Acth Problem

of 18
-
Upload
zaman-migozarad -
Category
Documents
-
view
225 -
download
0
Transcript of Acth Problem
-
8/3/2019 Acth Problem
1/18
Editors: Torre, Dario M.; Lamb, Geoffrey C.; Van Ruiswyk, Jerome J.; Schapira, Ralph M.
Title: Kochar's Clinical Medicine for Students, 5th Edition
Copyright 2009 Lippincott Williams & Wilkins
> Table of Contents > Part II - Diseases and Disorders > Endocrinology > Chapter 69 - Diseases of the Adrenal Glands
Chapter 69Diseases of the Adrenal Glands
Jennifer Zebrack
Albert Jochen
Diseases of the Adrenal CortexThe adrenal glands, located at the superior pole of each kidney, are comprised of two concentric layers: the cortex
and the medulla. The adrenal cortex consists of three layers that secrete glucocorticoids, mineralocorticoids, and
androgens.
GlucocorticoidsThe major regulatory system for cortisol is through hypothalamic corticotropin-releasing hormone (CRH) and
pituitary adrenocorticotropic hormone (ACTH). Secretion of ACTH is pulsatile, creating a daily diurnal variation in
cortisol secretion with maximal release in the morning.
MineralocorticoidsThe renin-angiotensin system is the principal regulator of aldosterone synthesis and release. Renin is produced by
the juxtaglomerular cells of the kidney, which catalyzes the conversion of renin substrate to angiotensin I (A-I).
Angiotensin-converting enzyme (ACE) converts A-I to angiotensin II (A-II), which stimulates aldosterone production in
the adrenal cortex. Aldosterone promotes renal tubular Na+ reabsorption and K+ and H+ ion excretion. The regulation
of renin depends on intravascular volume. For instance, upright posture, hemorrhage, diuretics, sodium restriction,
and edematous states increase renin secretion. Hyperkalemia and hyponatremia also strongly stimulate aldosterone
production.
Androgens and EstrogensACTH is the major stimulator of adrenal androgen secretion. Dehydroepiandrosterone (DHEA) and androstenedione
are the major androgens synthesized in the adrenals. DHEA is sulfated in the liver to yield DHEA-sulfate (DHEA-S).
Androstenedione is converted to the weak estrogen estrone by peripheral aromatase.
Adrenal InsufficiencyAdrenal insufficiency can result from primary destruction of the adrenal cortices (primary adrenal insufficiency or
Addison's disease), insufficient pituitary ACTH (secondary adrenal insufficiency), or decreased hypothalamic CRH
(corticotropin-releasing hormone) secretion (tertiary adrenal insufficiency).
Primary adrenal insufficiency results in a deficiency of cortisol and aldosterone with elevated plasma ACTH levels.
Secondary and tertiary adrenal insufficiency results in a deficiency of cortisol with preserved aldosterone secretion.
Etiology
Development of the clinical manifestations of primary adrenal insufficiency (Addison's disease) requires loss or
destruction of 90% or more of both adrenal cortices. In the United States, the most common cause of Addison's
P.428
Page 1 of 18
1/12/2012mk:@MSITStore:C:\Users\Gateway%20Tablet\Desktop\Kochar's%20Clinical%20Medicin ...
-
8/3/2019 Acth Problem
2/18
disease is the idiopathic type resulting from autoimmune destruction of the cortex. It is more common in women,
may be familial, and is usually diagnosed in the third to fifth decades of life. This disease shows a high association
with other autoimmune disorders, such as Hashimoto's hypothyroidism, Graves' hyperthyroidism, Type 1 diabetes
mellitus, pernicious anemia, autoimmune hepatitis, alopecia, and vitiligo. Tuberculosis is the second most frequent
cause in the United States and is a common cause in developing countries. Acute primary adrenal insufficiency
occurs most commonly in a patient with underactive glands who requires increased glucocorticoid production after
exposure to stress (e.g., sepsis, trauma or surgery). It also can follow acute bilateral destruction of the adrenal
glands (e.g., adrenal hemorrhage or infarction) (Table 69.1).
