CHF in English

of 58
-
Upload
dessyana-paulus -
Category
Documents
-
view
222 -
download
0
Transcript of CHF in English
-
8/13/2019 CHF in English
1/58
1
FOREWORD
First of all, lets thanks to Allah SWT, who has given us mercies and blessings,
the writer can finish this papers work which is about Congestive Heart Failure
(CHF) it purposes to complate english assignment that is given by lecturer.
Then a successive salawat not forget to send us to our great Prophet Muhamad
SAW, which has brought us from nature without the knowledge of the natural with
full knowledge of all powerful. So that spur us to further achievement in our lives.
The writer also wishes to say gratitude to Miss. Arma as the lecturer of english
who has guided, and given me an oppurtunity to make and to complate thisassignment. Writer realizes a lot of deficiencies in the writing of this paper. Criticism
and suggestions that are built, the author is expected for perfection this paper.
Jakarta, 26 April 2012
The writer
Groups of 1
iii
CONTENTS
-
8/13/2019 CHF in English
2/58
2
FOREWORD....iii
CONTENTS...iv
CHAPTER I INTODUCTION
A. Background.1B. The Purpose.1
1. General Purpose...12. Spesific Purpose...2
C. Plane of Problem.2D. Methode Of Writing2E. The Scope2F. Systemic Of Writing....2
CHAPTER II BASIC OF THEORY AND NURSING CARE
A. The Heart.4B. Heart Failure5C. Classifications.6D. Symptoms8E. Etiology...9F. Pathopysiology..11G. Pathoflow...18H. Test20I. Treatment...21J. Heart Failure Management21K. Congestive Heart Failure Intervension..23L. Complication of Heart Failure...24M.Physical examination.25
N.Nursing Care1. Patient Assessment Data Base.25
iv
2. Discharge plan.................................................................................................273. Diagnosis And Intervention.28
CHAPTER III CASE REPORT
-
8/13/2019 CHF in English
3/58
3
A. Case Report...44B. Fokus Data47C. Data Analysis....47D. Intervension...49E. Implementasion.49F. Evaluasion.52
CHAPTER IV CLOSING
A. Conclusion..53B. Suggestion..53
REFFERENCE54
v
-
8/13/2019 CHF in English
4/58
4
CHAPTER I
INTRODUCTION
A. BACKGROUNDCongestive Heart Failure (CHF) today is the only cardiovascular disease that has
increasing incidence and prevalence.Risk of death from heart failure ranged from 5-10% per
year in mild heart failure which will rise to 30-40% in severe heart failure. In addition, heart
failure is a disease that most often need a repeated treatment in the hospital (readmission)
although outpatient treatment has been given an optimal.
Congestive heart failure (CHF) is a complex clinical syndrome that can result from any
functional or structural cardiac disorder that impairs the ventricles ability to fill with or eject
blood. Since there is no definitive diagnostic test for heart failure, it remains a clinical
diagnosis that is largely based on a careful history and physical examination and supported by
ancillary tests such as chest radiograph, electrocardiogram, and echocardiography. The
diagnosis of heart failure is often determined by a careful history and physical examination
and characteristic chest radiograph findings.
Heart failure is a common disease, affecting approximately 5 million people in the United
States, and it occurs predominately in the elderly, with almost 80% of cases occurring in
patients over the age of 65. According to the research, the majority of elderly Heart Failure is
diagnosed can not live more than 5 years (Ebbersole, Hess, 1998).
With the background backs on these issues, the paper is made to find out more what it is
heart failure, how to handle it, until the nursing care to patient of heart failure.
B. THE PURPOSE1. General Purpose
The general purpose of this papers is aim to able to understand the definition, etiology,
classification, pathophysiology, diagnostic examination, treatment, and nursing care to
clients with congestive heart failure (CHF).
-
8/13/2019 CHF in English
5/58
5
2. Spesific PurposeSpesific purpose is of this papers is aim to :
a. Explain the definition of Congestive Heart failureb. Mention and explain the etiologyc. Mention the symptoms from Congestive Heart Failured. Explain the pathophysiology from congestive Heart Failuree. Mention the complication from Congestive Heart Failure
C. PLANE OF PROBLEM1. What is the definition of Congestive Heart Failure ?2. What is the etiology of Congestive heart failure ?3. What is the symptom of Congestive Heart Failure ?4. How is the pathophysiology of Congestive Heart Failure ?5. What is the treatment of Congestive Heart Failure ?6. What is the test of Congestive Heart Failure?7. What is the complication of Congestive Heart Failure?
D. METHODE OF WRITINGIn the writing of this paper we use books and internet as the source.
E. THE SCOPEThe scope of this paper is family and all the students. Students can explain the definition
of CHF, CHF etiology, pathophysiology of CHF, clinical manifestations of CHF, Medical
Management and Nursing Care should be given to clients with CHF.
F. SYSTEMIC OF WRITINGIn this papers, we used the systemic of write like this:
CHAPTER I INTODUCTION
G. BackgroundH. The Purpose
-
8/13/2019 CHF in English
6/58
6
3. General Purpose4. Spesific Purpose
I. Plane of ProblemJ. Methode Of WritingK. The ScopeL. Systemic Of WritingCHAPTER II BASIC OF THEORY AND NURSING CARE
O. The HeartP. Heart FailureQ. ClassificationsR. SymptomsS. EtiologyT. PathopysiologyU. PathoflowV. TestW.TreatmentX. Heart Failure ManagementY. Congestive Heart Failure IntervensionZ. Complication of Heart FailureAA. Physical examinationCHAPTER III CASE REPORT
G. Case ReportH. Fokus DataI. Data AnalysisJ. IntervensionK. ImplementasionL. EvaluasionCHAPTER IV CLOSING
C. CONCLUSIOND. SUGGESTION
-
8/13/2019 CHF in English
7/58
7
CHAPTER II
BASIC OF THEORY AND NURSING CARE
A. THE HEARTThe heart is responsible for pumping blood to all the organs in the body. It is highly
specialized muscle that is expected to work continously, without rest, for a lifetime. The heart
has aright and a left side. Each side has 2 chambers : the atrium and the ventricle. Special
valves divide the chambers and prevent blood from flowing backward.
Blood loaded with oxygen comes from the lungs and enters the left atrium. It stays there
until the mitral valve opens up and the atrium contracts. This forces the blood into the left
ventricle. The blood is then pumped to the rest of the body through the aortic valve into the
biggest blood vessel of the body, the aorta.
After the blood comes back from circulating through the body, it goes into the right
atrium. From there, it is pumped into the right ventricle through the tricuspid valve and then
to the lung through the pulmonic valve. In the lung, the blood picks up oxygen and returns to
the left atrium, where the whole cycle starts again. The heart needs a continous supply of
-
8/13/2019 CHF in English
8/58
8
oxygen and sugar to be able to function. Oxygen-rich blood is delivered to the heart through
the coronary arteries. These arteries branch off from the aorta.
B. HEART FAILURE
Heart failure is a condition where the heart is not able to pump blood to the rest of the
body at a normal rate. When the heart cannot pump all the blood it receives, excess fluidcould back up into the lungs and other parts of the body. The lack of blood being supplied to
the body in addition to the buildup of fluids causes symptoms of heart failure. When fluids
collect in the lungs, it is called congestion. That is why this disease is called congestive heart
failure.
There are 2 mechanisms of reduced cardiac output and heart failure: systolic dysfunction
and diastolic dysfunction.The most common causes of systolic dysfunction(defined by a left-
ventricular ejection fraction of_50%) are ischemic heart disease, idiopathic dilated
cardiomyopathy, hypertension, and valvular heart disease. Diastolic dysfunction (defined as
dysfunction of left-ventricular filling with preserved systolic function) may occur in up to 40
50% of patients with heart failure, it is more prevalent in women, and it increases in
frequency with each decade of life. Diastolic dysfunction can occur in many of the same
conditions that lead to systolic dysfunction. The most common causes are hypertension,
ischemic heart disease, hypertrophic cardiomyopathy, and restrictive cardiomyopathy. Many
patients who have symptoms suggestive of heart failure (shortness of breath, peripheraledema, paroxysmal nocturnal dyspnea) but also have preserved leftventricular function may
-
8/13/2019 CHF in English
9/58
9
not have diastolic dysfunction; instead, their symptoms are caused by other etiologies, such as
lung disease, obesity, or occult coronary ischemia.
There are several levels of congestive heart failure :
a. Mildb. Averagec. Severed. Very severeEach level may limit a persons activities more and more. With very severe heart failure, a
person may be short of breath or feel fatigued even at rest.
C. CLASSIFICATIONSThe New York Heart Association developed a system that has been used for many years
to provide a standardized set of criteria for the classification of heart failure based on the
severity of the condition. This is evaluated by symptoms and ability to function.
1. Class I: no undue symptoms associated with ordinary activity and no limitation ofphysical activity
2. Class II: slight limitation of physical activity; patient comfortable at rest3. Class III: marked limitation of physical activity; patient comfortable at rest4. Class IV: inability to carry on any physical activity without discomfort; symptoms of
cardiac insufficiency or chest pain possible even at rest.
Ef fects of Heart Failu re
1. Strength of muscle contractions is reduced.2.
Ability of the heart chambers to fill with blood is limited, so there is less blood to
pump out to tissues in the body.
3. The pumping heart chambers fill with too much blood; the the heart muscle is notstrong enough to pump out all the blood it receives.
-
8/13/2019 CHF in English
10/58
10
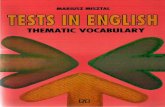
LEFT-SIDED AND RIGHT-SIDED HEART FAILURE
Heart failure can affect the left, right, or both
sides of the heart. The heart is made up of four
chambers. The leftatrium and the right atrium on
top mainly collect the blood, and the left ventricle
and right ventricle on the bottom pump the blood.
The right side of the heart receives oxygen-
depleted or used blood from the body and
pumps it to the lungs to be replenished with
oxygen. The left side receives oxygen-rich blood from the lungs and pumps it to the rest of
the body.
