Surgical treatment of patients with initially inoperable and/or metastatic gastrointestinal stromal...
8
Journal of Surgical Oncology 2006;93:304–311 Surgical Treatment of Patients With Initially Inoperable and/or Metastatic Gastrointestinal Stromal Tumors (GIST) During Therapy With Imatinib Mesylate PIOTR RUTKOWSKI, MD, PhD, 1 * ZBIGNIEW NOWECKI, 1 PAWEL NYCKOWSKI, 2 WIRGINIUSZ DZIEWIRSKI, 1 URSZULA GRZESIAKOWSKA, 3 ANNA NASIEROWSKA-GUTTMEJER, 4 MAREK KRAWCZYK, 2 AND WLODZIMIERZ RUKA 1 1 Department of Soft Tissue/Bone Sarcoma and Melanoma; M. Sklodowska-Curie Memorial Cancer Center and Institute of Oncology; Warsaw, Poland 2 Department of General and Liver Surgery; Medical University; Warsaw, Poland 3 Department of Radiology; M. Sklodowska-Curie Memorial Cancer Center and Institute of Oncology; Warsaw Poland 4 Department of Pathology, M. Sklodowska-Curie Memorial Cancer Center and Institute of Oncology; Warsaw Poland Background: The aim of the study was to analyze the surgical possibilities of unresectable and/or metastatic GIST CD117(þ) patients during imatinib treatment. Methods: We analyzed the results of surgery in 141 patients treated with imatinib for initially inoperable and/or metastatic GIST CD117(þ). Median follow-up time was 12 months (range: 3–26). Results: Surgery was performed as subsequent treatment in 24 patients (Group I, 17%) for resection of residual disease after complete/partial response and lack of further response to imatinib and as salvage therapy in eight patients (Group II, 6%), who progressed on initially successful imatinib therapy. In Group I, the viable GIST cells were not detected histologically in only three resection specimens. The first five patients in Group I did not receive imatinib further and we observed four recurrences. In next 19 patients, continuing imatinib after surgery, we observed only one relapse. In Group II, we continued imatinib therapy after high-risk surgical procedures, but in five patients we observed subsequent progression. Conclusions: Surgical removal of residual disease during imatinib treatment may allow for complete remission in selected GIST patients after response to therapy, theoretically prolonging durable remission, but it is necessary to continue imatinib for its maintenance. J. Surg. Oncol. 2006;93:304–311. ß 2006 Wiley-Liss, Inc. KEY WORDS: gastrointestinal stromal tumor; imatinib; response; surgery; combined treatment INTRODUCTION Gastrointestinal stromal tumors (GIST) are currently believed to be the most common mesenchymal neoplasm of the abdominal cavity [1]. Their common feature is the overexpression of transmembrane receptor tyrosine kinase KIT protein detected by CD117 immunostaining [2–5]. The introduction of imatinib mesylate—the rationally designed targeted antineoplastic drug—revo- lutionized the treatment of GIST CD117 positive. Several clinical trials that have been conducted, confirm the dramatic efficacy of imatinib in the treatment of GIST in majority of patients with inoperable and/or metastatic disease [6–8]. However, complete response during The preliminary data was presented during the Poster Discussion Sarcoma Session on the American Society of Clinical Oncology Annual Meeting 2005 in Orlando, Florida (13–17 May 2005). *Correspondence to: Piotr Rutkowski, MD, PhD, Department of Soft Tissue/Bone Sarcoma and Melanoma; M. Sklodowska-Curie Memorial Cancer Center and Institute of Oncology, Roentgena Str. 5; 02-781 Warsaw Poland. Fax.: þ 48 22 6439791. E-mail: [email protected] Received 6 July 2005; Accepted 18 November 2005 DOI 10.1002/jso.20466 Published online in Wiley InterScience (www.interscience.wiley.com). ß 2006 Wiley-Liss, Inc.
-
Upload
piotr-rutkowski -
Category
Documents
-
view
221 -
download
0
Transcript of Surgical treatment of patients with initially inoperable and/or metastatic gastrointestinal stromal...