The most common secondary cause of adrenal insufficiency is iatrogenic from prolonged use and subsequent
withdrawal of prescribed exogenous glucocorticoids such as prednisone (which results in significant ACTH
suppression, typically after about 30 days of administration). Other secondary and tertiary causes include any
disorder of the pituitary or hypothalamus, such as trauma (infundibular stalk section), postpartum necrosis
(Sheehan's syndrome), neoplasms, and inflammatory and granulomatous disorders (Table 69.1).
Clinical Manifestations
The evolution of adrenal insufficiency may be gradual or catastrophically sudden. The symptoms of adrenal
insufficiency are often nonspecific and include anorexia, nausea, vomiting, diarrhea, weight loss, hypotension,
fatigue, weakness, fever, and confusion. In primary adrenal insufficiency, signs of dehydration due to aldosterone
deficiency may be present (i.e., tachycardia, orthostatic hypotension). The characteristic hyperpigmentation of theskin (due to ACTH excess) is absent when the adrenal failure is acute, secondary, or tertiary. Hyponatremia is due
primarily to an impaired ability to excrete free water; thus, it is common to any type of adrenal insufficiency.
However, hyperkalemia and metabolic acidosis are absent in secondary or tertiary adrenal failure because
aldosterone secretion is preserved through the renin-angiotensin system. In acute adrenal crisis, the rapid reduction
in intravascular volume, vascular tone, and cardiac output can result in vascular collapse and shock.
In secondary adrenal insufficiency, patients may also have associated deficits of other pituitary hormones, such as
growth hormone, follicle-stimulating hormone, luteinizing hormone, and thyroid-stimulating hormone, manifesting as
growth retardation or delayed puberty in children and erectile dysfunction, amenorrhea, or hypothyroidism in
adults. If a pituitary tumor is the cause, headache, visual field loss, and/or cranial nerve palsies may be present.
P.429
Table 69.1 Etiology of adrenal insufficiency
Primary Secondary
Idiopathic/autoimmune
Tuberculosis
Adrenal hemorrhage
Bilateral infarction
Fungal infection
HIV/AIDS
Metastatic cancer
Bilateral adrenalectomy
Congenital adrenal hyperplasia
Drugs: mitotane, ketoconazole,metyrapone
Long-term glucocorticoid steroid use (abrupt
withdraw)
Neoplasms
Inflammatory lesions
Granulomatous disease
Trauma (infundibular stalk section)
Radiation
Necrosis (Sheehan's syndrome)
Page 2 of 18
1/12/2012mk:@MSITStore:C:\Users\Gateway%20Tablet\Desktop\Kochar's%20Clinical%20Medicin ...
-
8/3/2019 Acth Problem
3/18
Diagnosis
Adrenal insufficiency is best diagnosed by a rapid cosyntropin stimulation test. The test is best done between 6 a.m.
and 10 a.m. Plasma samples are drawn for cortisol before and 3 to 60 minutes after administering 0.25 mg of
cosyntropin intravenous (IV) or intramuscular (IM). Normally, the plasma cortisol should increase 8 g/dL above the
baseline, and it should exceed 20 g/dL at 30 to 60 minutes. Therefore a rise of cortisol level
-
8/3/2019 Acth Problem
4/18
Cushing's disease refers to a high cortisol state caused by a pituitary ACTH hypersecreting tumor (most common
cause), and less frequently pituitary hyperplasia. Cushing's disease is six times more common in women than in men;
the mean age at diagnosis is in the fourth decade.
Etiology
Because of the widespread pharmacologic use of glucocorticoids, the most common cause of Cushing's syndrome is
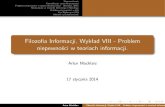
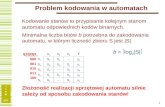
iatrogenic or exogenous glucocorticoid use. Endogenous cases (Fig. 69.1) may be either ACTH dependent (e.g.,
ACTH-secreting pituitary adenoma or ectopic ACTH-secreting neoplasm) or ACTH independent (e.g., adrenaladenoma, adrenal carcinoma). Benign adrenal tumors causing Cushing's syndrome predominantly produce
glucocorticoids; adrenal cancers, however, often secrete high levels of adrenal androgens and glucocorticoids.