Left-sided heart failure is the most
common type of heart failure.1 The left
ventricle on the lower left side of the heart is
the main pumping chamber. When it fails,
oxygen-rich blood is not pumped to the rest of
the body; instead, it can back up into the left
atrium and into the lungs, where it builds up.
Left-sided heart failure causes fatigue because
the body is not receiving enough blood and
shortness of breath because of the buildup of
fluid (congestion) in the lungs.
Right-sided heart failure usually happens as a result of left-sided heart failure. As the
failing left ventricle causes blood to build up in the lungs, the right ventricle finds it harder
and harder to pump blood to the lungs to pick up oxygen. Less commonly, right-sided heart
failure can also occur on its own, for example, when caused by lung disease (such as
emphysema) or heart valve problems. Right-sided heart failure can cause blood to back up in
theveins,resulting in swelling in the legs, ankles or belly, and can lead to shortness of breath
when the belly is enlarged. Right-sided heart failure can also cause fatigue when the left
http://void%280%29/http://void%280%29/http://void%280%29/http://void%280%29/ -
8/13/2019 CHF in English
11/58
11
ventricle doesn't fill with enough blood and can't supply the body with enough oxygen-rich
blood.
D. SYMPTOMSa. Shortness of breath (dyspnea)b. Shortness of breath when lying down (orthopnea)c. Shortness of breath while sleeping (paroxysmal or intermittent nocturnal dyspnea)d. Buildup of fluid in the lungs (pulmonary edema), frequently causing a person to
cough up blood-tinged sputum
e. Buildup of excess fluid (edema) in other parts of the body, causing weight gain,swelling of the ankles, legs, and back, and in extreme cases fluid accumulation in
the abdomen (ascites)f. Fatigue, weakness, and an inability to exert oneself physically or mentallyg. Blueness of the skin (cyanosis)
1. Symptoms of left-side heart failurea. Fatigue
b. Shortness of breath (dyspnea)c. Shortness of breath when lying down (othopnea)d. Paroxysmal (intermittent) nocturnal dyspneae. Accumulation of fluid in the lungs (pulmonaryedema), frequently causing a person
to cough up blood-tinged sputum
2. Symptoms of right-side heart failurea. Swelling (edema)
b. Dependent edema (edema that travels by gravity to the lowest portions of thebody)
c. Enlargement or swelling of the liver (hepatomegaly)d. Buildup of fluid in the abdominal cavity (ascites)e. Edema of the skin and soft tissues, causing swelling of the feet, ankles, and legsf. Excessive urination at night caused by fluid redistribution while a person is
sleeping lying down (nocturia)
-
8/13/2019 CHF in English
12/58
12
E. ETIOLOGYCongestive heart failure (CHF) is a syndrome that can be brought about by several causes.
Congestive heart failure is a weakening of the heart caused by an underlying heart or blood
vessel problem, or a combination of several different problems, including the following:
1. Weakened heart muscle (cardiomyopathy)2. Damaged heart valves3. Blocked blood vessels supplying the heart muscle (coronary arteries), which may lead
to a heart attack (This is known as ischemic cardiomyopathy. If there are other,
noncoronary causes, these are collectively termed nonischemic cardiomyopathy.)
4. Toxic exposures, such as alcohol or cocaine5. Infections, commonly viruses, which for unknown reasons affect the heart in only
certain individuals
6. High blood pressure that results in thickening of the heart muscle (left ventricularhypertrophy)
7. Congenital heart diseases8. Certain genetic diseases involving the heart9. Prolonged, serious arrhythmias10.
A variety of less common disorders in which the heart muscle is infiltrated by adisease process.
11.Heart failure can happen at any age, but it is more common in older people. As weage, our heart becomes a little weaker and the blood vessels get narrower.
12.Heart valve disease can also cause heart failure. The blood may leak back through adefective valve, causing the heart to work harder and blood and fluids to collect in the
lungs
13.Hypertension, or high blood pressure, increases the workload of the heart over time.This can lead to heart failure, as well.
14.Coronary artery disease can cause heart failure. Coronary artery disease developswhen fatty materials deposit in the coronary arteries. This causes the blood vessels of
the heart to become narrow and clogged.
15.Heart attacks may cause heart failure. Because part of the heart muscle is damaged ina heart attack, the heart pumps less effectively, which in turn may lead to congestive
heart failure.
16.In some cases, the heart gets infected or infalmed; this causes it to weaken, a conditioncalled cardiomyopathy. This may also result in congestive heart failure.
http://www.emedicinehealth.com/script/main/art.asp?articlekey=107600http://www.emedicinehealth.com/script/main/art.asp?articlekey=107600 -
8/13/2019 CHF in English
13/58
13
17.Other causes of heart failure include :a. Diabetes
b. Cancer treatment, radiation and some chemotherapy drugsc. Thyroid diseases, too much or too little thyroid hormonesd. Alcohol abuse.
There are over a hundred other less common causes of heart failure, which include a
variety of infections, exposures (such as radiation or chemotherapy), endocrine disorders
(including thyroid disorders), complications of other diseases, toxic effects, and genetic
predisposition. However, the cause of congestive heart failure is often idiopathic, or unknown.
People who have diabetes are at increased risk for both ischemic and nonischemic heart
failure. Congestive heart failure may be exacerbated by the following lifestyle habits:
1. Unhealthy habits, such assmoking and excessive use of alcohol2. Obesity and lack ofexercise (May contribute to congestive heart failure, either directly
or indirectly through accompanying high blood pressure, diabetes, and coronary artery
disease.)
3. High salt intake, which may cause more fluid retention4. Noncompliance with medications and other therapies
Whether through disease and/or complicating lifestyle choices, the pumping action of the
heart can be impaired by several physiologic mechanisms:
1. Direct heart muscle damage (cardiomyopathy):The heart muscle can become weakbecause of damage or disease and thus does not contract or squeeze as forcefully as it
should. This damage to the muscle can occur from any of the diseases mentioned
above, but sometimes, the cause is unknown.2. Damage to heart muscle due to blockage: When the coronary blood supply is
blocked, this results in a heart attack (myocardial infarction). A heart attack commonly
causes severe pain in the chest, shortness of breath, nausea, sweating, and/or a feeling
of impending doom. A heart attack may rapidly lead to either cardiac arrest (no
heartbeat) or permanent damage to the left ventricle. If this damage is bad enough, that
part of the heart will not work properly, which leads to heart failure. Prompt
(emergency) medical attention is critical for all heart attacks.
http://www.emedicinehealth.com/script/main/art.asp?articlekey=117701http://www.emedicinehealth.com/script/main/art.asp?articlekey=58855http://www.emedicinehealth.com/script/main/art.asp?articlekey=58939http://www.emedicinehealth.com/script/main/art.asp?articlekey=58700http://www.emedicinehealth.com/script/main/art.asp?articlekey=105801http://www.emedicinehealth.com/script/main/art.asp?articlekey=105801http://www.emedicinehealth.com/script/main/art.asp?articlekey=58700http://www.emedicinehealth.com/script/main/art.asp?articlekey=58939http://www.emedicinehealth.com/script/main/art.asp?articlekey=58855http://www.emedicinehealth.com/script/main/art.asp?articlekey=117701 -
8/13/2019 CHF in English
14/58
14
3. High blood pressure (hypertension):Abnormally high blood pressure increases theamount of work the left ventricle has to do to pump blood out to the circulatory
system. Over time, this greater workload can damage and weaken the heart, leading to
heart failure. Proper treatment of high blood pressure can prevent left ventricular
failure.
4. Heart valve problems:The valves of the heart normally keep the blood flowing inthe proper direction through the heart. Abnormal heart valves impede this forward
flow in one of two ways:
a. An incompetent valve is a valve that does not close properly when it should andallows blood to flow backward in the heart, "against the current." When blood
flows the wrong way across a valve, the heart has to work harder to keep up its
output. Eventually, this backed up blood accumulates in the lungs and the bodyand the heart muscle weakens.
b. A stenotic valve is a valve that does not open properly. Blood flow through thenarrowed opening is blocked, creating an increased workload on the heart that can
also lead to heart failure.
5. Abnormal rhythm or irregular heartbeat:Abnormal heart rhythms can lower theheart's effectiveness as a pump. The rhythm may be too slow or too fast, or irregular.
The heart has to pump harder to overcome these rhythm disorders. If this excessively
slow or fast heartbeat is sustained over hours, days, or weeks, the heart can weaken,
which may lead to heart failure.
F. PATHOPHYSIOLOGYHeart failure is caused by any condition which reduces the efficiency of the myocardium,
or heart muscle, through damage or overloading. As such, it can be caused by as diverse an
array of conditions as myocardial infarction (in which the heart muscle is starved of oxygen
and dies), hypertension (which increases the force of contraction needed to pump blood) and
amyloidosis (in which protein is deposited in the heart muscle, causing it to stiffen). Over
time these increases in workload will produce changes to the heart itself:
1. Reduced contractility, or force of contraction, due to overloading of the ventricle. Inhealth, increased filling of the ventricle results in increased contractility (by the Frank-
Starling law of the heart) and thus a rise in cardiac output. In heart failure this
mechanism fails, as the ventricle is loaded with blood to the point where heart muscle
http://www.news-medical.net/health/Heart-Failure.aspxhttp://www.news-medical.net/health/Heart-Failure.aspx -
8/13/2019 CHF in English
15/58
15
contraction becomes less efficient. This is due to reduced ability to cross-link actin
and myosin filaments in over-stretched heart muscle.
2. A reducedstroke volume, as a result of a failure of systole, diastole or both. Increasedend systolic volume is usually caused by reduced contractility. Decreased end diastolic
volume results from impaired ventricular filling as occurs when the compliance of
the ventricle falls (i.e. when the walls stiffen).
