
P L I E G O DE E S P E C I F I C A C I O N E S T E C N I C ...
A r e vi e w of te c h ni c a l adv anc e s in vir tua l co lon os c op y
Frans Vosa,c, Iwo Serliea,b, Rogier van Gelderd, J. Stokerd, Henri Vroomanc, Frits Postb
aPattern Recognition Group, Delft University of Technology, Delft, The NetherlandsbComputer Graphics & CAD/CAM Group, Delft University of Technology, Delft, The Netherlands
cBiomedical Imaging Group Rotterdam, Erasmus University Rotterdam, Rotterdam, The NetherlandsdDepartment of Radiology, Academic Medical Center, Amsterdam, The Netherlands
Abstract
Ear ly d etection o f p olyp s h as p r oven to lea d to a d ecr ea se in incid en ce of co lo n can cer . In th e pa s t few yea rs , vir tu a lcolo n os co py ha s b een develop ed as a pa tient-friend lys cr eening tech n iq ue. T he p r oced ur e com p rises the fo llowin g s teps . Fir st, the p a tien t’s colo n is clea ns ed an d tra ns a na llyinfla ted with a ir . S ub seq uently, a 3 D ima ge vo lu m e is a c-q uired o f th e a bd om en by CT or MRI . Fin ally, the bo wels ur fa ce is extra cted an d vis ua liz ed , a fter which th e p hysicia nvir tu ally na vig ates thr ou gh th e co lon a nd exam ines th e s ur -face for a bn or ma lities. T h is p ap er d es cr ib es th e pr o gr es s in r es ea rch for vir tua l co lon os cop y.
Keywords:
Med ical In fo r matics ; I mag e Pr ocess in g ; Scien tific V is ualiza-tio n; V irtual End os cop y.
Introduction
Color ectal m align an cies are amo n g th e leadin g cau ses of can cer d eath s in th e W es ter n wo r ld [ 1 ]. Ear ly detection of p olyp s h as p r ov en to lead to a d ecrease in incid ence [2 ] . To enable lar ge- scale s cr een in g, an eff ective pr ocedu re to d etects uch po lyp s is need ed.
U ntil r ecently, b ar ium en em a an d o ptical co lon os cop y wer ethe two pr ocedu res available fo r exam in in g the co lo n [3 ] [4 ].I n th e ’ do ub le co ntr as t b ar iu m enema’ , sever al p lan ar X -r ay images are acqu ir ed of th e ab do m en b y r otating th e camer aaro un d the p atien t. Im med iately befo r e im ag e acq u is itio n ab ar iu m s olution f ollow ed air is in jected in to th e b ow el via theanu s. Th e rad io -o paq ue b arium s tickin g to th e co lon w allenables th e v is ualizatio n o f th e s ur f ace as a wh ite s tr u ctur eo n a dar k backgr ou nd . I n co n ventio n al co lo no scop y an en do -s co pic cam er a is tr ans an ally gu ided thr ou gh th e colon . Bym an ip ulating th e tip o f the p ro b e, th e ph ys ician in s pects theinn er s u rf ace f or ab no rm alities . A dr aw back of th e bar iu menema is the radiation b u rd en . Mor eo v er , th e s en s itiv ity isr ather p oo r ( 50 -8 0%, f or po ly ps sm aller than 1 cm in diame-ter [ 3] ) . Co lon os co p y req uires intrav en ou s sed atio n , wh ilethe colo n as cen dens of ten can no t b e acces sed b y the end o -s co pe [ 4 ]. Th e sens itivity is es timated to b e in th e or d er o f 8 0- 82 % f or s m all po lyp s.
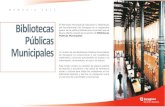
P eo ple eligib le f or screening o f ten avo id th e ex aminatio ns ,b ecau se of th e as so ciated d is co m fo rt [5 ]. I n the past f ewy ears , v ir tu al co lo n os co p y (V C) has b een dev elop ed as ap atient- fr ien dly alter nativ e [6 ] . Fir st, th e p atien t’ s colon is clean sed and tr an san ally in flated with air. Su bs equ en tly , a 3 Dimage v o lu me is acq u ir ed of the ab do m en b y CT or MRI .F in ally , the in terio r bo w el s ur f ace is ex tr acted an d vis ualized ,after w h ich the p hy s ician v ir tu ally n av ig ates th r ou gh th e co -lon and ex am ines th e s ur f ace fo r abn o r m alities ( Fig ur e 1) .
