REVI8H OF THE - World Bankdocuments.worldbank.org/curated/en/672701468114556663/... ·...
29
'""t} ANij TOBACe REVI8H OF THE NATIONAL FAMILY PLANNING PROGRAM July 31, 1973 Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized
Transcript of REVI8H OF THE - World Bankdocuments.worldbank.org/curated/en/672701468114556663/... ·...

t ANij TOBACe
REVI8H OF THE
NATIONAL FAMILY PLANNING PROGRAM
July 31 1973
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
wb350881
Typewritten Text
53182
TRPnnAD AND TOBArO
nEvT Fcl OF THS NATIOAL
i AmLY PLAiNING PROGRAJ1
Page No
i
I In roducion
II Or~ani7ation of the National Family Planning Program bullbullbullbullbull
III Present Status of thE Program bullbullbull 4
IV RE comlerdations 8
A oIulation Co~~cil bullbullbullbull 8
B A ~tatutory COUT1cil II II 9
C Office of the Fad 1y Plannin~ Program bullbullbullbull 11
r Deerttlal1zati ~ ~cjCImiddoter=J ~ ~I ( 12iii
Ircegration or Fltj~Ly llannirg with Maternal and Child Health Setvices bullbullbullbullbullbullbullbullbullbullbullbullbullbull 12
F Voiuntary Organi zations bullbullbullbullbullbullbullbullbullbullbullbullbullbullbullbullbullbullbullbull 14
1 Program Information bullbullbullbullbullbullbullbullbullbullbullbullbullbullbull 14
~i bull Field Workers bullbullbullbullbullbullbullbullbullbullbullbullbullbullbullbull 15
1 Mauagement Study yen bull bull bullbullbull bullbullbullbullbull 16
ANNE~ES
1 - Names of Persons Mat 2 - Clinic Case Card for Fimily Planning 3 - Daily Register
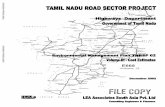
Chari Orgmization of the National Family Planning Board
This report is based Oll the findings of Mr RN Madhok who visited Trinidad and Tobago from April 9-23 as consultant to the Population and Nutrition Projects Department of the World Bank Mr RlT Madhok was formerly Additional Secretary Ministry of Health and Faroily PlaJming Government of India
1) rle Youc fUfCt1 oning in an atmosphere of Lncertairbully n(It-oL2 in the National Family Planning
amp11 t~ms c frence cf the Council should be
(ii) The PJPl1~atcYl CcmncU should be strengthened by including in it (a) the Permanent Secretary Ministry of Health (b) the Principal He(lical Officer in charge of MCH and family plannlng services () 8 representatlve of the Ministry of -inance (0) social scientst and (e) a representative dtich of the aSRociatioi1S of the medical nursing and teaching professions and cqantzations for womens welfare
(Hi [he Offh( ci h F Planning Program (Program Office) hould be strenghened by augmentation of staff at the professional as vel1 as supportive levels after a work study Ir ramptLicular a demographer a media expert and a trainingsdviseT should be inducted into the agency
(a) set anntncGgpts for the enrollment of acceptors at each cliniccenter and monitor progress in relation to these tarets
(b) establish schedules of periodic inspections of clinics
(c) cvnlvl 11 hlufltfmiddotr lgt1~n for the training of personnel and
(d) wor (ltH U 8t(nte~) for Tued1a communication in the light of public awareness and knowledge and the reach and cost-effe~tiveness of different media
v) The Ministry of Heath should invite suggestions from the Director of the Program and the Regional Directors with regard to the deshycentralization of administrative and financial powers currently ves ted in the 11ni8 try and work out a schedule of powers to be exercise tdltclcr )ve of Program adl11 nis tration
F~eld Workers
(vi) A cadre of field workers should be created to promote the accepshytance of family planning in the community As an experiment one such workar may be assign~d to a unit of 10000 population
(vi t) 1ne orgai c Y1 anlti j~lrcgemeu of the Program should be reviewed cmjoLntlyamly pcanning expet and management consultants
r L the fr]lcwing topics
a) thc 1lt0 V 71rmiddotlCi f Cn1t1t structure comprising the ~inis ill Hnal th ~he Ppulation Council and the Prc~r~1 Office ~te feRsibility of alternative models of inatit~~iacnt ~
(b) the s taft re(luirements as well as operating procedures of the Program Office
(c) the ltitin n t[iv and financial powers exercisable by Program uthori ties at different levels in relation to dgtE le31H of lesponsibili ty
(ci) trc JlU l1 of coordination and supervision of
(e) the staffing and working procedures of integrated MCH and family ptanling clinics including family planning counselling 8eVmiddot Ck ~UITli s Rilet recording of data As a part of the study ~ Ulti~cti(ns pe~iolmed by each category of staff - shyme6ic~1 rn ijed lerical -- should be examined to idemi whimiddot rune dons can appropriately be relegated to che next tower level so as to optimize the use of available ma1pow~r
(f) the system of flow of program information from the field and its processing and utilization in the Program Office
(g) he ost-ParttmPo13-Abortal Education and Referral Program and
(h) the requirement of field workers for conununity education creation oE ltiemand for family planning services and conshytinuous c0ntGci with acceptors (The type of functionary needed content and duration of training and the norms of work should be suggested)
I INTRODUCTtflN
101 0-1 behalf of t~ H~1k ~middotmiddotr R N Madhok (Consultant) visited Trini12d ad Toblg0~ middotl iL bullbull ~)3 0 review the administration and mal1agme)t )f thlt hsd j 11]) PVnning Program During his stay in Trinj dad 1- MadhJk ( iilh eprefEntatives of the Ministry of Health and the Topu ation C01Jii1 fuJI li5e appears in Annex 1)
102 ~pecifgtUy ~~C iVlsdhokcevievled the following aspects of the progam
a he future role of the Population Council -- whether it should )euro an advisory or all (~ecutive body its administration staffing and statutcry pmrer under a changed set up and the consequent changes required in theliinistry of Health for the implementation of the prc)gram
~ J the extent of (l~i-5ting (Jpcfntralization of administration of health and frunily planning services and its efficacy
c the desirabiLty of integrating family planning with maternal and child hcaLh services in the light of experience of inteshygrated i~lirJ(
d the efficie~ Cf~ll edsirg system of the flow of program information ac ~Hl red charges and
specific aspects of manager-lent and manpower utilization on which the management finn should concentrate during its study
103 The following report contains broad suggestions on changes rE qui ed in the existtYg structUrEgt
II ORGamp~IZATION OF THE NATIONAL F~~LY PLANNING PROGRAM
201 The administration of the National Family Planning Program is the rl~sp(jnsibility of the Ministry of Health In 1967 when family planning was adopted as an official policy the Health Minister at that time proposed the stallishment of a Population Council to advise the Minister on the organizashy1ion of a natiorlal prorrun 1i(h lIIotld coordinate all family planning effort n tle country Tlle Cabtn2t c~ciCled that
A Population Council of Trinidad and Tobago should be instituted for the purpose of giving overall direction to the Family Planning Program in Trinidad and Tobago with a view among other things to coordinating all fanily activi ties in the country II
- 2 shy
202 In pursuance of t l= foregoiny decision the following terms of refer nce were framed for the Po1)ulation Council
10 i~vll ditcoction to a Family Planning Program fo Y ltdd cHl T0bagn d th Ii view among other things to eo ~ ~c n lfllonrdnr activities in the
203 A PTOlllH~ f(cibor nf ttl rredical profession was appointed as Chailman llei the lill~1L y h2 jiamily Progran Ministry of Health as the Secrltar r (r th C~-ur~ ihe membership of the council comprised officials of tle t-instry of He3ltii and other departments representatives of the volultary agencies operating family planning services and leaders of opinion the present Chairman of the Council is an eminent gynecologist in privmiddotte practice and a former Minister of Health the members are as foIl 08
1- Chief Medicnl Officer MOR -l Spcclliflt ~middotjJ3C Officei- General Hospital
3 A rEpr~senative of the Ministry of Planning and Developneut
4 A represehtacive of the Central Statistical Office 5 Public Tidaions Officer Prime Ministers Office 6 ~ PrilLj~d t1lt dq Officer NOH 1 ~e( CL bull ~clmiddot ~~t)pulati on Program H Chid ~ea~h Educatoi ~lOH
9 A repres~rltatiVE of the Catholic Marriaie Advisory Council
10 amp 11 Re~)resentatives of che Family Planning Association 12 6 13 M~mbers or the Publi~
14 Diector Family Planning Program MOH - Secretary
Olj The Population CQtJrdJ hal three roles (a) policymaking ll) I rogralil formulation and evaitllt1()l and (c) providing general direction fllr program implementation Its composition is designed to ensure (a) intershydapamiddottmental coordination withill the (overnment (b) coordination between the ( Ole-nment program and the activi ties of voluntary agencies and (c) rapport vith pblic opinion
05 The Population Council is assisted in the task of program formushyIation by a numbe of committees ~thich are so constituted as to draw upon Ihe ex lertse avalIahI wi tlin the Government as well as outside Pre-eminent arnorg heseuro commictees s lhE lati()nal tH Program fnLMulation committee ihi(h technically speakirg is not a committee of the Council but a commitshytee of the MOH It inter-meshes with the Council since it is the policy of the Government to integrate family planning services with MCH services delivered through the network or health centersoffices of the Ministry of Health This committee is headed by the Principal Medical Officer of the MOH in dnrge oE Integrateci 2~edicil Care now restyled as Community Services
- 3 shy
which COlT bull Se 11CH anii IIgt sxvl(s I1H~ other committees are Community Educaior and Publidty Cvrm] ttec Research and Evaluation Committee Family
~du aton Comrnirii ~~e(i] CCimittee and inance Committee
OS i~ n1eptUd~ i p Ni ~runi t 1 an advisory body and as such itus 10 execl1lt)ltjmiddot n p-actice the Office of the Family Planning Prog) am e tabisLecl wirgtmiddotcn tilt2 middotlnitry of Health functions not only as the ecr ~tc dat of lIC )hiCJl but also as the instrument for carrying out lis lirEctvls Furtiie ch GOtdcCU has concerned itself nomiddott merely with broal i~ SUIS f10Hc out also vL detailed implementation The majority of t le r emmiddoters of rhe Council are in favor of Umi ting the Councils role to tile givlng of broad direction to the Program
20i The Office of thl~ Fitli1y Planning PrO~rall1 is comprised as follows
Dlrcct0r (Incant) Medilal OfHceuror (Famtly Planning) Nm-~If Offieer St~tistical afficer Health Educator 2 lield Workers (for follow up)
(OIlE positor vacant)
8CCiHWlcnt 2 clexks 2 typists 1 driver 2 proj ctionis 15 and 1 messenger
T- ~ g af f of the Office of the Famly Planning Program is under the discipline of thttinistry of Health since the Population Council is nei ther a departshymfntal unit nor a separate legal entity with its own fund
2 OB The places of )nrm1 atton Council and the Office of the Family p ~anr ins Program wi thi n the Minis try of Health as conceived originally by tile Government may be seen in the abbreviated version of the chart appearing hI different official documents and reproduced at the end of the report
~ 09 In April i973 at the time of the consultants visit there was In aCIDc)sphere of uncertainty about the administration of the family planning l)rogram as a result of changes in some of the top positions As a result of t c~binet reshuffle the portfolio of Health had changed hands The Permanent euroctet lry who is the princ~al ad~liser to the Minister was new as lras the r-i c al Yedic1l Officer h charge of Commurity Health Services (Mel[ and Pam ly Pl1nnhg) The Dtnct0 of family Planning who was managing the Office of middothe Family Planning Program and also serving as the Secretary of the PoshypUlition Council had reCiTed in March 1973 and a successor had not yet been named Meanwhile the Medical Officer for Family Planning (a part-time employee) was carrying out the functions of the Director in addition to her OWT Wi thin the Population Council the advisory agency for policy-making
and ccord~n8tionJ there was a groHinr feeling among the members that the ouncl1 510t1d shed thE respOJ1sibili ty for implementing the program a funeL on j ch nad heuroe added on to its advisory role with the passage of time
iO the 1 ~lp~1 the lines 0 responsibili cy were not clcay (e ned and Li1 refioal system was not fully functioning The post of Re ior 3 Director crth VIas vacant The policy seems to be to strengthen the 1St tu ion of Pt()1ic Flealth Office as an 3ency for the supervi-middot sion)pound ne district sflVices (health centers health offices and school servi ces ~l thin the ccnmty
II I PRES EN STATUS OF THE PROGRAM
301 ~he adl1linistrt~ivE changes narrated in para 209 have come about at fl tin e IJhen the P1ogram has entered a phase of declining performance as is 11 Jpal en from th colloHing figures taken from a report submitted to the Populaton Council
YrUL 10C7 ~j8 1969 1970 1971 1972
--- -- ------------~~ --~ - shy----shy
Ne Acceptors 3696 2731 16207 9997 9898
(End of October)
7560
Slur~e Family PlAnnto Program Report (no date)----AsII1Ulilg that th6 ttlrollmant of new acceptors during November-December 1972 prclrd at the 8ame rate as during the ten~onth period January-October
- 9i2the total enrollmslt in 1972 would be lebullbull than 8500
3(12 lhe total number of leW i-iCCeptors for 1971 shown in the foregoing tal11e 1s at variance with the following data from the 1971 Allnual Report
- 5 shy
~ev C~~ Contraceptive Method and Agency
nm Other Advice Total New Cases
Aeny
GovrrmenC ProEllil ___~zZ(lt1____ 97____2Lbull499___~528~___4i_750~_
Farr Uy Planning Association 2814 315 607 76
Catholic MarriaAdis1ry COLnc_H____
ge
74 88 162
otal 31[10 692 8724
_--__------------------shySOlrce Natio
1973 nal p
Fam29
ily Planning Program 1971 Annual Report April
NevmiddotrneJl~ss) the declining trend in annual performance after 1969 is manifest ana conpaes unsatisfactodly to the following targets set for the Program
Targets for Contraceptive Users - 1968-72
New Accep tots Old Cases Total
1968 20noO 20 000 lO noo
1969 20000 40 000 60000
1970 20000 60000 80000
1971 20000 80000 100000
-----__shySource National Family Planning Program
p i9
------------------------------------
- F shy
3JJ3 Ttl flient recrvitTrent has fallen off since 1969 in spite of a signif Icar t xpansinn ir the number of Government health facilities providing family paarin~ services FrCli1 7Hr to year Starting from scratch the number oE GovE(nment health irlstitl1tions delivering family planning services in isollL(Od ~ily pltJfAill~I ~J in c)lchiratinn ~7ith MCa services has lWW risEn t 4 lhis ie --tdt)p to t cii1ics organized by the Family Plannin Asce1ation bull U2 by tile Catholic Marriage Advisory Council which offers the ~h)lthm meti1middot1 nT
304 1i ciecli ne d~ d re11~m2nt of new acceptors coincidentally w-Lth th~ eXlsioH uf s-crLce facilities needs to be studied to identify the factors responsible for it eg the quality of services offered the strategy of commmic at~on and motivation and management and supervision One obvious gap is he abgtence of an agercy for promotion and extension of demand for family lal 111 If services -gt tLe field reliance being placed mainly on clinic counseUn H1d generaUzmiddotd mass media publicity The need for a field promoshytional agelcy is underscored by the dropout rate In 11 draft paper prepared by the Hed_cal Offic(1r for FIrnilv Planning it is stated that by the end of 1972 t ile Heuroe approxiclt ji rHJC cun~ent users of contraceptive methods and 33 per ert dropouts
305 rht~ program is cot merely clinic-centered but also female-oriented Recent Iy mellsages aimed at m11es and stressing joint male-female responsibishyIi ty l gtT j ecillc CImt-J 1 i~gtVt~ b~~in )7cn 1n0 the cOTul1mication activity sUf1 tv) c nts Em he 2iucaccw i milc8 and che distribution of condoms to them illVC he ~n or n~d iD r GJvefl1nenC s(~ctor The Family Planning Association has a130E~k11 the irti U3 1V~ to reis ter males ln industrial employment Tllese are steps in the ri)n dtrect1ongt but the size of the problem indicates the n~ ed OI a concerted effort en a much large r scale
306 Tre Program relies largely on the use of oral contraceptives as shown in the following table
Oral Other Advice Contraceptlves IUDs Methods Only Totals ( 100)
19)9 76 20 16207 ( 100)
1970 316 63 9997 ( 100)
1971 50n 4n 365 79 8724 (100)
Family Planning Association unpublished report
----
- 7 -
Althougr amJnp the neH acceptors in 1971 the users of oral pills were only 509 ~mon~ the old cases the figure was 119 The percentage of IUD users has remiined stagnant at an insignificant level this may be partly due to consume prefErence and pctrtly outng to lack of trained staff to undertake IlTD i1srti l7U There h hOHever a visible shi ft towards the uSe of othe~ ilettods (npchani81 and chemical) attributable to a scare about the side efects nf oral connaceptives Among these conventional methods the condom s 11 os popular
307 J t )resent fami ly planning services have been extended to 48 out of 106 hellth centersoffices run by the Government and the objective is to C)Vel t1e remaining health centersoffices within a short span of time so that adice and facilities for the practice of family planning are conshyvenient Ly wa nable to the people in all parts of the country By ann large sepanit e fITti ly planning eli nics are held on specified days as an addition to norrral lealth work Besides doctor sessions at the clinics supply sessions are rur by health visitors and nllrses assisted by clerks The nurses are authorjzed tc issue oral contraceptives for a period not exceeding three months ani the acceptor is required to attend a doctor session for advice during thi jnterval In 1971 the numbers of full-timepart-time staff in Gov~rtmnf centers renderinp family planning services were
Full-time Part-time
1elical Officers 14 8
NUseMidwives 35 19
Cl~rks 3 17
Now tile low~rnment -gtbjective is to integrate family planning services into MOl services and use the same staff being used for the delivery of both types of erlices at multi-purpose sessions However so far only 1A centers have interated family planntng with Men or gpoundmeral hpalth care sessions
3011 The Family Planning Association has eight unf-purpose centers where famil) pLmring services are available ftve days a week The Association employs tilrEe full-time and ttJO part-time doctors a complement of 14 nurSeS (who llave been trained to do pelvic examinations) and 11 other clinic staff membels The Association also has a number of voluntary workers in the clinics The CithoUt Marriage Advisory Council has three clinics but their contri shybution in terms of enrallment of acceptors is not signiflcant
3)9 A Post-PartumPost-ALortal Program was started in 1969 It is state I tlat about 14 percent of the patients reached attend a family planning clini~ 1iTj thin six weeks of the interview in the wards IhiR is qui te a low figur In 1970 when a system of home visits was tried under the Family Planning Aide Project in 7 clinics the rate of acceptance doubled in three clinils rose by 50 percent in two clinics and increased by 24 percent in one clini (No change was noticeable in the seventh clinic) No decision has been Inad~ tmiddot) continue extend or modify this Project
A Po~ulaton Council ~-----------
401 he fu~ura ro~ Lh~ ~~~01ati0n Council has to be considered in theli1 A the tasK t~ lL ahead of the ~ational Family Planning Program At pesent tile officil~r(QSrJ1Tl is prirnarily concentrating on two objectives (a) tIlE excpound1sinrt of fmd plannin~ services to tie remaining 58 health centen cLJs as rapi(ily as possible and (b) the integration of family planniT g VI tr MCH services Thus thG administration of family planning serviCHJ will be merged into and become part of the Community Health Services Since t is ()rganizationally undesirable to disturb unity of command a separa1e elteecutive agency for the administration of family planning services is preempted within the existing policy framework An executive role for thp Pcnulc tinn Council is there fore ruled out on this consideration
402 If the Population Council is to function as an advisory body at the p()Lic~ aId progra1l pLilnni-l level snd not to concern itself with the minutile If program execution there wonld be no advantage in giving it a statutory stltuS But if it were the policy of the Government to set up a verticll )middotro~ram for family planning ii th a field organization separate and distir~tOroll the HeaHh administration it would be quite appropriate to establish an autonOiTiOUS statut()y a~fgtny ntside the departmental setup of the MinisiY of Health d~b a budi~t md staff of its own commensurate vith the rE spo lsi hi Ii ty to be rEs j Freed from the usual departmental conshystrailts ~n the matters Cif sp(ndlng a1d hiring and firing of personnel such an aglncy c(uld move faster than a heavy-footed departmental formation wi thin a Mins trl bull Hovever a hody of this eharacter would need to be cas t in a cliffe ent m(ld than the present Population Council The shape that it would take lrould be more like a Board of Management with a full-time Chairman or Execuive Director and with more functional expertise than representational charater But an advisory council with an autonomous status and no responsishybilit f( r lrogrrun eXIGulion iould be a source of friction
403 r~e existence of the Population Council as an organ of policy advici has certain advantages Firstly it is a forum for developing a national poLicy in which officials and non-officials participate Secondly it pr )vi bulles a focus to ti1e official program vhich it otherwise may tend to lose as ~ontraceptive services are merged into the general health services Thirc lymiddot- and this is important -- the Ministry has extra-departmental advice availabL to it~ but the Ministers constitutional responsibility for the condl ct )f the national progl~lt~ le1lains unimpaired
404 ls an advisory Q(dy the Population Council should be more broanshybase( than it is at present For instance it should include representatives of tile organizations of employers and vorkers associations of the medical nursngmct teaching professions and organizations for womens welfare The Counil should also haye a social scientis t on it On the official side the
- 9 -
Permane It Secetary and the P1O (fen and FP) should be brought into the Council he inclusion of the Permenent Secretary would open a channel of communi~aton with the MOR ae the highest policy level next to the Minister and would (ontribute administrative expertise to the deliberations of the Cou1ci1 ~m f icili tali 5 (pleuenrti)D of th~ recommendations of the Council within the -rni and in OUltL depa-cments The inclusions of the PMO (MCH and FP) wOlld el) emphasi ~2 hs responsibi lity toward the family planninR program Some officrs of the HOH (eg Chief Health Educator Principal Nursin~ Office e) may 111 ea~e to be members though they may attend as requirE d nmiddot the agenda before the Council A representative of the Ministry of Fin nee stQuId be inc~uded in the Population Council This would make for a lettr appreciation of the needs of the Program in that Ministry and fadIi ate fj nancial sanct ions
B A~tatutory Council
40S In the foregotng Pgraphs the view has been expressed that within th edsting policy framework an advisory Population Council would be more tli)prcpriate than a COlincil wi th executive functions and powers that an advisory rOUlcil would not gain by having a statutory status and that if a statl1tory body 5s to be set up in lieu of the existing Council it would need tC b structured more Iiice a Board of Management than a council wi th a repre13entttional charact~( n the latter event the statutory council should have fu 1- time Executive Chairman or failing that an Executive Director functj oni1g undel- a Chairman trno can devote considerable time to the business of tlw COlncil
406 T1e Statutory Council should have its own budget with full operashytiona pOlo1ers It should have the authority to appoint its own staff and regulLte their conditions of service If it is constitutionally possible the Couner1 shollld be outside the jurisdiction of the Public Service Commission in pesornel matters
407 As an instrument of Government the Council should be subject to such ~eUfral or specific directives that the Ministry of Health may issue to it frcffi ime to time This should be written into the statute under which the Cmntil is set UD
408 The composition of the Council ould depend on the functions assig1ed to it It is suggested that the Council should not concern itself wl th the delivery of cliric selVices in the field The Ministry of Health may (ont nue to administer rampmily planning services at Government hospitals health cmters and health offices and the voluntary agencies should run thei] OWl ~rogram The following functions may be handled by the Council
- to shy
s rrogram plannin and target-setting
b proram monitoring and evalllation
c wiL of d 1ci(JTIdnCf by inspections
d Qrg8lizatim 0 es and marketing of contraceptive J~1J-s BLl (iV es at subs idi zed rates through es tablished 1 2 d(~ channel
e information mass media communication and audiovisual ublicity in the field
f prorrotion of famil~r plannIng acceptance through face-to-face cotlmunication by poundi eld workers in domiciliary visi ts
g trIining of personnel
II pr )motion of -esearch enJ
i financial support to voluntary agencies providing family planning services
409 n Statutory CCii1cil may corsi5t or an eminent non-official vith a comri tm ~~1t towacds foJlily plailninf nd the fol1owin~ members
I ~ bull Pfrmanent Secretary ltl-tIlH
Chief Hedical Officer HOH
i Principal ~ecHcal Office ~mH
d Pilhlic RellltionB OfJte(middotmiddot Prtm~ Ministere Office
A represen ta ti V~1 of the Ministry of Education
f ~ representative of the Ministry of Finance
g A representa~ive of the FPA
h A representative ot the C1AC
i H social scientist fcum tle University of the ~Jest Indies
j Three non-officials with experience in management and administration and the
k Director of the Family Planning Program - Secretary
- 11 shy
The COUlcil ITIltW constitute cOlClmittees for Finance - Accounts Personnel and Sup lies nd Stores ir~whi ch )nly members may be included Other commitles sc1h as those 01 training info1nation and education and researCl ara ~valuation r1ili also include experts from outside
410 he Off1ce raquo) cc im Panning Program which at present forms part of th ~Hnis try or [i n should be placed under the Council and its staff strelgtl ilcn~ii2 i~ r181 it may cease to depend upon the services of the Mir is t y of H~alth
C Office of the Family Planning Program
4 11ollwther the Offic~ of the Family Planning Program remains a part of the Mirisry of Health or is transferred under a statutory council if one is set uP i needs to be strengthened to meet the requirements of an expAndshying pr )gn m At present the following sys terns need to be ins ti tuted in this Office
a a 3ystem of setting annual targets for the enrollment of acceptors and the projection of service fadli ties in relation to these targets
I Ci ~ystem oE V)glC loHitoring (the monthly statistics flowing from the clini~s c~iiiain unproc(~s5erl for months)
a system of program evaluation eg demographic effect of tte program cost studies
1 an overall design for media communication based on a study of the reach a~d cost effectiveness of different media and the effect of the meflBsge content and
e a m88t~r plan for training which would comprise an assessment of the training needK of the existing staff and future reshycruits and a long-term plan divided into annual programs