3. Reduced spare capacity. As the heart works harder to meet normal metabolicdemands, the amount cardiac output can increase in times of increased oxygen demand
(e.g. exercise) is reduced. This contributes to the exercise intolerance commonly seen
in heart failure. This translates to the loss of one's cardiac reserve. The cardiac reserve
refers to the ability of the heart to work harder during exercise or strenuous activity.
Since the heart has to work harder to meet the normal metabolic demands, it isincapable of meeting the metabolic demands of the body during exercise.
4. Increasedheart rate,stimulated by increased sympathetic activity in order to maintaincardiac output. Initially, this helps compensate for heart failure by maintaining blood
pressure and perfusion, but places further strain on the myocardium, increasing
coronary perfusion requirements, which can lead to worsening of ischemic heart
disease. Sympathetic activity may also cause potentially fatal arrhythmias.
5. Hypertrophy (an increase in physical size) of the myocardium, caused by theterminally differentiated heart muscle fibres increasing in size in an attempt to
improve contractility. This may contribute to the increased stiffness and decreased
ability to relax during diastole.
6. Enlargement of the ventricles, contributing to the enlargement and spherical shape ofthe failing heart. The increase in ventricular volume also causes a reduction in stroke
volume due to mechanical and contractile inefficiency.
The general effect is one of reduced cardiac output and increased strain on the heart. This
increases the risk ofcardiac arrest (specifically due to ventricular dysrhythmias), and reduces
blood supply to the rest of the body. In chronic disease the reduced cardiac output causes a
number of changes in the rest of the body, some of which are physiological compensations,
some of which are part of the disease process:
1. Arterial blood pressure falls. This destimulates baroreceptors in the carotid sinus andaortic arch which link to the nucleus tractus solitarius. This center in the brain
increases sympathetic activity, releasing catecholamines into the blood stream.
http://www.news-medical.net/health/What-is-a-Stroke.aspxhttp://www.news-medical.net/health/What-is-Heart-Rate.aspxhttp://www.news-medical.net/health/What-is-Cardiac-Arrest.aspxhttp://www.news-medical.net/health/The-Human-Brain.aspxhttp://www.news-medical.net/health/The-Human-Brain.aspxhttp://www.news-medical.net/health/What-is-Cardiac-Arrest.aspxhttp://www.news-medical.net/health/What-is-Heart-Rate.aspxhttp://www.news-medical.net/health/What-is-a-Stroke.aspx -
8/13/2019 CHF in English
16/58
16
Binding to alpha-1 receptors results in systemic arterial vasoconstriction. This helps
restore blood pressure but also increases the total peripheral resistance, increasing the
workload of the heart. Binding to beta-1 receptors in the myocardium increases the
heart rate and make contractions more forceful, in an attempt to increase cardiac
output. This also, however, increases the amount of work the heart has to perform.
2. Increased sympathetic stimulation also causes thehypothalamus to secrete vasopressin(also known as antidiuretic hormone or ADH), which causes fluid retention at the
kidneys. This increases the blood volume and blood pressure.
3. Reduced perfusion (blood flow) to the kidneys stimulates the release of renin anenzyme which catalyses the production of the potent vasopressor angiotensin.
Angiotensin and itsmetabolites cause further vasocontriction, and stimulate increased
secretion of the steroid aldosterone from the adrenal glands.This promotes salt andfluid retention at the kidneys, also increasing the blood volume.
4. The chronically high levels of circulating neuroendocrine hormones such ascatecholamines, renin, angiotensin, and aldosterone affects the myocardium directly,
causing structural remodelling of the heart over the long term. Many of these
remodelling effects seem to be mediated by transforming growth factor beta (TGF-
beta), which is a common downstream target of the signal transduction cascade
initiated by catecholamines and angiotensin II, and also by epidermal growth factor
(EGF), which is a target of the signaling pathway activated by aldosterone
5. Reduced perfusion of skeletal muscle causes atrophy of the muscle fibres. This canresult in weakness, increased fatigueability and decreased peak strength - all
contributing to exercise intolerance.
The increased peripheral resistance and greater blood volume place further strain on the
heart and accelerates the process of damage to the myocardium. Vasoconstriction and fluid
retention produce an increased hydrostatic pressure in the capillaries. This shifts of the
balance of forces in favour of interstitial fluid formation as the increased pressure forces
additional fluid out of the blood, into the tissue. This results inedema (fluid build-up) in the
tissues. In right-sided heart failure this commonly starts in the ankles where venous pressure
is high due to the effects of gravity (although if the patient is bed-ridden, fluid accumulation
may begin in the sacral region.) It may also occur in the abdominal cavity, where the fluid
build-up is called ascites. In left-sided heart failure edema can occur in the lungs - this is
called cardiogenic pulmonary oedema. This reduces spare capacity for ventilation, causesstiffening of the lungs and reduces the efficiency of gas exchange by increasing the distance
http://www.news-medical.net/health/What-is-the-Hypothalamus.aspxhttp://www.news-medical.net/health/What-are-Hormones.aspxhttp://www.news-medical.net/health/Renin-What-is-Renin.aspxhttp://www.news-medical.net/health/Metabolites-What-are-Metabolites.aspxhttp://www.news-medical.net/health/What-Does-the-Adrenal-Gland-Do.aspxhttp://www.news-medical.net/health/What-are-Hormones.aspxhttp://www.news-medical.net/health/Edema-What-is-Edema.aspxhttp://www.news-medical.net/health/Heart-Failure.aspxhttp://www.news-medical.net/health/Heart-Failure.aspxhttp://www.news-medical.net/health/Edema-What-is-Edema.aspxhttp://www.news-medical.net/health/What-are-Hormones.aspxhttp://www.news-medical.net/health/What-Does-the-Adrenal-Gland-Do.aspxhttp://www.news-medical.net/health/Metabolites-What-are-Metabolites.aspxhttp://www.news-medical.net/health/Renin-What-is-Renin.aspxhttp://www.news-medical.net/health/What-are-Hormones.aspxhttp://www.news-medical.net/health/What-is-the-Hypothalamus.aspx -
8/13/2019 CHF in English
17/58
-
8/13/2019 CHF in English
18/58
18
Systolic dysfunction
Heart failure caused by systolic dysfunction is more readily recognized. It can be
simplistically described as failure of the pump function of the heart. It is characterized by a
decreased ejection fraction (less than 45%). The strength of ventricular contraction is
attenuated and inadequate for creating an adequate stroke volume, resulting in inadequate
cardiac output. In general, this is caused by dysfunction or destruction of cardiac myocytes or
their molecular components. In congenital diseases such as Duchennemuscular dystrophy,the
molecular structure of individual myocytes is affected. Myocytes and their components can be
damaged by inflammation (such as inmyocarditis)or by infiltration (such as in amyloidosis).
Toxins and pharmacological agents (such as ethanol, cocaine, and amphetamines) causeintracellular damage and oxidative stress. The most common mechanism of damage is
ischemia causing infarction and scar formation. After myocardial infarction, dead myocytes
are replaced by scar tissue, deleteriously affecting the function of the myocardium. On
echocardiogram, this is manifest by abnormal or absent wall motion.
Because the ventricle is inadequately emptied, ventricular end-diastolic pressure and
volumes increase. This is transmitted to the atrium. On the left side of the heart, the increased
pressure is transmitted to the pulmonary vasculature, and the resultant hydrostatic pressure
favors extravassation of fluid into the lung parenchyma, causing pulmonary edema. On the
http://www.news-medical.net/health/What-is-Muscular-Dystrophy.aspxhttp://www.news-medical.net/health/What-is-Myocarditis.aspxhttp://www.news-medical.net/health/What-is-Oxidative-Stress.aspxhttp://www.news-medical.net/health/What-is-Oxidative-Stress.aspxhttp://www.news-medical.net/health/What-is-Myocarditis.aspxhttp://www.news-medical.net/health/What-is-Muscular-Dystrophy.aspx -
8/13/2019 CHF in English
19/58
19
right side of the heart, the increased pressure is transmitted to the systemic venous circulation
and systemic capillary beds, favoring extravassation of fluid into the tissues of target organs
and extremities, resulting in dependent peripheraledema.
Diastolic dysfunction
Heart failure caused by diastolic dysfunction is generally described as the failure of the
ventricle to adequately relax and typically denotes a stiffer ventricular wall. This causes
inadequate filling of the ventricle, and therefore results in an inadequate stroke volume. The
failure of ventricular relaxation also results in elevated end-diastolic pressures, and the end
result is identical to the case of systolic dysfunction (pulmonary edema in left heart failure,
peripheral edema in right heart failure.)
Diastolic dysfunction can be caused by processes similar to those that cause systolic
dysfunction, particularly causes that affect cardiac remodeling.
Diastolic dysfunction may not manifest itself except in physiologic extremes if systolic
function is preserved. The patient may be completely asymptomatic at rest. However, they are
exquisitely sensitive to increases in heart rate, and sudden bouts of tachycardia (which can be
caused simply by physiological responses to exertion, fever, or dehydration, or by
pathological tachyarrhythmias such asatrial fibrillation with rapid ventricular response) may
result in flash pulmonary edema. Adequate rate control (usually with a pharmacological agent
that slows down AV conduction such as a calcium channel blocker or a beta-blocker) is
therefore key to preventing decompensation.