Journal of Surgical Oncology 2006;93:304–311
Surgical Treatment of Patients With Initially Inoperableand/or Metastatic Gastrointestinal Stromal Tumors(GIST) During Therapy With Imatinib Mesylate
PIOTR RUTKOWSKI, MD, PhD,1* ZBIGNIEW NOWECKI,1 PAWEL NYCKOWSKI,2 WIRGINIUSZ DZIEWIRSKI,1
URSZULA GRZESIAKOWSKA,3 ANNA NASIEROWSKA-GUTTMEJER,4 MAREK KRAWCZYK,2
AND WLODZIMIERZ RUKA1
1Department of Soft Tissue/Bone Sarcoma and Melanoma; M. Sklodowska-Curie Memorial Cancer Centerand Institute of Oncology; Warsaw, Poland
2Department of General and Liver Surgery; Medical University; Warsaw, Poland3Department of Radiology; M. Sklodowska-Curie Memorial Cancer Center and Institute of Oncology; Warsaw
Poland4Department of Pathology, M. Sklodowska-Curie Memorial Cancer Center and Institute of Oncology; Warsaw
Poland
Background: The aim of the study was to analyze the surgical possibilities ofunresectable and/or metastatic GIST CD117(þ) patients during imatinib treatment.Methods: We analyzed the results of surgery in 141 patients treated with imatinib forinitially inoperable and/or metastatic GIST CD117(þ). Median follow-up time was12 months (range: 3–26).Results: Surgery was performed as subsequent treatment in 24 patients (Group I,17%) for resection of residual disease after complete/partial response and lack offurther response to imatinib and as salvage therapy in eight patients (Group II, 6%),who progressed on initially successful imatinib therapy. In Group I, the viable GISTcells were not detected histologically in only three resection specimens. The first fivepatients in Group I did not receive imatinib further and we observed four recurrences.In next 19 patients, continuing imatinib after surgery, we observed only one relapse.In Group II, we continued imatinib therapy after high-risk surgical procedures, but infive patients we observed subsequent progression.Conclusions: Surgical removal of residual disease during imatinib treatment mayallow for complete remission in selected GIST patients after response to therapy,theoretically prolonging durable remission, but it is necessary to continue imatinib forits maintenance.J. Surg. Oncol. 2006;93:304–311. � 2006 Wiley-Liss, Inc.
KEY WORDS: gastrointestinal stromal tumor; imatinib; response; surgery;combined treatment
INTRODUCTION
Gastrointestinal stromal tumors (GIST) are currentlybelieved to be the most common mesenchymal neoplasmof the abdominal cavity [1]. Their common feature isthe overexpression of transmembrane receptor tyrosinekinase KIT protein detected by CD117 immunostaining[2–5]. The introduction of imatinib mesylate—therationally designed targeted antineoplastic drug—revo-lutionized the treatment of GIST CD117 positive. Severalclinical trials that have been conducted, confirm thedramatic efficacy of imatinib in the treatment of GIST in
majority of patients with inoperable and/or metastaticdisease [6–8]. However, complete response during
The preliminary data was presented during the Poster Discussion SarcomaSession on the American Society of Clinical Oncology Annual Meeting2005 in Orlando, Florida (13–17 May 2005).
*Correspondence to: Piotr Rutkowski, MD, PhD, Department of SoftTissue/Bone Sarcoma and Melanoma; M. Sklodowska-Curie MemorialCancer Center and Institute of Oncology, Roentgena Str. 5; 02-781 WarsawPoland. Fax.: þ 48 22 6439791. E-mail: [email protected]
Received 6 July 2005; Accepted 18 November 2005
DOI 10.1002/jso.20466
Published online in Wiley InterScience (www.interscience.wiley.com).
� 2006 Wiley-Liss, Inc.

imatinib therapy is restricted to a few patients only.Furthermore, with longer follow-up time we observeincreased progression rate during imatinib therapy. Thisimplies the necessity for further studies on new drugs inresistant cases [4,9] or attempts at introducing surgicaltreatment during imatinib therapy [10–15].
The purpose of our study was to analyze thepossibilities and the role of surgical treatment inunresectable or metastatic GIST CD117(þ) patientsduring imatinib treatment.
MATERIALS AND METHODS
We analyzed prospectively collected data of 141consecutive patients treated with imatnib mesylate dueto inoperable and/or metastatic gastrointestinal stromaltumors (82 male and 59 female; median age 55 years,range: 17–83) between September 1st 2001 and April 1st2005 at the Department of Soft Tissue/Bone Sarcomaand Melanoma of the M. Sklodowska-Curie MemorialCancer Center and Institute of Oncology (CCIO) inWarsaw, Poland. The criteria of eligibility for imatinibtreatment were as follows:
* histological diagnosis of GIST,* c-Kit (CD117) positive staining (Dako polyclonal
antibodies),* metastatic and/or inoperable lesions (inoperability was
established after explorative laparotomy and on thebasis and decision of tumor board),
* measurable disease on computed tomography scans,* WHO performance status �3,* no concomitant therapy for disease,* adequate renal and liver function.
