figure 1.11: Left: Propagation of a wave of electrical activation in a one-dimensionaltissue cable excited in its left side. The Beeler-Reuter model is used to describe cel-
lular dynamics. Right: Collision and subsequent annihilation of two action potentialwaves propagating in opposite directions.
1.5.2 PLANAR AND SPIRAL WAVES IN CARDIAC TISSUE
Due to the presence of the Laplacian operator, Eqs. (1.23) are essentially of thereaction-diffusion type. Interestingly, and even though they are essentially parabolicand therefore dissipative in nature, they allow unattenuated wave propagation (seeFig. 1.11). These waves are however distinctly different from those typically appear-ing in hyperbolic systems. When two action potentials waves meet head-on, theyannihilate, rather than pass through each other (Fig. 1.11, right). Also, when anaction potential encounters the edge of a system, it is annihilated instead of reected.
As it was explained in Sec. 1.3.1, normal cardiac rhythm is associated to theperiodic activation of the heart, which after starting in the sinoatrial node, rst excitesthe atria, propagating next through the ventricles in the form of a planar wave. Anyabnormal conduction of this excitation pulse can give rise to rapid rhythms calledtachycardias. One mechanism for the generation of tachycardias is reentry , which isrelated to solutions to the reaction-diffusion system given by Eqs. (1.23) in the formof spiral waves patterns. These rotating spiral waves have been observed in livingcardiac tissue (Downar et al., 1988; Frazier et al. , 1988; Davidenko et al., 1992; Grayet al., 1998; Witkowski et al., 1998; Emov et al. , 1999), after having been predictedbased on theoretical models (Moe et al., 1964; Winfree, 1980).
Different types of reentry can be distinguished. Anatomical reentry often occursfollowing a myocardial infarction, event where, due to the obstruction of one of thecoronary arteries, a portion of cardiac tissue dies from oxygen deprivation and formsa scar of nonconducting tissue. Under the appropriate conditions, the interaction of a wave front with this anatomical obstacle can lead to fragmentation of the wavefront and to spiral wave formation. Alternatively, reentry can occur in the absenceof a physical obstacle supporting the core of the spiral, what is known as functional reentry . Fig. 1.12 shows the generation of a spiral wave in a perfectly homogeneoussheet of cardiac isotropic tissue (Davidenko et al., 1992; Wohlfart and Ohlen, 1999;Otani, 2000). A planar action potential wave propagates upwards in the piece of
-
8/7/2019 matematyka w kardiologii
29/155
CHAPTER 1. Basics of cardiac electrical activity modeling 21
A
C
B
D
Figure 1.12: Creation of a spiral wave in the 3V model by ectopic activation inthe wake of a preceding wave. Model reproduces modied Beeler-Reuter dynamics
according to parameter set taken from Fenton and Karma (1998). (A) While theinitial excitation wave is moving upwards, an ectopic activation occurs in its wake(arrows indicate directions of movement). (B) Initially, the second activation wavecan only propagate sideward, since cells above it have just been excited and are stillrefractory. (C) As the second wave moves rightward, cells above it start recoveringexcitability, what allows the wavefront to curve. (D) Evolution of the self-maintainedwave in the tissue.
tissue, leaving behind a wake of refractory tissue which can not be re-excited imme-diately. Just behind this wave, a group of cells res abnormally, something that isknown to happen in some situations in the heart. Due to the recent passage of theoriginal action potential wave, the portion of the tissue above this abnormal ringregion is still in the refractory state. Therefore, the abnormal cell group excites awave which can only propagate sideward. Soon, however, the rightward propagatingwave nds that the cells above it are no longer refractory, initiating a curved upwardpropagation which ultimately yields the formation of the spiral wave pattern.