Left ventricular diastolic function can be determined through echocardiography by
measurement of various parameters such as the E/A ratio (early-to-atrial left ventricular filling
ratio), the E (early left ventricular filling) deceleration time, and the isovolumic relaxationtime.
http://www.news-medical.net/health/Edema-What-is-Edema.aspxhttp://www.news-medical.net/health/Dehydration-What-is-Dehydration.aspxhttp://www.news-medical.net/health/Atrial-fibrillation-%28AF%29.aspxhttp://www.news-medical.net/health/Calcium-What-is-Calcium.aspxhttp://www.news-medical.net/health/What-are-Beta-Blockers-Used-for.aspxhttp://www.news-medical.net/health/What-are-Beta-Blockers-Used-for.aspxhttp://www.news-medical.net/health/Calcium-What-is-Calcium.aspxhttp://www.news-medical.net/health/Atrial-fibrillation-%28AF%29.aspxhttp://www.news-medical.net/health/Dehydration-What-is-Dehydration.aspxhttp://www.news-medical.net/health/Edema-What-is-Edema.aspx -
8/13/2019 CHF in English
20/58
20
-
8/13/2019 CHF in English
21/58
21
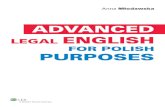
G. PATHOFLOWNon modifiable factors : modifiable factor :
Increase in age 55 years old in above sedentary lifestyle Gender
Decreased elasticity of blood and formation of plaques on blood vessels
Narrowing of the blood vessels
Necrosis and scarring of the vascular endothelium
Im ediment of blood flow to the bod
Increased work load of the heart
Dilatation of ventricles
Increased in reload
Increased stretchin of m ocardial muscle
Excessive stretchin of m ocardial muscle
Ineffective cardiac muscle contraction
Decreased contraction of cardiac muscle
Activation of neurohormonal pathways in order to increase circulating blood
Continued neurohormonal stimulation
Cardiac remodeling
Decreased blood filling
-
8/13/2019 CHF in English
22/58
-
8/13/2019 CHF in English
23/58
23
H. TEST1. Laboratory tests. Low serum sodium is common (dilutional hyponatremia from
expansion of extracellular fluid volume) and predictive of poor outcome; elevated
creatinine and liver function tests also are predictors of poor outcome.
2. Chest radiograph. Finding of increased pulmonary capillary pressure are seen inapproximately 50% of patients; bilateral pleural effusion and cardiomegaly also may
be present.
3. Electrocardiography (ECG). Q waves and left bundle branch block are good predictorsof systolic dysfunction. A wide QRS (more than 220 milliseconds) is predictive of
increased mortality.
4. Echocardiogram. A simple and useful tool, echocardiography can help determinesystolic versus diastolic dysfunction and left and/or right ventricular impairment.
5. Six minute walk test. Short distance correlates with higher mortality and increasedHF-related hospitalizations
6. Metabolic stress testing. Used to measure oxygen consumption; a peak oxygenconsumption of less than 12 to 14 mL/kg/min portends a poor prognosis.
-
8/13/2019 CHF in English
24/58
24
7. Endomyocardial biopsy. Biopsy may be useful in selected cases, such as suspectedamyloidosis, sarcoidosis, and giant cell myocarditis.
I. TREATMENTAcute
1. Nitrates. Nitrates are given sublingually or intravenously in cases in which preloadreduction is necessary. In the case of severe HF, nitroprusside administration should
be considered if both PCWP systemic vascular resistance (SVR) are elevated
2. Nesiritide. This from of human B-type natriuretic peptide causes vasodilation andincrease renal blood flow and urine output and has resulted in rapid symptomatic and
hemodynamic improvement in patiens with acutely decompenseted HF.
3.
Diuretics. Furosemide, 20 to 200 mg, is administered intravenously to alleviate lungedema due to volume overload, again by reducung preload. Addition of a thiazide (e.g
metolazone or chlorothiazide) may help potentiate diuresis. In cases of massive fluid
overload that spon poorly to diuretics, ultrafiltration may be effective.
4. Inotropic agents. No single agent has been found to be clinically superior, butadrenegric agents (such as dobutamine and dopamin and the phosphodiesterase
inhibitor, milrinone) each may have a role in certain hemodynamic states. Dopamin
may be preferable in those with low blood pressure because dobutamine reduces SVR
to a greater extent. (evidence based cardiology, peter J sharis,2003, lippincot william
and wilkins, philadelphia, USA).
J. HEART FAILURE MANAGEMENTTreatment focuses on improving the symptoms and preventing the progression of the
disease. Reversible causes of the heart failure also need to be addressed: (e.g. infection,
alcohol ingestion, anemia, thyrotoxicosis, arrhythmia, hypertension). Treatments includelifestyle and pharmacological modalities.
http://www.news-medical.net/health/Heart-Failure-Management.aspxhttp://www.news-medical.net/health/Heart-Failure.aspxhttp://www.news-medical.net/health/Heart-Failure.aspxhttp://www.news-medical.net/health/Heart-Failure-Management.aspx -
8/13/2019 CHF in English
25/58
25
Acute decompensation
In acute decompensated heart failure (ADHF), the immediate goal is to re-establish
adequate perfusion and oxygen delivery to end organs. This entails ensuring that airway,
breathing, and circulation are adequate. Immediated treatments usually involve some
combination of vasodilators such as nitroglycerin,diuretics such as furosemide, and possibly
non invasive positive pressure ventilation (NIPPV).
Chronic management
The goal is to prevent the development of acute decompensated heart failure, to counteract
the deleterious effects of cardiac remodeling, and to minimize the symptoms that the patient
suffers. In addition to pharmacologic agents (oral loop diuretics, beta-blockers, ACE
inhibitors or angiotensin receptor blockers, vasodilators, and in severe cardiomyopathy
aldosterone receptor antagonists), behavioral modification should be pursued, specifically
with regards to dietary guidelines regarding salt and fluid intake. Exercise should be
encouraged as tolerated, as sufficient conditioning can significantly improve quality-of-life.
In patients with severe cardiomyopathy, implantation of an automatic implantable
cardioverterdefibrillator(AICD) should be considered. A select population will also probably
benefit from ventricular resynchronization. In select cases, cardiac transplantation can be
considered. While this may resolve the problems associated with heart failure, the patient
generally must remain on an immunosuppressive regimen to prevent rejection, which has its
own significant downsides.
Palliative care and hospice
Without transplantation, heart failure caused by ischemic heart disease is not reversible,
and cardiac function typically deteriorates with time. (In particular, diastolic function worsensas a function of age even in individuals without ischemic heart disease.) The growing number
of patients with Stage Dheart failure (intractable symptoms of fatigue, shortness of breath or
chest pain at rest despite optimal medical therapy) should be considered forpalliative care or
hospice, according to American College of Cardiology/American Heart Association
guidelines.
http://www.news-medical.net/health/Diuretic-What-is-a-Diuretic.aspxhttp://www.news-medical.net/health/What-are-Beta-Blockers-Used-for.aspxhttp://www.news-medical.net/health/ACE-Inhibitors-What-are-ACE-Inhibitors.aspxhttp://www.news-medical.net/health/ACE-Inhibitors-What-are-ACE-Inhibitors.aspxhttp://www.news-medical.net/health/What-is-Cardiomyopathy.aspxhttp://www.news-medical.net/health/Defibrillator-What-is-a-Defibrillator.aspxhttp://www.news-medical.net/health/Heart-Failure.aspxhttp://www.news-medical.net/health/Palliative-Care-What-is-Palliative-Care.aspxhttp://www.news-medical.net/health/Cardiology-What-is-Cardiology.aspxhttp://www.news-medical.net/health/Cardiology-What-is-Cardiology.aspxhttp://www.news-medical.net/health/Palliative-Care-What-is-Palliative-Care.aspxhttp://www.news-medical.net/health/Heart-Failure.aspxhttp://www.news-medical.net/health/Defibrillator-What-is-a-Defibrillator.aspxhttp://www.news-medical.net/health/What-is-Cardiomyopathy.aspxhttp://www.news-medical.net/health/ACE-Inhibitors-What-are-ACE-Inhibitors.aspxhttp://www.news-medical.net/health/ACE-Inhibitors-What-are-ACE-Inhibitors.aspxhttp://www.news-medical.net/health/What-are-Beta-Blockers-Used-for.aspxhttp://www.news-medical.net/health/Diuretic-What-is-a-Diuretic.aspx -
8/13/2019 CHF in English
26/58
-
8/13/2019 CHF in English
27/58
27
since these patients are at higher risk for serious ventricular arrhythmias. In these
circumstances, an ICD may be implanted as part of a pacemaker device. This
defibrillator can detect and electrically shock a life-threatening arrhythmia back to
normal.
Cardiac Resynchronization Therapy (CRT):This involves a biventricular pacemaker
that is used to synchronize the pumping action of the left and right ventricles. Synchronization
improves the effectiveness of the heart as a pump, since with heart failure the pumping action
is sometimes uncoordinated.
1. One pacer lead is placed in a coronary vein on the back side of the heart, overlying theleft ventricle. The other pacer is placed in the usual right ventricular position. This
improves the coordination of contraction between the left and right ventricle,
especially if the patient has left bundle branch block (LBBB). In LBBB, the electrical
signal to the left ventricle is delayed.
2. Biventricular pacing has been shown to improve exercise capacity, preventprogression of heart failure symptoms, and prolong life in certain patients.
3. Cardiac resynchronization therapy is frequently combined with an ICD to shock aperson out of life-threatening arrhythmias, such as ventricular tachycardia or
ventricular fibrillation. The worse the function of the left ventricle, the higher the risk
for sudden death secondary to these arrhythmias.
Temporary Cardiac Support: An intra-aortic balloon pump is used as a temporary
support of left ventricle function, such as in a large heart attack, waiting for the heart to
recover. There are other similar devices that can be used to temporarily support the heart if
there is something that can be done for the underlying heart failure.
L. COMPLICATIONS OF HEART FAILURECongestive heart failure is caused by circulatory congestion myocardium dysfunction.
Place of congestion depends on the involved ventricle. Left ventricular dysfunction or heart
failure, left, causing congestion in the pulmonary vein, whereas right ventricular dysfunction
or right heart failure resulting in systemic venous congestion. Failure in both ventricles called
biventricular failure. Left heart failure is a mechanical complication of the most common after
myocardial myocardium,
-
8/13/2019 CHF in English
28/58
28
M.PHYSICAL EXAMINATION
N. NURSING CARE1. PATIENT ASSESSMENT DATA BASE
a. ACTIVITY/REST1)May report: Fatigue/exhaustion progressing throughout the day, Insomnia,
Chest pain with activity, Dyspnea at rest or with exertion
2)May exhibit: restlessness, mental status changes, e.g., lethargy, Vital signchanges with activity.
b. CIRCULATION1)May report: History of hypertension, recent/acute multiple Mls, previous
episodes of CHF, valvular heart disease, cardiac surgery, endocarditis, SLE,
anemia, septic shock. Swelling of feet, legs, abdomen, belt too tight (right-
sided failure).