412 Th2 Prograll afiie s~lould have the services of a demographer and a meeia expert A training adviser is expected to be provided by the PARO
413 1be Program Office should evolve schedules of field tours to overliee field operatio1s E~1eh health cente heal th office should be visi ted peridicaLy by the Milt~dical fElce- the Nursing Officer and the Health EduCltoI who should guide and assis t the local staff in carrying out the progam Their tour notes should go into separate dossiers for each institushytion and ~ach dossier should have basic demographic data about the area coveled by each institution These dossiers would be a useful record for revilwing l)errOmance The staff of the Program Office should be augmented to Ol)erte this control procedure
- 12 shy
D Decentralization of Powers
414 ~hete is a concentration of administrative and financial powers in the 11in s try of Health I-JllJCi1 results in an accumulation of references in the Miristl) and delays n field operations Specific powers should be delegated ~o (a) the PliO concerned with MCH and family planningmiddot (b) the Directcr o the Program Office (c) the Regional Director and (d) the County Medica1 Oficecs The Ministry should invite suggestions from these officers and wOlk 01t a schedule of delegated powers
415 A tdgh priority in the matter of delegation of powers is to arm the Regiond Directors with sufficient administrative and financial authority to implement with expedition the health and family planning programs of the Ministmiddoty 1 thin the areas in their jurisdictions
E Integration of Family Planning wi th Haternal and Child Health Services
416 At present family planning services are being provided at 48 Goverrnent hospitals health centers and health offices by using the full shytime E taf cf these institutions and employing part-time (sessional) doctors nurse~ anI clerks where necessary At 29 of these institutions separate famil cl~nics are held on specified days in the weck some being doctor sessi(ms mel others supply sessions run hy nurses and clerks At the remaining 18 imtit1tions family planning services are combined with antenatal child healtL cr postnatal services The Family Planning Association runs 8 unishypurpoe f am ly planning centers which provide daily services and contribute a 11 t le less than half the total number of new acceptors per year
417 N assessment has b~en marie of the effect of integrated MOl and famil~ p~ nnning services an the recrl1i tment of acceptors nor were ~ data readily avallable for this purpose It may be observed however that in a situation of shortages of trained personnel for health services utilization of the existing health staff and facilitieR for family planning is inevitable parU cllLrl y in the interior where such shortages are more pronounced This underlines the need of evaluation of the integrated xai and family planning progtam for its impact on the number of acceptors Also a study needs to be made of che utilization of medical and pilramedical manpower so that it leads to bdter ~llocation of duties and optimUJl utilization of personnel
418 ile integration of faMily planning into Mcn services has certain advalltages as well as attendant risks The advantages are
a Lbe association of family planning with the care of mothers and children helps project a benevolent image of family planning as a program of family welfare This creates a
- 13 shy
1imate favorab~e to the acceptance of family planning aa lt p-)si tL1e il-Eare rreasure rather than a negative program cE limiting c~ildren
h t elps erlist ~r2tion tf doctars and nurses who as c -~ass enjo tft~ Y)er)et~ a~d confidf~nce of the communities i712~ Eerve
c ~ieD of contact with women
d luni-purposa clhlics for ~lCH and family planning services are onenient for motn~rs who would have to travel considerable (listances to the clinics
e hete is better utilizat1on of Acarce heAlth manpower
419 he limitatio$ of integrating family planning with MCH servicesI
are the posiOili ties of loss of focus on family planning as a high priori ty prograrr ald the diffusion of pol1sibility for its implementation These could tlow ve r he safegurded agaifls t by adopting the following measures
a 11e job descriptions of doctors and nurses should be rewritten 0 include the family planning function
b hE perf0rt1iai1ce of ctoltors and nurses should be judged as much )y tbeir inteceq t in planning ~vork as in maternal and ~hjld care and this should he lade known to them
c )octors and nurses involved in ~CH services should be given middot)rj entation and traIning in famj ly planning and their interest 3UEtained by refresher courses seminars meetings and supplies of literature
d Thl techrical (xpert~ in the Office of the Family Planninl Program should maintain liaison with and guide the field agencies in implementing the family plannin~ program For this purpose schedules shoul d be marle out for periodic field inspections
420 It is suggested that the working of half-a-dozen centers where family plbnnLng services have been integrated wi th MCH sessions should be studiei for ehe purpose of standardizing the methodology of delivery of servicl~ Such a study should include staff strength patient load recoril shykeepills 10middot of patents in the clinic timing and frequency of clinic sesaios ani convenience vf patients
F Voluntary Organizations
421 I i~ internrticri31 expedence that the birth control movement is pion aTC tt volunh[~ JilC S Qltl that hen the national governments step in wi tl cmbi ti 019 prjhns wi thin the sLate welfare system voluntary bodies ieh tteir limited ilsrluces restrict their service activities and shift the emplasi i 0 educedgt (f the community training research and contracepshytive Sf vic not 1l7gtilflblr in he official program or in areas not reached by it In nagni tude and expanse the of ficial program in Trinidad and Tobago has alrad~ orertak~n Ce 101umary program Increasingly it will become the domLnart tartner in the total national program while the voluntary agencies will cOltirlU1~ to receive financial support and encouragement to set up high standaeis If service and explore new areas thus acting as a stimulus and an additi_e tl the official program
G FrOB-ram Infomation
422 Thre is no concurrent evaluation or monitoring of the Program The daa or lq72 flowing in from the clinics month by month have r8Jllsined unprocss~d tn the Program Office The official Annual Report - 1971 Sums up th~ poition as fcllo~s
ITThe Research and Evaluation component continued to be the weakest in the Population Program Although a systen of evaluation had been built into the program the follow-up procedures for analyzing the data and for correcting inshyconsistencies are inadequate Requests were made to extend the staff to establish a more viable unit but by the end of the year no chllnges had been made
423 T1e recording and riporting jJrocedures were revised effective Januery 1972 and there has been a further change recently at the instance of t1e Evaluation Adviser Under the system now established the clinics are lequ Lreurod to maintain the following records
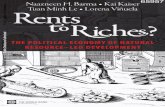
a Family Planning Clinic Case Card - New Cases This was introduced on January 1 1972 and has thirty-one entries giving age parity contraceptive listory pregnancies socio-economic background ource of family planning information and agency for notvat ion bull (Annex 2) The case card is made out in duplicate for each new acceptor and a copy sent to the Program Office
b Daily Regis ter This fs a ne~gt1 form recently introduced in replacement of the old regis ter and is preparen
- 15 shy
ie) ruplicate the original to be transmitted to the Program (fHce and the carbon copy to be retained in the clinic Th~ is a very 121zborute form requiring 36 entries to be aa~ for each Chse nel and old attending a session includin~ (ntries to cit L to contTaceptive supplies issued
AijCleX 3 T~13e fcnnG are required to be sent to the Program lffce in i7JO balches every month the first batch for the i IS fif~eeL days and the second for the remaining part of hE month The trtention is that the data appearing in the ~EZlic daily legis ter forms should be compiled in the Program Office and fed back to the clinics Although it is claimed that this new form has been pretested and is workable ex)erience alone will show whether the majority of clinic cL~rks are able to cope with it in a busy session
bull o now-Ho Card TIlis card is intended to keep track of ac ceptor--It has entries for name addresfI and month fcr which a visit is due for each year
bull Aphabe tical Index This is a card index of clients with aidresses
Each i)at en is given a simple clinic card on which the dates of further appo~utnli rc3 an~ indicated A special fonT[ has been devised for the reporting ot cases unler the Post-IartumPost-Abortal Education and Referral Program
424 J system of monitoring progrRm performance from month to month need to bE develQped as a high priori ty The problem is not so much reshycord ng mc transmission of data by the clinics but its aggregation and proclssi ng in the Program Office every month which at present takes a long time The Statistical Officer should have a statistical assistant to help him Ln I he taflk Monthly progress reports should be available to the Mini H t~ n H(llllth and A11 offt eerlil of the ProKrnm Office so that remedial ac tl m I lAY h(~ tuk~n n rll1u- WhOnh1f ~Hfl(AlJtlaTY
42 For the analysis of data and evaluation the Program office shouln haVE th(~ full-time services of a trained demographer
H Field Workers
42) Tie Program nemiddotis tne services of a cadre of field workers to enr)ll neii aceeptoTs follow up acceptors in their homes and revive the int 2remiddott of dropouts Such a category of workers could also be utilizerl for pr1fficting other health programs such as the VD campaign and the inmuni~ation program
47 As an experimental measure one field ~]orker may be assigned to a emi l~ of Hi 000 population This would mean 100 field workers in all
- 16 shy
Earh of the workers should preferably have harl a higher secondary education otherwLe 1gt junior secondalY education They should be married persons with middoti1ltt mot tl-an two or tlree children recruited from the locali ty in which they armiddot~ requlred to function Only persons who have the capaci ty to comnunl at~ and or6anl~e should c chosen A months ini tial orientation
slcu1d enable them to start functioning in the field though reshyfresher CO rSeS tvould be necesslt1ry in due course In Port-of-Spain married mer~ a1C women may be employed on a part-time basis
I Hanagement Study
428 A nanagement study of the Family Planning Program should include a sctu iny of the top m~nagement Atructure (Population Council - Office of the Fanil) PLanning Program - Principal Medical Officer for MCH and Family Planni Ig fetices) the field structure for the delivery of family planning servics (Re0ional Director - District Health Services) including the utilizlti(n if medical and paramedical personnel for adding the function of del ve y )f family planning services and the control and communication proCed1reF Lfnking the top management with the field structure
429 The management consultants may study the functioning of the Popul tio I Council and advise whether it adequately serves the purpose of givini po Licy direction to the Program and if not what changes in its compo itt m and operating procedures may be introduced without altering its bsic craracter as an advisory agency The consultants may suggest an alern at ve form of organizati)n and utilization of personnel which in thir p nion may be better adapted to the needs of the Program
430 Irrespective of whether the Population Council is maintained or it is replaced by an agency of a different character a formation like the Offic of be Family Planning Program would be necessary for the administrashytion i)f 1 he program a task for which i 1 appears inadequately equipped at preselt Its obvious requirements are in the areas of program monitoring and el7alnation program supervision communication and training The manag ememiddotlt consultants may study the structure and procedures of this form~ tio Gnd make suggestions with regard to the augmentation of professional and ~ upp)rt lng staffgt and modification of operating procedures
431 The linkage of the Office of the Family Planning Program with the Miniutry of Health (Central Office) and the District Health Services should be sudied In view of the policy of the Government to integrate MCH and faI11iLy rlallning services it should be examined whether the Principal Medi al Officer for Communi ty Heal th Services (MCH and Family Planning) should be agtpoj nt~d as the Chief of the Office of the Family Planning Program and an adTlilistrative officer of a suitable level inducted in that Office to assist him TIle implication of this suggestion is that the head of the Family PlanJling Program would control the District Health Services
- 17 shy
432 rf 1e management consultants should examine the delegation of adminshyistratiie Bld financial powers of the Ministry of Health to different levels of Progam aclrlirdstration viz bull PMO Program Office Regional Director and County ~djca~ Officers
l33 he system of 01 af Togram information from the clinlcs to the Pr()~ra1 O~fice and tOile processing and use of information in the latter office iholld )e studied
434 he working procedures at the integrated McP and family planning clinics shnuLl be studied This would involve a study of each stage which a clien tpcticmt has to go through from the point of entry to the point of exit after receiving advice service or supplies This study shoulci lead to star dartization of procedures and functions and evolution of -lork norms CognatE st tdies of the working procedures at uni-purpose family planning clinics and su~ply SEssions should also be undertaken An essential component of these ~ tad ~es would be to examine Nhich functions currently performed by docshytors lealh visitors nurses and midives respectively hav~ become so roushytinize ttl it they can he relegated (0 the next 10Her level
435 Reated to working procedures is the problem of job description of medcal 8nd parrunedical personnel involved in family planning from the centra i tc the field level This job description needs to be studied wi th a vie VIW8Id txaminiDg the uttlization of skills and allocation of time by the staff lcc(rd~ng to the functional prj ori ties
436 frV management consultants should study the workings of the curren slralgements fOJ family planning counselling under the Post-Partul11 Post-Abortal Education and Referral Program at the Port-of-Spain and San Fenaldo General Hospitals
437 SU1ect to the ItBrcement of the Gove1nment the management conshy8ultal ts ~hOLlld undertake a study of th requirement of field workers (home vinitcru) in tmtlUI of are nnd population cov(ra~e
ANNEX 1
Names of Persons Met
Ii Mr T C Taitt Pem1(H~nt 3~crtarY) Ministry of Health
2 Dr M n Henry Chitd Medical Officer Ministry of Health
Ellubeth Quam a Prindpal Medical Officer (1S)
4 Mr G Z Jaine ~ uJiector Population Council
5 Dr Norma Andrews Medical Officer Population Council
6 Mr Jc~n Coury~ Evaluation Adviser Population Council
7 Mr A Jriseph Principal Statistical Officer Population Council
8 Dr C 0 Colman Country Representative Pan American Health )rg ni~ation
9 Mr ranca Kippel Health Education Specialist Ministry of Iea th
10 (1 bullbullines Principal Nursing Officer Ministry of Health
11 Dr Mx won (formerlyHinistry of Health)
12 M3 late Carops Ex-Chairman of Population Council
--
4i 1_ middotIIlt F-ntCWclOotf_Y v OJ t tl
GOVIIlHMEIgt(I OF TINIOAD AND TOampAGQ - NNISTJY OF HIALftf AIJIE1 2NATIONAL FAMilY PLANNING PROGRAMME
F MIL Y PLANNING CUNIC CASE CARD - NEW CASES - NFPPl
li ~~___ 1 ________
~ ecll-U
-- --------------------- shy~) ~~middot~------------------~~~~~~---CIJ------ middot~ii--middot-middot----middot-middot---middot--------- shy
ltv Writt N_ 01(111________________
a ~4itiJtmiddotl_____ ilIIIltIoI~____~____~-__----- shybull ~4
fie l$ - JO tDql IIfIA- tr-JMimiddot _ iJ 1 Odoor o
14aorielaquol_ _~ 0 lio witIleo-La ~ 01 bull - OJ ( _01 1~ltgt1lh o bull- 0$
AacJcu 0 2 CIIriIWA 0 J Os 0
Yv~MONTH ltnollOf~nfIGHTI
Undu 1100U$ Utgtdn 5SCI Undu 11200 01 ~ 50 - 9949 amp100 - 1199 02UlOO - nn9E~ (
0)~ 10- $99 SiOO -- U9~ lOO -- U99 12400 - 1359)-------_-r----shy ~l)o SIS n600 - Hm1300 -- 019 OJ200 il~9 ~------ 99~ a 1)0 m Os1)00 -- l99 1400 -shy $4100 -- 1S999r--- shy
1500 donl S6000aad O399 - lt499I~- I 0lt
ltII
IJ -IC _~tltlioltgti lS
02 IaampJIIocI OJ 04 laM Os
w Oltwio I_-l(~u IrIaa U
h~~ ~Clubl 01 OJ
IS ~C-n 01 toSIitDI 02
Ji poundI on 01 IriIIIuy M ur 02 IV OJ
WU 10 pltIoII~ llaMtl 411 cIIiId 01 Ol it fIolto ~ do~ _14 rou IIlgtJo 1Ia1 ___~_ shy
40
It _ I 00 ~bull FPIiIJ 1
OJ 02 OJ 06
)0 III- iy wOWcf ~1
aMIIl Os
11 T 1gtlt ( h _______ 4)~
06
04 (MIbullbull middot bIrlI ~___~__~_ (-fIJI ~- -~-- (1HJ 49middot SJ
U 10k 01( 1__ raquo$-4
iU1) DOl F ToWotfOlnC DOl 001 or Do [IP 006 001 OIIgtu___Spltclty DOll Nltmo 010
U1Mo I orcpmiddot laquo55middot16
1lD 001 Foam Toblelf_ICim DOl Condom DOl CoomS~ 004 oe Oos WlttuJn 1J OIkr DSpody) 101~ ~Iu 006 Rhylhm 001 DOG OJO
no wI~lmm 4 cd
(I 0) 1110 01 Condor 03 (lorn bull l S~muoidIl 04 Faa TabioolfIIltr- Os RhyUlm 01 lnJrl tible O Advico 090 06
la slt 1)0 19 loti ~rltnlt) ([)sl or 1llOn) ____ --__ bullbully-J n SV - ~JcdS
v~ Cl NCI 0 30 OJI_O I Wr blJ1h 0 I ~ OJ 1 ~ (fOOd V 01 No 02 laquo 6) Cf4
WIiI 1 172
004 001
j D middotmiddot middot
1 ~
r
~
bull I
bullI I I
r c i
ANNEX 3 Pagemiddot 1 of 5
0 raquo rshy -lt l)J ~ 111 t G) 5 shy (J) ~ -
fT1u
i
MINISTTY OF Ho1TH
NTIONl F~ILY LNNING PR-GRbullbullM-tE
~~5tructions to C11nic ClerKa
How to co~ploto the Daily Rogister
~~ ~~v1sd Daily Rosi8ter replnc~D tho one which is now in use tb$ Monthly PC~ri rOt~ arti tho 01( Ci() Dod PollJ j f m It is a pre-coded form and 1411 cl~1p Jd tl a1I6iniul-mIHvn Oel Clinic nctivi~y
110 )rm rollt biJ coupJot)d lrl cupLtcoto using a o(roon shoot Tho top aheot or oriinai ~ust bl) 6(Ult to tho CQgt1tral O[[lCO and tho carbon copy retained in the Gliaic rilo dll the for6a that ar uD~d betwoen the 1st 4nd the 15th of the oIIollth aut bo subClittud tocho office 35 Lnc blttch Those oomp1cted betwoon tho 16th _lid tqemc of tho month must bo ~cnt in a secJnll batch
P lOvLior hns boon Illllde for 25 clients on cZlch forlll new forlll must b IIlied f r poundh 50[810n2 whothur or not ono or lIIore session are hoIdiit the clinic on he sarne day
I th ro alO more htl 25 clionta 1n attondnnco at tho session the additi shyOhAl m~bOl of clionts 10 clients nu~ber 26 27 etc sh0u1l be ontered on the next Imiddotrlll ~i ttout a1tpoundring the numbtlrs in the cvlumn hond Series
51 ppOfil th~ number of aUcnts lQr that session ws 5 this would mean thllt two rJlS ~ lst be 6ubllIitt~dl the first filled uF 1 tltgt 25 And the laquoIncond 1 to 10 Th~ cal bon ofies should bo st~plod togother at thu t0P l~rt h4nd corner of the torm ard ktpt in the Clinic filo lou IIlU6t stapl~ the originftls in the 8~~ monnshyer for lIub~ssion to the ofticl
ie h~ ll idontiflctior- (cc 1 - )
0 lot Ji 9 anythin~ hGro poundhia is int(mdClc for tha computer code
2 ~~pound~ - Print clOflrly tho name of your Clinic
C1Lic Huml or - (cc 4 - 8) Evar1 Clinic Numbor has 5 digits Virite each dig t il a t$purate box
It Pai~_thllsectgdllion (00 lt) -1 1) - Dl monll 10M
lw) bolte IlrO proY140d fetr olAoh pr 01 thQ dISh Enter tho dA) ldns a R
d16ih
emiddot5middot (0 11 I for 115t ( 0 21 for 5th etc Treat month the am pay
e ~ 10 ~ I for I-hrch 0 [2] for September Tho y~nr must be (into ad
I Z I ~ I I 71 q etc
Take as in IixulIple tho dOlte 3rd tllrch 1973 7~ie must bo written
[0131 LSLDI[7l3JDny Month Ye~r
5middot 1~J $~~ - Irom ~-------- To --------shytntol hOI II the time the Clinic 111118 in SW5sion emiddot8middot
(i) 11011 500 lm To 1200 non
(11) Frclt 100 pm To 400 pm
(iii ) IX-OG OO pllI To 6~00 pm
f
2
ADEJ ) Paae ) of S
6 Eov
_ 1hA 1gtIpoundC iIIUlt be nu~o7Ifd tler1ally 1 throurh n lU tbey Are Wled In ~1l8ellJ IInel 1301 tlU 1 Orcl 1 Wled tor a o5038ioll - -I 2 tonY tho _boul~ b I1WJbtl 1 and 2
hlrlll are 25 linos OIl the fOnl Ilnd thoae muet be UBtleS for 25 clients 9 one ior bullbull 01 I ini
ot ~h lc II ol1cM lOlivpound til e linic before soeinc DurOI or doc tor ilnc ii hox rristrltltion nUlJbet had alrearll been recorded on the Dai 1y Roiuter then n line ~hollld be drawn through that entry an1 the eliort nust not 06 includttd in tho totals tor that 0eDion
1lw Ileifitration Num)~r of cueh client must be IiIritten IS n 5-dlrlt oode ClhnC IH11IlElr 315 1IIU8 tborotore be enterod 18J010117]5]
~ Clt ZOt
Coda 1 Codo
10 ~tl c 2t j co 21)
~w elSe - Coda 1 0) d CltaEl - Code 2 Revislt Code 3
Only pound1 01 theBe coiles may be usod
11 prol-O~ ~Eil~1 (cc 22)
If ma climt was L drop-out IIho haoS returned now to the Clinio tor tho first no linmiddot bullwin lt1ro1eo o t he or she should be given CCe 1 It this do 5 II It nprlly leu this colWlln blank
u Hothod middothisllill loe 23)
NOh til t otly ~ Cod 16 tp he ontered in 2lpound of the columna oven thOUGh 10 co11lllJlB 10 provided on the torm The Codes llrol-
Oral Contraceptive Code 0 1 U D Code 1 Condom plUD Codo Z Condor (only) Code 3 Foum tAblets cream Code it DitphrClGJII Code 5 Rhythm Cde 6 Injectible Code 7 Advice Code 8 Other Code 9
It for middotDo-le 1 client rlllll ji yen cclldorls ord foam or creall Iou Qust entor Coole i (condom plulJ) in the appropri~te column This Quat be the only lIotmiddot) tarcie If an in the cnse of a tlnle clinic I the client is Bup)lieu lith COIlOrW only you rmot entEr CorlQ 3 (cpndolll) Do not use a ticII ~ tho (odo Nwber
It is CUi tomary fur 11 cliont 110 is beine put on the oral contraceptive for the first tiT1o and even on other occasionn be issued condoms and 11 crelle or foam a Ilell rI3 a pgtcket of pilla In such Cllses when the piDQ Ilre Ilctually iouou you tlust record Orll (Co~e 0) 08 tho onll metbod ilo othor ntry sll0uld ho nnrlo
Uovever n SJC~ canas vucru condoms and fOHa ~rc eiven but no pilJa (even thoJRh _t _n the intention to issue pills nt the noxt vioit) than the Mothol Th5 ifli t ohoulcl be recorded uo Condor Plus (Code 2)
13 Seen Bybullbullbullbullbull
~rot S-1 SO l
Doctor (Dr) - Code 1 j Nurse (Nul ) - Code 2
Clark (Olk-) - Code If tho Clhnt is vcen hy both tho llootor tlnd the Nurse enter Code 1 t Doctor It 6~61l by the Nurso only arite Code 2 Cod bullbull Cerk is l)llnt for FA Cllnica Clerks in tho Government Cli1t hiwo Llttoll istructed not to i56uo supplios on their own volition
14 fl221~
lhio S~tiCl of -Ie fvrtl t~ke 16 (llrci coluMna (cc 25-+0) nnd 10 tho only part at th iOIQ in llich iore thAn one cod is Zlccoptl1blo Tho purpoco of the )ecton is to 0 able to arrive nt the Cjunntity of 6tock dilltlitJutshyed YOI IIlUdt writo in the CllllOjH-iata colulna the nUllbJr of Il1ch 4rtic1o i~JSu~d ~lo e ha I Oral Contrcilpti vea are aub-di vi dod into types ae_ 3 PIllCKC 9 0 Elynnn LlUot be entered Codo in card column 25
If tor eXllrplc t l cliunt is iosued wi th packots of Zucynon nnd aJ(1 ~ivn 1 conuotll (8inoloo) you ouot enter in oard column 25 and 11 It
cnrd col~8 )2 and J (io 1 in card colucn 2 nnd 2 1n card coluun 33) Nota C)lldoIlU ale to b(t ruoordod individually not os packots of throo) Should n ne LlondoClo be isoued thil3 is to be rc-Qed as 09
If It clint 6 t~ot isoued Blly lIupplies thon you must writo Codo 1 in CQllAlilD 41
It Q eli nt isite the clinic to check on her LUD or her Diaphra~t IUId ro DI W 6 ppl ills nre ispounducd then Code 1 1s wri t ten in column 40
In the FA clinios here a variety ot orll contraceptiveo in orer~l tho elerll wilmiddot~ bJ provided with a specill code shoot The idontifyin coo will b wiittn in Column 29 nnd the nUlber of packets iosued in colwm )0
lralaer-In Code 1 lrllllsie r~ut Coda 2 leIllPQrArr Trnnsfer-In Codo gt
In the cao of n 2ratl8fcr-In I you lUot n160 cOrlpleto coluons 42-51
In the cllU J of A ~~emporary TranGfor-1n (an individual who i8 only v1citing fur clinic tor some epecial trcatcont hna who will bo rdnlnin
~middot(II~~~fO~l~SIl~I3~nn~~~h~rO~nh~1~~190~~nll 2-46 and ler rei IItrntion numbu in colullnll41-51
It the oli( nt i iNt a CrllnoforwIu - Out or loClporu1 tMn loave oolumn 1 blank
16 lr4nst(gtr-tl2~~morrry TilJnder-In (co 42-51) Forl1ltl CUn E1~ (cc 112-46)
hen you rei iatlr L irllsfcrln or Il TJlporary Trnnsfer-In you IIIUBt write I ere the five-digit clinio nucbor of the Clinic iraQ which tho ltlient Me (uIlO
2mer ]letr ~2n ~ (cc 47-51)
frlta fllao Clo r-~itrlltion Nuc~Er ot the client in the Former Clinic (i c bullbull th 1 Sis rnmiddotion ~UlIlh()r which the client carrics 1n the tormor clinio) bull
It tho Forrltl Ho( ist rntion Number iIJ not readily wnilnble you tluct oocpluto thtl epcciol [orlll Transfer-In Not Identifiod Dy Forrlcr RCGi(trn~ t10n Nwlbvr Or ~ flt)rCl is to be cOlplctcd for och cnso nnd th forlJO Ilubmi tted to thu )opllntion Prorrnnme Of fice tOGether with tho Dily Ro~iBtors lhwev~r should the clork leuTI of tho clint B FormlI Uocintra tion lUlllb r )0[(10 Cubmi ttinft the D1ily IOCI otro t hen the nUQbcr shoulo bo -ri ton in colucns 47-51 lna the special foro should lJo deotroyotl
l7 bullbullbullbullbull
r lt bull bull
ADXI ) Pap S ot S
11 UD LV~ (cc 525)
It tb( cliont io ~ivQn An IUD tor the firot tl~o then you should Sri to Codo 1 Inuort ill colurJI 52
It tho olimiddotsnt ia rvinGgtrtltld i th An I UD bullbull tben wse Coda 2 RelnDltlrt shyin (01Uil11 52
It the clLmt is ~tte~~dint chnic beruse her IUD CflClQ out by Haol (cxpll Iion i ~hcn fir te todo ~- UIlllrli1 53~
If c-ltr IU fj IIIS reov in -ne cllnic by tho doctor or nurso t~on vlritI Codec in column 5
II the eli nt otends eiLlie tld explin[l th(lt she rccovcd the IUD tlllleel nen write Coda H in Colwlm 53
It the IUD jr still within the uterus nd the WOIraquoI1 1 11rc6llJlnt thon lIrite 1gt40 4 in Column 53
lZ np h5t (ce 54) It 0 Pull 5mor ie t~ken durin thi visit tben Codo 1 ehould be ampDtere4 in ColWlln 54 Should he c110nt lltt rQ(uircd to rttturn to clin1c for a rogtol1t Pnl) t06t then CoLe 2 llhould bo middotwrittcn in column 54
It no Pllp Scou io taken tde visit Itove colUQn 54 blank
Iraferti1lli (CQ 55)
Ii the e liett io nl1 infortili tr eaoe use Cor1o Ill in colUQn 55
If tbia 1000 not tlpl lonve column 55 blonk
20 Totaltll
CO~1ploete the [)ldegO 1gty puti YI tne totals betweon the double lines nt tu b()ttctl Carrj colUlllnc 20 21 nd gt4 Must hlve tho Bnoe JllIIber and thiG Would coreslonc to the numocr ir attencbnco
Writ$ th to1ul nUlllior of Drop-Outs returned (c022)
Urito 41eo tb totnls fOJ each card column 0 to 9 under tho h(adinu Method thiB Vioit Show tho tote L fgtr OlCl type of contraceptive issued (cc 25-40)
1)0 Dot wrLte 1111 totll lUl(Ier Card Columns 15-19 29 41-51
21 COPmllh bull ~lt h~t~ Monthly ROilort
OQ thG DaLl oCator forlll thnt ccrrOspOldB to tho 1(8t 1$06610n lt 0
oth yo Olllt (vwlgtleto the items nt the botto of the [orampl This is tour ontll~1 n(olt nnd includcD tho totll lumber of sesions Ilntl tho total Iluolcr ( r crop-outs durinr the Qonth
An tiUlsilt n drir which n doctor liB in nttcndnncc is a doctor sOfll~1on and shoulc 00 re(liGtcnd in coltns 56-57 All other sessions 1116 conlliid~recl supply stllciona and thtlY 1110 rocordod in columns 58-59
the total Ilum)nl Jf drop-outo ld the drop-outs by method durinc the onth nre 10 bu oltorou in the inrlicllted boxes
72 Chad Your ~
Milke I ura th t all thE fijul4gtu rre c101r -tNever writo our nutlUQrS 50 InrjEl that they oxtend out of tho
ap~rotr1ato ~ox
Cheek to BoJa tht 1111 numuors 1110 in tho correct boxes -- CJslHloially when Writi1 the totlB
Mllxe Cirtc O thmiddott t1e infoT1I1ntion i6 clear on the corbon COllY before sep rmiddotinr the sheets