Figure 1 – Virtual endoscopic view of a protruding polyp
Rad io lo g is ts have im mediately r eco gn ized th e imp o rtan ce of this new tech no lo gy . Cur r en tly, VC is alr ead y clinically u sed in a few ins titutio n s [8 ] . Pr ogr es s in medical inf o rm atics h as m ad e a con sid er ab le co ntr ib utio n to its s ucces s [ 7] . Fo r g en -eral ap p licatio n, h o wever , fu rth er im pr ov em ents are r eq u ir ed o n patient f r iend lin es s, co st eff ectiven es s, sens itivity fo r po l-y ps and radiation d o se ( if an y) .
State-of-the-art methods
The v ir tual end os co p ic ex am in ation can be m o deled to co m -p rise f o ur s tag es : p atient pr ep a ra tion , ima ge a cqu is ition ,vis ua liz atio n an d d ia gn os tic exam in ation . I n th e n ex t s ectio ns w e will rev iew techn iq u es r elated to each step .
Patient preparation
F or o ptimal v is ualizatio n , pr op er patient p r ep ar ation is r e-q uired p rior to s can ning . Con ven tion ally, th e pr o cedu re co n -s is ts o f the fo llow ing s tep s [8 ] [9 ][ 1 0] :
• O n th e d ay b efo re th e ex aminatio n, th e patient is ask ed to d rink 4 - 5 liter o f a lax ative f luid ( e.g. X - pr ep , G olytely ,D ulco lax o r Clean Pr ep [1 0 ]) . Su ch a r eg im e is neces sary
s in ce r emain ing f aeces m ay easily be in terp r eted as p ol-y ps [ 11 ][ 12 ].
• I mm ed iately b ef or e d ata acq uisitio n, a bo wel r elaxantm ay b e adm in ister ed in tr aveno us ly. A lth ou gh th e b en e-f icial eff ect has b een d is pu ted [ 1 3] , man y in vestig ato rs u se G lu cag on or Bus cop an (1 mg ) to pr event m o vemen tar tif acts du e to peris tals is [1 0] .
• F or d is ten sio n an d to in tro du ce co ntr as t, d iff er en t agents h av e been pr o po sed. In CT co lo no s co py 1.5- 2.0 liter car -b on d io x id e o r ro om air is tr an s an ally br ou g ht in the co -lon [1 4] . F lu id gado lin iu m s olution s ( e.g. 2 0 m M/l) ar eapp lied in m agn etic reso n an ce im ag in g [ 15 ].
A pers is tin g p ro blem at th is s tag e is remain ing s too l. F ecalr es ts caus e f alse p o sitiv e find ing s and f lu id res ts o cclud ep ar ts o f the co lo n w all ( no tice th e f lu id s u rf ace in Fig ur e 1 atthe b ottom ).
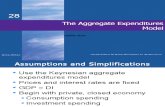
Figure 3 – Images acuired with CT (left) and MRI (right)
Data acquisition
A dv an ces in image acqu is ition tech no log y (MRI an d CT) h av e giv en a stro ng im petus to v ir tu al en do s co py . I n CT im -aging , the d evelo pm ent o f s piral m ulti- detecto r s cann er s en -abled acqu is ition w ith in a br eathh old at a h ig h r es olution [ 16 ]. Th us , m ov em en t artifacts are larg ely p reven ted an d p ar tial vo lu m e eff ects ar e red uced [ 11 ].
Table 1 – Typical scan parameters with CT colonoscopy
Acquisition pa-rameter
Low-doseprotocol
High-resolutionprotocol
Tube current 50-100 mA 120 mA
Collimation 2.5-5.0 mm 1.0-1.5 mm
Table feed/rotation 12.5-15.0 mm 6.0-7.5 mm
Rotation time 0.5-0.8 s 0.5-0.8 s
Rec. increment 1.5-3.0 mm 0.8 mm
S am ple s cann ing p ar ameter s fo r CT co lo no s co py ar e giv en in Tab le 1 [1 0] . A ty pical low do se p r otoco l yield s 20 0 -3 00 images o f 51 2 2 pixels at a reso lu tio n o f ab ou t 0 .7 5 2 x 3 mm 3 .The amo u nt o f images w ith a h ig h r es o lu tion pr oto co l can b e4 50 -5 00 slices of 0 .8 mm th ickn ess .
MR co lo n os co p y has com e w ithin r each with th e dev elop -m en t of in cr eas in gly f as ter gr ad ients . Tw o com m on s can ning p ro to co ls ap p ly a 3 D gr ad ient echo or a H aste s eq uence[ 9] [1 7] . Typ ical scan par am eter s are given in Tab le 2 [ 1 0] .
F acto rs in flu en cing co ntr as t ar e the flip an gle ( 3D G RE) and the ech o tim e ( Haste s eq u en ce). In a 3D G RE sequ ence th eh ig hest po ss ible flip an g le is cho sen to op tim ize p os itivecon tr as t ( br igh t co lon o n a d ar k b ack gr ou nd ). To m aximizethe n eg ative co ntras t in a Haste s eq u en ce an ech o tim e b e-tween 6 0 and 80 s ec. is s elected .