2)May exhibit: BP: May be low (pump failure); normal (mild chronic CHF); orhigh (fluid overload/increased SVR). Pulse pressure: May be narrow, reflectingreduced stroke volume. Heart rate: Tachycardia (left-sided failure). Heart
-
8/13/2019 CHF in English
29/58
29
rhytm: Dysrhytmias; e.g., atrial fibrillation, premature ventricular
contractions/tachycardia, heart blocks. Apical pulse: PMI msy be diffuse and
displaced inferiorly to the left. Heart sounds: S3 (gallop) is diagnostic; S4 may
occur; S1 and S2 may be softened.
Systolic and diastolic murmur may indicate the presence of valvular stenosis or
insufficiency. Pulse : Peripheral pulses diminished; alteration in strength of
beat may be noted; central pulses may be bounding, e.g., visible jugular,
carotid, abdominal pulsations.
Color: Ashen, pale, dusky, cyanotic. Nailbeds: Pale or cyanotic with slow
capillary refill. Liver: Enlarged/palpable, positive hepatojugular reflex. Breath
sound: Crackles, ronchi. Edema: May be dependent, genelized, or pitting,
especially in extremities; JVD.c. EGO INTEGRITY
1)May report: Anxiety, apprehension, fear. Stress related to illness/financialconcerns (job/cost of medical care).
2)May exhibit: Various behavioral manifestations, e.g., anxiety, anger, fearful,irritable.
d. ELIMINATION1)May report: Decreased voiding, dark urine Night voiding (nocturia).
Diarrhea/constipation.
e. FOOD/FLUID1)May report: Loss of appetite. Nausea/vomiting. Significant weight gain.
Lower extremity swelling. Tight clothing/shoes. Diet high in salt/processed
foods, fat, sugar, and caffeine. Use of diuretics.
2)May exhibit: Rapid weight gain. Abdominal distention (ascites); edema(general, dependent, brawn, pitting).
f. HYGIENE1)May report: Fatigue/weakness, exhaustion during self-care activities.2)May exhibit: Appearance indicative of neglect of personal care.
g. NEUROSENSORY1)May report: Weakness, dizziness, fainting episodes.2)May exhibit: Lethargy, confusion, disorientation. Behavior changes,
irritability.
-
8/13/2019 CHF in English
30/58
30
h. PAIN/ DISCOMFORT1) May report: Chest Pain, chronic or acute angina. Right upper abdominal
pain (RVF). Muscle aches.
2) May exhibit: Nervousness, restlessness.. Narrowed focus (withdrawal)i. RESPIRATION
1) May report: Dyspnea on exertion, sleeping sitting up, or with severalpillows. Cough with/ without sputum production. History of chronic lung
disease. Use of respiratory aids, e.g., oxygen or medications.
2) My exhibit: Respiration: Tachypnea; shallow, labored breathing; use ofaccessory muscles, nasal flaring. Cough: Dry/ hacking/ nonproductive or may
be gurgling with/ without sputum production. Sputum: may be blood-tinged,
pink/ frothy (pulmonary edema). Breath sounds: may be diminished, withbibasilar crackles and wheezes. Mentation: may be diminished; lethargy;
restlessness. Color: pallor or cyanosis.
j. SAFETY1) May exhibit: Changes in mention. Loss of strength/ muscle tone. Skin
excoriations.
k. SOCIAL INTERACTION1) May report: Decreased participation in usual social activities.
l. TEACHING/ LEARNING1) Mar report: Use/ misuse of cardiac medication, e.g.; -blockers, calcium
channel blockers. Recent/ recurrent hospitalizations.
2) May exhibit: evidence of failure to improve.
2. Discharge planConsiderations: DRG projected mean length of stay: 8.2 days
a. Assistance with shopping, transportation, self-care needs, homemaker/maintenance tasks.
b. Alteration in medication use/ therapy.c. Changes in physical layout of home.
-
8/13/2019 CHF in English
31/58
-
8/13/2019 CHF in English
32/58
32
Rationale: s and may be weak because of diminished pumping
action. Gallop rhythms are common and ), produced as blood flows
into noncompliant / distended chambers. Murmurs may reflect valvular
incompetence / stenosis.
c) Palpate peripheral pulsesRationale : decreased cardiac output may be reflected in diminished radial,
popliteal, dorsalis pedis, and posttibial pulses. Pulses may be fleeting or
irregular to palpitation, and pulsus alternans (strong beat alternating with
weak beat) may be present.
d) Monitor BPRationale: in early, moderate, or chronic CHF, BP may be elevated due to
increased SVR. In advanced CHF, the body may no longer be able tocompensate, and profound / irrefersible hypotension may occur.
e) Inspect skin for pallor, cyanosisRationale: pallor is indicative of diminished peripheral Perfusion
secondary to inadequate cardiac output, vasoconstriction, and anemia.
Cyanosis may develop min refractory CHF. Dependend areas are often
blue or mottled as venous congestion increases.
f) Monitor urine output, nothing decreasing output and dark / concentratedurine.
Rationale:, kidneys respond to reduced cardiac output by retaining water
and sodium. Urine output is usually decreased during the day because of
fluid shifts into tissues but may be increased at night as fluid returns to
circulation when patient is recumbent.
g) Assess changes in sensorium, e, g, lethargy, perfusion con-Fusion,disorientation, anxiety, and depression.
Rationale :may indicate inadequate cerebral perfusion secondary to
decreased cardiac output.
h) Provide rest semirecubent in bed chair. Assist with physical rest asindicated.
Rationale : physical rest should be maintained during acute Or refractory
CHF to improve efficiency of Cardiac contraction and to decrease
myocardial Oxygen demand / consumption and workload.
-
8/13/2019 CHF in English
33/58
33
i) Provide for psychologic rest by quit environment; Explaining medical /nursing management; helping patient avoid stressful situations, listening /
responding to expressions of feelings / fears.
Rationale :emotional stress produces vasoconstriction, which elevates BP
and increases heart rate / work.
j) Provide bedside commode. Have patient avoid Activities eliciting avalsalve response, e.g., Straining during defecation, holding breath During
position changes.
Rationale : commode use decreases work of getting to bathroom or
struggling to use bedpan.Valsalva maneuver causes vegal stimulation
followed by rebound tachycardia, which further compromises cardiac
function/output.k) Elevate legs, avoiding pressure under knee. Encourage active/passive
exercises. Increase ambulation/ activity as tolerated.
Rationale : Decreases venous stasis and may reduce incidence of
thrombus/embolus formation.
l) Check for calt tenderness, diminished pedal pulse Swelling . local redness,or pallor of extremity.
Rationale :reduced cardiac output, venous pooling/stasis and enforced
bedrest increases risk of trombohlebitis.
m)Withhold digitalis preparation and notify physician It marked changesoccur in cardiac rate or rhythm Or signs of digitalis toxicity occur.
Rationale : incidence of toxicity is high (20%) because of narrow
margin between therapeutic and Toxic ranges. Digoxin may have to be
disontinued in the presence of toxic drug levels, a slow heart rate or low
postassium level.
Collaborative
a) Administer supplemental oxgen by nasal can- uptake Nula/mask asindicated.
Rationale :increases avaible oxygen for myocardial To combat effects
of hypoxia/ ischemia.
b) Administer medications as indicated:Rationale :a variety of medications may be used to increase stroke
volume, improve contractility, and reduce congestion.
-
8/13/2019 CHF in English
34/58
34
1. diuretics, e.g., furosemide (lasix); ethacrynic acid (Edecrin);bumetanide (Bumex); supironolactone (Aldoctone)
Rationale :type and dosage of diuretic depends on degree of heart
failure and state of renal function. Preload reduction is most useful in
treating patients with a relatively normal cardiac output accompanied
by congestive symptoms. loop diuretics block chloride reabsorption,
thus interfering with the reabsorption of sodium and water.
2. vasodilators, e.g, nitrates (Nitro-Dur, Isordil);arteriodilators, e.g.,hydralazine (Apresoline); combination drugs, e.g., prazosin
(Minipress);;
Rationale :vasodilators are used to increase cardiac output, reducing
circulating volume (venodilators) and decreasing systemic vascularresistence (arteriodilators), thereby reducing ventricular workload.
3. digoxin (lanoxin);Rationale : increases force of myocardial contraction and slows heart
rate by decreasing conduction velocity and prolonging refractory period
of the AV junction to increase cardiac efficiency/output.
4. captopril (Capeton); lisinopril (prinvil); enalapril (vasotec);Rationale :ACE inhibitors may be used to control heart failure by
inhibiting angiotension conversion in the lungs and reduce
vasoconstriction, SVR, and BP.
5. Morphine sulfate;Rationale :decreases vascular resistance and venous return reducing
myocardial workload. Allays anxiety and breaks the feedback cycle of
anxiety/catecholamine release/anxiety.
6. Tranquilizers/sedatives;Rationale : promotes rest/relaxation reducing oxygen demand and
myocardial workload. note ; There is an ontrial oral analogue of
amrinone (inocor) a positive inotropic agent, called milrinone, which
may be suitable for longterm use.
7. Anticoagulants, e.g., low-dose heparin; warfarin (coumadin)Rationale :may be used prophylactically to prevent thrombus/emboli
formation in presence of risk factors such as venous stasis, enforced
bed rest, cardiac dysrhythmias, and history of previous thrombolic
episodes.