Jitn the Fomiddotl lien tly sien YOUl nr me 1t the bot tOil right hnnd corner btl forc subol ttinG it Keep tle CL rb n copy for your rocordn
i
-l ________~~---------~
I _1
Adminiatr-atlve SKVieu
P inba ~~~l1cal lrlnbin~~eltltcal -1 te~ra t~~rvicc (lnatittloaa)
--1- - shy -1------------_-L_ l-r-aJiil- shy _-L_tet1lal d
PlIinm1tJ8 atdUon DetalMid H8Il1tb ~ ________bull Care
-----~ Office of i
the FlIily _IPlill3 roarshy
1- - - -------RegiatUll urnr
ltIi 1 Drelttor Rcgicaat Director Souta Tabqo tacallortb ~ counu gt____ ~ (4 ouottet)
Off1ce of the Res10nal Diractoc L
r----- _L_ -- shy i I bull IREgional Ipitl I
District IIttaltb I bull Othn RelOl ond Hcpital CenteIntt itlt j In 1__ _shy-~- ---- -_j
J r Ii~lth
C~nlef
L
I Ihnlth lie I th Offlcu (1ft lc~
Coullty 1I0p1ta1
Henlth tentet
I

TRPnnAD AND TOBArO
nEvT Fcl OF THS NATIOAL
i AmLY PLAiNING PROGRAJ1
Page No
i
I In roducion
II Or~ani7ation of the National Family Planning Program bullbullbullbullbull
III Present Status of thE Program bullbullbull 4
IV RE comlerdations 8
A oIulation Co~~cil bullbullbullbull 8
B A ~tatutory COUT1cil II II 9
C Office of the Fad 1y Plannin~ Program bullbullbullbull 11
r Deerttlal1zati ~ ~cjCImiddoter=J ~ ~I ( 12iii
Ircegration or Fltj~Ly llannirg with Maternal and Child Health Setvices bullbullbullbullbullbullbullbullbullbullbullbullbullbull 12
F Voiuntary Organi zations bullbullbullbullbullbullbullbullbullbullbullbullbullbullbullbullbullbullbullbull 14
1 Program Information bullbullbullbullbullbullbullbullbullbullbullbullbullbullbull 14
~i bull Field Workers bullbullbullbullbullbullbullbullbullbullbullbullbullbullbullbull 15
1 Mauagement Study yen bull bull bullbullbull bullbullbullbullbull 16
ANNE~ES
1 - Names of Persons Mat 2 - Clinic Case Card for Fimily Planning 3 - Daily Register
Chari Orgmization of the National Family Planning Board
This report is based Oll the findings of Mr RN Madhok who visited Trinidad and Tobago from April 9-23 as consultant to the Population and Nutrition Projects Department of the World Bank Mr RlT Madhok was formerly Additional Secretary Ministry of Health and Faroily PlaJming Government of India
1) rle Youc fUfCt1 oning in an atmosphere of Lncertairbully n(It-oL2 in the National Family Planning
amp11 t~ms c frence cf the Council should be
(ii) The PJPl1~atcYl CcmncU should be strengthened by including in it (a) the Permanent Secretary Ministry of Health (b) the Principal He(lical Officer in charge of MCH and family plannlng services () 8 representatlve of the Ministry of -inance (0) social scientst and (e) a representative dtich of the aSRociatioi1S of the medical nursing and teaching professions and cqantzations for womens welfare
(Hi [he Offh( ci h F Planning Program (Program Office) hould be strenghened by augmentation of staff at the professional as vel1 as supportive levels after a work study Ir ramptLicular a demographer a media expert and a trainingsdviseT should be inducted into the agency
(a) set anntncGgpts for the enrollment of acceptors at each cliniccenter and monitor progress in relation to these tarets
(b) establish schedules of periodic inspections of clinics
(c) cvnlvl 11 hlufltfmiddotr lgt1~n for the training of personnel and
(d) wor (ltH U 8t(nte~) for Tued1a communication in the light of public awareness and knowledge and the reach and cost-effe~tiveness of different media
v) The Ministry of Heath should invite suggestions from the Director of the Program and the Regional Directors with regard to the deshycentralization of administrative and financial powers currently ves ted in the 11ni8 try and work out a schedule of powers to be exercise tdltclcr )ve of Program adl11 nis tration
F~eld Workers
(vi) A cadre of field workers should be created to promote the accepshytance of family planning in the community As an experiment one such workar may be assign~d to a unit of 10000 population
(vi t) 1ne orgai c Y1 anlti j~lrcgemeu of the Program should be reviewed cmjoLntlyamly pcanning expet and management consultants
r L the fr]lcwing topics
a) thc 1lt0 V 71rmiddotlCi f Cn1t1t structure comprising the ~inis ill Hnal th ~he Ppulation Council and the Prc~r~1 Office ~te feRsibility of alternative models of inatit~~iacnt ~
(b) the s taft re(luirements as well as operating procedures of the Program Office
(c) the ltitin n t[iv and financial powers exercisable by Program uthori ties at different levels in relation to dgtE le31H of lesponsibili ty
(ci) trc JlU l1 of coordination and supervision of
(e) the staffing and working procedures of integrated MCH and family ptanling clinics including family planning counselling 8eVmiddot Ck ~UITli s Rilet recording of data As a part of the study ~ Ulti~cti(ns pe~iolmed by each category of staff - shyme6ic~1 rn ijed lerical -- should be examined to idemi whimiddot rune dons can appropriately be relegated to che next tower level so as to optimize the use of available ma1pow~r
(f) the system of flow of program information from the field and its processing and utilization in the Program Office
(g) he ost-ParttmPo13-Abortal Education and Referral Program and
(h) the requirement of field workers for conununity education creation oE ltiemand for family planning services and conshytinuous c0ntGci with acceptors (The type of functionary needed content and duration of training and the norms of work should be suggested)
I INTRODUCTtflN
101 0-1 behalf of t~ H~1k ~middotmiddotr R N Madhok (Consultant) visited Trini12d ad Toblg0~ middotl iL bullbull ~)3 0 review the administration and mal1agme)t )f thlt hsd j 11]) PVnning Program During his stay in Trinj dad 1- MadhJk ( iilh eprefEntatives of the Ministry of Health and the Topu ation C01Jii1 fuJI li5e appears in Annex 1)
102 ~pecifgtUy ~~C iVlsdhokcevievled the following aspects of the progam
a he future role of the Population Council -- whether it should )euro an advisory or all (~ecutive body its administration staffing and statutcry pmrer under a changed set up and the consequent changes required in theliinistry of Health for the implementation of the prc)gram
~ J the extent of (l~i-5ting (Jpcfntralization of administration of health and frunily planning services and its efficacy
c the desirabiLty of integrating family planning with maternal and child hcaLh services in the light of experience of inteshygrated i~lirJ(
d the efficie~ Cf~ll edsirg system of the flow of program information ac ~Hl red charges and
specific aspects of manager-lent and manpower utilization on which the management finn should concentrate during its study
103 The following report contains broad suggestions on changes rE qui ed in the existtYg structUrEgt
II ORGamp~IZATION OF THE NATIONAL F~~LY PLANNING PROGRAM
201 The administration of the National Family Planning Program is the rl~sp(jnsibility of the Ministry of Health In 1967 when family planning was adopted as an official policy the Health Minister at that time proposed the stallishment of a Population Council to advise the Minister on the organizashy1ion of a natiorlal prorrun 1i(h lIIotld coordinate all family planning effort n tle country Tlle Cabtn2t c~ciCled that
A Population Council of Trinidad and Tobago should be instituted for the purpose of giving overall direction to the Family Planning Program in Trinidad and Tobago with a view among other things to coordinating all fanily activi ties in the country II
- 2 shy
202 In pursuance of t l= foregoiny decision the following terms of refer nce were framed for the Po1)ulation Council
10 i~vll ditcoction to a Family Planning Program fo Y ltdd cHl T0bagn d th Ii view among other things to eo ~ ~c n lfllonrdnr activities in the
203 A PTOlllH~ f(cibor nf ttl rredical profession was appointed as Chailman llei the lill~1L y h2 jiamily Progran Ministry of Health as the Secrltar r (r th C~-ur~ ihe membership of the council comprised officials of tle t-instry of He3ltii and other departments representatives of the volultary agencies operating family planning services and leaders of opinion the present Chairman of the Council is an eminent gynecologist in privmiddotte practice and a former Minister of Health the members are as foIl 08
1- Chief Medicnl Officer MOR -l Spcclliflt ~middotjJ3C Officei- General Hospital
3 A rEpr~senative of the Ministry of Planning and Developneut
4 A represehtacive of the Central Statistical Office 5 Public Tidaions Officer Prime Ministers Office 6 ~ PrilLj~d t1lt dq Officer NOH 1 ~e( CL bull ~clmiddot ~~t)pulati on Program H Chid ~ea~h Educatoi ~lOH
9 A repres~rltatiVE of the Catholic Marriaie Advisory Council
10 amp 11 Re~)resentatives of che Family Planning Association 12 6 13 M~mbers or the Publi~
14 Diector Family Planning Program MOH - Secretary
Olj The Population CQtJrdJ hal three roles (a) policymaking ll) I rogralil formulation and evaitllt1()l and (c) providing general direction fllr program implementation Its composition is designed to ensure (a) intershydapamiddottmental coordination withill the (overnment (b) coordination between the ( Ole-nment program and the activi ties of voluntary agencies and (c) rapport vith pblic opinion
05 The Population Council is assisted in the task of program formushyIation by a numbe of committees ~thich are so constituted as to draw upon Ihe ex lertse avalIahI wi tlin the Government as well as outside Pre-eminent arnorg heseuro commictees s lhE lati()nal tH Program fnLMulation committee ihi(h technically speakirg is not a committee of the Council but a commitshytee of the MOH It inter-meshes with the Council since it is the policy of the Government to integrate family planning services with MCH services delivered through the network or health centersoffices of the Ministry of Health This committee is headed by the Principal Medical Officer of the MOH in dnrge oE Integrateci 2~edicil Care now restyled as Community Services
- 3 shy
which COlT bull Se 11CH anii IIgt sxvl(s I1H~ other committees are Community Educaior and Publidty Cvrm] ttec Research and Evaluation Committee Family
~du aton Comrnirii ~~e(i] CCimittee and inance Committee
OS i~ n1eptUd~ i p Ni ~runi t 1 an advisory body and as such itus 10 execl1lt)ltjmiddot n p-actice the Office of the Family Planning Prog) am e tabisLecl wirgtmiddotcn tilt2 middotlnitry of Health functions not only as the ecr ~tc dat of lIC )hiCJl but also as the instrument for carrying out lis lirEctvls Furtiie ch GOtdcCU has concerned itself nomiddott merely with broal i~ SUIS f10Hc out also vL detailed implementation The majority of t le r emmiddoters of rhe Council are in favor of Umi ting the Councils role to tile givlng of broad direction to the Program
20i The Office of thl~ Fitli1y Planning PrO~rall1 is comprised as follows
Dlrcct0r (Incant) Medilal OfHceuror (Famtly Planning) Nm-~If Offieer St~tistical afficer Health Educator 2 lield Workers (for follow up)
(OIlE positor vacant)
8CCiHWlcnt 2 clexks 2 typists 1 driver 2 proj ctionis 15 and 1 messenger
T- ~ g af f of the Office of the Famly Planning Program is under the discipline of thttinistry of Health since the Population Council is nei ther a departshymfntal unit nor a separate legal entity with its own fund
2 OB The places of )nrm1 atton Council and the Office of the Family p ~anr ins Program wi thi n the Minis try of Health as conceived originally by tile Government may be seen in the abbreviated version of the chart appearing hI different official documents and reproduced at the end of the report
~ 09 In April i973 at the time of the consultants visit there was In aCIDc)sphere of uncertainty about the administration of the family planning l)rogram as a result of changes in some of the top positions As a result of t c~binet reshuffle the portfolio of Health had changed hands The Permanent euroctet lry who is the princ~al ad~liser to the Minister was new as lras the r-i c al Yedic1l Officer h charge of Commurity Health Services (Mel[ and Pam ly Pl1nnhg) The Dtnct0 of family Planning who was managing the Office of middothe Family Planning Program and also serving as the Secretary of the PoshypUlition Council had reCiTed in March 1973 and a successor had not yet been named Meanwhile the Medical Officer for Family Planning (a part-time employee) was carrying out the functions of the Director in addition to her OWT Wi thin the Population Council the advisory agency for policy-making
and ccord~n8tionJ there was a groHinr feeling among the members that the ouncl1 510t1d shed thE respOJ1sibili ty for implementing the program a funeL on j ch nad heuroe added on to its advisory role with the passage of time
iO the 1 ~lp~1 the lines 0 responsibili cy were not clcay (e ned and Li1 refioal system was not fully functioning The post of Re ior 3 Director crth VIas vacant The policy seems to be to strengthen the 1St tu ion of Pt()1ic Flealth Office as an 3ency for the supervi-middot sion)pound ne district sflVices (health centers health offices and school servi ces ~l thin the ccnmty
II I PRES EN STATUS OF THE PROGRAM
301 ~he adl1linistrt~ivE changes narrated in para 209 have come about at fl tin e IJhen the P1ogram has entered a phase of declining performance as is 11 Jpal en from th colloHing figures taken from a report submitted to the Populaton Council
YrUL 10C7 ~j8 1969 1970 1971 1972
--- -- ------------~~ --~ - shy----shy
Ne Acceptors 3696 2731 16207 9997 9898
(End of October)
7560
Slur~e Family PlAnnto Program Report (no date)----AsII1Ulilg that th6 ttlrollmant of new acceptors during November-December 1972 prclrd at the 8ame rate as during the ten~onth period January-October
- 9i2the total enrollmslt in 1972 would be lebullbull than 8500
3(12 lhe total number of leW i-iCCeptors for 1971 shown in the foregoing tal11e 1s at variance with the following data from the 1971 Allnual Report
- 5 shy
~ev C~~ Contraceptive Method and Agency
nm Other Advice Total New Cases
Aeny
GovrrmenC ProEllil ___~zZ(lt1____ 97____2Lbull499___~528~___4i_750~_
Farr Uy Planning Association 2814 315 607 76
Catholic MarriaAdis1ry COLnc_H____
ge
74 88 162
otal 31[10 692 8724
_--__------------------shySOlrce Natio
1973 nal p
Fam29
ily Planning Program 1971 Annual Report April
NevmiddotrneJl~ss) the declining trend in annual performance after 1969 is manifest ana conpaes unsatisfactodly to the following targets set for the Program
Targets for Contraceptive Users - 1968-72
New Accep tots Old Cases Total
1968 20noO 20 000 lO noo
1969 20000 40 000 60000
1970 20000 60000 80000
1971 20000 80000 100000
-----__shySource National Family Planning Program
p i9
------------------------------------
- F shy
3JJ3 Ttl flient recrvitTrent has fallen off since 1969 in spite of a signif Icar t xpansinn ir the number of Government health facilities providing family paarin~ services FrCli1 7Hr to year Starting from scratch the number oE GovE(nment health irlstitl1tions delivering family planning services in isollL(Od ~ily pltJfAill~I ~J in c)lchiratinn ~7ith MCa services has lWW risEn t 4 lhis ie --tdt)p to t cii1ics organized by the Family Plannin Asce1ation bull U2 by tile Catholic Marriage Advisory Council which offers the ~h)lthm meti1middot1 nT
304 1i ciecli ne d~ d re11~m2nt of new acceptors coincidentally w-Lth th~ eXlsioH uf s-crLce facilities needs to be studied to identify the factors responsible for it eg the quality of services offered the strategy of commmic at~on and motivation and management and supervision One obvious gap is he abgtence of an agercy for promotion and extension of demand for family lal 111 If services -gt tLe field reliance being placed mainly on clinic counseUn H1d generaUzmiddotd mass media publicity The need for a field promoshytional agelcy is underscored by the dropout rate In 11 draft paper prepared by the Hed_cal Offic(1r for FIrnilv Planning it is stated that by the end of 1972 t ile Heuroe approxiclt ji rHJC cun~ent users of contraceptive methods and 33 per ert dropouts
305 rht~ program is cot merely clinic-centered but also female-oriented Recent Iy mellsages aimed at m11es and stressing joint male-female responsibishyIi ty l gtT j ecillc CImt-J 1 i~gtVt~ b~~in )7cn 1n0 the cOTul1mication activity sUf1 tv) c nts Em he 2iucaccw i milc8 and che distribution of condoms to them illVC he ~n or n~d iD r GJvefl1nenC s(~ctor The Family Planning Association has a130E~k11 the irti U3 1V~ to reis ter males ln industrial employment Tllese are steps in the ri)n dtrect1ongt but the size of the problem indicates the n~ ed OI a concerted effort en a much large r scale
306 Tre Program relies largely on the use of oral contraceptives as shown in the following table
Oral Other Advice Contraceptlves IUDs Methods Only Totals ( 100)
19)9 76 20 16207 ( 100)
1970 316 63 9997 ( 100)
1971 50n 4n 365 79 8724 (100)
Family Planning Association unpublished report
----
- 7 -
Althougr amJnp the neH acceptors in 1971 the users of oral pills were only 509 ~mon~ the old cases the figure was 119 The percentage of IUD users has remiined stagnant at an insignificant level this may be partly due to consume prefErence and pctrtly outng to lack of trained staff to undertake IlTD i1srti l7U There h hOHever a visible shi ft towards the uSe of othe~ ilettods (npchani81 and chemical) attributable to a scare about the side efects nf oral connaceptives Among these conventional methods the condom s 11 os popular
307 J t )resent fami ly planning services have been extended to 48 out of 106 hellth centersoffices run by the Government and the objective is to C)Vel t1e remaining health centersoffices within a short span of time so that adice and facilities for the practice of family planning are conshyvenient Ly wa nable to the people in all parts of the country By ann large sepanit e fITti ly planning eli nics are held on specified days as an addition to norrral lealth work Besides doctor sessions at the clinics supply sessions are rur by health visitors and nllrses assisted by clerks The nurses are authorjzed tc issue oral contraceptives for a period not exceeding three months ani the acceptor is required to attend a doctor session for advice during thi jnterval In 1971 the numbers of full-timepart-time staff in Gov~rtmnf centers renderinp family planning services were
Full-time Part-time
1elical Officers 14 8
NUseMidwives 35 19
Cl~rks 3 17
Now tile low~rnment -gtbjective is to integrate family planning services into MOl services and use the same staff being used for the delivery of both types of erlices at multi-purpose sessions However so far only 1A centers have interated family planntng with Men or gpoundmeral hpalth care sessions
3011 The Family Planning Association has eight unf-purpose centers where famil) pLmring services are available ftve days a week The Association employs tilrEe full-time and ttJO part-time doctors a complement of 14 nurSeS (who llave been trained to do pelvic examinations) and 11 other clinic staff membels The Association also has a number of voluntary workers in the clinics The CithoUt Marriage Advisory Council has three clinics but their contri shybution in terms of enrallment of acceptors is not signiflcant
3)9 A Post-PartumPost-ALortal Program was started in 1969 It is state I tlat about 14 percent of the patients reached attend a family planning clini~ 1iTj thin six weeks of the interview in the wards IhiR is qui te a low figur In 1970 when a system of home visits was tried under the Family Planning Aide Project in 7 clinics the rate of acceptance doubled in three clinils rose by 50 percent in two clinics and increased by 24 percent in one clini (No change was noticeable in the seventh clinic) No decision has been Inad~ tmiddot) continue extend or modify this Project
A Po~ulaton Council ~-----------
401 he fu~ura ro~ Lh~ ~~~01ati0n Council has to be considered in theli1 A the tasK t~ lL ahead of the ~ational Family Planning Program At pesent tile officil~r(QSrJ1Tl is prirnarily concentrating on two objectives (a) tIlE excpound1sinrt of fmd plannin~ services to tie remaining 58 health centen cLJs as rapi(ily as possible and (b) the integration of family planniT g VI tr MCH services Thus thG administration of family planning serviCHJ will be merged into and become part of the Community Health Services Since t is ()rganizationally undesirable to disturb unity of command a separa1e elteecutive agency for the administration of family planning services is preempted within the existing policy framework An executive role for thp Pcnulc tinn Council is there fore ruled out on this consideration
402 If the Population Council is to function as an advisory body at the p()Lic~ aId progra1l pLilnni-l level snd not to concern itself with the minutile If program execution there wonld be no advantage in giving it a statutory stltuS But if it were the policy of the Government to set up a verticll )middotro~ram for family planning ii th a field organization separate and distir~tOroll the HeaHh administration it would be quite appropriate to establish an autonOiTiOUS statut()y a~fgtny ntside the departmental setup of the MinisiY of Health d~b a budi~t md staff of its own commensurate vith the rE spo lsi hi Ii ty to be rEs j Freed from the usual departmental conshystrailts ~n the matters Cif sp(ndlng a1d hiring and firing of personnel such an aglncy c(uld move faster than a heavy-footed departmental formation wi thin a Mins trl bull Hovever a hody of this eharacter would need to be cas t in a cliffe ent m(ld than the present Population Council The shape that it would take lrould be more like a Board of Management with a full-time Chairman or Execuive Director and with more functional expertise than representational charater But an advisory council with an autonomous status and no responsishybilit f( r lrogrrun eXIGulion iould be a source of friction
403 r~e existence of the Population Council as an organ of policy advici has certain advantages Firstly it is a forum for developing a national poLicy in which officials and non-officials participate Secondly it pr )vi bulles a focus to ti1e official program vhich it otherwise may tend to lose as ~ontraceptive services are merged into the general health services Thirc lymiddot- and this is important -- the Ministry has extra-departmental advice availabL to it~ but the Ministers constitutional responsibility for the condl ct )f the national progl~lt~ le1lains unimpaired
404 ls an advisory Q(dy the Population Council should be more broanshybase( than it is at present For instance it should include representatives of tile organizations of employers and vorkers associations of the medical nursngmct teaching professions and organizations for womens welfare The Counil should also haye a social scientis t on it On the official side the
- 9 -
Permane It Secetary and the P1O (fen and FP) should be brought into the Council he inclusion of the Permenent Secretary would open a channel of communi~aton with the MOR ae the highest policy level next to the Minister and would (ontribute administrative expertise to the deliberations of the Cou1ci1 ~m f icili tali 5 (pleuenrti)D of th~ recommendations of the Council within the -rni and in OUltL depa-cments The inclusions of the PMO (MCH and FP) wOlld el) emphasi ~2 hs responsibi lity toward the family planninR program Some officrs of the HOH (eg Chief Health Educator Principal Nursin~ Office e) may 111 ea~e to be members though they may attend as requirE d nmiddot the agenda before the Council A representative of the Ministry of Fin nee stQuId be inc~uded in the Population Council This would make for a lettr appreciation of the needs of the Program in that Ministry and fadIi ate fj nancial sanct ions
B A~tatutory Council
40S In the foregotng Pgraphs the view has been expressed that within th edsting policy framework an advisory Population Council would be more tli)prcpriate than a COlincil wi th executive functions and powers that an advisory rOUlcil would not gain by having a statutory status and that if a statl1tory body 5s to be set up in lieu of the existing Council it would need tC b structured more Iiice a Board of Management than a council wi th a repre13entttional charact~( n the latter event the statutory council should have fu 1- time Executive Chairman or failing that an Executive Director functj oni1g undel- a Chairman trno can devote considerable time to the business of tlw COlncil
406 T1e Statutory Council should have its own budget with full operashytiona pOlo1ers It should have the authority to appoint its own staff and regulLte their conditions of service If it is constitutionally possible the Couner1 shollld be outside the jurisdiction of the Public Service Commission in pesornel matters
407 As an instrument of Government the Council should be subject to such ~eUfral or specific directives that the Ministry of Health may issue to it frcffi ime to time This should be written into the statute under which the Cmntil is set UD
408 The composition of the Council ould depend on the functions assig1ed to it It is suggested that the Council should not concern itself wl th the delivery of cliric selVices in the field The Ministry of Health may (ont nue to administer rampmily planning services at Government hospitals health cmters and health offices and the voluntary agencies should run thei] OWl ~rogram The following functions may be handled by the Council
- to shy
s rrogram plannin and target-setting
b proram monitoring and evalllation
c wiL of d 1ci(JTIdnCf by inspections
d Qrg8lizatim 0 es and marketing of contraceptive J~1J-s BLl (iV es at subs idi zed rates through es tablished 1 2 d(~ channel
e information mass media communication and audiovisual ublicity in the field
f prorrotion of famil~r plannIng acceptance through face-to-face cotlmunication by poundi eld workers in domiciliary visi ts
g trIining of personnel
II pr )motion of -esearch enJ
i financial support to voluntary agencies providing family planning services
409 n Statutory CCii1cil may corsi5t or an eminent non-official vith a comri tm ~~1t towacds foJlily plailninf nd the fol1owin~ members
I ~ bull Pfrmanent Secretary ltl-tIlH
Chief Hedical Officer HOH
i Principal ~ecHcal Office ~mH
d Pilhlic RellltionB OfJte(middotmiddot Prtm~ Ministere Office
A represen ta ti V~1 of the Ministry of Education
f ~ representative of the Ministry of Finance
g A representa~ive of the FPA
h A representative ot the C1AC
i H social scientist fcum tle University of the ~Jest Indies
j Three non-officials with experience in management and administration and the
k Director of the Family Planning Program - Secretary
- 11 shy
The COUlcil ITIltW constitute cOlClmittees for Finance - Accounts Personnel and Sup lies nd Stores ir~whi ch )nly members may be included Other commitles sc1h as those 01 training info1nation and education and researCl ara ~valuation r1ili also include experts from outside
410 he Off1ce raquo) cc im Panning Program which at present forms part of th ~Hnis try or [i n should be placed under the Council and its staff strelgtl ilcn~ii2 i~ r181 it may cease to depend upon the services of the Mir is t y of H~alth
C Office of the Family Planning Program
4 11ollwther the Offic~ of the Family Planning Program remains a part of the Mirisry of Health or is transferred under a statutory council if one is set uP i needs to be strengthened to meet the requirements of an expAndshying pr )gn m At present the following sys terns need to be ins ti tuted in this Office
a a 3ystem of setting annual targets for the enrollment of acceptors and the projection of service fadli ties in relation to these targets
I Ci ~ystem oE V)glC loHitoring (the monthly statistics flowing from the clini~s c~iiiain unproc(~s5erl for months)
a system of program evaluation eg demographic effect of tte program cost studies
1 an overall design for media communication based on a study of the reach a~d cost effectiveness of different media and the effect of the meflBsge content and