Spiral waves can endure in tissue as persistent sources of electrical activation.The period of rotation of these spirals is normally faster than the normal periodof excitation of the hearts natural peacemaker (the sinoatrial node), leading to theacceleration of the cardiac rhythm associated with a tachycardia. Analogously, spiralwave breakup in multiple unorganized wavefronts (Winfree, 1991; B ar and Eiswirth,
-
8/7/2019 matematyka w kardiologii
30/155
22 1.6 Numerical solution of cardiac tissue models
Figure 1.13: Top row of the panel: Artifactual breakup in the 3V model due to coarsediscretization. Simulation done with x = 0 .025 cm, t = 0 .40 ms. Bottom rowof the panel: same simulation with x = 0 .025 cm, t = 0 .35 ms. The model isintegrated in both cases using nite differences in space and implicit integration intime. See text for details.
1993; Karma, 1994; Fenton and Karma, 1998; Fenton et al. , 2002) is believed to belinked to cardiac brillation , situation where the hearts electro-mechanical functionis completely impaired and the muscle becomes unable to pump blood throughoutthe body. See, for instance, the paper of Fenton et al. (2002) for a complete reviewon multiple mechanisms which can lead to cardiac rhythm degeneration into thispotentially fatal form of irregular activity.
1.6 N UMERICAL SOLUTION OF CARDIAC TISSUE MODELS
One basic problem in numerical cardiac tissue simulations is that the propagatingwaves of electrical activity involve very disparate time and space scales. The timescale of the rapid excitation upstroke (
3 ms) is two orders of magnitude faster
than the time scale of recovery (300 ms). Similarly, cardiac tissue simulationsconstitute a family of spatially extended systems where the size of the domain of interest is in general several orders of magnitude larger than the space scale of theactivation front. The presence of such uneven scales in the solutions to the problemmakes mandatory the use of small time and space steps in order to correctly resolvethe activation front. The need of numerical accuracy is actually critical in this typeof studies since multiple physical mechanisms (including ber anisotropy, recovery of the tissue, hysteresis, etc) are known to play a pivotal role in the development of spiralwave breakup (Fenton et al., 2002), and thus computer simulations of cardiac tissuemodels are required to be computed with sufficiently high spatiotemporal resolutionin order to separate the effect of these factors from possible artifactual breakups of
-
8/7/2019 matematyka w kardiologii
31/155
CHAPTER 1. Basics of cardiac electrical activity modeling 23
the solution due to the use of a excessively coarse discretization. As illustration, suchan artifactual breakup is shown in Fig. 1.13 for one of the models of study. Thiseffect can occur for large time and/or space steps t and x regardless of method.
Two different approaches to face simulation can be distinguished in the eld of computational electrophysiology. The rst group of researchers is formed by thosewho are more interested in the answer than the technique. People in this groupwant to get an answer as quickly and as easily as possible, and so use well known,reliable, readily implemented numerical schemes. Unfortunately, these easy methodsare relatively slow and cannot be used for large problems. This situation arises forinstance using nite differences to discretize the spatial derivatives in conjunctionwith low-order explicit integrators as the Euler method to time step the solution.Though these schemes have provided useful insight in many cases, the low-order of spatial derivatives imposes the use of excessively ne grids, whilst stability restrictionsseverely constraint the range of admissible time steps, thus making prohibitive thesolution of large problems both in terms of memory requirements and computationalefficiency.
As a result, the second group of researchers includes those who expend signi-cant efforts to develop complicated, hopefully better, numerical algorithms. Thesemethods include temporal and spatial adaptation, parallelism, and so on (Quan et al. ,1998; Cherry et al., 2000; Yu, 2001; Buist et al., 2003; Cherry et al., 2003; Pennacchio,2004; Trangenstein and Kim, 2004; Colli Franzone et al., 2006). The disadvantage of these methods is that it is not a simple matter for the people in the rst group to gearup to use or implement the sophisticated methods developed by the second group,nor is it obvious which direction to pursue, since different methods have different
advantages and disadvantages.Hence, an ideal equilibrium would be the use of numerical stencils featuring better
convergence properties than the methods of the rst group, but with a much easierimplementation that the algorithms of the latter. Among the different possibilities,spectral methods can be one of these possible alternatives.
