
Interstitial pneumonia in children as a clinical and ... · (-07...
7
EJMT 4(21) 2018 • European Journal of Medical Technologies 65 Copyright © 2018 by ISASDMT Corresponding address: Rafał Skowronek M.D., Ph.D. Department of Forensic Medicine and Toxicology, School of Medicine in Katowice, Medyków str 18, 40-752 Katowice, Poland e-mail: [email protected] phone 32 2088452 fax 32 2527591 Key words: atypical pneumonia, post-mortem diagnosis, SIDS, SUDI, children Interstitial pneumonia in children as a clinical and forensic medical problem Abstract The article presents current literature on interstitial pneumonia in children and infants in clinical and forensic medical aspect. Particular attention has been paid to the clinical course and etiological factors of the disease, as well as to the results of autopsy and histopathology. The article also discusses the possibility of extending the post-mortem studies with immunohistochemistry and genet- ic tests. Interstitial pneumonia in children, specially in infants, is still the leading cause of death in this age group. This problem is a challenge for paediatricians due to its atypical clinical course and the different etiological factors that are difficult to determine. In turn, that’s also complicated issue for forensic medical experts and pathomorphologists – due to its scant and often ambiguous mor- phological presentation, making it difficult to determine the cause of death. Michał Szczepański 1 , Rafał Skowronek 1 , Beata Sarecka-Hujar 2 , Dorota Raczkiewicz 3 , Ilona Kopyta 4 1 Department of Forensic Medicine and Toxicology, School of Medicine in Katowice, Medical University of Silesia in Katowice, Poland 2 Department of Pharmaceutical Technology, School of Pharmacy with the Division of Laboratory Medicine, Medical University of Silesia in Katowice, Poland 3 Institute of Statistics and Demography, Warsaw School of Economics, Warsaw, Poland 4 Department of Pediatric Neurology, School of Medicine in Katowice, Medical University of Silesia in Katowice, Poland European Journal of Medical Technologies 2018; 4(21): 65-71 Copyright © 2018 by ISASDMT All rights reserved www. medical-technologies.eu Published online 30.10.2018
Transcript of Interstitial pneumonia in children as a clinical and ... · (-07...
EJMT 4(21) 2018 • European Journal of Medical Technologies
65 Copyright © 2018 by ISASDMT
Corresponding address: Rafał Skowronek M.D., Ph.D. Department of Forensic Medicine and Toxicology, School of Medicine in Katowice, Medyków str 18, 40-752 Katowice, Polande-mail: [email protected] phone 32 2088452fax 32 2527591
Key words: atypical pneumonia, post-mortem diagnosis, SIDS, SUDI, children
Interstitial pneumonia in children as a clinical and forensic medical problem
Abstract The article presents current literature on interstitial pneumonia in children and infants in clinical and forensic medical aspect. Particular attention has been paid to the clinical course and etiological factors of the disease, as well as to the results of autopsy and histopathology. The article also discusses the possibility of extending the post-mortem studies with immunohistochemistry and genet-ic tests. Interstitial pneumonia in children, specially in infants, is still the leading cause of death in this age group. This problem is a challenge for paediatricians due to its atypical clinical course and the different etiological factors that are difficult to determine. In turn, that’s also complicated issue for forensic medical experts and pathomorphologists – due to its scant and often ambiguous mor-phological presentation, making it difficult to determine the cause of death.