e a m88t~r plan for training which would comprise an assessment of the training needK of the existing staff and future reshycruits and a long-term plan divided into annual programs
412 Th2 Prograll afiie s~lould have the services of a demographer and a meeia expert A training adviser is expected to be provided by the PARO
413 1be Program Office should evolve schedules of field tours to overliee field operatio1s E~1eh health cente heal th office should be visi ted peridicaLy by the Milt~dical fElce- the Nursing Officer and the Health EduCltoI who should guide and assis t the local staff in carrying out the progam Their tour notes should go into separate dossiers for each institushytion and ~ach dossier should have basic demographic data about the area coveled by each institution These dossiers would be a useful record for revilwing l)errOmance The staff of the Program Office should be augmented to Ol)erte this control procedure
- 12 shy
D Decentralization of Powers
414 ~hete is a concentration of administrative and financial powers in the 11in s try of Health I-JllJCi1 results in an accumulation of references in the Miristl) and delays n field operations Specific powers should be delegated ~o (a) the PliO concerned with MCH and family planningmiddot (b) the Directcr o the Program Office (c) the Regional Director and (d) the County Medica1 Oficecs The Ministry should invite suggestions from these officers and wOlk 01t a schedule of delegated powers
415 A tdgh priority in the matter of delegation of powers is to arm the Regiond Directors with sufficient administrative and financial authority to implement with expedition the health and family planning programs of the Ministmiddoty 1 thin the areas in their jurisdictions
E Integration of Family Planning wi th Haternal and Child Health Services
416 At present family planning services are being provided at 48 Goverrnent hospitals health centers and health offices by using the full shytime E taf cf these institutions and employing part-time (sessional) doctors nurse~ anI clerks where necessary At 29 of these institutions separate famil cl~nics are held on specified days in the weck some being doctor sessi(ms mel others supply sessions run hy nurses and clerks At the remaining 18 imtit1tions family planning services are combined with antenatal child healtL cr postnatal services The Family Planning Association runs 8 unishypurpoe f am ly planning centers which provide daily services and contribute a 11 t le less than half the total number of new acceptors per year
417 N assessment has b~en marie of the effect of integrated MOl and famil~ p~ nnning services an the recrl1i tment of acceptors nor were ~ data readily avallable for this purpose It may be observed however that in a situation of shortages of trained personnel for health services utilization of the existing health staff and facilitieR for family planning is inevitable parU cllLrl y in the interior where such shortages are more pronounced This underlines the need of evaluation of the integrated xai and family planning progtam for its impact on the number of acceptors Also a study needs to be made of che utilization of medical and pilramedical manpower so that it leads to bdter ~llocation of duties and optimUJl utilization of personnel
418 ile integration of faMily planning into Mcn services has certain advalltages as well as attendant risks The advantages are
a Lbe association of family planning with the care of mothers and children helps project a benevolent image of family planning as a program of family welfare This creates a
- 13 shy
1imate favorab~e to the acceptance of family planning aa lt p-)si tL1e il-Eare rreasure rather than a negative program cE limiting c~ildren
h t elps erlist ~r2tion tf doctars and nurses who as c -~ass enjo tft~ Y)er)et~ a~d confidf~nce of the communities i712~ Eerve
c ~ieD of contact with women
d luni-purposa clhlics for ~lCH and family planning services are onenient for motn~rs who would have to travel considerable (listances to the clinics
e hete is better utilizat1on of Acarce heAlth manpower
419 he limitatio$ of integrating family planning with MCH servicesI
are the posiOili ties of loss of focus on family planning as a high priori ty prograrr ald the diffusion of pol1sibility for its implementation These could tlow ve r he safegurded agaifls t by adopting the following measures
a 11e job descriptions of doctors and nurses should be rewritten 0 include the family planning function
b hE perf0rt1iai1ce of ctoltors and nurses should be judged as much )y tbeir inteceq t in planning ~vork as in maternal and ~hjld care and this should he lade known to them
c )octors and nurses involved in ~CH services should be given middot)rj entation and traIning in famj ly planning and their interest 3UEtained by refresher courses seminars meetings and supplies of literature
d Thl techrical (xpert~ in the Office of the Family Planninl Program should maintain liaison with and guide the field agencies in implementing the family plannin~ program For this purpose schedules shoul d be marle out for periodic field inspections
420 It is suggested that the working of half-a-dozen centers where family plbnnLng services have been integrated wi th MCH sessions should be studiei for ehe purpose of standardizing the methodology of delivery of servicl~ Such a study should include staff strength patient load recoril shykeepills 10middot of patents in the clinic timing and frequency of clinic sesaios ani convenience vf patients
F Voluntary Organizations
421 I i~ internrticri31 expedence that the birth control movement is pion aTC tt volunh[~ JilC S Qltl that hen the national governments step in wi tl cmbi ti 019 prjhns wi thin the sLate welfare system voluntary bodies ieh tteir limited ilsrluces restrict their service activities and shift the emplasi i 0 educedgt (f the community training research and contracepshytive Sf vic not 1l7gtilflblr in he official program or in areas not reached by it In nagni tude and expanse the of ficial program in Trinidad and Tobago has alrad~ orertak~n Ce 101umary program Increasingly it will become the domLnart tartner in the total national program while the voluntary agencies will cOltirlU1~ to receive financial support and encouragement to set up high standaeis If service and explore new areas thus acting as a stimulus and an additi_e tl the official program
G FrOB-ram Infomation
422 Thre is no concurrent evaluation or monitoring of the Program The daa or lq72 flowing in from the clinics month by month have r8Jllsined unprocss~d tn the Program Office The official Annual Report - 1971 Sums up th~ poition as fcllo~s
ITThe Research and Evaluation component continued to be the weakest in the Population Program Although a systen of evaluation had been built into the program the follow-up procedures for analyzing the data and for correcting inshyconsistencies are inadequate Requests were made to extend the staff to establish a more viable unit but by the end of the year no chllnges had been made
423 T1e recording and riporting jJrocedures were revised effective Januery 1972 and there has been a further change recently at the instance of t1e Evaluation Adviser Under the system now established the clinics are lequ Lreurod to maintain the following records
a Family Planning Clinic Case Card - New Cases This was introduced on January 1 1972 and has thirty-one entries giving age parity contraceptive listory pregnancies socio-economic background ource of family planning information and agency for notvat ion bull (Annex 2) The case card is made out in duplicate for each new acceptor and a copy sent to the Program Office
b Daily Regis ter This fs a ne~gt1 form recently introduced in replacement of the old regis ter and is preparen
- 15 shy
ie) ruplicate the original to be transmitted to the Program (fHce and the carbon copy to be retained in the clinic Th~ is a very 121zborute form requiring 36 entries to be aa~ for each Chse nel and old attending a session includin~ (ntries to cit L to contTaceptive supplies issued
AijCleX 3 T~13e fcnnG are required to be sent to the Program lffce in i7JO balches every month the first batch for the i IS fif~eeL days and the second for the remaining part of hE month The trtention is that the data appearing in the ~EZlic daily legis ter forms should be compiled in the Program Office and fed back to the clinics Although it is claimed that this new form has been pretested and is workable ex)erience alone will show whether the majority of clinic cL~rks are able to cope with it in a busy session
bull o now-Ho Card TIlis card is intended to keep track of ac ceptor--It has entries for name addresfI and month fcr which a visit is due for each year
bull Aphabe tical Index This is a card index of clients with aidresses
Each i)at en is given a simple clinic card on which the dates of further appo~utnli rc3 an~ indicated A special fonT[ has been devised for the reporting ot cases unler the Post-IartumPost-Abortal Education and Referral Program
424 J system of monitoring progrRm performance from month to month need to bE develQped as a high priori ty The problem is not so much reshycord ng mc transmission of data by the clinics but its aggregation and proclssi ng in the Program Office every month which at present takes a long time The Statistical Officer should have a statistical assistant to help him Ln I he taflk Monthly progress reports should be available to the Mini H t~ n H(llllth and A11 offt eerlil of the ProKrnm Office so that remedial ac tl m I lAY h(~ tuk~n n rll1u- WhOnh1f ~Hfl(AlJtlaTY
42 For the analysis of data and evaluation the Program office shouln haVE th(~ full-time services of a trained demographer
H Field Workers
42) Tie Program nemiddotis tne services of a cadre of field workers to enr)ll neii aceeptoTs follow up acceptors in their homes and revive the int 2remiddott of dropouts Such a category of workers could also be utilizerl for pr1fficting other health programs such as the VD campaign and the inmuni~ation program
47 As an experimental measure one field ~]orker may be assigned to a emi l~ of Hi 000 population This would mean 100 field workers in all
- 16 shy
Earh of the workers should preferably have harl a higher secondary education otherwLe 1gt junior secondalY education They should be married persons with middoti1ltt mot tl-an two or tlree children recruited from the locali ty in which they armiddot~ requlred to function Only persons who have the capaci ty to comnunl at~ and or6anl~e should c chosen A months ini tial orientation
slcu1d enable them to start functioning in the field though reshyfresher CO rSeS tvould be necesslt1ry in due course In Port-of-Spain married mer~ a1C women may be employed on a part-time basis
I Hanagement Study
428 A nanagement study of the Family Planning Program should include a sctu iny of the top m~nagement Atructure (Population Council - Office of the Fanil) PLanning Program - Principal Medical Officer for MCH and Family Planni Ig fetices) the field structure for the delivery of family planning servics (Re0ional Director - District Health Services) including the utilizlti(n if medical and paramedical personnel for adding the function of del ve y )f family planning services and the control and communication proCed1reF Lfnking the top management with the field structure
429 The management consultants may study the functioning of the Popul tio I Council and advise whether it adequately serves the purpose of givini po Licy direction to the Program and if not what changes in its compo itt m and operating procedures may be introduced without altering its bsic craracter as an advisory agency The consultants may suggest an alern at ve form of organizati)n and utilization of personnel which in thir p nion may be better adapted to the needs of the Program
430 Irrespective of whether the Population Council is maintained or it is replaced by an agency of a different character a formation like the Offic of be Family Planning Program would be necessary for the administrashytion i)f 1 he program a task for which i 1 appears inadequately equipped at preselt Its obvious requirements are in the areas of program monitoring and el7alnation program supervision communication and training The manag ememiddotlt consultants may study the structure and procedures of this form~ tio Gnd make suggestions with regard to the augmentation of professional and ~ upp)rt lng staffgt and modification of operating procedures
431 The linkage of the Office of the Family Planning Program with the Miniutry of Health (Central Office) and the District Health Services should be sudied In view of the policy of the Government to integrate MCH and faI11iLy rlallning services it should be examined whether the Principal Medi al Officer for Communi ty Heal th Services (MCH and Family Planning) should be agtpoj nt~d as the Chief of the Office of the Family Planning Program and an adTlilistrative officer of a suitable level inducted in that Office to assist him TIle implication of this suggestion is that the head of the Family PlanJling Program would control the District Health Services
- 17 shy
432 rf 1e management consultants should examine the delegation of adminshyistratiie Bld financial powers of the Ministry of Health to different levels of Progam aclrlirdstration viz bull PMO Program Office Regional Director and County ~djca~ Officers
l33 he system of 01 af Togram information from the clinlcs to the Pr()~ra1 O~fice and tOile processing and use of information in the latter office iholld )e studied
434 he working procedures at the integrated McP and family planning clinics shnuLl be studied This would involve a study of each stage which a clien tpcticmt has to go through from the point of entry to the point of exit after receiving advice service or supplies This study shoulci lead to star dartization of procedures and functions and evolution of -lork norms CognatE st tdies of the working procedures at uni-purpose family planning clinics and su~ply SEssions should also be undertaken An essential component of these ~ tad ~es would be to examine Nhich functions currently performed by docshytors lealh visitors nurses and midives respectively hav~ become so roushytinize ttl it they can he relegated (0 the next 10Her level
435 Reated to working procedures is the problem of job description of medcal 8nd parrunedical personnel involved in family planning from the centra i tc the field level This job description needs to be studied wi th a vie VIW8Id txaminiDg the uttlization of skills and allocation of time by the staff lcc(rd~ng to the functional prj ori ties
436 frV management consultants should study the workings of the curren slralgements fOJ family planning counselling under the Post-Partul11 Post-Abortal Education and Referral Program at the Port-of-Spain and San Fenaldo General Hospitals
437 SU1ect to the ItBrcement of the Gove1nment the management conshy8ultal ts ~hOLlld undertake a study of th requirement of field workers (home vinitcru) in tmtlUI of are nnd population cov(ra~e
ANNEX 1
Names of Persons Met
Ii Mr T C Taitt Pem1(H~nt 3~crtarY) Ministry of Health
2 Dr M n Henry Chitd Medical Officer Ministry of Health
Ellubeth Quam a Prindpal Medical Officer (1S)
4 Mr G Z Jaine ~ uJiector Population Council
5 Dr Norma Andrews Medical Officer Population Council
6 Mr Jc~n Coury~ Evaluation Adviser Population Council
7 Mr A Jriseph Principal Statistical Officer Population Council
8 Dr C 0 Colman Country Representative Pan American Health )rg ni~ation
9 Mr ranca Kippel Health Education Specialist Ministry of Iea th
10 (1 bullbullines Principal Nursing Officer Ministry of Health
11 Dr Mx won (formerlyHinistry of Health)
12 M3 late Carops Ex-Chairman of Population Council
--
4i 1_ middotIIlt F-ntCWclOotf_Y v OJ t tl
GOVIIlHMEIgt(I OF TINIOAD AND TOampAGQ - NNISTJY OF HIALftf AIJIE1 2NATIONAL FAMilY PLANNING PROGRAMME
F MIL Y PLANNING CUNIC CASE CARD - NEW CASES - NFPPl
li ~~___ 1 ________
~ ecll-U
-- --------------------- shy~) ~~middot~------------------~~~~~~---CIJ------ middot~ii--middot-middot----middot-middot---middot--------- shy
ltv Writt N_ 01(111________________
a ~4itiJtmiddotl_____ ilIIIltIoI~____~____~-__----- shybull ~4
fie l$ - JO tDql IIfIA- tr-JMimiddot _ iJ 1 Odoor o
14aorielaquol_ _~ 0 lio witIleo-La ~ 01 bull - OJ ( _01 1~ltgt1lh o bull- 0$
AacJcu 0 2 CIIriIWA 0 J Os 0
Yv~MONTH ltnollOf~nfIGHTI
Undu 1100U$ Utgtdn 5SCI Undu 11200 01 ~ 50 - 9949 amp100 - 1199 02UlOO - nn9E~ (
0)~ 10- $99 SiOO -- U9~ lOO -- U99 12400 - 1359)-------_-r----shy ~l)o SIS n600 - Hm1300 -- 019 OJ200 il~9 ~------ 99~ a 1)0 m Os1)00 -- l99 1400 -shy $4100 -- 1S999r--- shy
1500 donl S6000aad O399 - lt499I~- I 0lt
ltII
IJ -IC _~tltlioltgti lS
02 IaampJIIocI OJ 04 laM Os
w Oltwio I_-l(~u IrIaa U
h~~ ~Clubl 01 OJ
IS ~C-n 01 toSIitDI 02
Ji poundI on 01 IriIIIuy M ur 02 IV OJ
WU 10 pltIoII~ llaMtl 411 cIIiId 01 Ol it fIolto ~ do~ _14 rou IIlgtJo 1Ia1 ___~_ shy
40
It _ I 00 ~bull FPIiIJ 1
OJ 02 OJ 06
)0 III- iy wOWcf ~1
aMIIl Os
11 T 1gtlt ( h _______ 4)~
06
04 (MIbullbull middot bIrlI ~___~__~_ (-fIJI ~- -~-- (1HJ 49middot SJ
U 10k 01( 1__ raquo$-4
iU1) DOl F ToWotfOlnC DOl 001 or Do [IP 006 001 OIIgtu___Spltclty DOll Nltmo 010
U1Mo I orcpmiddot laquo55middot16
1lD 001 Foam Toblelf_ICim DOl Condom DOl CoomS~ 004 oe Oos WlttuJn 1J OIkr DSpody) 101~ ~Iu 006 Rhylhm 001 DOG OJO
no wI~lmm 4 cd
(I 0) 1110 01 Condor 03 (lorn bull l S~muoidIl 04 Faa TabioolfIIltr- Os RhyUlm 01 lnJrl tible O Advico 090 06
la slt 1)0 19 loti ~rltnlt) ([)sl or 1llOn) ____ --__ bullbully-J n SV - ~JcdS
v~ Cl NCI 0 30 OJI_O I Wr blJ1h 0 I ~ OJ 1 ~ (fOOd V 01 No 02 laquo 6) Cf4
WIiI 1 172
004 001
j D middotmiddot middot
1 ~
r
~
bull I
bullI I I
r c i
ANNEX 3 Pagemiddot 1 of 5
0 raquo rshy -lt l)J ~ 111 t G) 5 shy (J) ~ -
fT1u
i
MINISTTY OF Ho1TH
NTIONl F~ILY LNNING PR-GRbullbullM-tE
~~5tructions to C11nic ClerKa
How to co~ploto the Daily Rogister
~~ ~~v1sd Daily Rosi8ter replnc~D tho one which is now in use tb$ Monthly PC~ri rOt~ arti tho 01( Ci() Dod PollJ j f m It is a pre-coded form and 1411 cl~1p Jd tl a1I6iniul-mIHvn Oel Clinic nctivi~y
110 )rm rollt biJ coupJot)d lrl cupLtcoto using a o(roon shoot Tho top aheot or oriinai ~ust bl) 6(Ult to tho CQgt1tral O[[lCO and tho carbon copy retained in the Gliaic rilo dll the for6a that ar uD~d betwoen the 1st 4nd the 15th of the oIIollth aut bo subClittud tocho office 35 Lnc blttch Those oomp1cted betwoon tho 16th _lid tqemc of tho month must bo ~cnt in a secJnll batch
P lOvLior hns boon Illllde for 25 clients on cZlch forlll new forlll must b IIlied f r poundh 50[810n2 whothur or not ono or lIIore session are hoIdiit the clinic on he sarne day
I th ro alO more htl 25 clionta 1n attondnnco at tho session the additi shyOhAl m~bOl of clionts 10 clients nu~ber 26 27 etc sh0u1l be ontered on the next Imiddotrlll ~i ttout a1tpoundring the numbtlrs in the cvlumn hond Series
51 ppOfil th~ number of aUcnts lQr that session ws 5 this would mean thllt two rJlS ~ lst be 6ubllIitt~dl the first filled uF 1 tltgt 25 And the laquoIncond 1 to 10 Th~ cal bon ofies should bo st~plod togother at thu t0P l~rt h4nd corner of the torm ard ktpt in the Clinic filo lou IIlU6t stapl~ the originftls in the 8~~ monnshyer for lIub~ssion to the ofticl
ie h~ ll idontiflctior- (cc 1 - )
0 lot Ji 9 anythin~ hGro poundhia is int(mdClc for tha computer code
2 ~~pound~ - Print clOflrly tho name of your Clinic
C1Lic Huml or - (cc 4 - 8) Evar1 Clinic Numbor has 5 digits Virite each dig t il a t$purate box
It Pai~_thllsectgdllion (00 lt) -1 1) - Dl monll 10M
lw) bolte IlrO proY140d fetr olAoh pr 01 thQ dISh Enter tho dA) ldns a R
d16ih
emiddot5middot (0 11 I for 115t ( 0 21 for 5th etc Treat month the am pay
e ~ 10 ~ I for I-hrch 0 [2] for September Tho y~nr must be (into ad
I Z I ~ I I 71 q etc
Take as in IixulIple tho dOlte 3rd tllrch 1973 7~ie must bo written
[0131 LSLDI[7l3JDny Month Ye~r
5middot 1~J $~~ - Irom ~-------- To --------shytntol hOI II the time the Clinic 111118 in SW5sion emiddot8middot
(i) 11011 500 lm To 1200 non
(11) Frclt 100 pm To 400 pm
(iii ) IX-OG OO pllI To 6~00 pm
f
2
ADEJ ) Paae ) of S
6 Eov
_ 1hA 1gtIpoundC iIIUlt be nu~o7Ifd tler1ally 1 throurh n lU tbey Are Wled In ~1l8ellJ IInel 1301 tlU 1 Orcl 1 Wled tor a o5038ioll - -I 2 tonY tho _boul~ b I1WJbtl 1 and 2
hlrlll are 25 linos OIl the fOnl Ilnd thoae muet be UBtleS for 25 clients 9 one ior bullbull 01 I ini
ot ~h lc II ol1cM lOlivpound til e linic before soeinc DurOI or doc tor ilnc ii hox rristrltltion nUlJbet had alrearll been recorded on the Dai 1y Roiuter then n line ~hollld be drawn through that entry an1 the eliort nust not 06 includttd in tho totals tor that 0eDion
1lw Ileifitration Num)~r of cueh client must be IiIritten IS n 5-dlrlt oode ClhnC IH11IlElr 315 1IIU8 tborotore be enterod 18J010117]5]
~ Clt ZOt
Coda 1 Codo
10 ~tl c 2t j co 21)
~w elSe - Coda 1 0) d CltaEl - Code 2 Revislt Code 3
Only pound1 01 theBe coiles may be usod
11 prol-O~ ~Eil~1 (cc 22)
If ma climt was L drop-out IIho haoS returned now to the Clinio tor tho first no linmiddot bullwin lt1ro1eo o t he or she should be given CCe 1 It this do 5 II It nprlly leu this colWlln blank
u Hothod middothisllill loe 23)
NOh til t otly ~ Cod 16 tp he ontered in 2lpound of the columna oven thOUGh 10 co11lllJlB 10 provided on the torm The Codes llrol-
Oral Contraceptive Code 0 1 U D Code 1 Condom plUD Codo Z Condor (only) Code 3 Foum tAblets cream Code it DitphrClGJII Code 5 Rhythm Cde 6 Injectible Code 7 Advice Code 8 Other Code 9
It for middotDo-le 1 client rlllll ji yen cclldorls ord foam or creall Iou Qust entor Coole i (condom plulJ) in the appropri~te column This Quat be the only lIotmiddot) tarcie If an in the cnse of a tlnle clinic I the client is Bup)lieu lith COIlOrW only you rmot entEr CorlQ 3 (cpndolll) Do not use a ticII ~ tho (odo Nwber
It is CUi tomary fur 11 cliont 110 is beine put on the oral contraceptive for the first tiT1o and even on other occasionn be issued condoms and 11 crelle or foam a Ilell rI3 a pgtcket of pilla In such Cllses when the piDQ Ilre Ilctually iouou you tlust record Orll (Co~e 0) 08 tho onll metbod ilo othor ntry sll0uld ho nnrlo
Uovever n SJC~ canas vucru condoms and fOHa ~rc eiven but no pilJa (even thoJRh _t _n the intention to issue pills nt the noxt vioit) than the Mothol Th5 ifli t ohoulcl be recorded uo Condor Plus (Code 2)
13 Seen Bybullbullbullbullbull
~rot S-1 SO l
Doctor (Dr) - Code 1 j Nurse (Nul ) - Code 2
Clark (Olk-) - Code If tho Clhnt is vcen hy both tho llootor tlnd the Nurse enter Code 1 t Doctor It 6~61l by the Nurso only arite Code 2 Cod bullbull Cerk is l)llnt for FA Cllnica Clerks in tho Government Cli1t hiwo Llttoll istructed not to i56uo supplios on their own volition
14 fl221~
lhio S~tiCl of -Ie fvrtl t~ke 16 (llrci coluMna (cc 25-+0) nnd 10 tho only part at th iOIQ in llich iore thAn one cod is Zlccoptl1blo Tho purpoco of the )ecton is to 0 able to arrive nt the Cjunntity of 6tock dilltlitJutshyed YOI IIlUdt writo in the CllllOjH-iata colulna the nUllbJr of Il1ch 4rtic1o i~JSu~d ~lo e ha I Oral Contrcilpti vea are aub-di vi dod into types ae_ 3 PIllCKC 9 0 Elynnn LlUot be entered Codo in card column 25
If tor eXllrplc t l cliunt is iosued wi th packots of Zucynon nnd aJ(1 ~ivn 1 conuotll (8inoloo) you ouot enter in oard column 25 and 11 It
cnrd col~8 )2 and J (io 1 in card colucn 2 nnd 2 1n card coluun 33) Nota C)lldoIlU ale to b(t ruoordod individually not os packots of throo) Should n ne LlondoClo be isoued thil3 is to be rc-Qed as 09
If It clint 6 t~ot isoued Blly lIupplies thon you must writo Codo 1 in CQllAlilD 41
It Q eli nt isite the clinic to check on her LUD or her Diaphra~t IUId ro DI W 6 ppl ills nre ispounducd then Code 1 1s wri t ten in column 40
In the FA clinios here a variety ot orll contraceptiveo in orer~l tho elerll wilmiddot~ bJ provided with a specill code shoot The idontifyin coo will b wiittn in Column 29 nnd the nUlber of packets iosued in colwm )0
lralaer-In Code 1 lrllllsie r~ut Coda 2 leIllPQrArr Trnnsfer-In Codo gt
In the cao of n 2ratl8fcr-In I you lUot n160 cOrlpleto coluons 42-51
In the cllU J of A ~~emporary TranGfor-1n (an individual who i8 only v1citing fur clinic tor some epecial trcatcont hna who will bo rdnlnin
~middot(II~~~fO~l~SIl~I3~nn~~~h~rO~nh~1~~190~~nll 2-46 and ler rei IItrntion numbu in colullnll41-51
It the oli( nt i iNt a CrllnoforwIu - Out or loClporu1 tMn loave oolumn 1 blank
16 lr4nst(gtr-tl2~~morrry TilJnder-In (co 42-51) Forl1ltl CUn E1~ (cc 112-46)
hen you rei iatlr L irllsfcrln or Il TJlporary Trnnsfer-In you IIIUBt write I ere the five-digit clinio nucbor of the Clinic iraQ which tho ltlient Me (uIlO
2mer ]letr ~2n ~ (cc 47-51)
frlta fllao Clo r-~itrlltion Nuc~Er ot the client in the Former Clinic (i c bullbull th 1 Sis rnmiddotion ~UlIlh()r which the client carrics 1n the tormor clinio) bull
It tho Forrltl Ho( ist rntion Number iIJ not readily wnilnble you tluct oocpluto thtl epcciol [orlll Transfer-In Not Identifiod Dy Forrlcr RCGi(trn~ t10n Nwlbvr Or ~ flt)rCl is to be cOlplctcd for och cnso nnd th forlJO Ilubmi tted to thu )opllntion Prorrnnme Of fice tOGether with tho Dily Ro~iBtors lhwev~r should the clork leuTI of tho clint B FormlI Uocintra tion lUlllb r )0[(10 Cubmi ttinft the D1ily IOCI otro t hen the nUQbcr shoulo bo -ri ton in colucns 47-51 lna the special foro should lJo deotroyotl
l7 bullbullbullbullbull
r lt bull bull
ADXI ) Pap S ot S
11 UD LV~ (cc 525)
It tb( cliont io ~ivQn An IUD tor the firot tl~o then you should Sri to Codo 1 Inuort ill colurJI 52
It tho olimiddotsnt ia rvinGgtrtltld i th An I UD bullbull tben wse Coda 2 RelnDltlrt shyin (01Uil11 52
It the clLmt is ~tte~~dint chnic beruse her IUD CflClQ out by Haol (cxpll Iion i ~hcn fir te todo ~- UIlllrli1 53~
If c-ltr IU fj IIIS reov in -ne cllnic by tho doctor or nurso t~on vlritI Codec in column 5
II the eli nt otends eiLlie tld explin[l th(lt she rccovcd the IUD tlllleel nen write Coda H in Colwlm 53
It the IUD jr still within the uterus nd the WOIraquoI1 1 11rc6llJlnt thon lIrite 1gt40 4 in Column 53
lZ np h5t (ce 54) It 0 Pull 5mor ie t~ken durin thi visit tben Codo 1 ehould be ampDtere4 in ColWlln 54 Should he c110nt lltt rQ(uircd to rttturn to clin1c for a rogtol1t Pnl) t06t then CoLe 2 llhould bo middotwrittcn in column 54
It no Pllp Scou io taken tde visit Itove colUQn 54 blank
Iraferti1lli (CQ 55)
Ii the e liett io nl1 infortili tr eaoe use Cor1o Ill in colUQn 55
If tbia 1000 not tlpl lonve column 55 blonk
20 Totaltll
CO~1ploete the [)ldegO 1gty puti YI tne totals betweon the double lines nt tu b()ttctl Carrj colUlllnc 20 21 nd gt4 Must hlve tho Bnoe JllIIber and thiG Would coreslonc to the numocr ir attencbnco
Writ$ th to1ul nUlllior of Drop-Outs returned (c022)
Urito 41eo tb totnls fOJ each card column 0 to 9 under tho h(adinu Method thiB Vioit Show tho tote L fgtr OlCl type of contraceptive issued (cc 25-40)
1)0 Dot wrLte 1111 totll lUl(Ier Card Columns 15-19 29 41-51
21 COPmllh bull ~lt h~t~ Monthly ROilort
OQ thG DaLl oCator forlll thnt ccrrOspOldB to tho 1(8t 1$06610n lt 0
oth yo Olllt (vwlgtleto the items nt the botto of the [orampl This is tour ontll~1 n(olt nnd includcD tho totll lumber of sesions Ilntl tho total Iluolcr ( r crop-outs durinr the Qonth
An tiUlsilt n drir which n doctor liB in nttcndnncc is a doctor sOfll~1on and shoulc 00 re(liGtcnd in coltns 56-57 All other sessions 1116 conlliid~recl supply stllciona and thtlY 1110 rocordod in columns 58-59
the total Ilum)nl Jf drop-outo ld the drop-outs by method durinc the onth nre 10 bu oltorou in the inrlicllted boxes
72 Chad Your ~
Milke I ura th t all thE fijul4gtu rre c101r -tNever writo our nutlUQrS 50 InrjEl that they oxtend out of tho
ap~rotr1ato ~ox
Cheek to BoJa tht 1111 numuors 1110 in tho correct boxes -- CJslHloially when Writi1 the totlB