-
8/13/2019 CHF in English
35/58
35
c) Administer IV solutions, restricting total amount as indicated. Avoid salinesolutions
Rationale : because of existing elevated left ventricular pressure, patient
may not tolerate increased fluid volume (preload). CHF patients also
execrate less sodium, which cause fluid retention and increases myocardial
workload.
d) Monitor/replace electrolytes.Rationale :fluid shifts and use of diuretics can alter electrolytes (especially
potassium and chloride), which affect cardiac rhythm and contractility.
e) Monitor serial EGC and chest x-ray changesRationale : ST segment depression and T wave flattening can develop
because of increased myocardial oxygen demand, even if no coronaryartery disease is present. Chest x-ray may show enlarged heart and
changes of pulmonary congestion.
f) Monitor laboratory studies, e.g., BUN, creatinine;Rationale : Elevation of BUN/creatinine reflects kidney
hypoperfusion/failure.
1. liver function studies (AST, LDH);Rationale : AST/LDH may be elevated due to liver congestion and
indicate need for smaller dosages of medications that are detoxified by
the liver.
2. PT/APT/coagulation studies.Rationale :measure changes in coagulation processes or effectiveness
of anticoagulant therapy.
g) Prepare for insertion/maintain pacemaker, if indicated.Rationale :may be necessary to correct bradydysrhythmias unresponsive
to drug intervention, which can aggravate congestive failure/produce
pulmonary edema.
h) Prepare for surgery as indicated.Rationale :congestive failure due to ventricular aneurysm or valvular
dysfunction may require aneurysectomy or valve replacement to improve
myocardial contractility/function.
-
8/13/2019 CHF in English
36/58
36
b. Chest PainAcute (Chest) Pain related to myocardial ischemia resulting from coronary artery
occlusion with loss/restriction of blood flow to an area of the myocardium and
necrosis of the myocardium
1) Planning :STG : within 1 hour of nursing interventions, the client will have improved
comfort in chest as evidenced by :
a) States a decrease in the rating of chest painb) Is able to rest displays reduced tension, and sleeps comfortablyc) Requires decrease analgesia or nitroglycerinLTG : The client will have an improved feeling af control as evidenced by
verbalizing a sense of control over present situation and future outcomes
within 2 days of nursing interventions.
2) INTERVENTIONS :Independent:
a) Obtained resting vital signsRationale: Baseline data is important to help determine patients current
health status and evaluate efficacy of nursing interventions rendered.
b) Placed patient on complete bed rest during angina episodes.Rationale:Reduces mycocardial oxygen demand to minimize risk of tissue
injury.
c) Placed patient on semi-Fowlers position.Rationale : Relieves shortness of breath and decreases myocardial
workload.
d) Monitored vital signs q 5 minutes during initial anginal attack.Rationale:Blood pressure may initially rise and then fall if cardiac output
is compromised. Tachycardia also develops and may be sustained if cardiac
output falls.
e) Monitored heart rate and rhythmRationale : Patients with unstable angina have an increased risk of acute
life-threatening dysrhythmias
f) Maintained quiet, comfortable environment; restrict visitors as necessary.Rationale: Mental and emotional stress increases myocardial workload
-
8/13/2019 CHF in English
37/58
37
g) Provided light meals; encouraged patient to rest for 1 hr after mealsRationale: Decreases risk of myocardial attack by decreasing myocardial
workload.
h) Instructed patient to notify nurse immediately if chest pain occurs.Rationale: Pain and decreased cardiac output may complicate and prolong
an angina attack.
i) Provided emotional support.Rationale: Reduces anxiety.
j) Provided client teaching and discharge planning on:1. medication regimen2. ways to minimize
events that precipitate anginal attacks.Rationale :Patient must be taught on the proper use of medications along
with expected side effects (eg. Nitroglycerin). It is also important to
encourage patient to avoid stressful events, quit smoking, avoid
overexertion, have a regular exercise program, and maintain a low-fat, low
cholesterol diet and small, frequent meals.
Dependent:
a) Provided supplemental oxygen as orderedRationale : Increases oxygen available for myocardial uptake/reversal of
ischemia.
b) Administered antianginal medications as orderedRationale : Patients with angina pectoris are given medications that
promote vasodilation (e.g. nitroglycerin), reduce cardiac workload (e.g.
betablockers), reduce coronary artery spasms (e.g. calcium channel
blockers), and relieve pain (e.g. morphine sulfate)
Collaborative:
a) Monitored laboratory and serial ECG resultsRationale :Diagnostic studies such as ECG, ECG stress test, serum lipids,
cardiac enzymes, may be ordered to identify cause of angina pectoris and
other cardiac conditions.
b) Coordinated with dietary department regarding therapeutic diet for patientswith angina pectoris (low fat, low cholesterol).
-
8/13/2019 CHF in English
38/58
38
Rationale :Patients with angina pectoris are maintained on low-fat, low-
saturated cholesterol diet.
c. ACTIVITY INTOLERANCE1) May be related to : Imbalance between oxygen suplay/demand. Generalized
weakness. prolonged bed rest/immobility.
2) possibly evidenced by :Weaknes, fatigue. changes in vital signs, presencedysrhythmias. dyspnea. pallor. diaphoresis.
3) Desired outcomes/evaluation participate in desired activites; meet ownself-
4) Criteria patient will: care needs. Achieve measurable increase in activitytolerance, evidenced by reduced fatigue and weakness and vital signs withim
acceptable limita during activity.
5) Actions/interventionsIndependent
a) Check vital signs before and immediately after activity, especially if patientis on vasodilators, diuretics, or -blockers
Rationale :orthostatic hypotension can occur cause of medication effect
(va shift (dieresis) ; or compromised
b) Document cardiopulmonary response to activity. Note tachycardia,dysrhythmias, dyspnea, diaphoresis, pallor.
Rationale :compromised myocardium/inability to increase stroke volume
during activity may cause an immediate increase in heart rate and oxygen
demands, theraby aggravating weakness and fatigue
c)
Assess for other precipitators/causes of fatigue, e.g , treatments, pain,medications
Rationale :fatigue is aside of some medications (-blockers, tranquilizers,
and sedatives). Pain and stressful regimens also extract energy and produce
fatigue.
d) Evaluate accelerating activity intoleranceRationale : may denote increasing cardiac decompensation rather than
overactivity.
-
8/13/2019 CHF in English
39/58
-
8/13/2019 CHF in English
40/58
40
d) Establish fluid intake schedule, incorporating beverage preferenceswhen possible. Give frequent mouth care/ice chips as part of fluid
allotment.
Rationale : involving patient in therapy regimen may enhancing sense
of control and cooperation with restriction.
e) Weigh dailyRationale : documents changes in/resolution of edema in response to
therapy. A gain of 5 lb represents approximately 2 L of fluid.
Conversely, diuretics can result in rapid/excessive fluid shifts and
weight loss.
f) Assess for distended neck and peripheral vessels. Inspect dependentbody areas for edema with/without pitting; note presence of generalizedbody edema (anasarca).
Rationale : excessive fluid retention may be manifested by venous
engorgement and edema formation.
g) Change position frequently. Elevate feet when sitting. Inspect skinsurface, keep dry and provide padding as indicated.
Rationale : edema formation, slowed circulation, altered nutional intake
and prolonged immobility/bed rest a cumulative stressor which affect
skin integrity arrequire close supervision/preventive intervention
h) Auscultate breath sounds, noting decreased and/ adventition sounds, e.gcrackles, wheezes. Not presence of increased dyspnea, tachypnea,
orthopnea, paroxysmal nocturnal dyspnea, persistent cough.
Rational: Excess fluid volume often leads to pulmonary cogestion.
Symptoms of pulmonary edema may reflect acute left-sided heart
failure. Right-side heart failures respitarory symptoms (dyspnea
cough, orthopnea) may have slower onset but a more difficult to
reverse.
i) Investigate complaints of sudden extreme dypsnea/ air hunger, need tosit stragight up, sensation of suffocation, feelings of panic or impending
doom.
Rational: May indicate development of complications (pulmonary
edema/ embolus) and differs from orthopnea and paroxysmal nocturnal
dyspnea in that develops much more rapidly and requires immetate
intervention.
-
8/13/2019 CHF in English
41/58
41
j) Monitor BP and CVP (if available).Rational: Hypertension and elevated CVP suggests fluid volume excess
and may reflect developing/ increasing pulmonary congestion, heart
failure.
k) Assess bowel sounds. Note complaints of anorexia, nausea, abdominaldistention, constipation.
Rational: Visceral congestion (occurring in progress CHF), can alter
gastric/ intestinal function.
l) Provide small, frequent easily digestible meals.Rational: Reduced gastric motility can adversely affect digestion and
absorption. Small, frequent meals mayenhance digestion/ prevent
abdominal discomfort.m)Measure abdominal girth, as indicated.
Rational: In progressive right-sided heart failure, fluid may shift into
the peritoneal space, causing increasing abdominal girth (ascites).
n) Encaourage verbalization of feelings regarding limitations.Rational: Expression of feelings/ concerns may decreases stress/
anxiety, which is an energy drain and can contribute to feelings of
fatigue.
o) Palpate for hepatomegaly. Note complaints of right upper quadrantpain/ tenderness.
Rational: Advancing heart failure leads to venous congestion, resulting
in andominal distention, liver engorgement, and pain. This can alter
liver function and impair/ prolong drug metabolism.
p) Note increased lethargy, hypotension, muscle cramping.Rational: Signs of potassium and sodium deficits that may occur due to
fluid shifts and diuretic therapy.
Collaborative
Administer medications as indicated:
a) Diuretics, e.g furosemide (Lasix); bumetanide (Bumex).Rational: Increases rate of urine flow and may inhibit reabsorption of
sodium/ chloride in the renal tubules.
b) Thiazides with pottasium-sparing agents, e.g., spironolactone(Aldactone).
Rational: Promotes diuresis without excessive potassium losses.