Michał Szczepański1, Rafał Skowronek1, Beata Sarecka-Hujar2, Dorota Raczkiewicz3, Ilona Kopyta4
1 Department of Forensic Medicine and Toxicology, School of Medicine in Katowice, Medical University of Silesia in Katowice, Poland
2 Department of Pharmaceutical Technology, School of Pharmacy with the Division of Laboratory Medicine, Medical University of Silesia in Katowice, Poland
3 Institute of Statistics and Demography, Warsaw School of Economics, Warsaw, Poland
4 Department of Pediatric Neurology, School of Medicine in Katowice, Medical University of Silesia in Katowice, Poland
European Journal of Medical Technologies 2018; 4(21): 65-71
Copyright © 2018 by ISASDMT All rights reserved www. medical-technologies.eu Published online 30.10.2018

EJMT 4(21) 2018 • European Journal of Medical Technologies
66 Copyright © 2018 by ISASDMT
IntroductionIn general, pneumonia is the answer of “pulmonary tissue” to broadly understood inflammatory stimuli. Microbes are the most common stimulus, but it can also be non-infectious agents that cause an inflamma-tory reaction in the lung. Morphologically, this pro-cess manifests itself in retrogressive changes, blood flow disturbances and productive changes. It can roll – or more precisely – start mainly in the alveoli or in the lung stroma [1,2]. This process causes a reduction of the total lung capacity (to varying degrees), which is why it is included in the restrictive diffuse lung diseases of known aetiology. Clinical and histopatho-logical symptoms of the disease is extremely rich and depends primarily on the type of pathogenic agent, the form of inflammation and individual conditions of the patient (age, maturity of the immune system, general health status, etc.).
There are many ways to distinguish this group of diseases, which sometimes cause some classification difficulties. The division criteria are as follows: etio-logical factor (bacterial inflammation – specific and nonspecific, viral, fungal, parasitic, immunoaller-genic); the way of infection spread (bronchial, blood-borne, by continuity from surrounding tissues); type of inflammatory exudate (serous, catarrhal, fibrinous, purulent, hemorrhagic, gangrenous); circumstances in which the infection occurred (hospital-acquired pneumonia – HAP or community-acquired pneu-monia – CAP, so-called environmental); the extent of inflamed lung tissue and the type of involvement of the parenchyma (lobar inflammation or lobular, al-veolar, interstitial, pleural or non-pleural) [1–3].
According to Maitra and Kumar, the best division in everyday clinical practice is due to the clinical situation in which the infection occurs, i.e. “Pneu-monia syndrome”: HAP, aspiration pneumonia, chronic pneumonia, necrotizing pneumonia and lung abscess, and also immunocompromised indi-viduals’ pneumonia [4]. This division enables rapid implementation of pharmacological empirical ther-apy, because the list of etiological factors in a given clinical situation is relatively specific and commonly known [5].
Epidemiological data on the incidence of interstitial pneumonia and related mortality Pneumonia is one of the most common causes of death among respiratory diseases of the general pop-ulation. In Poland, in 2006, the standardized death rate due to pneumonia per 100,000 population was 19 cases [6]. Mortality among patients with commu-nity-acquired pneumonia treated out-patient does not exceed 1%, whereas when the patient is in need of hospitalization, it grows to 5–20% [7]. The risk factor for falling sick and death from pneumonia is age – mortality is highest in extreme age groups. Pneumo-nia remains one of the leading causes of children’s death, especially those who are under the age of one. According to the 1990 data of the WHO, in devel-oping countries pneumonia is the primary cause of 25% of deaths among children under five and in this respect it precedes even diarrhea (22%) [3]. Among children up to two years of age, there are two mil-lion deaths annually [8]. According to the data of the Central Statistical Office, in 2008, 69 children under 4 died in Poland for pneumonia (including 50 chil-dren up to 1 year of age) [9]. The percentage of infant deaths due to pneumonia per 1,000 live births in 2008 was 0.1, which means that one baby per 10,000 dies for this reason. It should be noted that this indicator has remained at a similar level since the beginning of the 21st century. Its significant reduction from 1.8 to 0.2 (from over 4% to around 1.8%) took place in the 1980s and 1990s [6,9].
Data from 2013 show that pneumonia in Poland caused 6.5% deaths among people aged 1-19 years, and since 2000 there has been an upward trend in mortality rates for this reason [10]. Causes of this phenomenon are not clear, but at least partly it may be associated with an increase in the frequency of pneumonia caused by unidentified infectious agents.