Mllxe Cirtc O thmiddott t1e infoT1I1ntion i6 clear on the corbon COllY before sep rmiddotinr the sheets
Jitn the Fomiddotl lien tly sien YOUl nr me 1t the bot tOil right hnnd corner btl forc subol ttinG it Keep tle CL rb n copy for your rocordn
i
-l ________~~---------~
I _1
Adminiatr-atlve SKVieu
P inba ~~~l1cal lrlnbin~~eltltcal -1 te~ra t~~rvicc (lnatittloaa)
--1- - shy -1------------_-L_ l-r-aJiil- shy _-L_tet1lal d
PlIinm1tJ8 atdUon DetalMid H8Il1tb ~ ________bull Care
-----~ Office of i
the FlIily _IPlill3 roarshy
1- - - -------RegiatUll urnr
ltIi 1 Drelttor Rcgicaat Director Souta Tabqo tacallortb ~ counu gt____ ~ (4 ouottet)
Off1ce of the Res10nal Diractoc L
r----- _L_ -- shy i I bull IREgional Ipitl I
District IIttaltb I bull Othn RelOl ond Hcpital CenteIntt itlt j In 1__ _shy-~- ---- -_j
J r Ii~lth
C~nlef
L
I Ihnlth lie I th Offlcu (1ft lc~
Coullty 1I0p1ta1
Henlth tentet
I

1) rle Youc fUfCt1 oning in an atmosphere of Lncertairbully n(It-oL2 in the National Family Planning
amp11 t~ms c frence cf the Council should be
(ii) The PJPl1~atcYl CcmncU should be strengthened by including in it (a) the Permanent Secretary Ministry of Health (b) the Principal He(lical Officer in charge of MCH and family plannlng services () 8 representatlve of the Ministry of -inance (0) social scientst and (e) a representative dtich of the aSRociatioi1S of the medical nursing and teaching professions and cqantzations for womens welfare
(Hi [he Offh( ci h F Planning Program (Program Office) hould be strenghened by augmentation of staff at the professional as vel1 as supportive levels after a work study Ir ramptLicular a demographer a media expert and a trainingsdviseT should be inducted into the agency
(a) set anntncGgpts for the enrollment of acceptors at each cliniccenter and monitor progress in relation to these tarets
(b) establish schedules of periodic inspections of clinics
(c) cvnlvl 11 hlufltfmiddotr lgt1~n for the training of personnel and
(d) wor (ltH U 8t(nte~) for Tued1a communication in the light of public awareness and knowledge and the reach and cost-effe~tiveness of different media
v) The Ministry of Heath should invite suggestions from the Director of the Program and the Regional Directors with regard to the deshycentralization of administrative and financial powers currently ves ted in the 11ni8 try and work out a schedule of powers to be exercise tdltclcr )ve of Program adl11 nis tration
F~eld Workers
(vi) A cadre of field workers should be created to promote the accepshytance of family planning in the community As an experiment one such workar may be assign~d to a unit of 10000 population
(vi t) 1ne orgai c Y1 anlti j~lrcgemeu of the Program should be reviewed cmjoLntlyamly pcanning expet and management consultants
r L the fr]lcwing topics
a) thc 1lt0 V 71rmiddotlCi f Cn1t1t structure comprising the ~inis ill Hnal th ~he Ppulation Council and the Prc~r~1 Office ~te feRsibility of alternative models of inatit~~iacnt ~
(b) the s taft re(luirements as well as operating procedures of the Program Office
(c) the ltitin n t[iv and financial powers exercisable by Program uthori ties at different levels in relation to dgtE le31H of lesponsibili ty
(ci) trc JlU l1 of coordination and supervision of
(e) the staffing and working procedures of integrated MCH and family ptanling clinics including family planning counselling 8eVmiddot Ck ~UITli s Rilet recording of data As a part of the study ~ Ulti~cti(ns pe~iolmed by each category of staff - shyme6ic~1 rn ijed lerical -- should be examined to idemi whimiddot rune dons can appropriately be relegated to che next tower level so as to optimize the use of available ma1pow~r
(f) the system of flow of program information from the field and its processing and utilization in the Program Office
(g) he ost-ParttmPo13-Abortal Education and Referral Program and
(h) the requirement of field workers for conununity education creation oE ltiemand for family planning services and conshytinuous c0ntGci with acceptors (The type of functionary needed content and duration of training and the norms of work should be suggested)
I INTRODUCTtflN
101 0-1 behalf of t~ H~1k ~middotmiddotr R N Madhok (Consultant) visited Trini12d ad Toblg0~ middotl iL bullbull ~)3 0 review the administration and mal1agme)t )f thlt hsd j 11]) PVnning Program During his stay in Trinj dad 1- MadhJk ( iilh eprefEntatives of the Ministry of Health and the Topu ation C01Jii1 fuJI li5e appears in Annex 1)
102 ~pecifgtUy ~~C iVlsdhokcevievled the following aspects of the progam
a he future role of the Population Council -- whether it should )euro an advisory or all (~ecutive body its administration staffing and statutcry pmrer under a changed set up and the consequent changes required in theliinistry of Health for the implementation of the prc)gram
~ J the extent of (l~i-5ting (Jpcfntralization of administration of health and frunily planning services and its efficacy
c the desirabiLty of integrating family planning with maternal and child hcaLh services in the light of experience of inteshygrated i~lirJ(
d the efficie~ Cf~ll edsirg system of the flow of program information ac ~Hl red charges and
specific aspects of manager-lent and manpower utilization on which the management finn should concentrate during its study
103 The following report contains broad suggestions on changes rE qui ed in the existtYg structUrEgt
II ORGamp~IZATION OF THE NATIONAL F~~LY PLANNING PROGRAM
201 The administration of the National Family Planning Program is the rl~sp(jnsibility of the Ministry of Health In 1967 when family planning was adopted as an official policy the Health Minister at that time proposed the stallishment of a Population Council to advise the Minister on the organizashy1ion of a natiorlal prorrun 1i(h lIIotld coordinate all family planning effort n tle country Tlle Cabtn2t c~ciCled that
A Population Council of Trinidad and Tobago should be instituted for the purpose of giving overall direction to the Family Planning Program in Trinidad and Tobago with a view among other things to coordinating all fanily activi ties in the country II
- 2 shy
202 In pursuance of t l= foregoiny decision the following terms of refer nce were framed for the Po1)ulation Council
10 i~vll ditcoction to a Family Planning Program fo Y ltdd cHl T0bagn d th Ii view among other things to eo ~ ~c n lfllonrdnr activities in the
203 A PTOlllH~ f(cibor nf ttl rredical profession was appointed as Chailman llei the lill~1L y h2 jiamily Progran Ministry of Health as the Secrltar r (r th C~-ur~ ihe membership of the council comprised officials of tle t-instry of He3ltii and other departments representatives of the volultary agencies operating family planning services and leaders of opinion the present Chairman of the Council is an eminent gynecologist in privmiddotte practice and a former Minister of Health the members are as foIl 08
1- Chief Medicnl Officer MOR -l Spcclliflt ~middotjJ3C Officei- General Hospital
3 A rEpr~senative of the Ministry of Planning and Developneut
4 A represehtacive of the Central Statistical Office 5 Public Tidaions Officer Prime Ministers Office 6 ~ PrilLj~d t1lt dq Officer NOH 1 ~e( CL bull ~clmiddot ~~t)pulati on Program H Chid ~ea~h Educatoi ~lOH
9 A repres~rltatiVE of the Catholic Marriaie Advisory Council
10 amp 11 Re~)resentatives of che Family Planning Association 12 6 13 M~mbers or the Publi~
14 Diector Family Planning Program MOH - Secretary
Olj The Population CQtJrdJ hal three roles (a) policymaking ll) I rogralil formulation and evaitllt1()l and (c) providing general direction fllr program implementation Its composition is designed to ensure (a) intershydapamiddottmental coordination withill the (overnment (b) coordination between the ( Ole-nment program and the activi ties of voluntary agencies and (c) rapport vith pblic opinion
05 The Population Council is assisted in the task of program formushyIation by a numbe of committees ~thich are so constituted as to draw upon Ihe ex lertse avalIahI wi tlin the Government as well as outside Pre-eminent arnorg heseuro commictees s lhE lati()nal tH Program fnLMulation committee ihi(h technically speakirg is not a committee of the Council but a commitshytee of the MOH It inter-meshes with the Council since it is the policy of the Government to integrate family planning services with MCH services delivered through the network or health centersoffices of the Ministry of Health This committee is headed by the Principal Medical Officer of the MOH in dnrge oE Integrateci 2~edicil Care now restyled as Community Services
- 3 shy
which COlT bull Se 11CH anii IIgt sxvl(s I1H~ other committees are Community Educaior and Publidty Cvrm] ttec Research and Evaluation Committee Family
~du aton Comrnirii ~~e(i] CCimittee and inance Committee
OS i~ n1eptUd~ i p Ni ~runi t 1 an advisory body and as such itus 10 execl1lt)ltjmiddot n p-actice the Office of the Family Planning Prog) am e tabisLecl wirgtmiddotcn tilt2 middotlnitry of Health functions not only as the ecr ~tc dat of lIC )hiCJl but also as the instrument for carrying out lis lirEctvls Furtiie ch GOtdcCU has concerned itself nomiddott merely with broal i~ SUIS f10Hc out also vL detailed implementation The majority of t le r emmiddoters of rhe Council are in favor of Umi ting the Councils role to tile givlng of broad direction to the Program
20i The Office of thl~ Fitli1y Planning PrO~rall1 is comprised as follows
Dlrcct0r (Incant) Medilal OfHceuror (Famtly Planning) Nm-~If Offieer St~tistical afficer Health Educator 2 lield Workers (for follow up)
(OIlE positor vacant)
8CCiHWlcnt 2 clexks 2 typists 1 driver 2 proj ctionis 15 and 1 messenger
T- ~ g af f of the Office of the Famly Planning Program is under the discipline of thttinistry of Health since the Population Council is nei ther a departshymfntal unit nor a separate legal entity with its own fund
2 OB The places of )nrm1 atton Council and the Office of the Family p ~anr ins Program wi thi n the Minis try of Health as conceived originally by tile Government may be seen in the abbreviated version of the chart appearing hI different official documents and reproduced at the end of the report
~ 09 In April i973 at the time of the consultants visit there was In aCIDc)sphere of uncertainty about the administration of the family planning l)rogram as a result of changes in some of the top positions As a result of t c~binet reshuffle the portfolio of Health had changed hands The Permanent euroctet lry who is the princ~al ad~liser to the Minister was new as lras the r-i c al Yedic1l Officer h charge of Commurity Health Services (Mel[ and Pam ly Pl1nnhg) The Dtnct0 of family Planning who was managing the Office of middothe Family Planning Program and also serving as the Secretary of the PoshypUlition Council had reCiTed in March 1973 and a successor had not yet been named Meanwhile the Medical Officer for Family Planning (a part-time employee) was carrying out the functions of the Director in addition to her OWT Wi thin the Population Council the advisory agency for policy-making
and ccord~n8tionJ there was a groHinr feeling among the members that the ouncl1 510t1d shed thE respOJ1sibili ty for implementing the program a funeL on j ch nad heuroe added on to its advisory role with the passage of time
iO the 1 ~lp~1 the lines 0 responsibili cy were not clcay (e ned and Li1 refioal system was not fully functioning The post of Re ior 3 Director crth VIas vacant The policy seems to be to strengthen the 1St tu ion of Pt()1ic Flealth Office as an 3ency for the supervi-middot sion)pound ne district sflVices (health centers health offices and school servi ces ~l thin the ccnmty
II I PRES EN STATUS OF THE PROGRAM
301 ~he adl1linistrt~ivE changes narrated in para 209 have come about at fl tin e IJhen the P1ogram has entered a phase of declining performance as is 11 Jpal en from th colloHing figures taken from a report submitted to the Populaton Council
YrUL 10C7 ~j8 1969 1970 1971 1972
--- -- ------------~~ --~ - shy----shy
Ne Acceptors 3696 2731 16207 9997 9898
(End of October)
7560
Slur~e Family PlAnnto Program Report (no date)----AsII1Ulilg that th6 ttlrollmant of new acceptors during November-December 1972 prclrd at the 8ame rate as during the ten~onth period January-October
- 9i2the total enrollmslt in 1972 would be lebullbull than 8500
3(12 lhe total number of leW i-iCCeptors for 1971 shown in the foregoing tal11e 1s at variance with the following data from the 1971 Allnual Report
- 5 shy
~ev C~~ Contraceptive Method and Agency
nm Other Advice Total New Cases
Aeny
GovrrmenC ProEllil ___~zZ(lt1____ 97____2Lbull499___~528~___4i_750~_
Farr Uy Planning Association 2814 315 607 76
Catholic MarriaAdis1ry COLnc_H____
ge
74 88 162
otal 31[10 692 8724
_--__------------------shySOlrce Natio
1973 nal p
Fam29
ily Planning Program 1971 Annual Report April
NevmiddotrneJl~ss) the declining trend in annual performance after 1969 is manifest ana conpaes unsatisfactodly to the following targets set for the Program
Targets for Contraceptive Users - 1968-72
New Accep tots Old Cases Total
1968 20noO 20 000 lO noo
1969 20000 40 000 60000
1970 20000 60000 80000
1971 20000 80000 100000
-----__shySource National Family Planning Program
p i9
------------------------------------
- F shy
3JJ3 Ttl flient recrvitTrent has fallen off since 1969 in spite of a signif Icar t xpansinn ir the number of Government health facilities providing family paarin~ services FrCli1 7Hr to year Starting from scratch the number oE GovE(nment health irlstitl1tions delivering family planning services in isollL(Od ~ily pltJfAill~I ~J in c)lchiratinn ~7ith MCa services has lWW risEn t 4 lhis ie --tdt)p to t cii1ics organized by the Family Plannin Asce1ation bull U2 by tile Catholic Marriage Advisory Council which offers the ~h)lthm meti1middot1 nT
304 1i ciecli ne d~ d re11~m2nt of new acceptors coincidentally w-Lth th~ eXlsioH uf s-crLce facilities needs to be studied to identify the factors responsible for it eg the quality of services offered the strategy of commmic at~on and motivation and management and supervision One obvious gap is he abgtence of an agercy for promotion and extension of demand for family lal 111 If services -gt tLe field reliance being placed mainly on clinic counseUn H1d generaUzmiddotd mass media publicity The need for a field promoshytional agelcy is underscored by the dropout rate In 11 draft paper prepared by the Hed_cal Offic(1r for FIrnilv Planning it is stated that by the end of 1972 t ile Heuroe approxiclt ji rHJC cun~ent users of contraceptive methods and 33 per ert dropouts
305 rht~ program is cot merely clinic-centered but also female-oriented Recent Iy mellsages aimed at m11es and stressing joint male-female responsibishyIi ty l gtT j ecillc CImt-J 1 i~gtVt~ b~~in )7cn 1n0 the cOTul1mication activity sUf1 tv) c nts Em he 2iucaccw i milc8 and che distribution of condoms to them illVC he ~n or n~d iD r GJvefl1nenC s(~ctor The Family Planning Association has a130E~k11 the irti U3 1V~ to reis ter males ln industrial employment Tllese are steps in the ri)n dtrect1ongt but the size of the problem indicates the n~ ed OI a concerted effort en a much large r scale
306 Tre Program relies largely on the use of oral contraceptives as shown in the following table
Oral Other Advice Contraceptlves IUDs Methods Only Totals ( 100)
19)9 76 20 16207 ( 100)
1970 316 63 9997 ( 100)
1971 50n 4n 365 79 8724 (100)
Family Planning Association unpublished report
----
- 7 -
Althougr amJnp the neH acceptors in 1971 the users of oral pills were only 509 ~mon~ the old cases the figure was 119 The percentage of IUD users has remiined stagnant at an insignificant level this may be partly due to consume prefErence and pctrtly outng to lack of trained staff to undertake IlTD i1srti l7U There h hOHever a visible shi ft towards the uSe of othe~ ilettods (npchani81 and chemical) attributable to a scare about the side efects nf oral connaceptives Among these conventional methods the condom s 11 os popular
307 J t )resent fami ly planning services have been extended to 48 out of 106 hellth centersoffices run by the Government and the objective is to C)Vel t1e remaining health centersoffices within a short span of time so that adice and facilities for the practice of family planning are conshyvenient Ly wa nable to the people in all parts of the country By ann large sepanit e fITti ly planning eli nics are held on specified days as an addition to norrral lealth work Besides doctor sessions at the clinics supply sessions are rur by health visitors and nllrses assisted by clerks The nurses are authorjzed tc issue oral contraceptives for a period not exceeding three months ani the acceptor is required to attend a doctor session for advice during thi jnterval In 1971 the numbers of full-timepart-time staff in Gov~rtmnf centers renderinp family planning services were
Full-time Part-time
1elical Officers 14 8
NUseMidwives 35 19
Cl~rks 3 17
Now tile low~rnment -gtbjective is to integrate family planning services into MOl services and use the same staff being used for the delivery of both types of erlices at multi-purpose sessions However so far only 1A centers have interated family planntng with Men or gpoundmeral hpalth care sessions
3011 The Family Planning Association has eight unf-purpose centers where famil) pLmring services are available ftve days a week The Association employs tilrEe full-time and ttJO part-time doctors a complement of 14 nurSeS (who llave been trained to do pelvic examinations) and 11 other clinic staff membels The Association also has a number of voluntary workers in the clinics The CithoUt Marriage Advisory Council has three clinics but their contri shybution in terms of enrallment of acceptors is not signiflcant
3)9 A Post-PartumPost-ALortal Program was started in 1969 It is state I tlat about 14 percent of the patients reached attend a family planning clini~ 1iTj thin six weeks of the interview in the wards IhiR is qui te a low figur In 1970 when a system of home visits was tried under the Family Planning Aide Project in 7 clinics the rate of acceptance doubled in three clinils rose by 50 percent in two clinics and increased by 24 percent in one clini (No change was noticeable in the seventh clinic) No decision has been Inad~ tmiddot) continue extend or modify this Project
A Po~ulaton Council ~-----------
401 he fu~ura ro~ Lh~ ~~~01ati0n Council has to be considered in theli1 A the tasK t~ lL ahead of the ~ational Family Planning Program At pesent tile officil~r(QSrJ1Tl is prirnarily concentrating on two objectives (a) tIlE excpound1sinrt of fmd plannin~ services to tie remaining 58 health centen cLJs as rapi(ily as possible and (b) the integration of family planniT g VI tr MCH services Thus thG administration of family planning serviCHJ will be merged into and become part of the Community Health Services Since t is ()rganizationally undesirable to disturb unity of command a separa1e elteecutive agency for the administration of family planning services is preempted within the existing policy framework An executive role for thp Pcnulc tinn Council is there fore ruled out on this consideration
402 If the Population Council is to function as an advisory body at the p()Lic~ aId progra1l pLilnni-l level snd not to concern itself with the minutile If program execution there wonld be no advantage in giving it a statutory stltuS But if it were the policy of the Government to set up a verticll )middotro~ram for family planning ii th a field organization separate and distir~tOroll the HeaHh administration it would be quite appropriate to establish an autonOiTiOUS statut()y a~fgtny ntside the departmental setup of the MinisiY of Health d~b a budi~t md staff of its own commensurate vith the rE spo lsi hi Ii ty to be rEs j Freed from the usual departmental conshystrailts ~n the matters Cif sp(ndlng a1d hiring and firing of personnel such an aglncy c(uld move faster than a heavy-footed departmental formation wi thin a Mins trl bull Hovever a hody of this eharacter would need to be cas t in a cliffe ent m(ld than the present Population Council The shape that it would take lrould be more like a Board of Management with a full-time Chairman or Execuive Director and with more functional expertise than representational charater But an advisory council with an autonomous status and no responsishybilit f( r lrogrrun eXIGulion iould be a source of friction
403 r~e existence of the Population Council as an organ of policy advici has certain advantages Firstly it is a forum for developing a national poLicy in which officials and non-officials participate Secondly it pr )vi bulles a focus to ti1e official program vhich it otherwise may tend to lose as ~ontraceptive services are merged into the general health services Thirc lymiddot- and this is important -- the Ministry has extra-departmental advice availabL to it~ but the Ministers constitutional responsibility for the condl ct )f the national progl~lt~ le1lains unimpaired
404 ls an advisory Q(dy the Population Council should be more broanshybase( than it is at present For instance it should include representatives of tile organizations of employers and vorkers associations of the medical nursngmct teaching professions and organizations for womens welfare The Counil should also haye a social scientis t on it On the official side the
- 9 -
Permane It Secetary and the P1O (fen and FP) should be brought into the Council he inclusion of the Permenent Secretary would open a channel of communi~aton with the MOR ae the highest policy level next to the Minister and would (ontribute administrative expertise to the deliberations of the Cou1ci1 ~m f icili tali 5 (pleuenrti)D of th~ recommendations of the Council within the -rni and in OUltL depa-cments The inclusions of the PMO (MCH and FP) wOlld el) emphasi ~2 hs responsibi lity toward the family planninR program Some officrs of the HOH (eg Chief Health Educator Principal Nursin~ Office e) may 111 ea~e to be members though they may attend as requirE d nmiddot the agenda before the Council A representative of the Ministry of Fin nee stQuId be inc~uded in the Population Council This would make for a lettr appreciation of the needs of the Program in that Ministry and fadIi ate fj nancial sanct ions
B A~tatutory Council
40S In the foregotng Pgraphs the view has been expressed that within th edsting policy framework an advisory Population Council would be more tli)prcpriate than a COlincil wi th executive functions and powers that an advisory rOUlcil would not gain by having a statutory status and that if a statl1tory body 5s to be set up in lieu of the existing Council it would need tC b structured more Iiice a Board of Management than a council wi th a repre13entttional charact~( n the latter event the statutory council should have fu 1- time Executive Chairman or failing that an Executive Director functj oni1g undel- a Chairman trno can devote considerable time to the business of tlw COlncil
406 T1e Statutory Council should have its own budget with full operashytiona pOlo1ers It should have the authority to appoint its own staff and regulLte their conditions of service If it is constitutionally possible the Couner1 shollld be outside the jurisdiction of the Public Service Commission in pesornel matters
407 As an instrument of Government the Council should be subject to such ~eUfral or specific directives that the Ministry of Health may issue to it frcffi ime to time This should be written into the statute under which the Cmntil is set UD
408 The composition of the Council ould depend on the functions assig1ed to it It is suggested that the Council should not concern itself wl th the delivery of cliric selVices in the field The Ministry of Health may (ont nue to administer rampmily planning services at Government hospitals health cmters and health offices and the voluntary agencies should run thei] OWl ~rogram The following functions may be handled by the Council
- to shy
s rrogram plannin and target-setting
b proram monitoring and evalllation
c wiL of d 1ci(JTIdnCf by inspections
d Qrg8lizatim 0 es and marketing of contraceptive J~1J-s BLl (iV es at subs idi zed rates through es tablished 1 2 d(~ channel
e information mass media communication and audiovisual ublicity in the field
f prorrotion of famil~r plannIng acceptance through face-to-face cotlmunication by poundi eld workers in domiciliary visi ts
g trIining of personnel
II pr )motion of -esearch enJ
i financial support to voluntary agencies providing family planning services
409 n Statutory CCii1cil may corsi5t or an eminent non-official vith a comri tm ~~1t towacds foJlily plailninf nd the fol1owin~ members
I ~ bull Pfrmanent Secretary ltl-tIlH
Chief Hedical Officer HOH
i Principal ~ecHcal Office ~mH
d Pilhlic RellltionB OfJte(middotmiddot Prtm~ Ministere Office
A represen ta ti V~1 of the Ministry of Education
f ~ representative of the Ministry of Finance
g A representa~ive of the FPA
h A representative ot the C1AC
i H social scientist fcum tle University of the ~Jest Indies
j Three non-officials with experience in management and administration and the
k Director of the Family Planning Program - Secretary
- 11 shy
The COUlcil ITIltW constitute cOlClmittees for Finance - Accounts Personnel and Sup lies nd Stores ir~whi ch )nly members may be included Other commitles sc1h as those 01 training info1nation and education and researCl ara ~valuation r1ili also include experts from outside
410 he Off1ce raquo) cc im Panning Program which at present forms part of th ~Hnis try or [i n should be placed under the Council and its staff strelgtl ilcn~ii2 i~ r181 it may cease to depend upon the services of the Mir is t y of H~alth
C Office of the Family Planning Program
4 11ollwther the Offic~ of the Family Planning Program remains a part of the Mirisry of Health or is transferred under a statutory council if one is set uP i needs to be strengthened to meet the requirements of an expAndshying pr )gn m At present the following sys terns need to be ins ti tuted in this Office
a a 3ystem of setting annual targets for the enrollment of acceptors and the projection of service fadli ties in relation to these targets
I Ci ~ystem oE V)glC loHitoring (the monthly statistics flowing from the clini~s c~iiiain unproc(~s5erl for months)
a system of program evaluation eg demographic effect of tte program cost studies
1 an overall design for media communication based on a study of the reach a~d cost effectiveness of different media and the effect of the meflBsge content and
e a m88t~r plan for training which would comprise an assessment of the training needK of the existing staff and future reshycruits and a long-term plan divided into annual programs
412 Th2 Prograll afiie s~lould have the services of a demographer and a meeia expert A training adviser is expected to be provided by the PARO
413 1be Program Office should evolve schedules of field tours to overliee field operatio1s E~1eh health cente heal th office should be visi ted peridicaLy by the Milt~dical fElce- the Nursing Officer and the Health EduCltoI who should guide and assis t the local staff in carrying out the progam Their tour notes should go into separate dossiers for each institushytion and ~ach dossier should have basic demographic data about the area coveled by each institution These dossiers would be a useful record for revilwing l)errOmance The staff of the Program Office should be augmented to Ol)erte this control procedure
- 12 shy
D Decentralization of Powers