-
8/13/2019 CHF in English
42/58
42
c) Potassium supplements, e.g., K Dur.Rational : Replaces potassium that is lost as a common side effect of
diuretic therapy, which can adversely affect cardiac function.
d) Maintain fluid/sodium restrictions as indicated.Rational : Reduces total body water/prevents fluid reaccumulation.
e) Consult with dietitian.Rational : May be necessary to provide diet acceptable to patient that
meets caloric needs within sodium restriction.
f) Monitor chest x-ray.Rational : Reveals changes indicative of increase/resolution of
pulmonary congestion.
g)
Assist with rotating tourniquets/phlebotomy, dialysis, or ultrafiltrationas indicated.
Rational : Although not frequently used, mechanical fluid removal may
be carried out to rapidly reduce circulating volume, especially in
pulmonary edema refractory to other therapies.
e. GAS EXCHANGE, IMPAIRED, HIGH RISK FOR1) Risk factors may include : Alveolar-capillary membrane changes, e.g., fluid
collection/shifts into interstitial space/alveoli.
2) Possibly evidenced by : [Not applicable; presence of signs and symptomsestablishes an actual diagnosis.
3) Desired outcomes/evaluation criteria-patient will : Demonstrate adequateventilation and oxygenation of tissues by ABGs/oxymetry within patients
normal ranges and free of symptoms of respiratory distress. Participate in
treatment regimen within level of ability/situation.
4) Actions/interventionsIndependent
a) Auscultate breath sounds noting crackles, wheezes.Rational : Reveals presence of pulmonary congestion/collection of
secretions indicating need for further intervention.
b) Instruct patient in effective coughing, deep breathing.Rational : Clears airways and facilitates oxygen delivery.
c) Encourage frequent position changes.Rational : Helps prevent atelectasis and pneumonia.
-
8/13/2019 CHF in English
43/58
43
d) Maintain chair/bedrest with head-of-bed elevated 20 to 30 degrees, semi-Fowlers position. Support arms with pillows.
Rational : Reduces oxygen consumption/demands and promotes maximal
lung inflation.
Collaborative
a) Monitor/graph serial ABGs, pulse oximetry.Rational : Hypoxemia can be severe during pulmonary edema.
Compensatory changes are usually present in chronic CHF.
b) Administer supplemental oxygen as indicated.Rational : Increases alveolar oxygen concentration, which may
correct/reduce tissue hypoxemia.
c)
Administer medications as indicated :Diuretics, e.g., furosemide (Lasix)
Rational : Reduces alveolar congestion, enhancing gas exchange.
Bronchodilators, e.g., aminophylline.
Rational : Increases oxygen delivery by dilating small airways and exerts
mild diuretic effect to aid in reducing pulmonary congestion.
f. SKIN INTEGRITY, IMPAIRED, HIGH RISK FOR1) Risk factors may include : Prolonged bed rest.2) Possibly evidenced by : [Not applicable; presence of signs and symptoms
establishes an actual diagnosis].
3) Desired outcomes/evaluation criteria-patient will: Demonstratebehaviors/techniques to prevent skin breakdown.
4) Actions/interventionsIndependent
a) Inspect skin, noting skeletal prominences, presence of edema, areas ofaltered circulation/pigmentation, or obesity/emaciation.
Rational : Skin is at risk because of impaired peripheral circulation,
physical immobility, and alterations in nutritional status.
b) Massage reddened or blanched areas.Rational : Improves blood flow, minimizing tissue hypoxia.
c) Reposition frequently in bed/chair, assist with active/passive range ofmotion exercises.
-
8/13/2019 CHF in English
44/58
44
Rational : Improves circulation/reduces time any one area is deprived of
blood flow.
d) Provide frequent skin care, minimize contact with moisture/excretions.Rational : Excessive dryness or moisture damages skin and hastens
breakdown.
e) Check fit of shoes/slippers and change as needed.Rational : Dependent edema may cause shoes to fit poorly, increasing risk
of pressure and skin breakdown on feet.
f) Avoid intramuscular medication.Rational : Interstitial edema and impaired circulation impede drug
absorption and predispose to tissue breakdown/development of infection.
Collaborative :
a) Provide alternating pressure/eggcrate mattress, sheep skin, elbow/heelprotectores.
Rational : Reduces pressure to skin, may improve circulation.
g. KNOWLEDGE DEFICIT (LERNING NEED), REGARDING CONDITION,TREATMENT REGIMEN.
1) May be related to: Lack of understanding/ misconceptions aboutinterrelatedness of cardiac function/ disease/ failure.
2) Possibly evidenced by :a) Questions.
b) Statements of concern/misconceptions.c) Recurrent, preventable episodes of CHF.
3) Desired outcomes/evaluation criteria-patient will :a) Identify relationship of ongoing therapies (treatment program) to
reductionof recurrent episodes and prevention of complications.
b) List signs/symptoms that require immediate intervention.c) Identify own stress/risk factors and some techniques for handling.d) Initiate necessary lifestyle/behavioral changes.
4) Actions/interventionsIndependent
a) Discuss normal heart function. Include information regarding patientsvariance from normal function. Explain difference between heart attack
and CHF.
-
8/13/2019 CHF in English
45/58
45
Rational : Knowledge of disease process and expectations can facilitate
adherence to prescribed treatment regimen.
b) Reinforce treatment rationale.Rational : Patient may believe it is acceptable to alter postdischarge
regimen when feeling well and symptom-free or when feeling below par,
which can increase the risk of exacerbation of symptoms. Understanding of
regimen, medications, and restrictions may augment cooperation with
control of symptoms.
c) Discuss importance of being as active as possible without becomingexhausted and to rest between activities.
Rational : Excessive physical activity can further weaken the heart,
exacerbating failure.d) Discuss importance of sodium limitation. Provide list of sodium content of
common foods that are to be avoided/limited. Encourage reading of labels
on food and drug packages.
Rational : Dietary intake of sodium above 3 g/d will offset diuretic effect.
Most common source of sodium is table salt and obviously salty foods,
although canned soups/vegetables, luncheon meats, and dairy products also
may contain high levels of sodium.
e) Discuss medications, purpose and side effects. Provide both oral andwritten instructions.
Rational : Understanding therapeutic needs and importance of prompt
reporting of side effects can prevent occurrence of drug-related
complications. Anxiety may block comprehension of input or details and
patient/SO may refer to written material at late date to refresh memory.
f) Recommend taking diuretic early in morning.Rational : Provides adequate time for drug effect before bed time to
prevent/limit interruption of sleep.
g) Instruct and receive return demonstration of ability to take and record dailypulse and when to notify health care provider, e.g., pulse above/below
preset rate, changes in rhythm/regularity.
Rational : Promotes self-monitoring of condition/drug effect. Early
detection of changes allows for timely intervention and may prevent
complications, such as digitalis toxicity.
-
8/13/2019 CHF in English
46/58
46
h) Explain and discuss patients role in control of risk factors (e.g., smoking)and precipitating or aggravating factors, (e.g., high salt diet,
inactivity/overexertion, exposure to extremes in temperature).
Rational : Adds to body of knowledge and permits patient to make
informed decisions regarding control of condition and prevention of
recurrence/complications. Smoking potentiates vasoconstriction; sodium
intake promotes water retention/edema formation improper balance
between activity/rest and exposure to extremes in temperature may result in
exhaustion/increased myocardial workload and increased risk of respiratory
infections.
i) Review signs/symptoms that require immediate medical attention, e.g.,rapid weight gain, edema, shortness of breath, increased fatigue, cough,hemoptysis, fever.
Rational : Self-monitoring increases patient responsibility in health
maintenance and aids in prevention of complication, e.g., pulmonary
edema, pneumonia.
j) Provide opportunities for patient/SO to ask questions, discuss concerns andto make necessary lifestyle changes.
Rational : Chronicity and reccurent/debilitating nature of CHF often
exhausts coping abilities and supportives capacity of both patient and SO,
leading to depression.
k) Stress importance of reporting signs/symptoms of digitalis toxicity, e.g.,development of GI and visual disturbances, changes in pulse rate/rhythm,
worsening of congestive failure.
Rational : Early recognition of developing complications and involvement
of health care provider may prevent toxicity/hospitalization.
Collaborative :
Refer to community resources/support groups and Visiting Nurse
Association as indicated.
Rational : May need additional assistance with self monitoring/home
management.
-
8/13/2019 CHF in English
47/58
47
CHAPTER III
CASE REPORT
A. CASE REPORTIdentity1. Client Identity
Name : Mr. F
Age : 57 years old
Address : Jl. Kenanga, No 57, Cilandak, Jakarta Selatan
Phone : 021- 7556432
Religion : Moslem
Education : S1 business management
Occupation/job tittle : CEO of rekayasa company
Nationality : Indonesian
Sex (M/F) : Male
Blood Group : B
Marital status : Married
Entrance Date :May 23, 2012
Reg Number : 238475
2. The Main Complaint : client complains of chest pain and shortness of breath3. Medical History
a. Medical Present History :1) The history of complaint :
He has 2 week history of progressive lower leg edema, chest pain, and
shortness of breath on exertion. He had also experienced a weight loss of
approxiamately 4 kilograms. Shortness of breath and general malaise hadincreased over the 3 days before admission.