In the forensic medical practice it was also con-firmed, that pneumonia is a significant cause of chil-dren’s death in the group of deaths from disease-relat-ed causes. Bloch-Bogusławska et al. analyzing a small
EJMT 4(21) 2018 • European Journal of Medical Technologies
67 Copyright © 2018 by ISASDMT
group of 14 newborns who died due to illness in the years 1992–2006, based on the results of microscopic studies, found that the most common (71%) cause of death in this group was respiratory failure due to pneumonia [11].
Clinical symptoms of interstitial pneumonia depending on age and etiological factorInterstitial pneumonia is a large group of diseases that includes both: infectious inflammations that affect different degrees of lung stroma, and less frequent id-iopathic inflammations that are part of a broad spec-trum of interstitial lung diseases [2,12]. This group includes atypical lung diseases, particularly difficult to diagnose, both in life-related diagnostics and post-mortem diagnostics – pathomorphological and forensic medical. This consists of: uncharacteristic
course of the disease and often scant symptomato-logy, a short period from the first onset to a dramatic deterioration, poor morphological image and the lack of established diagnostic criteria, especially in in-fant cases. For this type of inflammation predispose, among others, any immune disorders (deficiencies, autoimmune diseases) and malnutrition.
Clinical symptoms are scant, especially in chil-dren may be hidden (“fever-free pneumonia”) or limited to elevated temperature. Unfortunately, this often results in a delayed diagnosis or even a lack of it, which may raise suspicion of a medical error or negligence of parents. In such situations, it is neces-sary to obtain a forensic medical opinion (optimally in an expert team composed of a forensic medical ex-pert and a pediatrician) regarding, among others, the possibility of early diagnosis of a child’s illness and prevention of death. In the case of atypical pneumo-nia, sudden respiratory failure is disproportionate to previous physical and radiological symptoms.
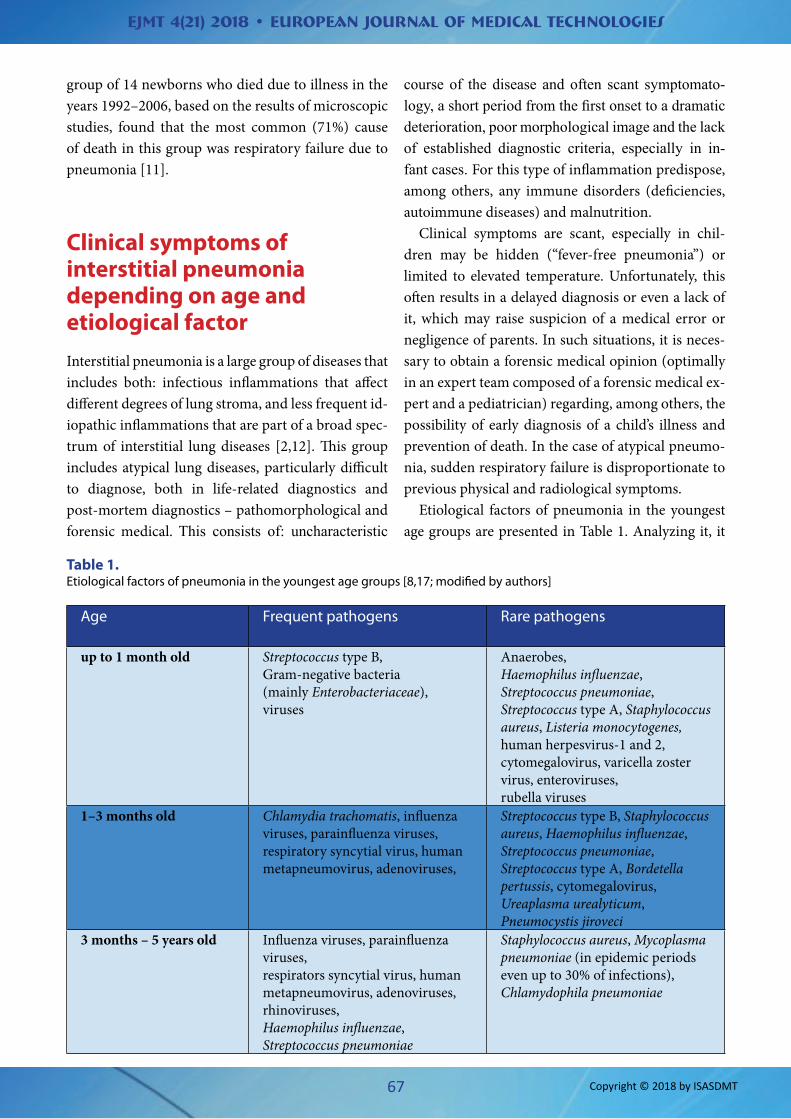
Etiological factors of pneumonia in the youngest age groups are presented in Table 1. Analyzing it, it
Age Frequent pathogens Rare pathogens
up to 1 month old Streptococcus type B, Gram-negative bacteria (mainly Enterobacteriaceae), viruses
Anaerobes, Haemophilus influenzae, Streptococcus pneumoniae, Streptococcus type A, Staphylococcus aureus, Listeria monocytogenes, human herpesvirus-1 and 2, cytomegalovirus, varicella zoster virus, enteroviruses, rubella viruses
1–3 months old Chlamydia trachomatis, influenza viruses, parainfluenza viruses, respiratory syncytial virus, human metapneumovirus, adenoviruses,
Streptococcus type B, Staphylococcus aureus, Haemophilus influenzae, Streptococcus pneumoniae, Streptococcus type A, Bordetella pertussis, cytomegalovirus, Ureaplasma urealyticum, Pneumocystis jiroveci