Ectopic ACTH secretion occurs in a few neoplasms (e.g., small cell carcinoma of the lung, carcinoid tumors,
pancreatic islet cell tumors), usually in men in the fifth decade and beyond.
Functioning benign adrenal adenomas and adrenocortical cancers each give rise to less than 10% of cases of Cushing's
syndrome. Benign adenomas are usually small and synthesize cortisol very efficiently. In contrast, functioning
Figure 69.1 Etiology of hypercortisolemia: Cushing's syndrome.
Page 4 of 18
1/12/2012mk:@MSITStore:C:\Users\Gateway%20Tablet\Desktop\Kochar's%20Clinical%20Medicin ...
-
8/3/2019 Acth Problem
5/18
adrenocortical cancers are very large at diagnosis and often produce adrenal steroids inefficiently.
Clinical Manifestations
The clinical features of hypercortisolemia are shown in Table 69.2. They include centripetal obesity, which is caused
by the accumulation of fat in trunk, face, and neck, hence the description of buffalo hump and moonfacies. At times, it is helpful to examine serial photographs of the patient, looking for evidence of progressivephysical changes consistent with excessive cortisol exposure. The facial plethora (round face) may be subtle (Fig.
69.3) or quite obvious (Fig. 69.4).
Patients may commonly experience proximal muscle wasting and weakness, which are caused by the catabolic effect
of high glucocorticoid levels on skeletal muscles. Hypertension, diabetes mellitus, osteoporosis, and depression are
often present. Thin skin, easy bruisability, violaceous striae (on breasts and abdomen) and skin atrophy are some of
the dermatologic manifestations of Cushing's syndrome.
Hyperpigmentation is most commonly found in sun or pressure exposed areas (elbows, knuckles, waist). It occurs
most often in patients with ectopic ACTH secreting tumors and less often in patients pituitary disease (Cushing's
disease). However, it is absent in high cortisol states caused by adrenal disease (Cushing's syndrome) because lack of
P.431
Table 69.2 Clinical manifestations of hypercortisolemia
Truncal obesity 95%
Menstrual Irregularities 80%
Hypertension 75%
Facial plethora (round face) 75%
Hirsutism/vellus type hair growth 65%
Gonadal dysfunction 50%
Violaceous striae 65%
Diabetes mellitus 65%
Hyperlipidemia 70%
Proximal muscle weakness 60%
Page 5 of 18
1/12/2012mk:@MSITStore:C:\Users\Gateway%20Tablet\Desktop\Kochar's%20Clinical%20Medicin ...
-
8/3/2019 Acth Problem
6/18
-
8/3/2019 Acth Problem
7/18
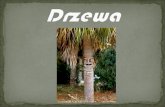
Figure 69.2 Diagnosis, workup, and differentiation of hypercortisolemia (Cushing's
disease/syndrome). UFC, urine-free cortisol.
Page 7 of 18
1/12/2012mk:@MSITStore:C:\Users\Gateway%20Tablet\Desktop\Kochar's%20Clinical%20Medicin ...
-
8/3/2019 Acth Problem
8/18
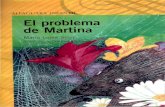
Figure 69.3 These photographs of a young woman with Cushing's syndrome show subtle changes in
the facial outlines over a 3-year period.
Page 8 of 18
1/12/2012mk:@MSITStore:C:\Users\Gateway%20Tablet\Desktop\Kochar's%20Clinical%20Medicin ...
-
8/3/2019 Acth Problem
9/18
Figure 69.4 This photograph of a middle-aged woman with Cushing's syndrome demonstrates the
characteristic plethoric facies.
Table 69.3 Frequency of occurrence and potential causes ofhypercortisolemia
Hypercortisolemia Ectopic ACTH Pituitary Adrenal
Hyperpigmentation ++ + -
Cause Ectopic ACTH secreting
tumor (+ACTH)
Pituitary tumor
(+ACTH)
Adrenal adenoma (-
ACTH)
Page 9 of 18
1/12/2012mk:@MSITStore:C:\Users\Gateway%20Tablet\Desktop\Kochar's%20Clinical%20Medicin ...