2) Predisposing factor :He had a- 20 year history of cigarette smoking
3) Duration :Had chest pain for arround 10 minutes
-
8/13/2019 CHF in English
48/58
48
4) Appear Pattern :Chest pain occurs when the client is doing the activity
5) Bear-down efforts to overcome :Clients overcome the chest pain and shortness of breath with resting
6) Medical Past Historya) Allergy History (drugs, food, animal, environment) :
Clients has not allergy history
b) Accident History :Clients has not accident and hospitalized history
c) History of drugs taking :Clients has not history of drug all this time before he comes to the hospital
7) Medical Family History (genogram and explanation) :Clients families has no heart disease
4. Physical Assesmenta. Eyes system : clients has no problem with his eyes system
b. Ears system : clients has no problem with his ears systemc. Respiratory system : clients has complain that he has a shortness of breath
with respiratory rate 25 times per minute.
d. Cardiovascular system : Clients complain chest pain. He also has a high bloodpressure (140/100). Cardiac examination demonstrated a laterally displaced apex
and fast first and second heart sounds.
e. Hematology system : Clients has no problem with his hematology systemf. Nervous system : Clients has no problem with his nervous systemg. Digestive system : Clients has no problem with his digestive systemh. Endocrine system : Clients has no problem with his endocrine systemi. Urogenitalia system : Clients has no problem with his urogenitalia system
j. Integument system :Clients has no problem with his integument systemk. Musculoskeletal system : clients complain that he felt malaise increased over the
3 days before admission.
-
8/13/2019 CHF in English
49/58
49
5. Supportive Data (diagnostic tests) :a. Hb : 13.4b. HT : 39c. Leukosit : 9.9d. Eritrosit : 4.35e. Trombosit : 450f. Protobintine : 13.2g. Ureum : 30h. Kreatinin : 1.4i. Natrium : 141
j. Kalium : 3.43k.
Chlorida : 105
l. CPK : 161m. CKMB (Lab) : 15n. Troponin T :
-
8/13/2019 CHF in English
50/58
50
In the emergency room, his temperature was 36.3o c, irregular pulse rate 142 per
minute, respiratory rate 25 per minute and blood pressure 140/100 mmHg. Head and neck
examination revealed a symmetrically en large, non-tender thyroid gland. Jugular venous
dilatation was observed. Cardiac examination demonstrated a laterally displaced apex and
fast first and second heart sounds. Murmurs were heard at the apex and left sternal border.
Chest examination revealed few basilar crackles over both lung fields. Moderate ankle
pitting edema was noted bilaterally.
Twelve-lead electrocardiogram (ECG) showed atrial fibrillation (AF) with rapid
ventricular response and diffused ischemic change. His hematology parameters were
normal. The serum total protein and albumin were 6.4 and 3.79/dL respectively.
B.
FOCUS DATA
SUBJECTIVE DATA OBJECTIVE DATA
1. Clients complain chest pain2. Clients complain lower leg edema and it
does not go away
3. Clients complain shortness of breath ifhas a high activity
4. Clients complain malaise
1.Edema seen in the legs the client2.Has weight loss 4 kilograms in a week (65
kilograms to 61 kilograms)
3.Vital sign :
C. PROBLEM ANALYSISNo Data Problem Etiology
1. Subjective Data :
1. client complains of chest painObjective Data :
1. Vital signa. Blood pressure : 140/100
b.RR : 25 times/minutec. Pulse rate : 142 times/minuted.Temperature : 36,3oC
2. ECG : lead 12 (AF)3. Chest pain scale : 7
Chest pain Myocardial ischemia resulting
from coronary artery occlusion
with loss/ restriction of blood
flow to an area of the
myocardium
-
8/13/2019 CHF in English
51/58
51
2. Subjective Data :
1. clients complained of shortness ofbreath when doing strenuous
activities
Objective Data :
1. edema seen at the foot of the client2. Vital sign
a. Blood pressure : 140/100b.RR : 25 times/minutec. Pulse rate : 142 times/minuted.Temperature : 36,3oC
3.
Heard sound crackles in his bothlungs
4. There is pitting edema grade 3
Shortness of breath Decrease in lung expansion
(fluid accumulation)
-
8/13/2019 CHF in English
52/58
52
E. IMPLEMENTATIONTanggal/
Waktu
NO.
DxIMPLEMENTATION INITIALS
24/5/2012 1.
2.
INDEPENDENT
k) Obtainetion resting vital signsl) Placetion patient on complete bed rest during angina episodes.
m)Placetion patient on semi-Fowlers position.n) Monitoretion vital signs q 5 minutes during initial anginal attack
o) Monitoretion heart rate and rhythmCOLABORATION
c) Monitored laboratory and serial ECG results
INDEPENDENT
1.Auscultation breath sounds noting crackles, wheezes.
2.Instruction patient in effective coughing, deep breathing.
3.Encouragion frequent position changes.
4.Maintaining chair/bed rest with head-of-bed elevated 20 to 30 degrees,semi-Fowlers position. Support arms with pillows.
COLABORATION
d) Administering medications as indicated :a. Diuretics, e.g., furosemide (Lasix)
b. Bronchodilators, e.g., aminophylline.25/5/2012 1. INDEPENDENT
1. Obtainetion resting vital signs
-
8/13/2019 CHF in English
53/58
53
2.
2. Placetion patient on complete bed rest during angina episodes.
3. Placetion patient on semi-Fowlers position.4. Monitoretion vital signs q 5 minutes during initial anginal attack
5. Monitoretion heart rate and rhythmCOLABORATION
1. Monitored laboratory and serial ECG results
INDEPENDENT
1. Auscultation breath sounds noting crackles, wheezes.
2.Instruction patient in effective coughing, deep breathing.
3.Encouragion frequent position changes.
4.Maintaining chair/bed rest with head-of-bed elevated 20 to 30 degrees,semi-Fowlers position. Support arms with pillows.
COLABORATION
1. Administering medications as indicated :a. Diuretics, e.g., furosemide (Lasix)
b. Bronchodilators, e.g., aminophylline.
F. EVALUATIONDATE DX HOURS EVALUATION INITIALS
24/5/2012 DX 1 14.00 pm S: clients say the pain was reduced by a scale of 4
O: Vital sign
1. Blood pressure : 130/1002. RR : 25 times/minute
-
8/13/2019 CHF in English
54/58
54
DX 2
3. Pulse rate : 125times/minute4. Temperature : 36,3oC
Chest pain scale : 4
A: intervention resolved in part
P: continued intervention
1. Obtained resting vital signs2. Placed patient on complete bed rest during
angina episodes
3. Placed patient on semi-Fowlers position.4. Monitored vital signs q 5 minutes during initial
anginal attack
5.
Monitored heart rate and rhythm6. Maintained quiet, comfortable environment;
restrict visitors as necessary
7. Provided light meals; encouraged patient to restfor 1 hr after meals
S: the client says shortness of breath remained
O: edema seen at the foot of the client
1. Vital signa. Blood pressure : 130/100
b. RR : 25 times/minutec. Pulse rate : 125 times/minuted. Temperature : 36,3oC
2. Heard sound crackles in his both lungs3. There is pitting edema grade 3
A:intervention has not been resolved
P: continued intervention
1. Auscultation breath sounds noting crackles,wheezes
2. Instruct patient in effective coughing, deepbreathing
3. Encourage frequent position changes.
-
8/13/2019 CHF in English
55/58
55
4. Maintain chair/ bed rest with head-of-bedelevated 20 to 30 degrees, semi-Fowlers
position. Support arms with pillows
25/5/2012 DX 1
DX 2
S: clients say the pain is gone
O: Vital sign
1. Blood pressure : 125/1002. RR : 25 times/minute3. Pulse rate : 100 times/minute4. Temperature : 36,3oC
ECG : lead 12 (AF)
A: intervention resolved
P: the intervention is stopped
S: shortness of breath decreases the client says
O:
1. Vital signa. Blood pressure : 125/100
b. RR : 25 times/minutec. Pulse rate : 100 times/minuted. Temperature : 36,3oC
2. Heard sound crackles in his both lungs3. There is pitting edema grade 3
A: intervention resolved in part
P: continued intervention
1. Auscultation breath sounds noting crackles,wheezes
2. Instruct patient in effective coughing, deepbreathing
3. Encourage frequent position changes.4. Maintain chair/ bed rest with head-of-bed
elevated 20 to 30 degrees, semi-Fowlers
position. Support arms with pillows
5. breath sounds noting crackles, wheezes
-
8/13/2019 CHF in English
56/58
56
6. Instruct patient in effective coughing, deepbreathing
7. Encourage frequent position changes.8. Maintain chair/ bedrest with head-of-bed
elevated 20 to 30 degrees, semi-Fowlers
position. Support arms with pillows
-
8/13/2019 CHF in English
57/58
57
CHAPTER IV
CLOSING
A. CONCLUSION1. Heart failure is a condition where the heart as a pump pathophysiology unable to meet
the needs blood to tissue metabolism
2. Factors that can trigger the development of heart failure through the suppression of asudden circulation can be: arrhythmias, systemic infections and lung infections and
pulmonary embolism.
3. Complications caused by CHF include deep venous thrombosis, digitalis toxicity andcardiogenic shock. Investigations can be performed in patients with CHF is a chest
radiograph, ECG, EKG, and others. Management that can be done by health,
especially nurses and physicians include: pharmacological management, non-
pharmacological and health education.
4. Heart failure is handled by common action to reduce the workload of the heart andselective manipulation of the three major determinants of myocardial function, either
individually or a combination of: an initial load, contractility, and the load end.
B. ADVICEIt is desirable to avoid the disease congestive heart failure is performed by avoiding the
cause of the disease such as maintaining a healthy lifestyle, especially in the food consumed is
expected to not only look delicious but also consider the nutrients contained in, the food.
-
8/13/2019 CHF in English
58/58
REFFERENCE
1. http://www.emedicinehealth.com/congestive_heart_failure/page12_em.htm#Interventions
2. http://www.hearthealthywomen.org/cardiovascular-disease/heart-failure/heart-failure-4.html
http://www.emedicinehealth.com/congestive_heart_failure/page12_em.htm#Interventionshttp://www.emedicinehealth.com/congestive_heart_failure/page12_em.htm#Interventionshttp://www.emedicinehealth.com/congestive_heart_failure/page12_em.htm#Interventionshttp://www.emedicinehealth.com/congestive_heart_failure/page12_em.htm#Interventionshttp://www.emedicinehealth.com/congestive_heart_failure/page12_em.htm#Interventionshttp://www.emedicinehealth.com/congestive_heart_failure/page12_em.htm#Interventions