1.7 S PECTRALLY ACCURATE METHODS
Spectral methods are a class of spatial discretizations for partial differential equations,characterized for providing very accurate approximations of sufficiently smooth solu-tions (Gottlieb and Orszag, 1977; Canuto et al. , 1988; Sanz-Serna, 1995; Fornberg,1996; Trefethen, 2000). Because of their high-order accuracy properties, they havebecome widespread over the last decades in various elds, including uid dynamics,quantum mechanics, heat conduction, or weather prediction (Canuto et al., 1988;Iliev et al., 1994; Ben-Yu, 1998; Peyret, 2002).
One of the key components for the formulation of spectral methods are the trial functions (also called the expansion or approximating functions), which are linearcombinations of suitable basis functions, used to provide the approximate represen-tation of the solution. The choice of these functions is one of the features that dis-tinguishes spectral methods from nite-element and nite-difference methods. Thetrial basis functions for a spectral method are global, innitely differentiable, and
-
8/7/2019 matematyka w kardiologii
32/155
24 1.7 Spectrally accurate methods
nearly orthogonal. In contrast, in nite-elements or nite-differences methods, trialfunctions are chosen to be local, low-order, non innitely differentiable functions.
This difference can be illustrated as follows. Let for instance {x1, . . . , x n}denotea uniform grid, with x j +1
x j = h for each j , and consider a set of corresponding datavalues {u1, . . . , u n}. Then, the unique local polynomial p j of degree 2 satisfying p j (x j1) = u j1, p j (x j ) = u j , and p j (x j +1 ) = u j +1 is given by
p j (x) = u j1a1(x) + u j a0(x) + u j +1 a1(x) (1.24)
where a1(x) = ( x x j )(x x j +1 )/ 2h2, a0(x) = (x x j1)(x x j +1 )/h 2, anda1(x) = ( x x j1)(x x j )/ 2h2. Differentiating once the interpolant and evaluatingat x = x j then givesu(x j )
u j +1 u j12h
(1.25)
which is the standard second-order nite difference approximation of the rst deriva-tive of u at x j . On the contrary, and instead of only using the information of neigh-boring points to compute the spatial derivatives, the idea under spectral methods isto build a global interpolant I (x) through all nodal values u j
I (x) =N 1
k=0
akk(x), (1.26)
and to compute the derivatives of u as the derivatives of this interpolant, where theset {k(x)}represents the set of trial functions used in the spectral method to expandthe approximate solution to the partial differential equation.
Among all possible bases, the most frequently used trial functions are trigono-metric polynomials, Chebyshev polynomials, or Legendre polynomials. In the case of trigonometric polynomials (similar results can be obtained for the other bases), co-efficients ak of expansion (1.26) are related to the Fourier coefficients of the functionto approximate. For a sufficiently smooth function, its associated Fourier coefficientsare rapidly decaying with wavenumber. The reason is that a smooth function changesslowly, and since high wavenumbers correspond to rapidly oscillating waves, such afunction contains little energy at high wavenumbers. If this is satised, then theerrors introduced by discretization are small, since these errors are caused by thealiasing of high wavenumbers to low wavenumbers.
As a result, the truncated series of a sufficiently smooth function converges fasterthan any nite power of 1 /N . This property, oftenly referred to as spectral conver-gence, can be observed in Fig. 1.14. In this gure, errors in the L2-norm are shownfor the computation of the second derivative of the function
f (x) = tanh kx
1 x2, x[1, 1] (1.27)
where a hyperbolic-tangent function has been chosen in order to replicate the sharpactivation front of the cardiac action potential prole. The weight 1 / 1 x2 isincluded to guarantee that the argument varies from
to
as x ranges from
-1 to 1, therefore assuring zero derivative of function f at x = 1, hence agree-ing with the boundary conditions we are interested in for the numerical solution of
-
8/7/2019 matematyka w kardiologii
33/155
CHAPTER 1. Basics of cardiac electrical activity modeling 25
101
102
10310
12
1010
108
106
104
10 2
100
102
N
e r r o r
i n s e c o n
d d e r i v a t
i v e N2
101
102
10310
8
106
104
102
100
102
N
e r r o r
i n s e c o n
d d e r i v a t
i v e
N2
Figure 1.14: Convergence results in L2-norm in the computation of the second deriva-tive of the hyperbolic-tangent prole given by Eq. (1.27), using a Fourier spectralmethod in a cosines basis (red triangles) and standard centered second-order nitedifferences (black circles), for k = 10 (left) and k = 50 (right).