Table 2 – Typical scan parameters with MR colonoscopy
Acquisition pa-rameter
3D GRE Haste
Tr, Te, Flip angle min, min, max -, 60-80, 90°
Slice thickness 1.2-6.0 mm 8 mm
Matrix 256x160 256x160
Field of view 36-44 cm 36-44 cm
Both pr o ne an d su pin e scann in g r em ain s es sen tial bo th w ith CT an d MRI to enh an ce distens io n and r eso lv e p os sib le am -b ig uities du e to sto ol r ests [1 8 ]. Clearly, su ch an app r oach g oes at th e exp en se of a do ub led r ad iatio n d os e w ith CT. O nthe o th er han d, s ub - op tim al con trast an d res olutio n still o b -s tr ucts larg e-s cale ap plication of MRI [1 0] .
Visualization
F or v is u alization o f CT or MRI vo lu m e data, ther e ar e two techn iq u es av ailable: su r face f ittin g and d irect vo lu me ren-d er in g [ 19 ]. Su rf ace f ittin g is a pr epr oces s in g s tep to ex tr actiso -v alu ed s u rf aces fr om th e data vo lum e. Th e ’m arching cub es ’ alg or ith m [2 0 ] is of ten u sed to th is en d, resu lting in anapp ro xim atio n b y lar ge tr iang le m esh es . Con ven tion ally, 3 D gr ap hics hard w ar e can b e u sed f or f ast v isu alization . Then um ber o f gen er ated po ly g on s, h o wever , gr ow s ex p on en -tially w ith the v olu me s ize. Fo r h ig h r es olu tion data, thisn um ber is ty p ically b etw een 1 05 an d 10 6 tr iang les . Thu s, in -ter activ e viewing is o nly p os sible u sin g p ow er fu l gr ap hics acceler ato rs , o r af ter a redu ction o f the m esh s ize [ 21 ] ( wh ich is at th e ex p en se o f los s in accu r acy an d f in e d etails [2 2 ]) .
I nf or matio n o n th e local sign al valu es is lo st in s ur f ace ex -tractio n . Dir ect vo lum e r en derin g (D VR) pr es erv es su ch in -f or matio n by pr ojectin g an im ag e o f the 3 D d ata v olu me o nthe s cr een [ 2 3] [2 4] . A n examp le of D VR is vo lum e r ay cas t-ing ( Fig ur e 4 ). The im ag e is gen er ated by castin g a r ay fr om the v iew po in t thr ou g h each pixel o n the s cr een in to the datav olum e. Next, the v o lu me is s am p led alo ng th e ray . A tr an s -f er f un ction as so ciates the d ata v alu es w ith v alu es f or co lo r ( RG B) an d op acity ( 0 -1 ). Th e co lor o f each image pixel isd eter min ed b y ’ co mp o siting ’ th e colo r an d o pacity valu es in f ro nt-to -b ack o rd er alon g the r ay.
Both surface fitting and DVR have been successfully ap-plied in virtual colonoscopy.
Diagnostic examination
Cur rently, m o st imp lem en tatio ns of s u rf ace and v o lu me r en-d er in g d o no t allow in ter active visu alizatio n. To m eet ther eal- tim e co n strain t, im age s eq u en ces are g enerated o ff -lin ef or later diagn os tic exam in atio n b y the p hy s ician . View ing
p os itio n s ar e tak en on a central p ath thr ou g h th e colon ’ s lu -m en . Sev er al strateg ies w er e pr o po sed in th e literatu re[ 26 ][ 27 ] to autom atically o btain the path , s uch as sk ele-ton ization o f the s egm en ted colo n’ s inter io r v olu me. Ty p i-cally , image sequ en ces ar e gener ated , that s ho w v iews f r om coecu m to rectu m an d v ice v er sa. Thu s , th e amo un t o f dis -p layed s ur face is m aximized . Su ch an ap pr oach still y ields s electiv e views o n the co lo n wall: im po rtan t s ur f ace par ts m ay b e m is sed , wh ile ins ign if icant p arts ar e con s id er ed twice.