-
8/3/2019 Acth Problem
10/18
Once hypercortisolemia is established, the distinction between ACTH dependence and ACTH independence should
follow, based on measurement of plasma ACTH; levels exceeding 20 pg/mL indicate ACTH-dependent
hypercortisolism. Patients with primary adrenal neoplasms have a suppressed or low plasma ACTH (
-
8/3/2019 Acth Problem
11/18
In primary hyperaldosteronism, the intravascular volume is typically high. Key manifestations include hypertension,
spontaneous hypokalemia, metabolic alkalosis, low plasma renin activity, and an elevated plasma aldosterone level.
The hypertension usually is moderate and is due to the sodium-retaining effects of the mineralocorticoid. Rarely, the
hypokalemia may evoke easy fatigability, anorexia, muscle weakness, and cramps.
Diagnosis
Screening for primary hyperaldosteronism should be performed in hypertensive patients with spontaneoushypokalemia below 3.5 mEq/L, or a serum K+ below 3.0 mEq/L while taking a diuretic. The first phase of the workup
includes screening tests, followed by testing to confirm the diagnosis (Table 69.4). In primary hyperaldosteronism
PRA is low, PAC is elevated, and PAC/PRA ratio is >20 (elevated). Testing is optimal when the individual is salt
loaded and when the hypokalemia is corrected. Before biochemical testing, the following medications should be
discontinued: all antihypertensive agents except peripheral -1 antagonists and central -2 agonists for at least 1
week, diuretics for 4 weeks, and estrogen and spironolactone for 6 weeks.
Over 90% of cases of primary hyperaldosteronism are due to either APA or IHA, so the last phase involves
differentiating between these two causes. High-resolution CT is performed initially because it localizes the APA in
70% to 80% of cases. Bilateral adrenal vein catheterization is the most definitive means to distinguish between APA
and IHA.
Treatment
Patients with an APA who are at low surgical risk should undergo unilateral adrenalectomy. One year following a
successful surgery, 80% to 90% of patients remain normotensive and normokalemic. After 5 years, however, 50%
develop recurrence of the hypertension while remaining normokalemic; the reason for this is not clear. Factors
predicting persistence or recurrence of hypertension after unilateral adrenalectomy include duration of hypertension
and family history of hypertension.
In patients with IHA, bilateral adrenalectomy is ineffective in controlling hypertension, so medical management is
the treatment of choice. Patients should follow a low-sodium diet (
-
8/3/2019 Acth Problem
12/18
Congenital Adrenal Hyperplasia
Congenital adrenal hyperplasia (CAH) is a family of autosomal recessive disorders resulting from defects inglucocorticoid, mineralocorticoid, and androgen production. Deficient cortisol biosynthesis causes a compensatory
rise in pituitary ACTH, resulting in adrenocortical hyperplasia and overproduction of the steroids that precede the
enzymatic defect.
Etiology
CAH can result from any one of five enzyme deficiencies: 21-hydroxylase, 11-hydroxylase, 3-hydroxysteroid
dehydrogenase, 17-hydroxylase, or 20,22-desmolase. Classic 21-hydroxylase deficiency, the only human leukocyte
antigenlinked type, accounts for more than 90% of cases of CAH. The next most common, 11-hydroxylase
deficiency, accounts for almost 5% of cases.
Clinical ManifestationsCAH can take two forms: a classic, congenital form with nearly total enzymatic deficiency or, more often, a late-
onset form with a partial enzymatic deficiency and onset after puberty. Clinical features depend on which steroids
are deficient or in excess, as well as the absolute degree of deficiency or excess. The manifestations of the most
common form, 21-hydroxylase deficiency, usually include virilization in females or ambiguous genitalia, salt-wasting,
nephropathy, hyponatremia, and hyperkalemia. 11-Hydroxylase deficiency typically presents with virilization in
females or ambiguous genitalia, high blood pressure, and hypokalemic alkalosis.