Imatinib treatment was started from the dose of 400 mgonce daily orally. The response to treatment wasevaluated according to the RECIST criteria withcomputed tomography imaging examinations performedevery 2–3 months. In case of progression, the imatinibdose was increased to 600–800 mg daily.
In this group of patients, we evaluated the possibilitiesof surgical treatment, which was performed for two mainindications: I—-resection of residual lesions, which hadbeen estimated as resectable after maximal radiologicalresponse to imatinib (two subsequent computed tomo-graphy examinations with no further response) and II—progressive lesions, which had previously responded toimatinib therapy (at least stable disease confirmed). Eachpatient considered for imatinib treatment, and then forsurgery, provided informed consent in accordance withinstitutional regulatory requirements.
In 12 patients, DNAwas available for genomic analysisand extracted from paraffin-embedded or fresh frozen
tumor tissue before imatinib treatment. Exons 9, 11, 13,and 17 of the c-kit gene were amplified by PCR andsequenced.
For statistical computations, the contingency tableswere analyzed by the chi-square test. Groups werecompared for age differences using the t-test for normaldistribution of parameters; for other parameters with non-normal distribution the Mann–Whitney U-test was used.The Kaplan–Meier method was used for the analysis ofsurvival curves. Progression-free survival (PFS) time wascalculated from the date of the start of surgery duringimatinib treatment to the date of the most recent follow-up or progression or death. The curves were comparedusing the log-rank test. Differences were consideredstatistically significant if P-values were <0.05.
Median follow-up time for survivors after surgery inthe entire group of patients was 12 months (range: 3–26 months).
RESULTS
In the entire group of patients, 32 (23%) underwentsurgical removal of the lesions during imatinib treatment.In 24 patients, (Group I, 17%) surgery was used assubsequent treatment for the resection of residual diseaseafter radiological complete/partial response (CR/PR) nolonger responding to imatinib treatment (median durationof imatinib treatment before surgery: 14 months, range:4–32 months), and as salvage therapy in 8 patients(Group II, 6%), who progressed on initially successfulimatinib therapy (PR or stable disease, SD) (medianduration of imatinib treatment before surgery: 20 months,range: 10–31 months). The surgical procedures com-prised only abdominal operations due to intraperitoneal/liver dissemination. The characteristics of patients in bothgroups are presented in Table I. Only one primary tumorwas estimated as low-risk of recurrence and one asintermediate-risk (both in Group I) according to theNational Health Institute pathological consensus [5], allothers were high risk or overtly malignant tumors withdissemination at the time of diagnosis. Mutational statusof tumors before imatinib treatment (c-kit) was known ineight patients from Group I (in all of these cases mutationsin exon 11 were detected) and in four patients from GroupII (three mutations in exon 11 and one in exon 9).
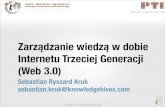
In Group I, the viable GIST cells were not detectedhistologically in the resection specimens of three patientsonly (12.5%) (although radiologically complete remis-sions were suggested preoperatively in six cases). Allother pathological examinations revealed viable GISTCD117-positive cell in variable proportions (Fig. 1).Surgical procedures in Group I consisted of seven liverresections (four hemihepatectomies and three non-anatomical excisions; in two cases combined with
Journal of Surgical Oncology DOI 10.1002/jso
Post-Imatinib Surgery in GIST 305

radiofrequency ablation of lesions in the remnant part ofthe liver, in one with crioablation of lesions in theremaining part of the liver and in one followed byresection of primary GIST of the gastric cardia after14 months), 12 resections of intraperitoneal lesions withomentectomy (in one case combined with radiofrequencyablation of a liver lesion and in four cases with partialresection of small bowel), one proximal partial gastrect-omy with splenectomy and omentectomy, one localresection of a duodenal lesion and 3 explorativelaparotomies limited to biopsy of suspicious tissue(radiological/pathological CR). Postoperative complica-tions comprised three cases of prolonged ileus treatedconservatively and one wound infection. All resections inGroup I were assessed pathologically as R0/R1. In fivecases, in this group initially unresectable primary tumors
were downsized to a surgically approachable extent. Allpatients in Group I are still alive. The first five patients(Group IB) did not receive further imatinib treatment andwe observed recurrences in four of five cases (6, 9, 12,and 16 months after surgery). The reintroduction ofimatinib again caused partial response in all four cases(Fig. 2) and one patient underwent another laparotomywith the resection of intraperitoneal remnants. Thereforethe next 19 patients (Group IA) continued IM aftersurgery, and we observed only one case of diseaseprogression/relapse (after 14 months from surgery andafter 44 months from the start of imatinib treatment) witha median follow-up time of 9 months.