Figure 4 – The principle of volume ray casting
To so lv e the latter in eff iciency , so - called pano r am ic v iew sare cur r en tly exp lo r ed . O ne app r oach im plies f old in g ou t thecolon , and s p read in g the in ner w all o n a flat plane, so th at th ef ull su r face is exp o sed f or exam in ation . Sev eral techn iq u es are d es cribed in th e literatu re, f ro m s im ple cylind rical coo r -d in ate trans f or ms , to co m plex co nf or m al m ap p in gs [2 8] [2 9 ].The cylind rical tran sf or m p ro du ces ex cess iv e d is tor tion s ,w hile lo cal g eo metr y is m uch better p reserv ed in a co nf o rm alm ap ping . A s an alter nativ e, w e h av e w or ked o n an ’u nf old ed cub ic’ r en der in g (s ee Fig ur e 5) [3 0] . Thu s, a fu ll 36 0 d egr eev iew is allo w ed f ro m a g iven po int.
Figure 5 – Our unfolded cube representation
A ny v is u alization tech niq ue r elies h eav ily o n a p ro per r ep re-s en tatio n of th e geo metr ic in fo r matio n. I mp o rtan t cu es su chas vascu larizatio n tex tu r e ar e u navailable. Fo r o ptim al ex -p lo itation o f s ur face geo metr y, so me meth od s f or au to maticd etectio n of po ly ps have been s u gg es ted . Co m m on tech -n iq ues are b ased on lo cal p rincipal cur vatu r es , cir cle f ittin gand analys is of s ur f ace n or mal o rien tatio n [ 31 ][ 3 2] . Th o ug hcur rently rather cr u de, autom atic po lyp d etectio n m ay w ells er ve as a v isu al s u pp or t f or in sp ectio n.
Ongoing research
This section describ es o n go in g w or k s pecifically in r elation to requ iremen ts s uch as p atient co mf o rt, co s t eff ectiven es s,s en sitiv ity and r adiatio n d os e.
Patient preparation
P reviou s ly , r em ainin g sto ol w as id en tif ied as an im po rtantimp ed im ent f o r pr actical pu rp os es. To r ed uce s uch artif acts,o ptim al clean sing is ess ential. Th e p atient fr ien dlin es s , ho w -ever, is enh anced if a less intens iv e clean s ing r eg ime cou ld b e perf o rm ed . I n CT co lo no s co py bo th r equ ir ements m ay b em et b y w ay o f a r ad io- op aqu e su b s tance ( e.g. io dine) add edto th e lax ative f lu id [3 3 ]. Con s eq uently , lab eled sto ol can beidentif ied b y a h ig h s ig n al d en s ity [ 12 ]. U n fo rtu nately , con -tradicto ry r esu lts r eg ar d in g sen sitiv ity ar e r ep or ted [ 34 ].
S to ol is m or e m ob ile w ith the liqu id co ntras t ag ent in MRcolon os cop y [ 35 ]. F o r th at reas o n, im ag in g in pr o ne and su -p in e po s itio n in its elf is us ually s u ff icient to d istin gu ish f ecalm ater ial. A ch an ge in po sitio n o f th e p atien t is also r equ ir ed in MRI to red is tr ib u te air so th at o b scur ed parts o f th e colo ns ur face may b ecom e v is ib le. A ny remaining am bigu ities cau sed b y faeces may b e p revented by or al in gestion o fg ad olin ium in com bin atio n w ith a s to o l so ftener [ 35 ]. A s ar es ult, fecal r es ts get the s am e char acteris tics as the su r -r ou nd in g g ad o linium so lu tio n.
I nf or matio n abo ut th e per fu sion can b e ob tained b y in tr ave-n ou s co n tr as t injectio n b oth in CT an d MR co lo n os co py .I od in ated co n tr as t ( 1.6 g iod in e/s ) s ig nifican tly imp ro v es p olyp d etection w ith CT [3 6] . Con nected to MR g ado liniu mand b lo o d po o l ag en ts pr o mise to f ulf il this aim [1 0] . I n du etim e su ch metho ds m ay facilitate ind irect v isu alization of th em uco s al colo r an d d ig ital clean sing .
Data acquisition
The o bv iou s d rawb ack o f CT is the us e o f io nizin g r ad iatio n.N ot s ur p risin gly, s everal autho r s des cr ib e eff or ts to m in imizethe r ad iatio n exp os u re ( w itho ut jeop ard izing th e sen sitivity) [ 37 ][ 38 ] . At 70 m A, scan n in g in su pin e a nd pr on e p os ition cor resp o nd s to a rad iatio n do se fo r a b ar ium enem a. I t h as b een dem on str ated th at lo wering th e exp os ur e to 5 0 mA do es n ot aff ect th e s en s itiv ity [ 38 ] . Th e b en ef its o f MRI in thisr es pect ar e o bv io us . A no ther ad v an tag e is MRI’ s eno rm ou s p oten tial fo r v is ualizin g con trast in s of t tis su e ( str uctu res b eh in d the co lo n wall) . Regr ettab ly , CT im ag e r es olu tion an dcon tr as t b etw een co lon w all and in ter io r ar e s up erior [ 1 0] .A ls o, th e co s t fo r con tr ast m aterial an d eq u ip men t fo r MRI is h ig her. Cu rr ent MR s lice th ickn ess ( s pecifically in a H astes eq uence) is to o lar ge f o r th e d etectio n of sm aller p oly ps .Mor eo ver , sig nal in h om og eneities , du e to receiver b ias and g ad olin ium s u sp en sion , com p licate visu alizatio n. A s y et, CTw ill rem ain s tate o f the ar t, alth ou g h fu rth er d evelo pm ent o f MR co lo n os co p y is ju stif ied.