Diagnosis
In CAH, the steroid precursors to the defective enzymes are elevated; these steroids are used for diagnosis when
CAH is suspected. For instance, in 21-hydroxylase and 11-hydroxylase deficiency, plasma 17-OH progesterone and 11-
deoxycortisol are typically elevated, respectively. In mild or late forms, measurement of the plasma steroid
precursor after exogenous cosyntropin stimulation may be necessary for diagnosis.
Treatment
The enzymatic defects that impair cortisol and mineralocorticoid synthesis are treated respectively with
glucocorticoids and mineralocorticoids. The consequent reduction in release of pituitary ACTH results in suppression
of the overproduced adrenocortical steroids.
24-h urinary potassium
(mEq)
>30
CT, computed tomography; PAC, plasma aldosterone concentration; PRA, panel reactive antibody.
Page 12 of 18
1/12/2012mk:@MSITStore:C:\Users\Gateway%20Tablet\Desktop\Kochar's%20Clinical%20Medicin ...
-
8/3/2019 Acth Problem
13/18
Diseases of the Adrenal MedullaDerived from embryonic neural crest cells, the adrenal medulla is composed primarily of chromaffin cells that
convert the amino acid tyrosine to catecholamines (epinephrine, norepinephrine, dopamine). Released in response
to stress, catecholamines are important mediators of the central and autonomic nervous systems. Because the
predominant catecholamine, epinephrine, has a slightly higher affinity for -adrenergic receptors, the mainhemodynamic effect is cardiac, increasing both heart rate and contractility. Combined with an 1-mediated
vasoconstriction, these collective effects significantly raise the blood pressure. Neoplasms are the most significant ofall the adrenal medullary disorders, presenting most commonly as pheochromocytomas in adults and neuroblastomas
in children (one of the common solid tumors of childhood).
PheochromocytomaPheochromocytomas are autonomously functioning, catecholamine-secreting, chromaffin-cell neoplasms.
Etiology
About 90% are benign solitary nodules found within the adrenal medulla itself. However, because they can arise any
where neural crest tissue has migrated during the course of embryonic development, approximately 10% are located
intra-abdominally in close proximity to the celiac or mesenteric sympathetic ganglia. Adrenal medullarypheochromocytomas are almost always (90%) unilateral. Bilateral lesions usually occur as familial neoplasms, as in
type IIa (Sipple's syndrome) or type IIb multiple endocrine neoplasia syndrome (Table 69.5). The multiple endocrine
neoplasia syndromes are transmitted as autosomal dominant diseases with incomplete penetrance and variable
expression.
P.437
Page 13 of 18
1/12/2012mk:@MSITStore:C:\Users\Gateway%20Tablet\Desktop\Kochar's%20Clinical%20Medicin ...
-
8/3/2019 Acth Problem
14/18
-
8/3/2019 Acth Problem
15/18
Diagnosis
The most commonly used screening test is a 24-hour urine measurement of catecholamines (norepinephrine and
epinephrine) or their metabolites (metanephrine and vanillylmandelic acid). Because many medications (levodopa,
tricyclic antidepressants, and decongestants) influence the test results, all medications should be withheld for a
minimum of 1 to 2 days, if possible, before collecting the urine sample. The sensitivity and specificity of plasma and
urinary catecholamines is shown in Table 69.7. In most diagnoses of pheochromocytoma, the total urinary
metanephrine and catecholamines (norepinephrine and epinephrine) exceed 1,000 g per 24 hours and 150 g per
24 hours, respectively.
Plasma norepinephrine, another useful screening test in pheochromocytomas, typically exceeds 2,000 pg/mL.
However, because catecholamine secretion may be intermittent, single plasma catecholamine measurements may be
less sensitive than urinary levels. Recently, measurement of plasma metanephrine levels has been shown to have ahigher sensitivity and specificity than the level of urinary catecholamine and their metabolites for the diagnosis of
both sporadic and familial pheochromocytoma.
Once a pheochromocytoma is confirmed biochemically, localization with CT or MRI should follow. Radionuclide tests
with 131I-meta-iodobenzylguanidine, a radioactive amine taken up and concentrated by adrenergic chromaffin cells,
are useful if extra-adrenal or metastatic pheochromocytomas are suspected.