In Group II, in all cases the pathological examinationconfirmed viable high-cellular disease. The surgicalprocedures comprised mostly extensive intraabdominal
Journal of Surgical Oncology DOI 10.1002/jso
TABLE I. Patient Characteristics (Groups: I, GIST Patients After Resection of Residual Lesions, Which had Been Estimated asResectable After Maximal Radiological Response to Imatinib; II, GIST Patients After Resection of Progressive Lesions, who hadPreviously Responded to Imatinib Therapy)
Clinicopathological feature
I II Total
P-value24 patients 8 patients 32 patients
Age [years]
Range 19–70 36–67 19–70
Mean 55 years 55 years 55
Median 56 years 55 years 56 n.s.
Gender
Female 10 (42%) 2 (25%) 12 (37.5%)
Male 14 (58%) 6 (75%) 20 (62.5%) n.s.
Primary tumor site
Stomach 9 (37.5%) 1 (12.5%) 10 (31.25%)
Duodenum 1(4.2%) 0 (0%) 1 (3.1%)
Small bowel 13 (54.1%) 5 (62.5%) 18 (56.25%)
Large bowel/rectum 0 (0%) 2 (25%) 2 (6.3%)
Intraperitoneally with unknown primary origin 1 (4.2%) 0 (0%) 1 (3.1%) n.s.
Primary tumor size [cm]
Median 10 cm 10 cm 10 cm
Range 2.5–40 cm 7–18 cm 2.5–40 cm n.s.
Mitotic count in 50 high power fields of primary tumors
Median 12 10 12
Range 1–70 1–40 1–70 n.s.
Time to recurrence after primary operation R0/R1
Range 2–72 months* 6–120 months** 2–120 months
Median 17 months 12 months 14.5 months n.s.
Duration of imatinib therapy before surgery [months]
Range 4–32 months 10–31 months 4–32 months
Median 14 months 20 months 15 months n.s.
Extent of disease
Primary unresectable tumor 3 (12.5%) 0 (0%) 3 (9.4%)
Primary unresectable tumorþ liver metastases 1 (4.2%) 1 (12.5%) 2 (6.25%)
Primary unresectable tumorþ intraperitoneal metastases 1 (4.2%) 1 (12.5%) 2 (6.25%)
Intraperitoneal metastases 12 (50.0%) 4 (50.0%) 16 (50.0%)
Liver metastases 4 (16.6%) 0 (0%) 4 (12.5%)
Liverþ intraperitoneal metastases 3 (12.5%) 2 (25.0%) 5 (15.6%) n.s.
Pts, patients; n.s., not significant statistically; *, for 19 patients (5 patients did not undergo resection of their primary tumor due to initial
unresectability); **, for 6 patients (2 patients did not undergo resection of their primary tumor due to initial unresectability).
306 Rutkowski et al.

resections with multiple bowel anastomoses. In thisgroup, surgery was associated with a high risk ofcomplications: one perioperative death due to uncon-trolled bleeding, one case of ileus and one case of smallbowel perforation treated surgically. Only in two casesthe surgical procedures were assessed microscopically asR0/R1, in the other six cases we were not able to removeall macroscopic pathological lesions (resection R2).After resection of progressive lesions we continuedimatinib therapy, but in five of seven cases (excludingone postoperative death) we observed subsequent diseaseprogression. Two of these patients died due to diseaseprogression in 8 and 14 months after operation.
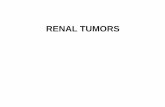
The progression-free survival curves after surgery forGIST patients during imatinib therapy in above-men-tioned groups we demonstrated on Figure 3. The detailedoutcomes of treatment of all 32 patients are shown inTable II.