Eqs. (1.23). For comparison, convergence results of a Fourier spectral method arepresented against results for a standard second order nite-differences method. Thesharpness of the hyperbolic-tangent prole is dramatically accentuated as parameterk is increased, what obviously affects to the convergence properties of both methods.However, in all situations the spectral stencil proves to be more accurate than thelow order scheme. Indeed, much more favorable results would have been obtained if a smoother function, rather than a shock like prole, had been used.
Despite their higher order of convergence, little use of spectral methods has beenmade in the discipline of cardiac computational electrophysiology. The only publica-tions that can be found in the literature are the work of Trayanova and Pilkington(1993), where a Fourier spectral method is used for solving the bidomain model, andthe papers of Zhan and Ng (2000) and Ng and Yan (2003), involving mapped Cheby-shev methods in the solution of the monodomain equations coupled to the Luo-Rudy Imodel. Nevertheless, there exists some complementary bibliography making use of these methods for closely related studies in excitable media and reaction-diffusionsystems (see, for instance, the work of Bayliss et al., 1989; Karma, 1990; Ruuth,1995; Jones and OBrien, 1996; Yagisita et al., 1998). In any case, the absence of spectral schemes in the eld should be assessed more to a possible unawareness of these numerical techniques rather than to difficulties in their implementation. In fact,in some situations the development of a spectral method can be even easier than, orat least as easy as, the coding of a nite difference scheme.
Finally, some of the spectral methods considered in this thesis are referred to aspseudospectral . This term alludes to that the numerical stencil is based on collocation,i.e., pointwise evaluations in which the strong formulation of the partial differential
-
8/7/2019 matematyka w kardiologii
34/155
26 1.8 Thesis summary
equation is required to be satised exactly at a special set of points, the so-calledcollocation points. This is contrary to the case of a Galerkin approach, where thedifferential equation is enforced by requiring that the integral of the residual times aproperly chosen set of test functions (which can be equal or different to the basis of trial functions) to be zero, accounting in the process after some integration by partsfor any remaining boundary conditions. In other words, when the partial differentialequation is written in terms of the coefficients of the expansion, the method is saidto be a Galerkin spectral method, whereas if it is written in terms of nodal values,the method is referred as pseudospectral.
1.8 T HESIS SUMMARY
The present manuscript is divided into two main parts. The use and applications
of simplied ionic models in the study of cardiac processes is considered in the rstpart of the thesis, while the second part is primarily devoted to the use of spectralmethods for the numerical simulation of the reaction-diffusion equations that arise incardiac modeling, as well as the extension of these numerical methods to their use inirregular domains.