3 months – 5 years old Influenza viruses, parainfluenza viruses, respirators syncytial virus, human metapneumovirus, adenoviruses, rhinoviruses, Haemophilus influenzae, Streptococcus pneumoniae
Staphylococcus aureus, Mycoplasma pneumoniae (in epidemic periods even up to 30% of infections), Chlamydophila pneumoniae
Table 1. Etiological factors of pneumonia in the youngest age groups [8,17; modified by authors]
EJMT 4(21) 2018 • European Journal of Medical Technologies
68 Copyright © 2018 by ISASDMT
should be remembered, that more and more often at-tention is paid to the fact, that the boundary of the domination of specific pathogens gradually dimin-ishes depending on the age of the child [13,14]. Infec-tious interstitial pneumonias are most often caused by viruses (influenza, parainfluenza, chickenpox, measles, adenovirus, CMV, etc.), so-called atypical bacteria (Mycoplasma sp., Chlamydia sp., Legionella sp., Rickettsia sp., Francisella tularensis) and fungi (e.g., Pneumocystis jiroveci) [1,3,15,16].
The concept of “atypity” is basically a histori-cal term, because it was created at a time when the available research methods didn’t allow to show the presence of microorganisms responsible for infec-tion in materials collected from patients, and the use of penicillin did not bring the expected result [18]. This concept was introduced to medical terminol-ogy in 1938. At that time, eight cases were described where pharyngitis caused by an unknown pathogen (probably Mycoplasma pneumoniae), accompanied by flu-like symptoms, evolved into inflammation of the larynx, trachea, bronchi and lungs [4]. Today, in the times of molecular biology and genetics achieve-ments, when we know and can identify atypical mi-croorganisms, this term is valid only in the context of different clinical symptoms of inflammation caused by them, not recalling the course of “typical” bacte-rial inflammation, e.g. classic lobar pneumococcal lung inflammation [19-21].
Mycoplasma pneumoniae – the most common atypical bacterium – is responsible for about 2–39% of atypical pneumonia [13,22]. The development of mycoplasma pneumonia is subacute, with gradually increasing persistent cough, initially dry, then with the expectoration [3]. Clinical symptoms may affect not only the lungs, but also extrapulmonary loca-tions: skin (rashes, erythema multiforme), circula-tory system (pericarditis, arrhythmias), hematopoi-etic system (thrombocytopenia, haemolytic anemia), osteoarticular system (arthritis, muscle pain), the digestive system (nausea, vomiting, hepatitis), the nervous system (aseptic encephalitis and meningitis, ataxia) and the kidneys (glomerulonephritis) [8]. The clinical course of chlamydial pneumonia is similar to mycoplasma pneumonia. However, characteris-tic symptoms are: hoarseness and conjunctivitis [3].