DISCUSSION
In primary gastrointestinal stromal tumors, radicalsurgery is the treatment of choice, even thoughapproximately half of the patients with potentiallycurative operations develop recurrent or metastaticdisease [16–19]. In case of recurrent/locally advancedor disseminated disease, surgery is generally not curativewith 90–100% recurrence rate after resection [20]. Theimatinib mesylate treatment of inoperable and/or meta-static gastrointestinal stromal tumors with CD117-positive immunostaining is the first example of effectivemoleculary targeted treatment of solid malignant neo-plasm. The clinical activity of this small-moleculeselective inhibitor of tyrosine kinases, including KIT,
Bcr/Abl, and platelet-derived growth factor receptor(PDGFR), was confirmed in GIST in several clinicaltrials. Currently imatinib in an initial dose of 400 mgdaily is approved worldwide as the only nonsurgicaltreatment method of inoperable and/or metastatic GIST.Approximately two-third of GIST patients achieve anobjective response during imatinib treatment and further20% of cases show durable disease stabilization, yetdespite this complete remissions are rare [6,8]. Moreover,within 2–3 years of imatinib treatment approximately40–50% of patients progress showing secondary resis-tance to imatinib [8,21]. All these issues may constituteperspectives for the application of surgical treatment.There are three potential areas for surgery duringimatinib therapy of GIST. The first is ‘‘standard’’ surgicaltreatment enforced by complications during therapy, suchas: gastrointestinal bleeding, bowel obstruction, orabscess. The second objective is the removal of residuallesions, which have remained despite imatinib therapyafter previous response to treatment. The third issue is theresection of progressive disease (mainly in patients whohad primarily responded to imatinib) to overcomeresistance to this therapy.
In our study, we have demonstrated that the surgicalremoval of disease remnants may allow to achievecomplete remission in selected GIST patients after partialresponse. Approximately 17% of all patients initiallyevaluated as unresectable and/or metastatic were esti-mated as resectable as the result of imatinib therapy (andsome of them even turned resectable in case of initialinoperability). This policy appears attractive especially inview of the fact, that the long-lasting favorable results ofthe treatment of other disseminated soft-tissue sarcomascan be achieved only by administering combinations of
Journal of Surgical Oncology DOI 10.1002/jso
Fig. 1. Immunohistochemical positive staining for CD117 of gastric GIST before imatinib treatment (diffuse staining) (A) and of the specimenafter partial gastrectomy after partial response during imatinib therapy (single cells) (B). [Color figure can be viewed in the online issue, availableat www.interscience.wiley.com.]
Post-Imatinib Surgery in GIST 307

Journal of Surgical Oncology DOI 10.1002/jso
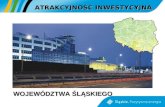
Fig. 2. GIST patient with liver metastasis (A) resected after partial response (15/06/2003) achieved during imatinib treatment (400mg dailyfrom 24/10/2002) (B,C) and recurrence after 1-year cessation of imatinib [D]. After the reintroduction of imatinib the patient again demonstratedPR (E).
308 Rutkowski et al.

chemotherapy and surgical removal of metastases. Thiscan theoretically prolong durable remission, because theexcision of the tumors is performed before the develop-ment of imatinib resistance, and thus the probability ofdeveloping a resistant clone of GIST cells is proportionalto the tumor mass. There exists a number of reportsdocumenting the common persistence of viable GISTcells after imatinib therapy as well as the development ofacquired resistance to imatinib [5,13,22–26]. Our dataalso suggest, that it is necessary to continue imatinib afterthe excision of all visible lesions in order to maintaindisease remission by controlling microscopic residualdisease. This is consistent with the findings of otherauthors [13,14,22,24]. The breaks in imatinib treatmentshould be kept as short as possible. Obviously, we do notyet know the absolute impact of adjuvant surgery duringimatinib therapy on patient outcomes and the real benefitsof this policy. According to the European Society ofMedical Oncology (ESMO) consensus surgical therapyduring imatinib treatment remains experimental [4]. Thisissue calls for further studies, but the available pre-liminary results of other authors [13,14,22,24,27] suggestthe favorable outcomes of combination of surgery withimatinib. In these series, the durable complete remissionswere commonly observed in patients who becameresectable and continued imatinib therapy after surgery.There are still some crucial points to resolve. Theimplementation of surgery at the most appropriate time is
possible only if the imatinib therapy is conducted by amultidisciplinary team directly cooperating with thesurgeon (or even by the surgeon). The optimal time forthe implementation of surgical treatment is probably themoment of disease stabilization without further responseto imatinib after observing radiologically maximal initialresponse—usually it corresponds to the interval between6th and the 18th month from the onset of imatinibtherapy. It is necessary to establish standard criteria(including molecular, if possible) of surgery for residualdisease during imatinib therapy. Imaging techniques suchas computed tomography, recommended for the evalua-tion of response to imatinib, or even positron emissiontomography, may underestimate the presence of residuallesions (in six of our patients imaging examinationssuggested complete remission, however during laparot-omy in three of them we found residual lesions in whichthe presence of viable cells was confirmed in the courseof pathological examination). It is very important tocarefully explore all sites of primarily observed dis-ease. We also suggest performing omentectomy, becausethe greater omentum is a common site of GISTmetastases. Liver metastases are usually distributed indifferent segments, so their removal often necessitatescombining surgical excision with tissue destruction withthe use of cryoablation or radiofrequency ablation. Thislatter method was shown to be effective in GISTpatients [28].