Visualization
S ur face rend ering ( S F) is o ften ap plied in V C un d er the as -s um ptio n that the s ign al ch an ge betw een w all and lu men isins tantaneou s . To av oid d ecim ation , o nly th o se p o ly go ns m ay b e s ub mitted to th e r en derin g pip elin e that are v is iblef ro m th e v iew in g fr u stru m [ 6] . I nf or m atio n abo ut th e detailed s tr uctu r e of th e mu cos a, ho wever , is om itted [ 22 ] .
I n [2 2] it is d em on s tr ated ho w the m u co sal inter f ace can b eb etter v is ualized b y d ir ect v olu me r end er in g ( DVR). Mor eo -v er , ex p lo ratio n of th e tis su e b en eath th e s ur face is s u pp or ted
b y a so p histicated adaptation o f the tr an sf er fu n ctio n. Th elatter asp ect m ay h elp in d iff er en tiating benign tiss ue f ro m m alig n an cies .
Cur rently, in teractive f r am e rates in D VR are o n ly availablef or m od erately- sized d ata v olum es on high -en d gr ap hics w or ks tatio ns , b y us ing s p ecial- p ur po s e hard w ar e [ 25 ] or r en derin g alg or ithm s [ 22 ] . Pers p ectiv e pr ojectio n is req uired f or a g o od v iew o f the co lo n in ter io r , bu t is no t alw ay s s up -p or ted b y eff icient DVR alg or ith ms or h ar d ware. The s itu a-tio n in visu alizatio n sp eed is chang ing r ap idly, an d real- tim es ur face an d v olum e r en der in g will so o n be av ailab le o ncom mo n P C platf or ms . W ith SF as w ell as w ith D VR, real- tim e in ter actio n is no t y et g en erally available. Th is h in -d rance, ho wev er , is so lv ed merely by generatin g a s eq uen ceo f im ag es of f lin e.
Figure 6 – Stair-step and shine-through artifacts. Left andright images were created with different transfer functions
Diagnostic examination
A n ob vio us d r aw back of r eview in g the data b y m ean s of as eq uence o f images is th e lim ited su r face in v iew . Fo r a u ni-d ir ectio nal m ov ie ( f ro m coecu m to rectu m) , as mu ch as 2 5 %o f th e colon may be miss ed [3 0] . Bi- d ir ectio nal s eq uencesr ed uce this n um ber to 7%. O nly w hen later al as w ell as top and b ottom r end er in g s ar e add ed , com es th e f ull s ur face in v iew. O u r un f olded cub ic rend er ing s tries to ach iev e th isr es ult (F ig u re 4 ) [ 30 ].
Typ ical ar tif acts d u ring ex plor ation ar e cau sed b y im pr o perclean sin g, in co rr ect s eg m en tatio n an d s ub -o p timal r es olu tion [ 11 ]. P recau tio ns agains t incom plete cleaning were discus sedear lier . F ig u re 6 s h ow s the char acter is tic s tair- step an d s hine- thr ou gh ar tif acts , cau sed b y sev er e aniso tr o py in the s liced ir ectio n res pectiv ely im pr op er op acity s ettin g. Th e stair -s tep artif act jus t h in der s th e v is ualization and can o nly be av oid ed b y us in g thin ner slices. Ph ys ician s m us t be sp ecifically awar eo f th e s hine- th ro ug h artifact as it m ay eas ily r esu lt in f als ep os itiv e and fals e n eg ative f in d in gs . These misin terp retatio n scan b e avo id ed to s o me ex tent b y adap ting th e tr ans fer f un c-tio n at each time a su sp iciou s area is en co u nter ed.