Chlamydophila pneumoniae induces the production of IgE in the child’s body, hence allergic reactions are possible. In the diagnosis of both diseases, radiologi-cal, microbiological and serological tests for specific antibodies are helpful in the face of usually scant clin-ical symptoms. For the diagnosis of interstitial pneu-monia caused by an atypical infection, organ biopsy is, in most cases, not performed [8].
Viral infections, another cause of atypical pneu-monia, can occur at any age. In adult’s age group it is most often caused by influenza A and B viruses, whereas in children’s age group also by respiratory syncytial virus (RSV), human metapneumovirus (hMPV), parainfluenza viruses, adenovirus, corona-virus, rhinovirus, enterovirus, human herpesvirus-1 and 2 (HHV-1 and 2), cytomegalovirus (CMV) and varicella zoster virus (VZV) [8,17]. Viral infection, causing inactivation of the mucociliary clearance mechanism, predisposes to the development of se-condary bacterial infection. The overlap of these two processes not only makes it difficult to diagnose, but – more importantly – definitely worsens the progno-sis for a sick child. In summary, the clinical presenta-tion of the above mentioned pneumonias is usually oligosymptomatic and the course of these diseases is sometimes extremely dynamic.
Post-mortem image of interstitial pneumonia and forensic medical diagnostic possibilities
Sudden deaths of infants and children are invariably an important diagnostic problem for a forensic medi-cal expert, because an autopsy usually does not al-low to determine the cause of death, which does not change the fact that this is a necessary examination and should be ordered and carried out in each case [23,24]. Histopathological examination also rela-tively often does not allow resolved unambiguously in this regard, including the determination of the etiological factor. Only some microorganisms cause characteristic changes in cells, e.g. “eye-owl” cells in CMV infection [25,26].
EJMT 4(21) 2018 • European Journal of Medical Technologies
69 Copyright © 2018 by ISASDMT
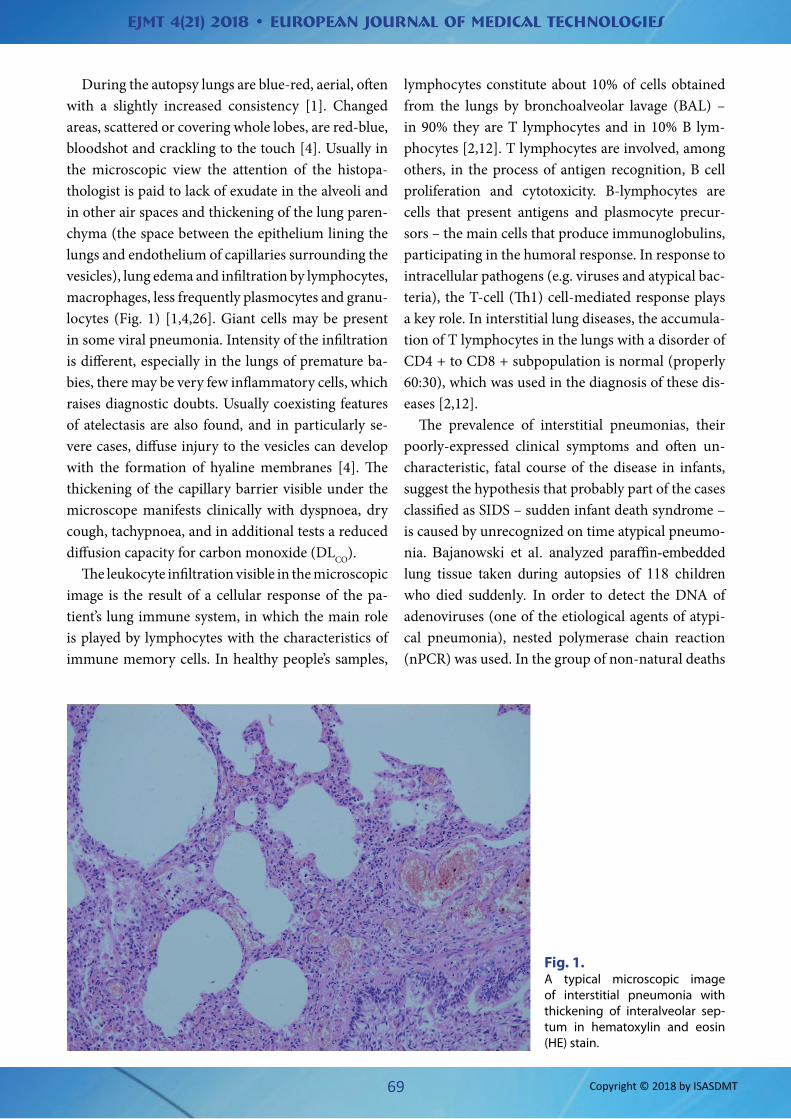
During the autopsy lungs are blue-red, aerial, often with a slightly increased consistency [1]. Changed areas, scattered or covering whole lobes, are red-blue, bloodshot and crackling to the touch [4]. Usually in the microscopic view the attention of the histopa-thologist is paid to lack of exudate in the alveoli and in other air spaces and thickening of the lung paren-chyma (the space between the epithelium lining the lungs and endothelium