Journal of Surgical Oncology DOI 10.1002/jso
Fig. 3. Progression-free survival (from date of surgery) of GIST patients operated during imatinibtreatment: IA, after CR/PR and continued imatinib therapy (19 patients); IB, after CR/PR and stoppedimatinib therapy (5 patients); II, due to progression during imatinib therapy (8 patients).
Post-Imatinib Surgery in GIST 309

In case of progression during imatinib therapy, theindications for surgery should be analyzed individually.Although, it has been stated that in case of progressionsurgery is feasible, yet it is associated with a high risk ofcomplications and, probably, gives minimal benefits [22].We do not agree with the opinion, that surgery in focal/localized (not diffuse) progression is effective (in three offive patients with limited progressive disease, weobserved rapid progression after resection of progressinglesions). In most of these cases only R2 resection waspossible, which should be generally avoided in oncolo-gical surgery. There are some investigational methods for
the management of GIST patients who progress onimatinib. One is increasing the dose of the drug toovercome resistance, but this is effective in a smallpercentage of cases. One report has advocated thepossibility of intermittent administration of imatinib incase of acquired resistance [29]. The other direction is theexperimental use of other tyrosine kinase inhibitors ornovel treatment strategies (such as RAD001, PKC412,AMG 706, or SU11248) [4,9]. Currently, in our opinion,the treatment of choice in patients with imatinib resistantprogression should constitute of second-line experimen-tal molecular-targeted therapies.
Journal of Surgical Oncology DOI 10.1002/jso
TABLE II. Detailed Characteristics of the Initial Features and Outcomes of Surgical Treatment During Imatinib Therapy of 32 GISTPatients
No. Primary tumor site
Primary
tumor size
[cm]
Reason for
imatinib therapy
Response to
imatinib therapy
(radiologically)
Type of operation
(R0/R1/R2)
Survival (after operation)
[months] and disease status
during last follow-up
1 Stomach 10 PUTþLM PR R1 23 NED
2 Stomach 6 LM PR R0 12 NED
3 Stomach 17 ID CR R0 9 NED
4 Stomach 30 ID PR R0/R1* 7 NED
5 Stomach 40 PUT PR R1 3 NED
6 Stomach 2.5 ID PR R0/R1* 4 NED
7 Duodenum 3 PUT CR R0 7 NED
8 Small bowel 7 LM PR R0 16 NED
9 Small bowel 12 LMþ ID PR R0 14 NED
10 Small bowel 10 LMþ ID PR R1 16 AWD
11 Small bowel 20 ID PR R0/R1* 15 NED
12 Small bowel 8 ID CR R0/R1* 18 NED
13 Small bowel 12 ID PR R0/R1* 9 NED
14 Small bowel 9 ID CR R0/R1* 11 NED
15 Small bowel 9 LM PR R0 6 NED
16 Small bowel 5 LM PR R0 3 NED
17 Small bowel 20 PUTþ ID PR R0/R1* 5 NED
18 Small bowel 11 ID PR R0/R1* 4 NED
19 Intraperitoneally with
unknown primary origin
16 ID PR R0/R1* 9 NED
20 Stomach 14 PUT PR R0 22 NED
21 Stomach 10 LM PR R0 26 AWD
22 Stomach 12 ID CR R0 18 NED
23 Small bowel 10 ID CR R0 20{ NED
24 Small bowel 15 LMþ ID PR R0 25 AWD
25 Stomach 10 LMþ ID PD** after SD R2 12 AWD
26 Small bowel 10 ID PD** after PR R0/R1* 17 NED
27 Small bowel 10 ID PD*** after PR R1 14 DOD
28 Small bowel 10 ID PD** after PR R1 17 AWD
29 Small bowel 9 LMþ ID PD** after PR R2 12 AWD
30 Small bowel 7 ID PD*** after PR R2 8 AWD
31 Large bowel 7 PUTþ ID PD** after PR R1 8 DOD
32 Large bowel 18 PUTþLM PD*** after PR R1 0 POD
LM, liver metastases; PUT, primary unresectable tumor; ID, intraperitoneal dissemination; CR, complete response; PR, partial response; PD,
progressive disease; R0, microscopically radical resection; R1, microscopically non-radical resection (*in a majority of cases with intraperitoneal
metastases R0/R1 resections were grouped together due to non-reliable distinction of these two types of operations); R2, macroscopically
non-radical resection; DR, disease recurrence; ** limited progression; *** diffuse progression; NED, no evidence of disease, AWD, alive with
disease; DOD, died of disease; POD, perioperative death; {patient underwent resection of intraperitoneal residual disease after reintroduction of
imatinib.