The eff ectiven es s o f CT co lo no s co py has been ex ten sivelys tu died in th e liter atur e ( [1 0] sh ow s a n ice s um m ar y) . I n on eo f th e lates t r ev iew s [3 9 ] th e s en sitiv ity f or p o ly ps larg er th an 1 0 mm ap pr ox imates 1 00 %. Fo r po lyp s f ro m 5- 1 0 mm th is com es to 6 1- 8 0% ( th ere is n o data on sm aller p oly ps ). N o tm uch liter atu re is available reg ar din g MRI. In [ 1 7] , MRCs en sitiv ity f or p oly ps larg er th an 1 0 m m is fo un d to be 96 %.F or p oly ps b etw een 6 -1 0 m m it is 6 1%, w hile sm aller m as s es r em ain u nd etected . The p o or p er f or man ce o f b oth techn iq u es w ith sm aller po ly ps is n o t co ns idered v er y imp or tan t. N ear ly all o f them are b en ign , w hile th eir identif icatio n may increasethe n um b er o f u nn ecess ar y o peratio ns [1 0] . The s tro ng co r -r elatio n between po ly p s ize and the risk of m align an t trans -
f or m atio n jus tif ies a m in im um p oly p size of 5 mm .
Conclusions
V C is b eco min g a state-o f -the ar t scr eening to ol fo r co lor ec-tal p oly ps . I n a few y ear s time, a s tan dard ized p ro to co l h as emerg ed . P ro gr es s in medical inf o rm atics h ad an im po rtan tcon tr ib u tion to its develop ment. Mod ern imag e pr o cess in g and v is u alization tech niq ues en abled mo delin g an d r en der in go f in ner v iew s on th e co lon w all. Fu r th er im pr ov ements,h ow ev er , are need ed .
The cleans in g r eg im e m ay be les s s tr ict to enh an ce patientaccep tan ce. I n ad ditio n, to ols s ho uld b e dev is ed to cop e w ith f aeces. An y s uch techn iq u e sh ou ld facilitate a lo w nu mb er of f alse p o sitiv es and un ob s tr ucted v iew s on th e su r face ( n oo cclu sio n by remain ing f luid) . MR co lon os co p y can b e im -p ro ved r eg ar d in g res olution ( slice th ickn es s ) an d s ig nal h o -m og en eity. A ltern atively , CT radiation d o se h as to b e r e-d uced to its minimu m . Th e p oo r inter activ ity d ur ing exp lor a-tio n req uires enh an cem en t, so th at in r eal tim e ins pection is p os sible. At last, techn iqu es ar e needed to review th e fullcolon s u rf ace at on ce.
The r es ear ch describ ed in this p ap er in dicates th at imp o rtan ts teps ar e mad e in th e rig ht d ir ectio n . It is exp ected th at V Cw ill becom e a s tand ard ized to ol fo r r ad io lo g is ts .
References
[ 1] P otter J D, S lattery ML, Bos tick RM. Colon cancer : ar ev iew o f th e epidem io lo g y. Epidemio l Rev 19 93 : 1 5p p. 4 99 - 54 5.
[ 2] Tor ib rar a NW , S leis eng er MH . Scr eening f o r co lor ectalcan cer. N Eng l J Med 1 99 5: 3 3 2 pp . 8 61 -8 6 7.
[ 3] D od d GD . Colo n cancer an d p olyp s imag in g per sp ec-tiv es . Pro c Fir st I n ter na tion a l Sym po sium on Virtua lColon os cop y, Bos ton U niv er sity Pr es s , 19 9 8: p p. 15 -1 7 .
[ 4] Rex D K, Cu tler CS , Lem mel GT. Co lon os cop y mis -r ates o f aden om as d eterm ined by back - to -b ack colo no -s co pies . G as tr oen ter olog y 19 97 : 11 2 pp . 2 4- 28 .
[ 5] W in aw er SJ , F letcher RH, Miller L. Co lo rectal can cer s cr eenin g: clin ical gu id elines and r ation ale. G as tr o-enter olog y 19 97 : 11 2 pp . 5 9 4- 64 2.
[ 6] H on g L, Mu rak i S, K auf man A , He T. V irtual v oy ag e:inter activ e n av ig ation in the h u man colon . Pro c ACMS IG GRAPH Co nf. A CM P r es s, 1 99 7; p p . 27 - 34 .
[ 7] Lor en sen W E, Jo lesz FA , K ik in is R. Th e ex plo ratio n of cro ss -s ectio n al d ata w ith a v ir tual end os co p e. I nter a ctT echn a n d th e New H ealth Pa ra d 19 95 : 4 59 p p . 22 1- 2 30 .
[ 8] H elen M, F er u cci JT. V ir tual en d os co p y beco m es v ia-b le o ption . G as tr oen ter olog y 1 99 9: 11 4 pp . 5 7- 68 .
[ 9] Lub oldt W, Bauerf ein d P, Steiner P , F ried M, K res tin G P, D eb atin J F. P relim in ary ass ess men t of th ree d i-m en s io nal m ag netic r es o nance imagin g fo r v ar io u scolon ic diso r ders . L an cet 19 99 : 3 49 p p . 12 88 - 12 91 .