Treatment
Pheochromocytoma is almost always cured by surgical excision of the tumor. The recent development of
laparoscopic surgical techniques has provided a safe alternative to open surgical techniques. An -adrenergic
blocking agent (e.g., phenoxybenzamine, 10 mg twice daily, then increase by 10 mg every 2 days until blood
pressure is controlled) is administered for at least 14 days prior to surgery in order to avoid an intraoperativehypertensive crisis. Phentolamine (a reversible -blocker) and nitroprusside (a direct-acting arterial vasodilator)
usually are used to manage any hypertensive crises that arise during the induction of anesthesia or during surgery.
When -blockade fails to control the hypertension metyrosine, a tyrosine hydroxylase inhibitor, which reduces
tumor stores of catecholamines, also may be used for preoperative management of pheochromocytoma.
Successful preoperative -blockade lowers intraoperative fluid requirements, decreases the need for intraoperative
medication to control blood pressure, and attenuates blood loss. Severe hypotension after tumor excision usually is
avoided by perioperative plasma volume expansion with normal saline. Following -blockade, -blockers are used
Anxiety 2550 Paroxysmal hypertension 2550
Tremulousness 2550 Weight loss 2550
Chest pain 2550 Tremor 2550
Abdominal pain 2550 Pallor 2550
Nausea/emesis 2550
Weakness/fatigue 2550
Page 15 of 18
1/12/2012mk:@MSITStore:C:\Users\Gateway%20Tablet\Desktop\Kochar's%20Clinical%20Medicin ...
-
8/3/2019 Acth Problem
16/18
preoperatively to control tachycardia.
Complications/Prognosis
Unrecognized pheochromocytomas are potentially lethal. Hypertensive crisis or shock may be precipitated by drugs,
anesthetic agents, surgery for unrelated conditions, or childbirth. However, with
early diagnosis, these patients have a very high cure rate. Inoperable or malignant pheochromocytomas are managedmedically with - and -adrenergic blockade. If these agents fail to provide symptom relief, metyrosine may be
added. In these rare patients, the 5-year survival rate is less than 50%.
Incidental Adrenal MassSince the advent of abdominal imaging using CT or MRI, the incidentally discovered adrenal mass (the so-called
adrenal incidentaloma) has become a common radiographic finding and clinical dilemma. The incidence of detection
of such adrenal masses is common and ranges from 0.5% to 10% of such imaging studies.
Etiology
Common causes of an adrenal mass can be found in Table 69.8 and include both benign adenomas and malignant
tumors (primary adrenocortical carcinoma or metastatic lesions). Primary malignancies that most commonly
metastasize to the adrenals include breast, lung, lymphoma, melanoma, and colon. The majority of small (
-
8/3/2019 Acth Problem
17/18
Diagnosis
Initially, the appearance of the CT or MRI scan images taken in context with a thorough history and physical
examination may provide clues to the nature of the mass. Evidence is sought for signs of Cushing's syndrome,
pheochromocytoma, primary hyperaldosteronism, nonadrenal malignancies, and adrenocortical carcinoma. Initial
screening tests shown in Table 69.9 should be performed. Patients who have a primary cancer elsewhere may require
needle biopsy to evaluate for adrenal metastasis. A pheochromocytoma should be excluded before needle biopsy is
Table 69.8 Differential diagnosis of adrenal mass
Benign nonfunctional adrenal cortical adenoma
Benign functional adrenal cortical adenomaCushing's syndrome
Virilizing
Feminizing
Hyperaldosteronism
Primary adrenal cortical carcinoma
Nonfunctional
Functional
Tumors of the adrenal medulla
Pheochromocytoma
Ganglioneuromas/neuroblastoma
Benign adrenal cyst
Myelolipoma
Intra-adrenal hemorrhageMetastases from other primary malignancies
Congenital adrenal hyperplasia
Table 69.9 Screening laboratory assessment for adrenal incidentaloma
Overnight 1-mg dexamethasone suppression test or 24-hour urinary free cortisol
Serum dehydroepiandrosterone sulfateSerum potassium
Aldosterone: Plasma rennin activity (if serum potassium
-
8/3/2019 Acth Problem
18/18
performed.
Treatment
For small lesions (