Cases 1–19 correspond to group IA; Cases 20–24 to group IB and cases 25–32 to group II.
310 Rutkowski et al.

Another logical concept is the use of imatinib incombination with surgery in primary GIST. The role ofimatinib therapy in adjuvant and neoadjuvant setting hasnot been established yet and is being evaluated in clinicaltrials (ACOSOG Z9000 and Z9001; RTOG S0132 andEORTC 62024) [30,31].
To conclude, surgical removal of residual diseaseduring imatinib treatment may allow to obtain completeremission in selected GIST patients who had shownresponse to therapy. It is necessary to continue imatinibafter surgery. Our data implies, that taking into accountdurable remission after surgery during imatinib therapy,and followed by continuing of imatinib administration,this combination strategy may provide survival benefit. Itremains to be determined whether this multimodalapproach may exceed the benefits associated withimatinib monotherapy. In case of progression duringimatinib therapy, the indications for surgery should beindividualized with utmost caution.
ACKNOWLEDGMENTS
We thank M. Symonides MD, PhD for translationassistance.
REFERENCES
1. Nilsson B, Bumming P, Meis-Kindblom JM, et al.: Gastrointest-inal stromal tumors: The incidence, prevalence, clinical course,and prognostication in preimatinib mesylate era. Cancer 2005;103:821–829.
2. Hirota S, Isozaki K, Moriyama Y, et al.: Gain-of-functionmutations of c-kit in human gastrointestinal stromal tumors.Science 1998;279:577–580.
3. Corless CL, Fletcher JA, Heinrich MC: Biology of gastrointest-inal stromal tumors. J Clin Oncol 2004;22:3813–3825.
4. Blay JY, Bonvalot S, Casali P, et al.: Consensus meeting for themanagement of gastrointestinal stromal tumors. Report of theGIST Consensus Conference of 20–21 March 2004, underauspices of ESMO. Ann Oncol 2005;16:566–578.
5. Fletcher CDM, Berman JJ, Corless C, et al.: Diagnosis ofgastrointestinal stromal tumors: A consensus approach. HumPathol 2002;33:459–465.
6. Demetri GD, von Mehren M, Blanke CD, et al.: Efficacy andsafety of imatinib mesylate in advanced gastrointestinal stromaltumors. NEJM 2002;347:472–480.
7. van Oosterom AT, Judson I, Verweij J, et al.: Safety and efficacyof imatinib (STI571) in metastatic gastrointestinal stromaltumors; a phase I study. Lancet 2001;358:1421–1423.
8. Verweij J, Casali PG, Zalcberg J, et al.: Progression-free survivalin gastrointestinal stromal tumours with high-dose imatinib:Randomised trial. Lancet 2004;364:1127–1134.
9. Demetri GD, George S, Heinrich MC, et al.: Clinical activity andtolerability of the multi-targeted tyrosine kinase inhibitorSU11248 in patients (pts) with metastatic gastrointestinal stromaltumor (GIST) refractory to imatinib mesilate. Meeting Proceed-ings American Society Clinical Oncology 2003;22:814; abstract3273.
10. Neuhaus SJ, Clark MA, Hayes AJ, et al.: Surgery forgastrointestinal stromal tumour in the post-imatinib era. ANZJ Surg 2005;75:165–172.
11. Bonvalot S. Surgical treatment of GIST in the era of Gleevec. AnnChir 2005;130:144–151.
12. Heinrich MC, Corless CL. Gastric GI stromal tumors (GISTs):The role of surgery in the era of targeted therapy. J Surg Oncol2005;90:195–207.
13. Hohenberger P, Reichardt P, Gebauer B, et al.: Gastrointestinalstromal tumors (GIST)- current concepts of surgical management.Dtsch Med Wochenschr 2004;129:1817–1820.