[ 10 ] F letcher J G, Lu bo ld t W . CT co lo no gr ap hy an d MR
colon ogr ap hy : cur ren t statu s, r esear ch direction s and com paris on . Eur Rad iol 20 00 : 1 0 pp . 7 86 -8 0 1.
[ 11 ] F en lo n H M. I m ag e Ar tef acts on v irtual colon o scop y .Pro c Secon d I nter na tion a l Sym po sium On Virtua lCo lon os co p y. Bos ton U niv er sity Pr es s , 19 9 8; p p. 40 -4 1 .
[ 12 ] Lak ar e S , Wan M, Sato M, Kauf man A . 3 D DigitalClean sin g Us ing S eg m en tatio n Ray s. Pro c IEEE Vis u -a liza tio n Co n f. A CM P res s, 2 0 00 ; pp . 3 7- 4 4.
[ 13 ] Y ee J , H un g RK, A ker kar G A, W all S D. Th e us e-f ulness of g lucag on hy dr o ch lo rid e fo r colon ic dis tentio n in CT co lo no gr ap hy . Am J Ro entgen ol 1 99 9: 17 3. p p .1 69 -1 72 .
[ 14 ] Rog alla P, S ch midt E, K or v es M, H am m BK. O ptim alcolon d isten tio n fo r v ir tual co lon os cop y: r o om air ver -s us CO2 in su f f lation . Rad io lo g y 19 99 : 2 13 p . 3 42 .
[ 15 ] Lub oldt W, Bauerf ein d W, Wild er m uth S , Debatin J F .Con tr as t o ptimizatio n fo r ass es s ment of the co lo n ic w alland lum en in MR colo no gr ap hy . J Mag n Res on Im ag -ing 19 99 : 9 p p. 74 5- 75 0 .
[ 16 ] H alligan S , F en lo n H M. S cience, medicin e, an d fu tur e -v ir tu al co lo n os co py . Brit Med J 1 99 9: 3 1 9 pp . 1 24 9- 1 25 2.
[ 17 ] Lub oldt W, S teiner P , Bau er fein d P , P elko nen P , D e-b atin J F . Detection of m ass les ion s w ith MR co lo n ogr a-p hy . Rad io lo g y 19 98 : 2 07 p p . 59 -6 5 .
[ 18 ] Chen SC, Lu D SK , Hecht J R, Kadell BM. CT co lo no -gr ap hy : v alue of s can ning in b oth the su pine an d p ro nep os itio n s. Am J Ro entgen ol 19 99 : 1 72 p p . 59 5- 5 99 .
[ 19 ] S hahidi R. S u rf ace r en der in g v er su s v olum e r en der in gin medical im ag in g: tech n iq ues and ap plication s. Pro cI EEE Vis ua liz atio n Con f. ACM Pr ess , 1 99 6; p p . 43 9 -4 40 .
[ 20 ] Lor en sen W E, Clin e H E. Marching cu bes : a hig h res o -lutio n 3 D su r face co ns tr u ctio n alg or ith m. Pro c ACMS IG GRAPH Co nf. A CM P r es s, 19 87 ; p p. 1 6 3- 16 9.
[ 21 ] G ar land M, H eck bert PS . S ur face simp lif ication u s in gq uadr atic er r or m etr ics. Pro c ACM S IG G RAPH Co nf.A CM P res s, 1 9 97 ; pp . 2 09 - 21 6.
[ 22 ] H op per K D, Ly ribo z AT, Kasales CJ . Mu co s al d etail atCT virtual r eality: s u rf ace v er su s v olum e r en d er in g.Rad io lo g y 20 00 : 2 14 p p . 51 7- 5 22 .
[ 23 ] Lev oy M. D is p lay of su rf ace f ro m v olu me d ata. I EEECom p Gr a ph a n d Ap pl 19 88 : 8 p p. 29 -3 7.
[ 24 ] K au fm an A. Volum e Vis ua liz atio n . Los A lam ito s (CA) :I EEE Co m pu ter S ociety Pr ess , 19 9 1.
[ 25 ] P fister H, H ard en ber gh J , S eiler L. The V olu mePr o r eal- tim e ray cas tin g sy s tem. Pro c SI G GRAPH Co nf.A CM P res s, 1 9 99 ; pp . 2 51 - 26 0.
[ 26 ] P aik D, Beau lieu CF , J eff rey RB, Rub in GD , N ap el S.A utom atic fligh t path plann in g f or v irtual end os cop y.Med Phys 19 98 : 2 5 pp . 6 29 -6 3 7.
[ 27 ] Bitter I , Sato M, Bend er M. CEA S AR: A sm oo th , accu -r ate an d r ob u st cen ter lin e ex tr actio n alg or ith m. Pro cI EEE Vis ua liz a tio n Co n f. ACM Pr ess , 2 00 0; p p . 45 - 52 .