414 ~hete is a concentration of administrative and financial powers in the 11in s try of Health I-JllJCi1 results in an accumulation of references in the Miristl) and delays n field operations Specific powers should be delegated ~o (a) the PliO concerned with MCH and family planningmiddot (b) the Directcr o the Program Office (c) the Regional Director and (d) the County Medica1 Oficecs The Ministry should invite suggestions from these officers and wOlk 01t a schedule of delegated powers
415 A tdgh priority in the matter of delegation of powers is to arm the Regiond Directors with sufficient administrative and financial authority to implement with expedition the health and family planning programs of the Ministmiddoty 1 thin the areas in their jurisdictions
E Integration of Family Planning wi th Haternal and Child Health Services
416 At present family planning services are being provided at 48 Goverrnent hospitals health centers and health offices by using the full shytime E taf cf these institutions and employing part-time (sessional) doctors nurse~ anI clerks where necessary At 29 of these institutions separate famil cl~nics are held on specified days in the weck some being doctor sessi(ms mel others supply sessions run hy nurses and clerks At the remaining 18 imtit1tions family planning services are combined with antenatal child healtL cr postnatal services The Family Planning Association runs 8 unishypurpoe f am ly planning centers which provide daily services and contribute a 11 t le less than half the total number of new acceptors per year
417 N assessment has b~en marie of the effect of integrated MOl and famil~ p~ nnning services an the recrl1i tment of acceptors nor were ~ data readily avallable for this purpose It may be observed however that in a situation of shortages of trained personnel for health services utilization of the existing health staff and facilitieR for family planning is inevitable parU cllLrl y in the interior where such shortages are more pronounced This underlines the need of evaluation of the integrated xai and family planning progtam for its impact on the number of acceptors Also a study needs to be made of che utilization of medical and pilramedical manpower so that it leads to bdter ~llocation of duties and optimUJl utilization of personnel
418 ile integration of faMily planning into Mcn services has certain advalltages as well as attendant risks The advantages are
a Lbe association of family planning with the care of mothers and children helps project a benevolent image of family planning as a program of family welfare This creates a
- 13 shy
1imate favorab~e to the acceptance of family planning aa lt p-)si tL1e il-Eare rreasure rather than a negative program cE limiting c~ildren
h t elps erlist ~r2tion tf doctars and nurses who as c -~ass enjo tft~ Y)er)et~ a~d confidf~nce of the communities i712~ Eerve
c ~ieD of contact with women
d luni-purposa clhlics for ~lCH and family planning services are onenient for motn~rs who would have to travel considerable (listances to the clinics
e hete is better utilizat1on of Acarce heAlth manpower
419 he limitatio$ of integrating family planning with MCH servicesI
are the posiOili ties of loss of focus on family planning as a high priori ty prograrr ald the diffusion of pol1sibility for its implementation These could tlow ve r he safegurded agaifls t by adopting the following measures
a 11e job descriptions of doctors and nurses should be rewritten 0 include the family planning function
b hE perf0rt1iai1ce of ctoltors and nurses should be judged as much )y tbeir inteceq t in planning ~vork as in maternal and ~hjld care and this should he lade known to them
c )octors and nurses involved in ~CH services should be given middot)rj entation and traIning in famj ly planning and their interest 3UEtained by refresher courses seminars meetings and supplies of literature
d Thl techrical (xpert~ in the Office of the Family Planninl Program should maintain liaison with and guide the field agencies in implementing the family plannin~ program For this purpose schedules shoul d be marle out for periodic field inspections
420 It is suggested that the working of half-a-dozen centers where family plbnnLng services have been integrated wi th MCH sessions should be studiei for ehe purpose of standardizing the methodology of delivery of servicl~ Such a study should include staff strength patient load recoril shykeepills 10middot of patents in the clinic timing and frequency of clinic sesaios ani convenience vf patients
F Voluntary Organizations
421 I i~ internrticri31 expedence that the birth control movement is pion aTC tt volunh[~ JilC S Qltl that hen the national governments step in wi tl cmbi ti 019 prjhns wi thin the sLate welfare system voluntary bodies ieh tteir limited ilsrluces restrict their service activities and shift the emplasi i 0 educedgt (f the community training research and contracepshytive Sf vic not 1l7gtilflblr in he official program or in areas not reached by it In nagni tude and expanse the of ficial program in Trinidad and Tobago has alrad~ orertak~n Ce 101umary program Increasingly it will become the domLnart tartner in the total national program while the voluntary agencies will cOltirlU1~ to receive financial support and encouragement to set up high standaeis If service and explore new areas thus acting as a stimulus and an additi_e tl the official program
G FrOB-ram Infomation
422 Thre is no concurrent evaluation or monitoring of the Program The daa or lq72 flowing in from the clinics month by month have r8Jllsined unprocss~d tn the Program Office The official Annual Report - 1971 Sums up th~ poition as fcllo~s
ITThe Research and Evaluation component continued to be the weakest in the Population Program Although a systen of evaluation had been built into the program the follow-up procedures for analyzing the data and for correcting inshyconsistencies are inadequate Requests were made to extend the staff to establish a more viable unit but by the end of the year no chllnges had been made
423 T1e recording and riporting jJrocedures were revised effective Januery 1972 and there has been a further change recently at the instance of t1e Evaluation Adviser Under the system now established the clinics are lequ Lreurod to maintain the following records
a Family Planning Clinic Case Card - New Cases This was introduced on January 1 1972 and has thirty-one entries giving age parity contraceptive listory pregnancies socio-economic background ource of family planning information and agency for notvat ion bull (Annex 2) The case card is made out in duplicate for each new acceptor and a copy sent to the Program Office
b Daily Regis ter This fs a ne~gt1 form recently introduced in replacement of the old regis ter and is preparen
- 15 shy
ie) ruplicate the original to be transmitted to the Program (fHce and the carbon copy to be retained in the clinic Th~ is a very 121zborute form requiring 36 entries to be aa~ for each Chse nel and old attending a session includin~ (ntries to cit L to contTaceptive supplies issued
AijCleX 3 T~13e fcnnG are required to be sent to the Program lffce in i7JO balches every month the first batch for the i IS fif~eeL days and the second for the remaining part of hE month The trtention is that the data appearing in the ~EZlic daily legis ter forms should be compiled in the Program Office and fed back to the clinics Although it is claimed that this new form has been pretested and is workable ex)erience alone will show whether the majority of clinic cL~rks are able to cope with it in a busy session
bull o now-Ho Card TIlis card is intended to keep track of ac ceptor--It has entries for name addresfI and month fcr which a visit is due for each year
bull Aphabe tical Index This is a card index of clients with aidresses
Each i)at en is given a simple clinic card on which the dates of further appo~utnli rc3 an~ indicated A special fonT[ has been devised for the reporting ot cases unler the Post-IartumPost-Abortal Education and Referral Program
424 J system of monitoring progrRm performance from month to month need to bE develQped as a high priori ty The problem is not so much reshycord ng mc transmission of data by the clinics but its aggregation and proclssi ng in the Program Office every month which at present takes a long time The Statistical Officer should have a statistical assistant to help him Ln I he taflk Monthly progress reports should be available to the Mini H t~ n H(llllth and A11 offt eerlil of the ProKrnm Office so that remedial ac tl m I lAY h(~ tuk~n n rll1u- WhOnh1f ~Hfl(AlJtlaTY
42 For the analysis of data and evaluation the Program office shouln haVE th(~ full-time services of a trained demographer
H Field Workers
42) Tie Program nemiddotis tne services of a cadre of field workers to enr)ll neii aceeptoTs follow up acceptors in their homes and revive the int 2remiddott of dropouts Such a category of workers could also be utilizerl for pr1fficting other health programs such as the VD campaign and the inmuni~ation program
47 As an experimental measure one field ~]orker may be assigned to a emi l~ of Hi 000 population This would mean 100 field workers in all
- 16 shy
Earh of the workers should preferably have harl a higher secondary education otherwLe 1gt junior secondalY education They should be married persons with middoti1ltt mot tl-an two or tlree children recruited from the locali ty in which they armiddot~ requlred to function Only persons who have the capaci ty to comnunl at~ and or6anl~e should c chosen A months ini tial orientation
slcu1d enable them to start functioning in the field though reshyfresher CO rSeS tvould be necesslt1ry in due course In Port-of-Spain married mer~ a1C women may be employed on a part-time basis
I Hanagement Study
428 A nanagement study of the Family Planning Program should include a sctu iny of the top m~nagement Atructure (Population Council - Office of the Fanil) PLanning Program - Principal Medical Officer for MCH and Family Planni Ig fetices) the field structure for the delivery of family planning servics (Re0ional Director - District Health Services) including the utilizlti(n if medical and paramedical personnel for adding the function of del ve y )f family planning services and the control and communication proCed1reF Lfnking the top management with the field structure
429 The management consultants may study the functioning of the Popul tio I Council and advise whether it adequately serves the purpose of givini po Licy direction to the Program and if not what changes in its compo itt m and operating procedures may be introduced without altering its bsic craracter as an advisory agency The consultants may suggest an alern at ve form of organizati)n and utilization of personnel which in thir p nion may be better adapted to the needs of the Program
430 Irrespective of whether the Population Council is maintained or it is replaced by an agency of a different character a formation like the Offic of be Family Planning Program would be necessary for the administrashytion i)f 1 he program a task for which i 1 appears inadequately equipped at preselt Its obvious requirements are in the areas of program monitoring and el7alnation program supervision communication and training The manag ememiddotlt consultants may study the structure and procedures of this form~ tio Gnd make suggestions with regard to the augmentation of professional and ~ upp)rt lng staffgt and modification of operating procedures
431 The linkage of the Office of the Family Planning Program with the Miniutry of Health (Central Office) and the District Health Services should be sudied In view of the policy of the Government to integrate MCH and faI11iLy rlallning services it should be examined whether the Principal Medi al Officer for Communi ty Heal th Services (MCH and Family Planning) should be agtpoj nt~d as the Chief of the Office of the Family Planning Program and an adTlilistrative officer of a suitable level inducted in that Office to assist him TIle implication of this suggestion is that the head of the Family PlanJling Program would control the District Health Services
- 17 shy
432 rf 1e management consultants should examine the delegation of adminshyistratiie Bld financial powers of the Ministry of Health to different levels of Progam aclrlirdstration viz bull PMO Program Office Regional Director and County ~djca~ Officers
l33 he system of 01 af Togram information from the clinlcs to the Pr()~ra1 O~fice and tOile processing and use of information in the latter office iholld )e studied
434 he working procedures at the integrated McP and family planning clinics shnuLl be studied This would involve a study of each stage which a clien tpcticmt has to go through from the point of entry to the point of exit after receiving advice service or supplies This study shoulci lead to star dartization of procedures and functions and evolution of -lork norms CognatE st tdies of the working procedures at uni-purpose family planning clinics and su~ply SEssions should also be undertaken An essential component of these ~ tad ~es would be to examine Nhich functions currently performed by docshytors lealh visitors nurses and midives respectively hav~ become so roushytinize ttl it they can he relegated (0 the next 10Her level
435 Reated to working procedures is the problem of job description of medcal 8nd parrunedical personnel involved in family planning from the centra i tc the field level This job description needs to be studied wi th a vie VIW8Id txaminiDg the uttlization of skills and allocation of time by the staff lcc(rd~ng to the functional prj ori ties
436 frV management consultants should study the workings of the curren slralgements fOJ family planning counselling under the Post-Partul11 Post-Abortal Education and Referral Program at the Port-of-Spain and San Fenaldo General Hospitals
437 SU1ect to the ItBrcement of the Gove1nment the management conshy8ultal ts ~hOLlld undertake a study of th requirement of field workers (home vinitcru) in tmtlUI of are nnd population cov(ra~e
ANNEX 1
Names of Persons Met
Ii Mr T C Taitt Pem1(H~nt 3~crtarY) Ministry of Health
2 Dr M n Henry Chitd Medical Officer Ministry of Health
Ellubeth Quam a Prindpal Medical Officer (1S)
4 Mr G Z Jaine ~ uJiector Population Council
5 Dr Norma Andrews Medical Officer Population Council
6 Mr Jc~n Coury~ Evaluation Adviser Population Council
7 Mr A Jriseph Principal Statistical Officer Population Council
8 Dr C 0 Colman Country Representative Pan American Health )rg ni~ation
9 Mr ranca Kippel Health Education Specialist Ministry of Iea th
10 (1 bullbullines Principal Nursing Officer Ministry of Health
11 Dr Mx won (formerlyHinistry of Health)
12 M3 late Carops Ex-Chairman of Population Council
--
4i 1_ middotIIlt F-ntCWclOotf_Y v OJ t tl
GOVIIlHMEIgt(I OF TINIOAD AND TOampAGQ - NNISTJY OF HIALftf AIJIE1 2NATIONAL FAMilY PLANNING PROGRAMME
F MIL Y PLANNING CUNIC CASE CARD - NEW CASES - NFPPl
li ~~___ 1 ________
~ ecll-U
-- --------------------- shy~) ~~middot~------------------~~~~~~---CIJ------ middot~ii--middot-middot----middot-middot---middot--------- shy
ltv Writt N_ 01(111________________
a ~4itiJtmiddotl_____ ilIIIltIoI~____~____~-__----- shybull ~4
fie l$ - JO tDql IIfIA- tr-JMimiddot _ iJ 1 Odoor o
14aorielaquol_ _~ 0 lio witIleo-La ~ 01 bull - OJ ( _01 1~ltgt1lh o bull- 0$
AacJcu 0 2 CIIriIWA 0 J Os 0
Yv~MONTH ltnollOf~nfIGHTI
Undu 1100U$ Utgtdn 5SCI Undu 11200 01 ~ 50 - 9949 amp100 - 1199 02UlOO - nn9E~ (
0)~ 10- $99 SiOO -- U9~ lOO -- U99 12400 - 1359)-------_-r----shy ~l)o SIS n600 - Hm1300 -- 019 OJ200 il~9 ~------ 99~ a 1)0 m Os1)00 -- l99 1400 -shy $4100 -- 1S999r--- shy
1500 donl S6000aad O399 - lt499I~- I 0lt
ltII
IJ -IC _~tltlioltgti lS
02 IaampJIIocI OJ 04 laM Os
w Oltwio I_-l(~u IrIaa U
h~~ ~Clubl 01 OJ
IS ~C-n 01 toSIitDI 02
Ji poundI on 01 IriIIIuy M ur 02 IV OJ
WU 10 pltIoII~ llaMtl 411 cIIiId 01 Ol it fIolto ~ do~ _14 rou IIlgtJo 1Ia1 ___~_ shy
40
It _ I 00 ~bull FPIiIJ 1
OJ 02 OJ 06
)0 III- iy wOWcf ~1
aMIIl Os
11 T 1gtlt ( h _______ 4)~
06
04 (MIbullbull middot bIrlI ~___~__~_ (-fIJI ~- -~-- (1HJ 49middot SJ
U 10k 01( 1__ raquo$-4
iU1) DOl F ToWotfOlnC DOl 001 or Do [IP 006 001 OIIgtu___Spltclty DOll Nltmo 010
U1Mo I orcpmiddot laquo55middot16
1lD 001 Foam Toblelf_ICim DOl Condom DOl CoomS~ 004 oe Oos WlttuJn 1J OIkr DSpody) 101~ ~Iu 006 Rhylhm 001 DOG OJO
no wI~lmm 4 cd
(I 0) 1110 01 Condor 03 (lorn bull l S~muoidIl 04 Faa TabioolfIIltr- Os RhyUlm 01 lnJrl tible O Advico 090 06
la slt 1)0 19 loti ~rltnlt) ([)sl or 1llOn) ____ --__ bullbully-J n SV - ~JcdS
v~ Cl NCI 0 30 OJI_O I Wr blJ1h 0 I ~ OJ 1 ~ (fOOd V 01 No 02 laquo 6) Cf4
WIiI 1 172
004 001
j D middotmiddot middot
1 ~
r
~
bull I
bullI I I
r c i
ANNEX 3 Pagemiddot 1 of 5
0 raquo rshy -lt l)J ~ 111 t G) 5 shy (J) ~ -
fT1u
i
MINISTTY OF Ho1TH
NTIONl F~ILY LNNING PR-GRbullbullM-tE
~~5tructions to C11nic ClerKa
How to co~ploto the Daily Rogister
~~ ~~v1sd Daily Rosi8ter replnc~D tho one which is now in use tb$ Monthly PC~ri rOt~ arti tho 01( Ci() Dod PollJ j f m It is a pre-coded form and 1411 cl~1p Jd tl a1I6iniul-mIHvn Oel Clinic nctivi~y
110 )rm rollt biJ coupJot)d lrl cupLtcoto using a o(roon shoot Tho top aheot or oriinai ~ust bl) 6(Ult to tho CQgt1tral O[[lCO and tho carbon copy retained in the Gliaic rilo dll the for6a that ar uD~d betwoen the 1st 4nd the 15th of the oIIollth aut bo subClittud tocho office 35 Lnc blttch Those oomp1cted betwoon tho 16th _lid tqemc of tho month must bo ~cnt in a secJnll batch
P lOvLior hns boon Illllde for 25 clients on cZlch forlll new forlll must b IIlied f r poundh 50[810n2 whothur or not ono or lIIore session are hoIdiit the clinic on he sarne day
I th ro alO more htl 25 clionta 1n attondnnco at tho session the additi shyOhAl m~bOl of clionts 10 clients nu~ber 26 27 etc sh0u1l be ontered on the next Imiddotrlll ~i ttout a1tpoundring the numbtlrs in the cvlumn hond Series
51 ppOfil th~ number of aUcnts lQr that session ws 5 this would mean thllt two rJlS ~ lst be 6ubllIitt~dl the first filled uF 1 tltgt 25 And the laquoIncond 1 to 10 Th~ cal bon ofies should bo st~plod togother at thu t0P l~rt h4nd corner of the torm ard ktpt in the Clinic filo lou IIlU6t stapl~ the originftls in the 8~~ monnshyer for lIub~ssion to the ofticl
ie h~ ll idontiflctior- (cc 1 - )
0 lot Ji 9 anythin~ hGro poundhia is int(mdClc for tha computer code
2 ~~pound~ - Print clOflrly tho name of your Clinic
C1Lic Huml or - (cc 4 - 8) Evar1 Clinic Numbor has 5 digits Virite each dig t il a t$purate box
It Pai~_thllsectgdllion (00 lt) -1 1) - Dl monll 10M
lw) bolte IlrO proY140d fetr olAoh pr 01 thQ dISh Enter tho dA) ldns a R
d16ih
emiddot5middot (0 11 I for 115t ( 0 21 for 5th etc Treat month the am pay
e ~ 10 ~ I for I-hrch 0 [2] for September Tho y~nr must be (into ad
I Z I ~ I I 71 q etc
Take as in IixulIple tho dOlte 3rd tllrch 1973 7~ie must bo written
[0131 LSLDI[7l3JDny Month Ye~r
5middot 1~J $~~ - Irom ~-------- To --------shytntol hOI II the time the Clinic 111118 in SW5sion emiddot8middot
(i) 11011 500 lm To 1200 non
(11) Frclt 100 pm To 400 pm
(iii ) IX-OG OO pllI To 6~00 pm
f
2
ADEJ ) Paae ) of S
6 Eov
_ 1hA 1gtIpoundC iIIUlt be nu~o7Ifd tler1ally 1 throurh n lU tbey Are Wled In ~1l8ellJ IInel 1301 tlU 1 Orcl 1 Wled tor a o5038ioll - -I 2 tonY tho _boul~ b I1WJbtl 1 and 2
hlrlll are 25 linos OIl the fOnl Ilnd thoae muet be UBtleS for 25 clients 9 one ior bullbull 01 I ini
ot ~h lc II ol1cM lOlivpound til e linic before soeinc DurOI or doc tor ilnc ii hox rristrltltion nUlJbet had alrearll been recorded on the Dai 1y Roiuter then n line ~hollld be drawn through that entry an1 the eliort nust not 06 includttd in tho totals tor that 0eDion
1lw Ileifitration Num)~r of cueh client must be IiIritten IS n 5-dlrlt oode ClhnC IH11IlElr 315 1IIU8 tborotore be enterod 18J010117]5]
~ Clt ZOt
Coda 1 Codo
10 ~tl c 2t j co 21)
~w elSe - Coda 1 0) d CltaEl - Code 2 Revislt Code 3
Only pound1 01 theBe coiles may be usod
11 prol-O~ ~Eil~1 (cc 22)
If ma climt was L drop-out IIho haoS returned now to the Clinio tor tho first no linmiddot bullwin lt1ro1eo o t he or she should be given CCe 1 It this do 5 II It nprlly leu this colWlln blank
u Hothod middothisllill loe 23)
NOh til t otly ~ Cod 16 tp he ontered in 2lpound of the columna oven thOUGh 10 co11lllJlB 10 provided on the torm The Codes llrol-
Oral Contraceptive Code 0 1 U D Code 1 Condom plUD Codo Z Condor (only) Code 3 Foum tAblets cream Code it DitphrClGJII Code 5 Rhythm Cde 6 Injectible Code 7 Advice Code 8 Other Code 9
It for middotDo-le 1 client rlllll ji yen cclldorls ord foam or creall Iou Qust entor Coole i (condom plulJ) in the appropri~te column This Quat be the only lIotmiddot) tarcie If an in the cnse of a tlnle clinic I the client is Bup)lieu lith COIlOrW only you rmot entEr CorlQ 3 (cpndolll) Do not use a ticII ~ tho (odo Nwber
It is CUi tomary fur 11 cliont 110 is beine put on the oral contraceptive for the first tiT1o and even on other occasionn be issued condoms and 11 crelle or foam a Ilell rI3 a pgtcket of pilla In such Cllses when the piDQ Ilre Ilctually iouou you tlust record Orll (Co~e 0) 08 tho onll metbod ilo othor ntry sll0uld ho nnrlo
Uovever n SJC~ canas vucru condoms and fOHa ~rc eiven but no pilJa (even thoJRh _t _n the intention to issue pills nt the noxt vioit) than the Mothol Th5 ifli t ohoulcl be recorded uo Condor Plus (Code 2)
13 Seen Bybullbullbullbullbull
~rot S-1 SO l
Doctor (Dr) - Code 1 j Nurse (Nul ) - Code 2
Clark (Olk-) - Code If tho Clhnt is vcen hy both tho llootor tlnd the Nurse enter Code 1 t Doctor It 6~61l by the Nurso only arite Code 2 Cod bullbull Cerk is l)llnt for FA Cllnica Clerks in tho Government Cli1t hiwo Llttoll istructed not to i56uo supplios on their own volition
14 fl221~
lhio S~tiCl of -Ie fvrtl t~ke 16 (llrci coluMna (cc 25-+0) nnd 10 tho only part at th iOIQ in llich iore thAn one cod is Zlccoptl1blo Tho purpoco of the )ecton is to 0 able to arrive nt the Cjunntity of 6tock dilltlitJutshyed YOI IIlUdt writo in the CllllOjH-iata colulna the nUllbJr of Il1ch 4rtic1o i~JSu~d ~lo e ha I Oral Contrcilpti vea are aub-di vi dod into types ae_ 3 PIllCKC 9 0 Elynnn LlUot be entered Codo in card column 25
If tor eXllrplc t l cliunt is iosued wi th packots of Zucynon nnd aJ(1 ~ivn 1 conuotll (8inoloo) you ouot enter in oard column 25 and 11 It
cnrd col~8 )2 and J (io 1 in card colucn 2 nnd 2 1n card coluun 33) Nota C)lldoIlU ale to b(t ruoordod individually not os packots of throo) Should n ne LlondoClo be isoued thil3 is to be rc-Qed as 09
If It clint 6 t~ot isoued Blly lIupplies thon you must writo Codo 1 in CQllAlilD 41
It Q eli nt isite the clinic to check on her LUD or her Diaphra~t IUId ro DI W 6 ppl ills nre ispounducd then Code 1 1s wri t ten in column 40
In the FA clinios here a variety ot orll contraceptiveo in orer~l tho elerll wilmiddot~ bJ provided with a specill code shoot The idontifyin coo will b wiittn in Column 29 nnd the nUlber of packets iosued in colwm )0
lralaer-In Code 1 lrllllsie r~ut Coda 2 leIllPQrArr Trnnsfer-In Codo gt
In the cao of n 2ratl8fcr-In I you lUot n160 cOrlpleto coluons 42-51
In the cllU J of A ~~emporary TranGfor-1n (an individual who i8 only v1citing fur clinic tor some epecial trcatcont hna who will bo rdnlnin
~middot(II~~~fO~l~SIl~I3~nn~~~h~rO~nh~1~~190~~nll 2-46 and ler rei IItrntion numbu in colullnll41-51
It the oli( nt i iNt a CrllnoforwIu - Out or loClporu1 tMn loave oolumn 1 blank
16 lr4nst(gtr-tl2~~morrry TilJnder-In (co 42-51) Forl1ltl CUn E1~ (cc 112-46)
hen you rei iatlr L irllsfcrln or Il TJlporary Trnnsfer-In you IIIUBt write I ere the five-digit clinio nucbor of the Clinic iraQ which tho ltlient Me (uIlO
2mer ]letr ~2n ~ (cc 47-51)
frlta fllao Clo r-~itrlltion Nuc~Er ot the client in the Former Clinic (i c bullbull th 1 Sis rnmiddotion ~UlIlh()r which the client carrics 1n the tormor clinio) bull
It tho Forrltl Ho( ist rntion Number iIJ not readily wnilnble you tluct oocpluto thtl epcciol [orlll Transfer-In Not Identifiod Dy Forrlcr RCGi(trn~ t10n Nwlbvr Or ~ flt)rCl is to be cOlplctcd for och cnso nnd th forlJO Ilubmi tted to thu )opllntion Prorrnnme Of fice tOGether with tho Dily Ro~iBtors lhwev~r should the clork leuTI of tho clint B FormlI Uocintra tion lUlllb r )0[(10 Cubmi ttinft the D1ily IOCI otro t hen the nUQbcr shoulo bo -ri ton in colucns 47-51 lna the special foro should lJo deotroyotl
l7 bullbullbullbullbull
r lt bull bull
ADXI ) Pap S ot S
11 UD LV~ (cc 525)
It tb( cliont io ~ivQn An IUD tor the firot tl~o then you should Sri to Codo 1 Inuort ill colurJI 52
It tho olimiddotsnt ia rvinGgtrtltld i th An I UD bullbull tben wse Coda 2 RelnDltlrt shyin (01Uil11 52
It the clLmt is ~tte~~dint chnic beruse her IUD CflClQ out by Haol (cxpll Iion i ~hcn fir te todo ~- UIlllrli1 53~
If c-ltr IU fj IIIS reov in -ne cllnic by tho doctor or nurso t~on vlritI Codec in column 5
II the eli nt otends eiLlie tld explin[l th(lt she rccovcd the IUD tlllleel nen write Coda H in Colwlm 53
It the IUD jr still within the uterus nd the WOIraquoI1 1 11rc6llJlnt thon lIrite 1gt40 4 in Column 53
lZ np h5t (ce 54) It 0 Pull 5mor ie t~ken durin thi visit tben Codo 1 ehould be ampDtere4 in ColWlln 54 Should he c110nt lltt rQ(uircd to rttturn to clin1c for a rogtol1t Pnl) t06t then CoLe 2 llhould bo middotwrittcn in column 54
It no Pllp Scou io taken tde visit Itove colUQn 54 blank
Iraferti1lli (CQ 55)
Ii the e liett io nl1 infortili tr eaoe use Cor1o Ill in colUQn 55
If tbia 1000 not tlpl lonve column 55 blonk
20 Totaltll
CO~1ploete the [)ldegO 1gty puti YI tne totals betweon the double lines nt tu b()ttctl Carrj colUlllnc 20 21 nd gt4 Must hlve tho Bnoe JllIIber and thiG Would coreslonc to the numocr ir attencbnco
Writ$ th to1ul nUlllior of Drop-Outs returned (c022)
Urito 41eo tb totnls fOJ each card column 0 to 9 under tho h(adinu Method thiB Vioit Show tho tote L fgtr OlCl type of contraceptive issued (cc 25-40)
1)0 Dot wrLte 1111 totll lUl(Ier Card Columns 15-19 29 41-51
21 COPmllh bull ~lt h~t~ Monthly ROilort
OQ thG DaLl oCator forlll thnt ccrrOspOldB to tho 1(8t 1$06610n lt 0
oth yo Olllt (vwlgtleto the items nt the botto of the [orampl This is tour ontll~1 n(olt nnd includcD tho totll lumber of sesions Ilntl tho total Iluolcr ( r crop-outs durinr the Qonth
An tiUlsilt n drir which n doctor liB in nttcndnncc is a doctor sOfll~1on and shoulc 00 re(liGtcnd in coltns 56-57 All other sessions 1116 conlliid~recl supply stllciona and thtlY 1110 rocordod in columns 58-59
the total Ilum)nl Jf drop-outo ld the drop-outs by method durinc the onth nre 10 bu oltorou in the inrlicllted boxes
72 Chad Your ~
Milke I ura th t all thE fijul4gtu rre c101r -tNever writo our nutlUQrS 50 InrjEl that they oxtend out of tho
ap~rotr1ato ~ox
Cheek to BoJa tht 1111 numuors 1110 in tho correct boxes -- CJslHloially when Writi1 the totlB
Mllxe Cirtc O thmiddott t1e infoT1I1ntion i6 clear on the corbon COllY before sep rmiddotinr the sheets
Jitn the Fomiddotl lien tly sien YOUl nr me 1t the bot tOil right hnnd corner btl forc subol ttinG it Keep tle CL rb n copy for your rocordn
i
-l ________~~---------~
I _1
Adminiatr-atlve SKVieu
P inba ~~~l1cal lrlnbin~~eltltcal -1 te~ra t~~rvicc (lnatittloaa)
--1- - shy -1------------_-L_ l-r-aJiil- shy _-L_tet1lal d
PlIinm1tJ8 atdUon DetalMid H8Il1tb ~ ________bull Care
-----~ Office of i
the FlIily _IPlill3 roarshy
1- - - -------RegiatUll urnr
ltIi 1 Drelttor Rcgicaat Director Souta Tabqo tacallortb ~ counu gt____ ~ (4 ouottet)
Off1ce of the Res10nal Diractoc L
r----- _L_ -- shy i I bull IREgional Ipitl I
District IIttaltb I bull Othn RelOl ond Hcpital CenteIntt itlt j In 1__ _shy-~- ---- -_j
J r Ii~lth
C~nlef
L
I Ihnlth lie I th Offlcu (1ft lc~
Coullty 1I0p1ta1
Henlth tentet
I

(vi t) 1ne orgai c Y1 anlti j~lrcgemeu of the Program should be reviewed cmjoLntlyamly pcanning expet and management consultants
r L the fr]lcwing topics