of capillaries surrounding the vesicles), lung edema and infiltration by lymphocytes, macrophages, less frequently plasmocytes and granu-locytes (Fig. 1) [1,4,26]. Giant cells may be present in some viral pneumonia. Intensity of the infiltration is different, especially in the lungs of premature ba-bies, there may be very few inflammatory cells, which raises diagnostic doubts. Usually coexisting features of atelectasis are also found, and in particularly se-vere cases, diffuse injury to the vesicles can develop with the formation of hyaline membranes [4]. The thickening of the capillary barrier visible under the microscope manifests clinically with dyspnoea, dry cough, tachypnoea, and in additional tests a reduced diffusion capacity for carbon monoxide (DLCO).
The leukocyte infiltration visible in the microscopic image is the result of a cellular response of the pa-tient’s lung immune system, in which the main role is played by lymphocytes with the characteristics of immune memory cells. In healthy people’s samples,
lymphocytes constitute about 10% of cells obtained from the lungs by bronchoalveolar lavage (BAL) – in 90% they are T lymphocytes and in 10% B lym-phocytes [2,12]. T lymphocytes are involved, among others, in the process of antigen recognition, B cell proliferation and cytotoxicity. B-lymphocytes are cells that present antigens and plasmocyte precur-sors – the main cells that produce immunoglobulins, participating in the humoral response. In response to intracellular pathogens (e.g. viruses and atypical bac-teria), the T-cell (Th1) cell-mediated response plays a key role. In interstitial lung diseases, the accumula-tion of T lymphocytes in the lungs with a disorder of CD4 + to CD8 + subpopulation is normal (properly 60:30), which was used in the diagnosis of these dis-eases [2,12].
The prevalence of interstitial pneumonias, their poorly-expressed clinical symptoms and often un-characteristic, fatal course of the disease in infants, suggest the hypothesis that probably part of the cases classified as SIDS – sudden infant death syndrome – is caused by unrecognized on time atypical pneumo-nia. Bajanowski et al. analyzed paraffin-embedded lung tissue taken during autopsies of 118 children who died suddenly. In order to detect the DNA of adenoviruses (one of the etiological agents of atypi-cal pneumonia), nested polymerase chain reaction (nPCR) was used. In the group of non-natural deaths
Fig. 1. A typical microscopic image of interstitial pneumonia with thickening of interalveolar sep-tum in hematoxylin and eosin (HE) stain.