In chapter 2 we investigate the use of mathematical modeling to simulate theelectrical activity of the human heart ventricles. In the last years, more and morecardiac models are continuous and incessantly appearing as more aspects of the un-derlying cardiac processes are unraveled. This rise in the number of cell models hasbeen especially remarkable for several animal species, including rabbit, guinea pig,
swine, rat, or dog. Surprisingly, only three models have been published to reproducethe electrical behavior of the human ventricles (Priebe and Beuckelmann, 1998; Iyeret al., 2004; Ten Tusscher et al., 2004), and to date the dynamics of the three of themhave not even been carefully compared. In this chapter, reentry dynamics for all pre-viously existing human ventricular models are simulated for the rst time in tissue.The chapter is completed with the presentation of a new ionic model which, despiteof being designed to remain as simple as possible, is able to reproduce all importantelectrophysiological properties of the human cardiac myocytes while outperformingthe other models in several orders of magnitude in terms of computational efficiency.In addition, and contrary to what happens with some of the previous models, thenew model contains descriptions for human epicardial, endocardial and midmyocar-dial cells, which represent the three main categories of ventricular myocytes. Wevalidate the model against the available experimental data, including action poten-tial shape, action potential duration restitution, conduction velocity restitution, aswell as other important quantities of relevance in electrophysiology which are knownto be different between the three types of cells.
The usefulness of the new model is demonstrated in chapter 3 by addressing thecharacterization and study of an important hereditary genetic disease: the Brugadasyndrome (Brugada and Brugada, 1992, 1997; Brugada et al., 1998). This diseaseis estimated to cause 4-12% of all sudden cardiac deaths in humans, primarily thoserelated to patients without identiable structural abnormalities. Contrary to manyother cardiac disorders, whose clinical manifestations and life-threatening risks areenhanced at fast pacing or high mechanical loads, such as during intense physical
-
8/7/2019 matematyka w kardiologii
35/155
CHAPTER 1. Basics of cardiac electrical activity modeling 27
activity, interestingly the Brugada syndrome primarily manifests at rest causing thedeath of patients during sleeping (Nademanee et al. , 1997; Vatta et al., 2002). Al-though several authors have provided experimental evidences for the different ionicmechanisms that are thought to underlie the disease (Yan and Antzelevitch, 1999;Antzelevitch, 2001), only two previous in silico studies about Brugada syndrome canbe found in the literature (Clancy and Rudy, 2002; Miyoshi et al., 2003). However,none of these models do completely describe the disease, and hence our model is usedto try to gain further insights into all possible factors which might play an active rolein the spontaneous triggering of arrhythmias in this life-threatening disorder.
Efficient techniques for the numerical resolution of the partial differential equa-tions that describe electrical activity propagation in cardiac tissue are presented inchapter 4 . Since solutions to these equations are characterized by the presence of very disparate time and space scales and very steep activation fronts, it is henceclear that the optimal choice of solvers for this type of systems would be the use of numerical methods able to feature both time and space adaptability (Cherry et al. ,2000; Yu, 2001; Cherry et al. , 2003; Colli Franzone et al. , 2006). However, seriousdifficulties in implementation make the coding of these applications a costly task,with development times that can range even in the scale of years. Thus, and with anespecial emphasis placed on the ease of implementation, we focus here on the study of different numerical algorithms that, despite not featuring spatial adaptability, couldyield a reduction of the number of required discretization points and shorter executiontimes. Therefore, and although we do not expect a priori such a huge reduction in thenumber of mesh points as in the case of other problems characterized by smootherspatiotemporal behaviors, we carry out in this chapter a complete study on the appli-cability of high-order methods for our problem of interest, proving how the spectralmodeling of cardiac tissue propagation is not only advantageous in terms of mem-ory requirements but also computationally efficient relative to execution times. Thisalso includes for the rst time the coupling of a detailed second-generation model of the cardiac cellular membrane (Nygren et al., 1998) to suitable implementations of pseudospectral and Galerkin spectral schemes.