[ 28 ] Beaulieu CF, Jeff rey RB, N ap el S. D isp lay m od el fo rCT co lo no gr ap hy : P art I I. Rad io lo g y 19 99 : 2 12 p p .2 03 -2 12 .
[ 29 ] H ak er S , A ng enent S , Tan n en baum A, K ikinis R. No n d is to rting f lattenin g fo r v ir tu al co lon os co p y. Pro cMICCAI con f. Sp ring er, 2 0 00 : pp . 3 58 - 36 6.
[ 30 ] S er lie I WO , V os F M, Po st FH . Cu b ic r end er in g in v ir -tual en d os co p y. S ub m itted f or p u blication to EG/ I EEEVis Sym Con f 2 00 1.
[ 31 ] Beaulieu CF. Co mp uter aid ed d etectio n o f co lon ic po l-y ps . S econ d I nter na tion a l Sym po sium on Virtua lColo n os co py. Bos to n U niv er sity Pr es s , 20 00 ; p p. 73 -7 7.
[ 32 ] S um mers RM, Beaulieu CF, Napel S. A uto matic p olyp d etecto r f or CT co lo no gr ap hy : f easib ility s tu dy . Rad io l-o gy 20 00 : 2 16 p p . 28 4- 2 90 .
[ 33 ] W ax MR. Virtu al colo no sco py - CT co ntras t ag ents.S econ d I nter na tion a l Sym po sium on Virtua l Colon o -s cop y. Bos to n U niv er sity Pr es s , 19 98 ; p p. 66 -6 8.
[ 34 ] P in eau BC, V ining D J . Ab ility o f v ir tual co lon os cop yto detect patients w ith color ectal p o ly ps . G as tr o-enter olog y 19 99 : 11 6 (S up p l A4 8 5) .
[ 35 ] W eisenh aup t D , Patak MA, Fr oehlich J , Ruehm S, D e-b atin J F . Feacal tag ging to avo id co lon ic cleans ing b e-f or e MRI colo no gr ap hy . L an cet 19 99 : 3 54 , p p. 8 35 - 8 36 .
[ 36 ] Mor in MM, Kr u sk al J B, Far ell RJ , Rey n olds K F , Rap -top ou lo s V D. In tr av eno us co ntras t mater ial enh an ces the d iag no stic accu r acy o f CT co lo no gr ap hy . Rad io lo g y1 99 9: 2 1 3 (S u pp l. 2 5 7) .
[ 37 ] Brink J A . Rad iation do se: imp act o f mu lti-s lice CT.S econ d I nter na tion a l Sym po sium on Virtua l Colon o s-cop y. Bos to n U niv er sity Pr es s , 19 98 ; p p. 27 -2 9.
[ 38 ] G elder RE van , Stok er J, Lameris J S. Radiation d o ser ed uctio n fo r 3 D- CT co lo no gr ap hy . S econ d I nter na -tio na l S ym po s iu m on Virtu al Colo no sco py. Bos to n U niv er sity Pr es s , 20 00 ; p . 9 6.
[ 39 ] J oh ns on CD , D achm an CD . CT co lo no gr ap hy : the n extcolon s creen ing exam in ation ? Rad io lo g y 20 00 : 2 16 p p .3 31 -3 41 .
[ 40 ] McF ar lan d EG . Clinical ex perien ce of po ly p d etectio n.S econ d I nter na tion a l S ym po s iu m o n Virtu al Co lo no -s cop y. Bos to n U niv er sity Pr es s , 19 98 ; p p. 19 -2 0.
[ 41 ] H ietala R, O ikarinen J . A Visibility D eter min atio n A l-g or ithm fo r I nter activ e V ir tu al En do s co py . Pro c. I EEEVis ua liz atio n Con f. ACM Pr ess , 2 00 0; p p . 29 - 36 .
Address for correspondence
F.M. Vos, Lorentzweg 1, 2628 CJ Delft, The NetherlandsE: [email protected]; Phone.: +31 15 278 3221, Fax: +31 278 6740.






![News · 2016. 8. 1. · 111 z Iti -o L a al c c: E u a 113 u E Iti E O U.] z c u O E a c: E E u c c Iti u o E c: E O t: c c c a c c tri M o x: c 111 u c a c a c: u a u E a a o E c](https://static.fdocuments.pl/doc/165x107/60e5a31d1fe7095a1e6569ba/news-2016-8-1-111-z-iti-o-l-a-al-c-c-e-u-a-113-u-e-iti-e-o-u-z-c-u-o-e.jpg)