EJMT 4(21) 2018 • European Journal of Medical Technologies
70 Copyright © 2018 by ISASDMT
no adenovirus DNA was found, in the group with-out histopathological image of interstitial pneumo-nia adenovirus DNA was found in 10.2% of samples, while in the group with advanced microscopic im-age of interstitial pneumonia adenovirus DNA was present in 26% of samples [19]. In post-mortem di-agnosis of interstitial pneumonias, immunohistoche-mical methods are very rarely attempted. Ogbuihi and Zink, using monoclonal antibodies directed against leukocytic antigens, intended to character-ize the cellular components in the interstitium of the lungs of children who died with SIDS. It is true that they failed to confirm the inflammatory origin of the focal cell proliferation observed in SIDS, but they proved the inflammatory nature of cells infiltrating the lung subareas in cases of interstitial inflamma-tion [27]. Among newer works, attention is drawn to Dettmeyer’s report that cells infected with CMV vi-rus typically present a positive immunohistochemi-cal reaction to E-selectin [26].
In conclusion, interstitial pneumonia in children, especially in infant patients, is still the leading cause of death in this age group. This problem is a challenge for pediatricians due to the atypical clinical course and the etiological factor that is difficult to deter-mine. In turn, that’s also complicated issue for foren-sic medical experts and pathomorphologists – due to its scant and often ambiguous morphological image, making it difficult to determine the cause of death.
References1. Papla B, Stachura J. Choroby płuc, opłucnej i śród-
piersia. [W:] Domagała W. [red.]. Patologia znaczy słowo o chorobie. Tom I. Wyd. III. Polska Akademia Umiejętności, Kraków 2016.
2. Stocker JTh, Husain AN, Dehner LP. Acquired non-neoplastic neonatal and pediatric diseases. [A:] Tomashefski JF [ed.]. Dail and Hammar’s Pulmona-ry Pathology. Volume I: Nonneoplastic lung dise-ase. Springer, 2008, 176-227.
3. Szumińska-Napiontek E, Wysocki J. Antybiotyki w leczeniu zapaleń płuc u dzieci. Przew Lek 2001, 4(7), 128-132.
4. Maitra A, Kumar V. Płuca i górne drogi oddecho-we. [W:] Kumar V, Cotran RS, Robbins SL. Robbins
Patologia. Wyd. I polskie. Urban & Partner, Wro-cław 2005, 519-580.
5. Blyth CC, Gerber JS. Macrolides in Children With Community-Acquired Pneumonia: Panacea or Pla-cebo? J Pediatric Infect Dis Soc 2018, 7(1), 71-77.
6. Wojtyniak B, Stokwiszewski J, Goryński P, [et al.]. Długość życia i umieralność ludności Polski. [W:] Wojtyniak B, Goryński P. [red.]. Sytuacja zdrowotna ludności Polski. Narodowy Instytut Zdrowia Publicz-nego – Państwowy Zakład Higieny 2008, 31-86.
7. Kuś J. Zapalenia płuc wywołane przez drob-noustroje. [W:] Szczeklik A. [red.]. Choroby we-wnętrzne. Stan wiedzy na 2010. Medycyna Prak-tyczna 2010, 618-638.
8. Krenke K, Lange J. Zapalenia płuc. [W:] Kulus M. [red.]. Choroby układu oddechowego u dzieci. Wolters Kluwer Polska, Warszawa 2010, 146-177.
9. Zgony. [W:] Rocznik Demograficzny 2010. GUS 2010, 308-397.
10. Mazur J, Malinowska-Cieślik M, Oblacińska A. Przyczyny zgonów dzieci i młodzieży w wieku 1-19 lat w Polsce w świetle międzynarodowych statystyk od 2000 roku. Dev. Period. Med. 2017, 21(2), 111-123.
11. Bloch-Bogusławska E, Wolska E, Paradowska A. Zgony dzieci w wieku noworodkowym ze szcze-gólnym uwzględnieniem dzieciobójstwa w ma-teriałach Zakładu Medycyny Sądowej w Bydgosz-czy w latach 1992-2006. Arch Med Sąd Kryminol. 2008, 58, 145-149.
12. Nicholson AG. Interstitial Pneumonias. [A]: Toma-shefski JF. [ed.]. Dail and Hammar’s Pulmonary Pathology. Volume I: Nonneoplastic Lung Disease. Springer, 2008, 695-721.