a) thc 1lt0 V 71rmiddotlCi f Cn1t1t structure comprising the ~inis ill Hnal th ~he Ppulation Council and the Prc~r~1 Office ~te feRsibility of alternative models of inatit~~iacnt ~
(b) the s taft re(luirements as well as operating procedures of the Program Office
(c) the ltitin n t[iv and financial powers exercisable by Program uthori ties at different levels in relation to dgtE le31H of lesponsibili ty
(ci) trc JlU l1 of coordination and supervision of
(e) the staffing and working procedures of integrated MCH and family ptanling clinics including family planning counselling 8eVmiddot Ck ~UITli s Rilet recording of data As a part of the study ~ Ulti~cti(ns pe~iolmed by each category of staff - shyme6ic~1 rn ijed lerical -- should be examined to idemi whimiddot rune dons can appropriately be relegated to che next tower level so as to optimize the use of available ma1pow~r
(f) the system of flow of program information from the field and its processing and utilization in the Program Office
(g) he ost-ParttmPo13-Abortal Education and Referral Program and
(h) the requirement of field workers for conununity education creation oE ltiemand for family planning services and conshytinuous c0ntGci with acceptors (The type of functionary needed content and duration of training and the norms of work should be suggested)
I INTRODUCTtflN
101 0-1 behalf of t~ H~1k ~middotmiddotr R N Madhok (Consultant) visited Trini12d ad Toblg0~ middotl iL bullbull ~)3 0 review the administration and mal1agme)t )f thlt hsd j 11]) PVnning Program During his stay in Trinj dad 1- MadhJk ( iilh eprefEntatives of the Ministry of Health and the Topu ation C01Jii1 fuJI li5e appears in Annex 1)
102 ~pecifgtUy ~~C iVlsdhokcevievled the following aspects of the progam
a he future role of the Population Council -- whether it should )euro an advisory or all (~ecutive body its administration staffing and statutcry pmrer under a changed set up and the consequent changes required in theliinistry of Health for the implementation of the prc)gram
~ J the extent of (l~i-5ting (Jpcfntralization of administration of health and frunily planning services and its efficacy
c the desirabiLty of integrating family planning with maternal and child hcaLh services in the light of experience of inteshygrated i~lirJ(
d the efficie~ Cf~ll edsirg system of the flow of program information ac ~Hl red charges and
specific aspects of manager-lent and manpower utilization on which the management finn should concentrate during its study
103 The following report contains broad suggestions on changes rE qui ed in the existtYg structUrEgt
II ORGamp~IZATION OF THE NATIONAL F~~LY PLANNING PROGRAM
201 The administration of the National Family Planning Program is the rl~sp(jnsibility of the Ministry of Health In 1967 when family planning was adopted as an official policy the Health Minister at that time proposed the stallishment of a Population Council to advise the Minister on the organizashy1ion of a natiorlal prorrun 1i(h lIIotld coordinate all family planning effort n tle country Tlle Cabtn2t c~ciCled that
A Population Council of Trinidad and Tobago should be instituted for the purpose of giving overall direction to the Family Planning Program in Trinidad and Tobago with a view among other things to coordinating all fanily activi ties in the country II
- 2 shy
202 In pursuance of t l= foregoiny decision the following terms of refer nce were framed for the Po1)ulation Council
10 i~vll ditcoction to a Family Planning Program fo Y ltdd cHl T0bagn d th Ii view among other things to eo ~ ~c n lfllonrdnr activities in the
203 A PTOlllH~ f(cibor nf ttl rredical profession was appointed as Chailman llei the lill~1L y h2 jiamily Progran Ministry of Health as the Secrltar r (r th C~-ur~ ihe membership of the council comprised officials of tle t-instry of He3ltii and other departments representatives of the volultary agencies operating family planning services and leaders of opinion the present Chairman of the Council is an eminent gynecologist in privmiddotte practice and a former Minister of Health the members are as foIl 08
1- Chief Medicnl Officer MOR -l Spcclliflt ~middotjJ3C Officei- General Hospital
3 A rEpr~senative of the Ministry of Planning and Developneut
4 A represehtacive of the Central Statistical Office 5 Public Tidaions Officer Prime Ministers Office 6 ~ PrilLj~d t1lt dq Officer NOH 1 ~e( CL bull ~clmiddot ~~t)pulati on Program H Chid ~ea~h Educatoi ~lOH
9 A repres~rltatiVE of the Catholic Marriaie Advisory Council
10 amp 11 Re~)resentatives of che Family Planning Association 12 6 13 M~mbers or the Publi~
14 Diector Family Planning Program MOH - Secretary
Olj The Population CQtJrdJ hal three roles (a) policymaking ll) I rogralil formulation and evaitllt1()l and (c) providing general direction fllr program implementation Its composition is designed to ensure (a) intershydapamiddottmental coordination withill the (overnment (b) coordination between the ( Ole-nment program and the activi ties of voluntary agencies and (c) rapport vith pblic opinion
05 The Population Council is assisted in the task of program formushyIation by a numbe of committees ~thich are so constituted as to draw upon Ihe ex lertse avalIahI wi tlin the Government as well as outside Pre-eminent arnorg heseuro commictees s lhE lati()nal tH Program fnLMulation committee ihi(h technically speakirg is not a committee of the Council but a commitshytee of the MOH It inter-meshes with the Council since it is the policy of the Government to integrate family planning services with MCH services delivered through the network or health centersoffices of the Ministry of Health This committee is headed by the Principal Medical Officer of the MOH in dnrge oE Integrateci 2~edicil Care now restyled as Community Services
- 3 shy
which COlT bull Se 11CH anii IIgt sxvl(s I1H~ other committees are Community Educaior and Publidty Cvrm] ttec Research and Evaluation Committee Family
~du aton Comrnirii ~~e(i] CCimittee and inance Committee
OS i~ n1eptUd~ i p Ni ~runi t 1 an advisory body and as such itus 10 execl1lt)ltjmiddot n p-actice the Office of the Family Planning Prog) am e tabisLecl wirgtmiddotcn tilt2 middotlnitry of Health functions not only as the ecr ~tc dat of lIC )hiCJl but also as the instrument for carrying out lis lirEctvls Furtiie ch GOtdcCU has concerned itself nomiddott merely with broal i~ SUIS f10Hc out also vL detailed implementation The majority of t le r emmiddoters of rhe Council are in favor of Umi ting the Councils role to tile givlng of broad direction to the Program
20i The Office of thl~ Fitli1y Planning PrO~rall1 is comprised as follows
Dlrcct0r (Incant) Medilal OfHceuror (Famtly Planning) Nm-~If Offieer St~tistical afficer Health Educator 2 lield Workers (for follow up)
(OIlE positor vacant)
8CCiHWlcnt 2 clexks 2 typists 1 driver 2 proj ctionis 15 and 1 messenger
T- ~ g af f of the Office of the Famly Planning Program is under the discipline of thttinistry of Health since the Population Council is nei ther a departshymfntal unit nor a separate legal entity with its own fund
2 OB The places of )nrm1 atton Council and the Office of the Family p ~anr ins Program wi thi n the Minis try of Health as conceived originally by tile Government may be seen in the abbreviated version of the chart appearing hI different official documents and reproduced at the end of the report
~ 09 In April i973 at the time of the consultants visit there was In aCIDc)sphere of uncertainty about the administration of the family planning l)rogram as a result of changes in some of the top positions As a result of t c~binet reshuffle the portfolio of Health had changed hands The Permanent euroctet lry who is the princ~al ad~liser to the Minister was new as lras the r-i c al Yedic1l Officer h charge of Commurity Health Services (Mel[ and Pam ly Pl1nnhg) The Dtnct0 of family Planning who was managing the Office of middothe Family Planning Program and also serving as the Secretary of the PoshypUlition Council had reCiTed in March 1973 and a successor had not yet been named Meanwhile the Medical Officer for Family Planning (a part-time employee) was carrying out the functions of the Director in addition to her OWT Wi thin the Population Council the advisory agency for policy-making
and ccord~n8tionJ there was a groHinr feeling among the members that the ouncl1 510t1d shed thE respOJ1sibili ty for implementing the program a funeL on j ch nad heuroe added on to its advisory role with the passage of time
iO the 1 ~lp~1 the lines 0 responsibili cy were not clcay (e ned and Li1 refioal system was not fully functioning The post of Re ior 3 Director crth VIas vacant The policy seems to be to strengthen the 1St tu ion of Pt()1ic Flealth Office as an 3ency for the supervi-middot sion)pound ne district sflVices (health centers health offices and school servi ces ~l thin the ccnmty
II I PRES EN STATUS OF THE PROGRAM
301 ~he adl1linistrt~ivE changes narrated in para 209 have come about at fl tin e IJhen the P1ogram has entered a phase of declining performance as is 11 Jpal en from th colloHing figures taken from a report submitted to the Populaton Council
YrUL 10C7 ~j8 1969 1970 1971 1972
--- -- ------------~~ --~ - shy----shy
Ne Acceptors 3696 2731 16207 9997 9898
(End of October)
7560
Slur~e Family PlAnnto Program Report (no date)----AsII1Ulilg that th6 ttlrollmant of new acceptors during November-December 1972 prclrd at the 8ame rate as during the ten~onth period January-October
- 9i2the total enrollmslt in 1972 would be lebullbull than 8500
3(12 lhe total number of leW i-iCCeptors for 1971 shown in the foregoing tal11e 1s at variance with the following data from the 1971 Allnual Report
- 5 shy
~ev C~~ Contraceptive Method and Agency
nm Other Advice Total New Cases
Aeny
GovrrmenC ProEllil ___~zZ(lt1____ 97____2Lbull499___~528~___4i_750~_
Farr Uy Planning Association 2814 315 607 76
Catholic MarriaAdis1ry COLnc_H____
ge
74 88 162
otal 31[10 692 8724
_--__------------------shySOlrce Natio
1973 nal p
Fam29
ily Planning Program 1971 Annual Report April
NevmiddotrneJl~ss) the declining trend in annual performance after 1969 is manifest ana conpaes unsatisfactodly to the following targets set for the Program
Targets for Contraceptive Users - 1968-72
New Accep tots Old Cases Total
1968 20noO 20 000 lO noo
1969 20000 40 000 60000
1970 20000 60000 80000
1971 20000 80000 100000
-----__shySource National Family Planning Program
p i9
------------------------------------
- F shy
3JJ3 Ttl flient recrvitTrent has fallen off since 1969 in spite of a signif Icar t xpansinn ir the number of Government health facilities providing family paarin~ services FrCli1 7Hr to year Starting from scratch the number oE GovE(nment health irlstitl1tions delivering family planning services in isollL(Od ~ily pltJfAill~I ~J in c)lchiratinn ~7ith MCa services has lWW risEn t 4 lhis ie --tdt)p to t cii1ics organized by the Family Plannin Asce1ation bull U2 by tile Catholic Marriage Advisory Council which offers the ~h)lthm meti1middot1 nT
304 1i ciecli ne d~ d re11~m2nt of new acceptors coincidentally w-Lth th~ eXlsioH uf s-crLce facilities needs to be studied to identify the factors responsible for it eg the quality of services offered the strategy of commmic at~on and motivation and management and supervision One obvious gap is he abgtence of an agercy for promotion and extension of demand for family lal 111 If services -gt tLe field reliance being placed mainly on clinic counseUn H1d generaUzmiddotd mass media publicity The need for a field promoshytional agelcy is underscored by the dropout rate In 11 draft paper prepared by the Hed_cal Offic(1r for FIrnilv Planning it is stated that by the end of 1972 t ile Heuroe approxiclt ji rHJC cun~ent users of contraceptive methods and 33 per ert dropouts
305 rht~ program is cot merely clinic-centered but also female-oriented Recent Iy mellsages aimed at m11es and stressing joint male-female responsibishyIi ty l gtT j ecillc CImt-J 1 i~gtVt~ b~~in )7cn 1n0 the cOTul1mication activity sUf1 tv) c nts Em he 2iucaccw i milc8 and che distribution of condoms to them illVC he ~n or n~d iD r GJvefl1nenC s(~ctor The Family Planning Association has a130E~k11 the irti U3 1V~ to reis ter males ln industrial employment Tllese are steps in the ri)n dtrect1ongt but the size of the problem indicates the n~ ed OI a concerted effort en a much large r scale
306 Tre Program relies largely on the use of oral contraceptives as shown in the following table
Oral Other Advice Contraceptlves IUDs Methods Only Totals ( 100)
19)9 76 20 16207 ( 100)
1970 316 63 9997 ( 100)
1971 50n 4n 365 79 8724 (100)
Family Planning Association unpublished report
----
- 7 -
Althougr amJnp the neH acceptors in 1971 the users of oral pills were only 509 ~mon~ the old cases the figure was 119 The percentage of IUD users has remiined stagnant at an insignificant level this may be partly due to consume prefErence and pctrtly outng to lack of trained staff to undertake IlTD i1srti l7U There h hOHever a visible shi ft towards the uSe of othe~ ilettods (npchani81 and chemical) attributable to a scare about the side efects nf oral connaceptives Among these conventional methods the condom s 11 os popular
307 J t )resent fami ly planning services have been extended to 48 out of 106 hellth centersoffices run by the Government and the objective is to C)Vel t1e remaining health centersoffices within a short span of time so that adice and facilities for the practice of family planning are conshyvenient Ly wa nable to the people in all parts of the country By ann large sepanit e fITti ly planning eli nics are held on specified days as an addition to norrral lealth work Besides doctor sessions at the clinics supply sessions are rur by health visitors and nllrses assisted by clerks The nurses are authorjzed tc issue oral contraceptives for a period not exceeding three months ani the acceptor is required to attend a doctor session for advice during thi jnterval In 1971 the numbers of full-timepart-time staff in Gov~rtmnf centers renderinp family planning services were
Full-time Part-time
1elical Officers 14 8
NUseMidwives 35 19
Cl~rks 3 17
Now tile low~rnment -gtbjective is to integrate family planning services into MOl services and use the same staff being used for the delivery of both types of erlices at multi-purpose sessions However so far only 1A centers have interated family planntng with Men or gpoundmeral hpalth care sessions
3011 The Family Planning Association has eight unf-purpose centers where famil) pLmring services are available ftve days a week The Association employs tilrEe full-time and ttJO part-time doctors a complement of 14 nurSeS (who llave been trained to do pelvic examinations) and 11 other clinic staff membels The Association also has a number of voluntary workers in the clinics The CithoUt Marriage Advisory Council has three clinics but their contri shybution in terms of enrallment of acceptors is not signiflcant
3)9 A Post-PartumPost-ALortal Program was started in 1969 It is state I tlat about 14 percent of the patients reached attend a family planning clini~ 1iTj thin six weeks of the interview in the wards IhiR is qui te a low figur In 1970 when a system of home visits was tried under the Family Planning Aide Project in 7 clinics the rate of acceptance doubled in three clinils rose by 50 percent in two clinics and increased by 24 percent in one clini (No change was noticeable in the seventh clinic) No decision has been Inad~ tmiddot) continue extend or modify this Project
A Po~ulaton Council ~-----------
401 he fu~ura ro~ Lh~ ~~~01ati0n Council has to be considered in theli1 A the tasK t~ lL ahead of the ~ational Family Planning Program At pesent tile officil~r(QSrJ1Tl is prirnarily concentrating on two objectives (a) tIlE excpound1sinrt of fmd plannin~ services to tie remaining 58 health centen cLJs as rapi(ily as possible and (b) the integration of family planniT g VI tr MCH services Thus thG administration of family planning serviCHJ will be merged into and become part of the Community Health Services Since t is ()rganizationally undesirable to disturb unity of command a separa1e elteecutive agency for the administration of family planning services is preempted within the existing policy framework An executive role for thp Pcnulc tinn Council is there fore ruled out on this consideration
402 If the Population Council is to function as an advisory body at the p()Lic~ aId progra1l pLilnni-l level snd not to concern itself with the minutile If program execution there wonld be no advantage in giving it a statutory stltuS But if it were the policy of the Government to set up a verticll )middotro~ram for family planning ii th a field organization separate and distir~tOroll the HeaHh administration it would be quite appropriate to establish an autonOiTiOUS statut()y a~fgtny ntside the departmental setup of the MinisiY of Health d~b a budi~t md staff of its own commensurate vith the rE spo lsi hi Ii ty to be rEs j Freed from the usual departmental conshystrailts ~n the matters Cif sp(ndlng a1d hiring and firing of personnel such an aglncy c(uld move faster than a heavy-footed departmental formation wi thin a Mins trl bull Hovever a hody of this eharacter would need to be cas t in a cliffe ent m(ld than the present Population Council The shape that it would take lrould be more like a Board of Management with a full-time Chairman or Execuive Director and with more functional expertise than representational charater But an advisory council with an autonomous status and no responsishybilit f( r lrogrrun eXIGulion iould be a source of friction
403 r~e existence of the Population Council as an organ of policy advici has certain advantages Firstly it is a forum for developing a national poLicy in which officials and non-officials participate Secondly it pr )vi bulles a focus to ti1e official program vhich it otherwise may tend to lose as ~ontraceptive services are merged into the general health services Thirc lymiddot- and this is important -- the Ministry has extra-departmental advice availabL to it~ but the Ministers constitutional responsibility for the condl ct )f the national progl~lt~ le1lains unimpaired
404 ls an advisory Q(dy the Population Council should be more broanshybase( than it is at present For instance it should include representatives of tile organizations of employers and vorkers associations of the medical nursngmct teaching professions and organizations for womens welfare The Counil should also haye a social scientis t on it On the official side the
- 9 -
Permane It Secetary and the P1O (fen and FP) should be brought into the Council he inclusion of the Permenent Secretary would open a channel of communi~aton with the MOR ae the highest policy level next to the Minister and would (ontribute administrative expertise to the deliberations of the Cou1ci1 ~m f icili tali 5 (pleuenrti)D of th~ recommendations of the Council within the -rni and in OUltL depa-cments The inclusions of the PMO (MCH and FP) wOlld el) emphasi ~2 hs responsibi lity toward the family planninR program Some officrs of the HOH (eg Chief Health Educator Principal Nursin~ Office e) may 111 ea~e to be members though they may attend as requirE d nmiddot the agenda before the Council A representative of the Ministry of Fin nee stQuId be inc~uded in the Population Council This would make for a lettr appreciation of the needs of the Program in that Ministry and fadIi ate fj nancial sanct ions
B A~tatutory Council
40S In the foregotng Pgraphs the view has been expressed that within th edsting policy framework an advisory Population Council would be more tli)prcpriate than a COlincil wi th executive functions and powers that an advisory rOUlcil would not gain by having a statutory status and that if a statl1tory body 5s to be set up in lieu of the existing Council it would need tC b structured more Iiice a Board of Management than a council wi th a repre13entttional charact~( n the latter event the statutory council should have fu 1- time Executive Chairman or failing that an Executive Director functj oni1g undel- a Chairman trno can devote considerable time to the business of tlw COlncil
406 T1e Statutory Council should have its own budget with full operashytiona pOlo1ers It should have the authority to appoint its own staff and regulLte their conditions of service If it is constitutionally possible the Couner1 shollld be outside the jurisdiction of the Public Service Commission in pesornel matters
407 As an instrument of Government the Council should be subject to such ~eUfral or specific directives that the Ministry of Health may issue to it frcffi ime to time This should be written into the statute under which the Cmntil is set UD
408 The composition of the Council ould depend on the functions assig1ed to it It is suggested that the Council should not concern itself wl th the delivery of cliric selVices in the field The Ministry of Health may (ont nue to administer rampmily planning services at Government hospitals health cmters and health offices and the voluntary agencies should run thei] OWl ~rogram The following functions may be handled by the Council
- to shy
s rrogram plannin and target-setting
b proram monitoring and evalllation
c wiL of d 1ci(JTIdnCf by inspections
d Qrg8lizatim 0 es and marketing of contraceptive J~1J-s BLl (iV es at subs idi zed rates through es tablished 1 2 d(~ channel
e information mass media communication and audiovisual ublicity in the field
f prorrotion of famil~r plannIng acceptance through face-to-face cotlmunication by poundi eld workers in domiciliary visi ts
g trIining of personnel
II pr )motion of -esearch enJ
i financial support to voluntary agencies providing family planning services
409 n Statutory CCii1cil may corsi5t or an eminent non-official vith a comri tm ~~1t towacds foJlily plailninf nd the fol1owin~ members
I ~ bull Pfrmanent Secretary ltl-tIlH
Chief Hedical Officer HOH
i Principal ~ecHcal Office ~mH
d Pilhlic RellltionB OfJte(middotmiddot Prtm~ Ministere Office
A represen ta ti V~1 of the Ministry of Education
f ~ representative of the Ministry of Finance
g A representa~ive of the FPA
h A representative ot the C1AC
i H social scientist fcum tle University of the ~Jest Indies
j Three non-officials with experience in management and administration and the
k Director of the Family Planning Program - Secretary
- 11 shy
The COUlcil ITIltW constitute cOlClmittees for Finance - Accounts Personnel and Sup lies nd Stores ir~whi ch )nly members may be included Other commitles sc1h as those 01 training info1nation and education and researCl ara ~valuation r1ili also include experts from outside
410 he Off1ce raquo) cc im Panning Program which at present forms part of th ~Hnis try or [i n should be placed under the Council and its staff strelgtl ilcn~ii2 i~ r181 it may cease to depend upon the services of the Mir is t y of H~alth
C Office of the Family Planning Program
4 11ollwther the Offic~ of the Family Planning Program remains a part of the Mirisry of Health or is transferred under a statutory council if one is set uP i needs to be strengthened to meet the requirements of an expAndshying pr )gn m At present the following sys terns need to be ins ti tuted in this Office
a a 3ystem of setting annual targets for the enrollment of acceptors and the projection of service fadli ties in relation to these targets
I Ci ~ystem oE V)glC loHitoring (the monthly statistics flowing from the clini~s c~iiiain unproc(~s5erl for months)
a system of program evaluation eg demographic effect of tte program cost studies
1 an overall design for media communication based on a study of the reach a~d cost effectiveness of different media and the effect of the meflBsge content and
e a m88t~r plan for training which would comprise an assessment of the training needK of the existing staff and future reshycruits and a long-term plan divided into annual programs
412 Th2 Prograll afiie s~lould have the services of a demographer and a meeia expert A training adviser is expected to be provided by the PARO
413 1be Program Office should evolve schedules of field tours to overliee field operatio1s E~1eh health cente heal th office should be visi ted peridicaLy by the Milt~dical fElce- the Nursing Officer and the Health EduCltoI who should guide and assis t the local staff in carrying out the progam Their tour notes should go into separate dossiers for each institushytion and ~ach dossier should have basic demographic data about the area coveled by each institution These dossiers would be a useful record for revilwing l)errOmance The staff of the Program Office should be augmented to Ol)erte this control procedure
- 12 shy
D Decentralization of Powers
414 ~hete is a concentration of administrative and financial powers in the 11in s try of Health I-JllJCi1 results in an accumulation of references in the Miristl) and delays n field operations Specific powers should be delegated ~o (a) the PliO concerned with MCH and family planningmiddot (b) the Directcr o the Program Office (c) the Regional Director and (d) the County Medica1 Oficecs The Ministry should invite suggestions from these officers and wOlk 01t a schedule of delegated powers
415 A tdgh priority in the matter of delegation of powers is to arm the Regiond Directors with sufficient administrative and financial authority to implement with expedition the health and family planning programs of the Ministmiddoty 1 thin the areas in their jurisdictions
E Integration of Family Planning wi th Haternal and Child Health Services
416 At present family planning services are being provided at 48 Goverrnent hospitals health centers and health offices by using the full shytime E taf cf these institutions and employing part-time (sessional) doctors nurse~ anI clerks where necessary At 29 of these institutions separate famil cl~nics are held on specified days in the weck some being doctor sessi(ms mel others supply sessions run hy nurses and clerks At the remaining 18 imtit1tions family planning services are combined with antenatal child healtL cr postnatal services The Family Planning Association runs 8 unishypurpoe f am ly planning centers which provide daily services and contribute a 11 t le less than half the total number of new acceptors per year
417 N assessment has b~en marie of the effect of integrated MOl and famil~ p~ nnning services an the recrl1i tment of acceptors nor were ~ data readily avallable for this purpose It may be observed however that in a situation of shortages of trained personnel for health services utilization of the existing health staff and facilitieR for family planning is inevitable parU cllLrl y in the interior where such shortages are more pronounced This underlines the need of evaluation of the integrated xai and family planning progtam for its impact on the number of acceptors Also a study needs to be made of che utilization of medical and pilramedical manpower so that it leads to bdter ~llocation of duties and optimUJl utilization of personnel
418 ile integration of faMily planning into Mcn services has certain advalltages as well as attendant risks The advantages are
a Lbe association of family planning with the care of mothers and children helps project a benevolent image of family planning as a program of family welfare This creates a
- 13 shy
1imate favorab~e to the acceptance of family planning aa lt p-)si tL1e il-Eare rreasure rather than a negative program cE limiting c~ildren
h t elps erlist ~r2tion tf doctars and nurses who as c -~ass enjo tft~ Y)er)et~ a~d confidf~nce of the communities i712~ Eerve
c ~ieD of contact with women
d luni-purposa clhlics for ~lCH and family planning services are onenient for motn~rs who would have to travel considerable (listances to the clinics