In chapter 5 we present a novel approach to overcome the biggest limitation of numerical simulation using classical spectral methods: their applicability to irregu-larly shaped domains. The high order of these methods is based on the use of globalrather than local interpolants in order to approximate the solution to the partialdifferential equation to solve. These interpolants are expanded in an appropriate or-thonormal basis, properly selected to describe the geometry of interest. Hence, it isclear that is not easy to dene such a interpolating basis if our integration domainis irregularly shaped. We solve the problem by extending the irregular domain of interest into a rectangular geometry by means of what is generally called a ctitiousdomain or domain embedding method (Buzbee et al., 1971; Elghaoui and Pasquetti,1996; Angot et al., 1999; Glowinski et al. , 1999). Even in the presence of irregularboundaries or holes within the integration domain, the resulting numerical approach,called the Spectral Smoothed Boundary method, is proved to still retain for ourproblem of interest the same convergence properties previously observed in regulardomains for spectral methods over low-order schemes. Hence, our work constitutesthe rst study in which purely spectral methods have been used to obtain solutions
-
8/7/2019 matematyka w kardiologii
36/155
28 1.8 Thesis summary
of evolution problems described by partial differential equations in this type of com-plicated, irregularly shaped geometries. The results obtained here may also apply toa number of other excitable systems with similar properties.
Portions of the methodology developed for the Spectral Smoothed Boundarymethod can be also employed to further develop other early proposed numericalschemes, as is demonstrated in chapter 6 for the case of mixed spectral/boundaryelement methods for the solution of partial differential equations of elliptic type (El-ghaoui and Pasquetti, 1996, 1999). The critical part of these methods is the extensionof the inhomogeneous term of the partial differential equation to the regular geome-try in which the domain of interest is embedded. We prove here how our smoothedboundary approach satisfy the same properties that other explicit extensions given inthe literature (Boyd, 2002, 2005), but exhibiting a number of additional advantageswhich allows to extend its applicability to any type of irregular domain.
-
8/7/2019 matematyka w kardiologii
37/155
Part I
Simplied mathematical modeling of human ventricular action potentials
-
8/7/2019 matematyka w kardiologii
38/155
-
8/7/2019 matematyka w kardiologii
39/155
Chapter 2Minimal model for human ventricularaction potentials in tissue
2.1 I NTRODUCTION
Modeling the dynamics of wave propagation in human ventricular tissue
and studying their relation to cardiac arrhythmias requires the use of specic ionic models, capable not only of reproducing key characteristicsat single cell level, such as rate dependencies of human action potential
duration (Franz et al., 1983, 1988), but also other tissue-level properties, such as ratedependence of conduction velocity, wave curvature, minimum rate for conductionblock, or action potential morphologies. Tissue characteristics like these are impor-tant since they have been shown to affect the initiation, dynamics and stability of reentrant waves (Banville and Gray, 2002; Fenton et al., 2002; Cherry and Fenton,2004). In addition, it is desirable to have models that: (i) can be easily congured toreproduce these experimentally measured tissue characteristics from various regionsof normal and diseased ventricles, (ii) are relatively fast to compute, and (iii) retainenough complexity to reproduce tissue behavior accurately while remaining simpleenough to gain insights into the parameters responsible for what is observed.
To date, only three different ionic models have been developed to reproduce humanventricular cell dynamics. The Priebe and Beuckelmann (1998) model, which consistsof 22 variables, was developed to study the cellular electrophysiological consequencesof heart failure and abnormal automaticity. This model was derived from the LR-IImodel, with only ve of the ionic currents based on experiments in human myocytes.The ten Tusscher-Noble-Noble-Panlov model (Ten Tusscher et al., 2004) consists of 17 variables, and uses new formulations for most of the major ionic currents, all of them based on experiments in human ventricular myocytes or expressions of humanion channels. Finally, the Iyer-Mazhari-Winslow model (Iyer et al., 2004) consists of 67 variables, and is also based on data from human myocytes and recombinant human
31
-
8/
![MATEMATYKA UNIWERSYTECKA W LO - SKRYPTpreisner/dyd/2019_14lo/files/...Wrocław,3grudnia2020 MATEMATYKA UNIWERSYTECKA W LO - SKRYPT MARCINPREISNER [MARCIN.PREISNER@UWR.EDU.PL] Spis](https://static.fdocuments.pl/doc/165x107/60a8ed210b91f36df23a9ba2/matematyka-uniwersytecka-w-lo-preisnerdyd201914lofiles-wrocaw3grudnia2020.jpg)