13. Woźniakowska-Gęsicka T, Kamer B, Kiciński P, [et al.]. Epidemiologia i obraz kliniczny zapalenia płuc o etiologii Mycoplasma pneumoniae u dzie-ci. Przegląd Pediatryczny 2008, 38, 237-242.
14. Le Roux DM, Zar HJ. Community-acquired pneu-monia in children – a changing spectrum of dise-ase. Pediatr Radiol. 2017, 47(11), 1392-1398.
15. Rudan I, Boschi-Pinto C, Biloglav Z, [et al.]. Epide-miology and etiology of childhood pneumonia. Bull World Health Organ. 2008, 86(5), 408-416.
16. Rudan I, O’Brien KL, Nair H, [et al.]. Child Health Epidemiology Reference Group (CHERG). Epide-miology and etiology of childhood pneumonia in 2010: estimates of incidence, severe morbidity, mortality, underlying risk factors and causative
EJMT 4(21) 2018 • European Journal of Medical Technologies
71 Copyright © 2018 by ISASDMT
pathogens for 192 countries. J Glob Health 2013, 3(1), 010401.
17. Pawlik J. Bakteryjne zapalenia płuc u dzieci. Etiolo-gia i przebieg kliniczny. Klinika Pediatryczna 1998, 6, 13-16.
18. Korzon M. Atypowe zapalenie płuc u dzieci i mło-dzieży. Forum Medycyny Rodzinnej 2009, 3, 92–98.
19. Bajanowski T, Wiegand P, Cecchi R, [et al.]. Detection and significance of adenoviruses in cases of sud-den infant death. Virchows Arch. 1996, 428, 113-8.
20. Chang HY, Chang LY, Shao PL, [et al.]. Comparison of real-time polymerase chain reaction and sero-logical tests for the confirmation of Mycoplasma pneumoniae infection in children with clinical dia-gnosis of atypical pneumonia. J Microbiol Immu-nol Infect. 2014, 47(2), 137-144.
21. Nowak A, Skowronek R, Reichman-Warmusz E, [et al.]. Badania wirusologiczne w diagnostyce nagłych niespodziewanych zgonów dzieci. Arch Med Sąd Kryminol. 2013, 63(2), 118-126.
22. Toltzis P. 50 Years Ago in The Journal of Pedia-trics: Mycoplasma pneumoniae (Eaton Atypical
Pneumonia Agent) in Children’s Respiratory Infec-tions. J Pediatr. 2015, 166 (5), 1207.
23. Daş T, Sargan A, Yağmur G, [et al.]. Viral Pneumo-nias in Forensic Autopsies: Evaluation and Classifi-cation of Histopathologic Changes With Microbio-logic Correlation. Am J Forensic Med Pathol. 2016, 37(4), 255-263.
24. Turner GD, Bunthi C, Wonodi CB, [et al.]. The role of postmortem studies in pneumonia etiology re-search. Clin Infect Dis. 2012, 54 Suppl 2, S165-71.
25. Potter’s Pathology of the Fetus, Infant and Child, 2nd Edition. Gilbert-Barness. B. [ed.]. Mosby Else-vier, 2007.
26. Dettmeyer RB, Forensic Histopathology. Funda-mentals and Perspectives, 2nd Edition. Springer--Verlag, Berlin Heidelberg 2018.
27. Ogbuihi S, Zink P. Cellular components in inter-stitial lung tissue in sudden infant death – immu-nohistochemical characterization. Z Rechtsmed. 1989, 102, 133-42.









![i c r o b i ol gy: pen c p l p ie s cse Applied ... › open-access › histoplasmosis...Histoplasmosis is a community acquired infection, most often presenting as pneumonia [1]. Although](https://static.fdocuments.pl/doc/165x107/5f25c3316b13c70c666ee5cb/i-c-r-o-b-i-ol-gy-pen-c-p-l-p-ie-s-cse-applied-a-open-access-a-histoplasmosis.jpg)