14. Bauer S, Hartmann JT, de Wit M, et al.: Resection of residualdisease in patients with metastatic gastrointestinal tumorsresponding to treatment with imatinib. Int J Cancer 2005;117:316–325.
15. Scaife CL, Hunt KK, Patel SR, et al.: Is there a role for surgery inpatients with ‘‘unresectable’’ cKITþ gastrointestinal stromaltumors treated with imatinib mesylate? Am J Surg 2003;186:665–669.
16. Aparicio T, Boige V, Sabourin JC, et al.: Prognostic factors aftersurgery of primary resectable gastrointestinal stromal tumours.Eur J Surg Oncol 2004;30:1098–1103.
17. Rutkowski P, Nyckowski P, Grzesiakowska U, et al.: The clinicalcharacteristics and the role of surgery and imatinib treatment inpatients with liver metastases from c-Kit positive gastrointestinalstromal tumors (GIST). Neoplasma 2003;50:438–442.
18. Mudan SS, Conlon KC, Woodruff JM, et al.: Salvage surgery forpatients with recurrent gastrointestinal sarcomas: Prognosticfactors to guide patient selection. Cancer 2000;88:66–74.
19. DeMatteo RP, Lewis JJ, Leung D, et al.: Two hundredgastrointestinal stromal tumors. Recurrence patterns and prog-nostic factors for survival. Ann Surg 2000;231:51–58.
20. Roberts PJ, Eisenberg B. Clinical presentation of gastrointestinalstromal tumors and treatement of operable disease. Eur J Cancer2002;38:S37–S38.
21. Van Glabbeke M, Verweij J, Casali PG, et al.: Early and lateresistance to imatinib in advanced gastro-intestinal stomal tumorsare predicted by different prognostic factors: A EuropeanOrganisation for Research and Treatment of Cancer—ItalianSarcoma Group—Australian Gastrointestinal Trials GroupsStudy. J Clin Oncol 2005;23:5795–5804.
22. Hohenberger P, Bauer S, Schneider U, et al.: Tumor resectionfollowing imatinib pretreatment in GI stromal tumors. Proc AmSoc Clin Oncol 2003;22:818: abstract 3288.
23. Wardelmann E, Thomas N, Merkelabch-Bruse S, et al.: Acquiredresistance to imatinib in gastrointestinal stromal tumours causedby multiple KIT mutations. Lancet Oncol 2005;6:249–251.
24. Gronchi A, Fiore M, Bertulli R, et al.: Surgery of residual diseasefollowing imatinib mesylate in advanced gastrointestinal stromaltumors (GIST). J Clin Oncol 2005; Suppl, 2005 ASCO AnnualMeeting Proceedings: 825s; abstract 9038.
25. Bauer S, Hartmann JT, Lang H, et al.: Imatinib may enablecomplete resection in previously unresectable or metastatic GIST.Proc Am Soc Clin Oncol 2004;23:819, abstract 9023.
26. Bumming P, Andersson J, Meis-Kindblom JM, et al.: Neoadju-vant, adjuvant and palliative treatment of gastrointestinal stromaltumours (GIST) with imatinib: A centre-based study of 17patients. Br J Cancer 2003;89:460–464.
27. Andtbacka R, Cormier JN, Scaife CL, et al.: Surgical resections ofgastrointestinal stromal tumors after treatment with imatinib. AnnSurg Oncol 2005;2:S35; abstract 89.
28. Dileo P, Randhawa R, Vansonnenberg E, et al.: Safety and efficacyof percutaneous radio-frequency ablation (RFA) in patients (pts)with metastatic gastrointestinal stromal tumor (GIST) with clonalevolution of lesions refractory to imatinib mesylate (IM). ProcAm Soc Clin Oncol 2004;23:820. Abstract 9024.
29. Morabito A, Longo R, Carilio G, et al.: Clinical benefit of inter-mittent administration of imatinib in a patient with metastaticgastrointestinal stromal tumour. Clin Oncol 2005;17:96–97.
30. Eisenberg BL, Judson I. Surgery and imatinib in the managementof GIST: Emerging approaches to adjuvant and neoadjuvanttherapy. Ann Surg Oncol 2004;11:465–475.
31. Eisenberg BL. Combining imatinib mesylate with surgery forpatients with gastrointestinal stromal tumors: Rationale andongoing trials. Monographs in Gastrointestinal Stromal Tumors2004; 1; 1 and 2:9–14.
Journal of Surgical Oncology DOI 10.1002/jso
Post-Imatinib Surgery in GIST 311