e hete is better utilizat1on of Acarce heAlth manpower
419 he limitatio$ of integrating family planning with MCH servicesI
are the posiOili ties of loss of focus on family planning as a high priori ty prograrr ald the diffusion of pol1sibility for its implementation These could tlow ve r he safegurded agaifls t by adopting the following measures
a 11e job descriptions of doctors and nurses should be rewritten 0 include the family planning function
b hE perf0rt1iai1ce of ctoltors and nurses should be judged as much )y tbeir inteceq t in planning ~vork as in maternal and ~hjld care and this should he lade known to them
c )octors and nurses involved in ~CH services should be given middot)rj entation and traIning in famj ly planning and their interest 3UEtained by refresher courses seminars meetings and supplies of literature
d Thl techrical (xpert~ in the Office of the Family Planninl Program should maintain liaison with and guide the field agencies in implementing the family plannin~ program For this purpose schedules shoul d be marle out for periodic field inspections
420 It is suggested that the working of half-a-dozen centers where family plbnnLng services have been integrated wi th MCH sessions should be studiei for ehe purpose of standardizing the methodology of delivery of servicl~ Such a study should include staff strength patient load recoril shykeepills 10middot of patents in the clinic timing and frequency of clinic sesaios ani convenience vf patients
F Voluntary Organizations
421 I i~ internrticri31 expedence that the birth control movement is pion aTC tt volunh[~ JilC S Qltl that hen the national governments step in wi tl cmbi ti 019 prjhns wi thin the sLate welfare system voluntary bodies ieh tteir limited ilsrluces restrict their service activities and shift the emplasi i 0 educedgt (f the community training research and contracepshytive Sf vic not 1l7gtilflblr in he official program or in areas not reached by it In nagni tude and expanse the of ficial program in Trinidad and Tobago has alrad~ orertak~n Ce 101umary program Increasingly it will become the domLnart tartner in the total national program while the voluntary agencies will cOltirlU1~ to receive financial support and encouragement to set up high standaeis If service and explore new areas thus acting as a stimulus and an additi_e tl the official program
G FrOB-ram Infomation
422 Thre is no concurrent evaluation or monitoring of the Program The daa or lq72 flowing in from the clinics month by month have r8Jllsined unprocss~d tn the Program Office The official Annual Report - 1971 Sums up th~ poition as fcllo~s
ITThe Research and Evaluation component continued to be the weakest in the Population Program Although a systen of evaluation had been built into the program the follow-up procedures for analyzing the data and for correcting inshyconsistencies are inadequate Requests were made to extend the staff to establish a more viable unit but by the end of the year no chllnges had been made
423 T1e recording and riporting jJrocedures were revised effective Januery 1972 and there has been a further change recently at the instance of t1e Evaluation Adviser Under the system now established the clinics are lequ Lreurod to maintain the following records
a Family Planning Clinic Case Card - New Cases This was introduced on January 1 1972 and has thirty-one entries giving age parity contraceptive listory pregnancies socio-economic background ource of family planning information and agency for notvat ion bull (Annex 2) The case card is made out in duplicate for each new acceptor and a copy sent to the Program Office
b Daily Regis ter This fs a ne~gt1 form recently introduced in replacement of the old regis ter and is preparen
- 15 shy
ie) ruplicate the original to be transmitted to the Program (fHce and the carbon copy to be retained in the clinic Th~ is a very 121zborute form requiring 36 entries to be aa~ for each Chse nel and old attending a session includin~ (ntries to cit L to contTaceptive supplies issued
AijCleX 3 T~13e fcnnG are required to be sent to the Program lffce in i7JO balches every month the first batch for the i IS fif~eeL days and the second for the remaining part of hE month The trtention is that the data appearing in the ~EZlic daily legis ter forms should be compiled in the Program Office and fed back to the clinics Although it is claimed that this new form has been pretested and is workable ex)erience alone will show whether the majority of clinic cL~rks are able to cope with it in a busy session
bull o now-Ho Card TIlis card is intended to keep track of ac ceptor--It has entries for name addresfI and month fcr which a visit is due for each year
bull Aphabe tical Index This is a card index of clients with aidresses
Each i)at en is given a simple clinic card on which the dates of further appo~utnli rc3 an~ indicated A special fonT[ has been devised for the reporting ot cases unler the Post-IartumPost-Abortal Education and Referral Program
424 J system of monitoring progrRm performance from month to month need to bE develQped as a high priori ty The problem is not so much reshycord ng mc transmission of data by the clinics but its aggregation and proclssi ng in the Program Office every month which at present takes a long time The Statistical Officer should have a statistical assistant to help him Ln I he taflk Monthly progress reports should be available to the Mini H t~ n H(llllth and A11 offt eerlil of the ProKrnm Office so that remedial ac tl m I lAY h(~ tuk~n n rll1u- WhOnh1f ~Hfl(AlJtlaTY
42 For the analysis of data and evaluation the Program office shouln haVE th(~ full-time services of a trained demographer
H Field Workers
42) Tie Program nemiddotis tne services of a cadre of field workers to enr)ll neii aceeptoTs follow up acceptors in their homes and revive the int 2remiddott of dropouts Such a category of workers could also be utilizerl for pr1fficting other health programs such as the VD campaign and the inmuni~ation program
47 As an experimental measure one field ~]orker may be assigned to a emi l~ of Hi 000 population This would mean 100 field workers in all
- 16 shy
Earh of the workers should preferably have harl a higher secondary education otherwLe 1gt junior secondalY education They should be married persons with middoti1ltt mot tl-an two or tlree children recruited from the locali ty in which they armiddot~ requlred to function Only persons who have the capaci ty to comnunl at~ and or6anl~e should c chosen A months ini tial orientation
slcu1d enable them to start functioning in the field though reshyfresher CO rSeS tvould be necesslt1ry in due course In Port-of-Spain married mer~ a1C women may be employed on a part-time basis
I Hanagement Study
428 A nanagement study of the Family Planning Program should include a sctu iny of the top m~nagement Atructure (Population Council - Office of the Fanil) PLanning Program - Principal Medical Officer for MCH and Family Planni Ig fetices) the field structure for the delivery of family planning servics (Re0ional Director - District Health Services) including the utilizlti(n if medical and paramedical personnel for adding the function of del ve y )f family planning services and the control and communication proCed1reF Lfnking the top management with the field structure
429 The management consultants may study the functioning of the Popul tio I Council and advise whether it adequately serves the purpose of givini po Licy direction to the Program and if not what changes in its compo itt m and operating procedures may be introduced without altering its bsic craracter as an advisory agency The consultants may suggest an alern at ve form of organizati)n and utilization of personnel which in thir p nion may be better adapted to the needs of the Program
430 Irrespective of whether the Population Council is maintained or it is replaced by an agency of a different character a formation like the Offic of be Family Planning Program would be necessary for the administrashytion i)f 1 he program a task for which i 1 appears inadequately equipped at preselt Its obvious requirements are in the areas of program monitoring and el7alnation program supervision communication and training The manag ememiddotlt consultants may study the structure and procedures of this form~ tio Gnd make suggestions with regard to the augmentation of professional and ~ upp)rt lng staffgt and modification of operating procedures
431 The linkage of the Office of the Family Planning Program with the Miniutry of Health (Central Office) and the District Health Services should be sudied In view of the policy of the Government to integrate MCH and faI11iLy rlallning services it should be examined whether the Principal Medi al Officer for Communi ty Heal th Services (MCH and Family Planning) should be agtpoj nt~d as the Chief of the Office of the Family Planning Program and an adTlilistrative officer of a suitable level inducted in that Office to assist him TIle implication of this suggestion is that the head of the Family PlanJling Program would control the District Health Services
- 17 shy
432 rf 1e management consultants should examine the delegation of adminshyistratiie Bld financial powers of the Ministry of Health to different levels of Progam aclrlirdstration viz bull PMO Program Office Regional Director and County ~djca~ Officers
l33 he system of 01 af Togram information from the clinlcs to the Pr()~ra1 O~fice and tOile processing and use of information in the latter office iholld )e studied
434 he working procedures at the integrated McP and family planning clinics shnuLl be studied This would involve a study of each stage which a clien tpcticmt has to go through from the point of entry to the point of exit after receiving advice service or supplies This study shoulci lead to star dartization of procedures and functions and evolution of -lork norms CognatE st tdies of the working procedures at uni-purpose family planning clinics and su~ply SEssions should also be undertaken An essential component of these ~ tad ~es would be to examine Nhich functions currently performed by docshytors lealh visitors nurses and midives respectively hav~ become so roushytinize ttl it they can he relegated (0 the next 10Her level
435 Reated to working procedures is the problem of job description of medcal 8nd parrunedical personnel involved in family planning from the centra i tc the field level This job description needs to be studied wi th a vie VIW8Id txaminiDg the uttlization of skills and allocation of time by the staff lcc(rd~ng to the functional prj ori ties
436 frV management consultants should study the workings of the curren slralgements fOJ family planning counselling under the Post-Partul11 Post-Abortal Education and Referral Program at the Port-of-Spain and San Fenaldo General Hospitals
437 SU1ect to the ItBrcement of the Gove1nment the management conshy8ultal ts ~hOLlld undertake a study of th requirement of field workers (home vinitcru) in tmtlUI of are nnd population cov(ra~e
ANNEX 1
Names of Persons Met
Ii Mr T C Taitt Pem1(H~nt 3~crtarY) Ministry of Health
2 Dr M n Henry Chitd Medical Officer Ministry of Health
Ellubeth Quam a Prindpal Medical Officer (1S)
4 Mr G Z Jaine ~ uJiector Population Council
5 Dr Norma Andrews Medical Officer Population Council
6 Mr Jc~n Coury~ Evaluation Adviser Population Council
7 Mr A Jriseph Principal Statistical Officer Population Council
8 Dr C 0 Colman Country Representative Pan American Health )rg ni~ation
9 Mr ranca Kippel Health Education Specialist Ministry of Iea th
10 (1 bullbullines Principal Nursing Officer Ministry of Health
11 Dr Mx won (formerlyHinistry of Health)
12 M3 late Carops Ex-Chairman of Population Council
--
4i 1_ middotIIlt F-ntCWclOotf_Y v OJ t tl
GOVIIlHMEIgt(I OF TINIOAD AND TOampAGQ - NNISTJY OF HIALftf AIJIE1 2NATIONAL FAMilY PLANNING PROGRAMME
F MIL Y PLANNING CUNIC CASE CARD - NEW CASES - NFPPl
li ~~___ 1 ________
~ ecll-U
-- --------------------- shy~) ~~middot~------------------~~~~~~---CIJ------ middot~ii--middot-middot----middot-middot---middot--------- shy
ltv Writt N_ 01(111________________
a ~4itiJtmiddotl_____ ilIIIltIoI~____~____~-__----- shybull ~4
fie l$ - JO tDql IIfIA- tr-JMimiddot _ iJ 1 Odoor o
14aorielaquol_ _~ 0 lio witIleo-La ~ 01 bull - OJ ( _01 1~ltgt1lh o bull- 0$
AacJcu 0 2 CIIriIWA 0 J Os 0
Yv~MONTH ltnollOf~nfIGHTI
Undu 1100U$ Utgtdn 5SCI Undu 11200 01 ~ 50 - 9949 amp100 - 1199 02UlOO - nn9E~ (
0)~ 10- $99 SiOO -- U9~ lOO -- U99 12400 - 1359)-------_-r----shy ~l)o SIS n600 - Hm1300 -- 019 OJ200 il~9 ~------ 99~ a 1)0 m Os1)00 -- l99 1400 -shy $4100 -- 1S999r--- shy
1500 donl S6000aad O399 - lt499I~- I 0lt
ltII
IJ -IC _~tltlioltgti lS
02 IaampJIIocI OJ 04 laM Os
w Oltwio I_-l(~u IrIaa U
h~~ ~Clubl 01 OJ
IS ~C-n 01 toSIitDI 02
Ji poundI on 01 IriIIIuy M ur 02 IV OJ
WU 10 pltIoII~ llaMtl 411 cIIiId 01 Ol it fIolto ~ do~ _14 rou IIlgtJo 1Ia1 ___~_ shy
40
It _ I 00 ~bull FPIiIJ 1
OJ 02 OJ 06
)0 III- iy wOWcf ~1
aMIIl Os
11 T 1gtlt ( h _______ 4)~
06
04 (MIbullbull middot bIrlI ~___~__~_ (-fIJI ~- -~-- (1HJ 49middot SJ
U 10k 01( 1__ raquo$-4
iU1) DOl F ToWotfOlnC DOl 001 or Do [IP 006 001 OIIgtu___Spltclty DOll Nltmo 010
U1Mo I orcpmiddot laquo55middot16
1lD 001 Foam Toblelf_ICim DOl Condom DOl CoomS~ 004 oe Oos WlttuJn 1J OIkr DSpody) 101~ ~Iu 006 Rhylhm 001 DOG OJO
no wI~lmm 4 cd
(I 0) 1110 01 Condor 03 (lorn bull l S~muoidIl 04 Faa TabioolfIIltr- Os RhyUlm 01 lnJrl tible O Advico 090 06
la slt 1)0 19 loti ~rltnlt) ([)sl or 1llOn) ____ --__ bullbully-J n SV - ~JcdS
v~ Cl NCI 0 30 OJI_O I Wr blJ1h 0 I ~ OJ 1 ~ (fOOd V 01 No 02 laquo 6) Cf4
WIiI 1 172
004 001
j D middotmiddot middot
1 ~
r
~
bull I
bullI I I
r c i
ANNEX 3 Pagemiddot 1 of 5
0 raquo rshy -lt l)J ~ 111 t G) 5 shy (J) ~ -
fT1u
i
MINISTTY OF Ho1TH
NTIONl F~ILY LNNING PR-GRbullbullM-tE
~~5tructions to C11nic ClerKa
How to co~ploto the Daily Rogister
~~ ~~v1sd Daily Rosi8ter replnc~D tho one which is now in use tb$ Monthly PC~ri rOt~ arti tho 01( Ci() Dod PollJ j f m It is a pre-coded form and 1411 cl~1p Jd tl a1I6iniul-mIHvn Oel Clinic nctivi~y
110 )rm rollt biJ coupJot)d lrl cupLtcoto using a o(roon shoot Tho top aheot or oriinai ~ust bl) 6(Ult to tho CQgt1tral O[[lCO and tho carbon copy retained in the Gliaic rilo dll the for6a that ar uD~d betwoen the 1st 4nd the 15th of the oIIollth aut bo subClittud tocho office 35 Lnc blttch Those oomp1cted betwoon tho 16th _lid tqemc of tho month must bo ~cnt in a secJnll batch
P lOvLior hns boon Illllde for 25 clients on cZlch forlll new forlll must b IIlied f r poundh 50[810n2 whothur or not ono or lIIore session are hoIdiit the clinic on he sarne day
I th ro alO more htl 25 clionta 1n attondnnco at tho session the additi shyOhAl m~bOl of clionts 10 clients nu~ber 26 27 etc sh0u1l be ontered on the next Imiddotrlll ~i ttout a1tpoundring the numbtlrs in the cvlumn hond Series
51 ppOfil th~ number of aUcnts lQr that session ws 5 this would mean thllt two rJlS ~ lst be 6ubllIitt~dl the first filled uF 1 tltgt 25 And the laquoIncond 1 to 10 Th~ cal bon ofies should bo st~plod togother at thu t0P l~rt h4nd corner of the torm ard ktpt in the Clinic filo lou IIlU6t stapl~ the originftls in the 8~~ monnshyer for lIub~ssion to the ofticl
ie h~ ll idontiflctior- (cc 1 - )
0 lot Ji 9 anythin~ hGro poundhia is int(mdClc for tha computer code
2 ~~pound~ - Print clOflrly tho name of your Clinic
C1Lic Huml or - (cc 4 - 8) Evar1 Clinic Numbor has 5 digits Virite each dig t il a t$purate box
It Pai~_thllsectgdllion (00 lt) -1 1) - Dl monll 10M
lw) bolte IlrO proY140d fetr olAoh pr 01 thQ dISh Enter tho dA) ldns a R
d16ih
emiddot5middot (0 11 I for 115t ( 0 21 for 5th etc Treat month the am pay
e ~ 10 ~ I for I-hrch 0 [2] for September Tho y~nr must be (into ad
I Z I ~ I I 71 q etc
Take as in IixulIple tho dOlte 3rd tllrch 1973 7~ie must bo written
[0131 LSLDI[7l3JDny Month Ye~r
5middot 1~J $~~ - Irom ~-------- To --------shytntol hOI II the time the Clinic 111118 in SW5sion emiddot8middot
(i) 11011 500 lm To 1200 non
(11) Frclt 100 pm To 400 pm
(iii ) IX-OG OO pllI To 6~00 pm
f
2
ADEJ ) Paae ) of S
6 Eov
_ 1hA 1gtIpoundC iIIUlt be nu~o7Ifd tler1ally 1 throurh n lU tbey Are Wled In ~1l8ellJ IInel 1301 tlU 1 Orcl 1 Wled tor a o5038ioll - -I 2 tonY tho _boul~ b I1WJbtl 1 and 2
hlrlll are 25 linos OIl the fOnl Ilnd thoae muet be UBtleS for 25 clients 9 one ior bullbull 01 I ini
ot ~h lc II ol1cM lOlivpound til e linic before soeinc DurOI or doc tor ilnc ii hox rristrltltion nUlJbet had alrearll been recorded on the Dai 1y Roiuter then n line ~hollld be drawn through that entry an1 the eliort nust not 06 includttd in tho totals tor that 0eDion
1lw Ileifitration Num)~r of cueh client must be IiIritten IS n 5-dlrlt oode ClhnC IH11IlElr 315 1IIU8 tborotore be enterod 18J010117]5]
~ Clt ZOt
Coda 1 Codo
10 ~tl c 2t j co 21)
~w elSe - Coda 1 0) d CltaEl - Code 2 Revislt Code 3
Only pound1 01 theBe coiles may be usod
11 prol-O~ ~Eil~1 (cc 22)
If ma climt was L drop-out IIho haoS returned now to the Clinio tor tho first no linmiddot bullwin lt1ro1eo o t he or she should be given CCe 1 It this do 5 II It nprlly leu this colWlln blank
u Hothod middothisllill loe 23)
NOh til t otly ~ Cod 16 tp he ontered in 2lpound of the columna oven thOUGh 10 co11lllJlB 10 provided on the torm The Codes llrol-
Oral Contraceptive Code 0 1 U D Code 1 Condom plUD Codo Z Condor (only) Code 3 Foum tAblets cream Code it DitphrClGJII Code 5 Rhythm Cde 6 Injectible Code 7 Advice Code 8 Other Code 9
It for middotDo-le 1 client rlllll ji yen cclldorls ord foam or creall Iou Qust entor Coole i (condom plulJ) in the appropri~te column This Quat be the only lIotmiddot) tarcie If an in the cnse of a tlnle clinic I the client is Bup)lieu lith COIlOrW only you rmot entEr CorlQ 3 (cpndolll) Do not use a ticII ~ tho (odo Nwber
It is CUi tomary fur 11 cliont 110 is beine put on the oral contraceptive for the first tiT1o and even on other occasionn be issued condoms and 11 crelle or foam a Ilell rI3 a pgtcket of pilla In such Cllses when the piDQ Ilre Ilctually iouou you tlust record Orll (Co~e 0) 08 tho onll metbod ilo othor ntry sll0uld ho nnrlo
Uovever n SJC~ canas vucru condoms and fOHa ~rc eiven but no pilJa (even thoJRh _t _n the intention to issue pills nt the noxt vioit) than the Mothol Th5 ifli t ohoulcl be recorded uo Condor Plus (Code 2)
13 Seen Bybullbullbullbullbull
~rot S-1 SO l
Doctor (Dr) - Code 1 j Nurse (Nul ) - Code 2
Clark (Olk-) - Code If tho Clhnt is vcen hy both tho llootor tlnd the Nurse enter Code 1 t Doctor It 6~61l by the Nurso only arite Code 2 Cod bullbull Cerk is l)llnt for FA Cllnica Clerks in tho Government Cli1t hiwo Llttoll istructed not to i56uo supplios on their own volition
14 fl221~
lhio S~tiCl of -Ie fvrtl t~ke 16 (llrci coluMna (cc 25-+0) nnd 10 tho only part at th iOIQ in llich iore thAn one cod is Zlccoptl1blo Tho purpoco of the )ecton is to 0 able to arrive nt the Cjunntity of 6tock dilltlitJutshyed YOI IIlUdt writo in the CllllOjH-iata colulna the nUllbJr of Il1ch 4rtic1o i~JSu~d ~lo e ha I Oral Contrcilpti vea are aub-di vi dod into types ae_ 3 PIllCKC 9 0 Elynnn LlUot be entered Codo in card column 25
If tor eXllrplc t l cliunt is iosued wi th packots of Zucynon nnd aJ(1 ~ivn 1 conuotll (8inoloo) you ouot enter in oard column 25 and 11 It
cnrd col~8 )2 and J (io 1 in card colucn 2 nnd 2 1n card coluun 33) Nota C)lldoIlU ale to b(t ruoordod individually not os packots of throo) Should n ne LlondoClo be isoued thil3 is to be rc-Qed as 09
If It clint 6 t~ot isoued Blly lIupplies thon you must writo Codo 1 in CQllAlilD 41
It Q eli nt isite the clinic to check on her LUD or her Diaphra~t IUId ro DI W 6 ppl ills nre ispounducd then Code 1 1s wri t ten in column 40
In the FA clinios here a variety ot orll contraceptiveo in orer~l tho elerll wilmiddot~ bJ provided with a specill code shoot The idontifyin coo will b wiittn in Column 29 nnd the nUlber of packets iosued in colwm )0
lralaer-In Code 1 lrllllsie r~ut Coda 2 leIllPQrArr Trnnsfer-In Codo gt
In the cao of n 2ratl8fcr-In I you lUot n160 cOrlpleto coluons 42-51
In the cllU J of A ~~emporary TranGfor-1n (an individual who i8 only v1citing fur clinic tor some epecial trcatcont hna who will bo rdnlnin
~middot(II~~~fO~l~SIl~I3~nn~~~h~rO~nh~1~~190~~nll 2-46 and ler rei IItrntion numbu in colullnll41-51
It the oli( nt i iNt a CrllnoforwIu - Out or loClporu1 tMn loave oolumn 1 blank
16 lr4nst(gtr-tl2~~morrry TilJnder-In (co 42-51) Forl1ltl CUn E1~ (cc 112-46)
hen you rei iatlr L irllsfcrln or Il TJlporary Trnnsfer-In you IIIUBt write I ere the five-digit clinio nucbor of the Clinic iraQ which tho ltlient Me (uIlO
2mer ]letr ~2n ~ (cc 47-51)
frlta fllao Clo r-~itrlltion Nuc~Er ot the client in the Former Clinic (i c bullbull th 1 Sis rnmiddotion ~UlIlh()r which the client carrics 1n the tormor clinio) bull
It tho Forrltl Ho( ist rntion Number iIJ not readily wnilnble you tluct oocpluto thtl epcciol [orlll Transfer-In Not Identifiod Dy Forrlcr RCGi(trn~ t10n Nwlbvr Or ~ flt)rCl is to be cOlplctcd for och cnso nnd th forlJO Ilubmi tted to thu )opllntion Prorrnnme Of fice tOGether with tho Dily Ro~iBtors lhwev~r should the clork leuTI of tho clint B FormlI Uocintra tion lUlllb r )0[(10 Cubmi ttinft the D1ily IOCI otro t hen the nUQbcr shoulo bo -ri ton in colucns 47-51 lna the special foro should lJo deotroyotl
l7 bullbullbullbullbull
r lt bull bull
ADXI ) Pap S ot S
11 UD LV~ (cc 525)
It tb( cliont io ~ivQn An IUD tor the firot tl~o then you should Sri to Codo 1 Inuort ill colurJI 52
It tho olimiddotsnt ia rvinGgtrtltld i th An I UD bullbull tben wse Coda 2 RelnDltlrt shyin (01Uil11 52
It the clLmt is ~tte~~dint chnic beruse her IUD CflClQ out by Haol (cxpll Iion i ~hcn fir te todo ~- UIlllrli1 53~
If c-ltr IU fj IIIS reov in -ne cllnic by tho doctor or nurso t~on vlritI Codec in column 5
II the eli nt otends eiLlie tld explin[l th(lt she rccovcd the IUD tlllleel nen write Coda H in Colwlm 53
It the IUD jr still within the uterus nd the WOIraquoI1 1 11rc6llJlnt thon lIrite 1gt40 4 in Column 53
lZ np h5t (ce 54) It 0 Pull 5mor ie t~ken durin thi visit tben Codo 1 ehould be ampDtere4 in ColWlln 54 Should he c110nt lltt rQ(uircd to rttturn to clin1c for a rogtol1t Pnl) t06t then CoLe 2 llhould bo middotwrittcn in column 54
It no Pllp Scou io taken tde visit Itove colUQn 54 blank
Iraferti1lli (CQ 55)
Ii the e liett io nl1 infortili tr eaoe use Cor1o Ill in colUQn 55
If tbia 1000 not tlpl lonve column 55 blonk
20 Totaltll
CO~1ploete the [)ldegO 1gty puti YI tne totals betweon the double lines nt tu b()ttctl Carrj colUlllnc 20 21 nd gt4 Must hlve tho Bnoe JllIIber and thiG Would coreslonc to the numocr ir attencbnco
Writ$ th to1ul nUlllior of Drop-Outs returned (c022)
Urito 41eo tb totnls fOJ each card column 0 to 9 under tho h(adinu Method thiB Vioit Show tho tote L fgtr OlCl type of contraceptive issued (cc 25-40)
1)0 Dot wrLte 1111 totll lUl(Ier Card Columns 15-19 29 41-51
21 COPmllh bull ~lt h~t~ Monthly ROilort
OQ thG DaLl oCator forlll thnt ccrrOspOldB to tho 1(8t 1$06610n lt 0
oth yo Olllt (vwlgtleto the items nt the botto of the [orampl This is tour ontll~1 n(olt nnd includcD tho totll lumber of sesions Ilntl tho total Iluolcr ( r crop-outs durinr the Qonth
An tiUlsilt n drir which n doctor liB in nttcndnncc is a doctor sOfll~1on and shoulc 00 re(liGtcnd in coltns 56-57 All other sessions 1116 conlliid~recl supply stllciona and thtlY 1110 rocordod in columns 58-59
the total Ilum)nl Jf drop-outo ld the drop-outs by method durinc the onth nre 10 bu oltorou in the inrlicllted boxes
72 Chad Your ~
Milke I ura th t all thE fijul4gtu rre c101r -tNever writo our nutlUQrS 50 InrjEl that they oxtend out of tho
ap~rotr1ato ~ox
Cheek to BoJa tht 1111 numuors 1110 in tho correct boxes -- CJslHloially when Writi1 the totlB
Mllxe Cirtc O thmiddott t1e infoT1I1ntion i6 clear on the corbon COllY before sep rmiddotinr the sheets
Jitn the Fomiddotl lien tly sien YOUl nr me 1t the bot tOil right hnnd corner btl forc subol ttinG it Keep tle CL rb n copy for your rocordn
i
-l ________~~---------~
I _1
Adminiatr-atlve SKVieu
P inba ~~~l1cal lrlnbin~~eltltcal -1 te~ra t~~rvicc (lnatittloaa)
--1- - shy -1------------_-L_ l-r-aJiil- shy _-L_tet1lal d
PlIinm1tJ8 atdUon DetalMid H8Il1tb ~ ________bull Care
-----~ Office of i
the FlIily _IPlill3 roarshy
1- - - -------RegiatUll urnr
ltIi 1 Drelttor Rcgicaat Director Souta Tabqo tacallortb ~ counu gt____ ~ (4 ouottet)
Off1ce of the Res10nal Diractoc L
r----- _L_ -- shy i I bull IREgional Ipitl I
District IIttaltb I bull Othn RelOl ond Hcpital CenteIntt itlt j In 1__ _shy-~- ---- -_j
J r Ii~lth
C~nlef
L
I Ihnlth lie I th Offlcu (1ft lc~
Coullty 1I0p1ta1
Henlth tentet
I

I INTRODUCTtflN
101 0-1 behalf of t~ H~1k ~middotmiddotr R N Madhok (Consultant) visited Trini12d ad Toblg0~ middotl iL bullbull ~)3 0 review the administration and mal1agme)t )f thlt hsd j 11]) PVnning Program During his stay in Trinj dad 1- MadhJk ( iilh eprefEntatives of the Ministry of Health and the Topu ation C01Jii1 fuJI li5e appears in Annex 1)
102 ~pecifgtUy ~~C iVlsdhokcevievled the following aspects of the progam
a he future role of the Population Council -- whether it should )euro an advisory or all (~ecutive body its administration staffing and statutcry pmrer under a changed set up and the consequent changes required in theliinistry of Health for the implementation of the prc)gram
~ J the extent of (l~i-5ting (Jpcfntralization of administration of health and frunily planning services and its efficacy
c the desirabiLty of integrating family planning with maternal and child hcaLh services in the light of experience of inteshygrated i~lirJ(
d the efficie~ Cf~ll edsirg system of the flow of program information ac ~Hl red charges and
specific aspects of manager-lent and manpower utilization on which the management finn should concentrate during its study
103 The following report contains broad suggestions on changes rE qui ed in the existtYg structUrEgt
II ORGamp~IZATION OF THE NATIONAL F~~LY PLANNING PROGRAM
201 The administration of the National Family Planning Program is the rl~sp(jnsibility of the Ministry of Health In 1967 when family planning was adopted as an official policy the Health Minister at that time proposed the stallishment of a Population Council to advise the Minister on the organizashy1ion of a natiorlal prorrun 1i(h lIIotld coordinate all family planning effort n tle country Tlle Cabtn2t c~ciCled that
A Population Council of Trinidad and Tobago should be instituted for the purpose of giving overall direction to the Family Planning Program in Trinidad and Tobago with a view among other things to coordinating all fanily activi ties in the country II
- 2 shy
202 In pursuance of t l= foregoiny decision the following terms of refer nce were framed for the Po1)ulation Council
10 i~vll ditcoction to a Family Planning Program fo Y ltdd cHl T0bagn d th Ii view among other things to eo ~ ~c n lfllonrdnr activities in the
203 A PTOlllH~ f(cibor nf ttl rredical profession was appointed as Chailman llei the lill~1L y h2 jiamily Progran Ministry of Health as the Secrltar r (r th C~-ur~ ihe membership of the council comprised officials of tle t-instry of He3ltii and other departments representatives of the volultary agencies operating family planning services and leaders of opinion the present Chairman of the Council is an eminent gynecologist in privmiddotte practice and a former Minister of Health the members are as foIl 08
1- Chief Medicnl Officer MOR -l Spcclliflt ~middotjJ3C Officei- General Hospital
3 A rEpr~senative of the Ministry of Planning and Developneut
4 A represehtacive of the Central Statistical Office 5 Public Tidaions Officer Prime Ministers Office 6 ~ PrilLj~d t1lt dq Officer NOH 1 ~e( CL bull ~clmiddot ~~t)pulati on Program H Chid ~ea~h Educatoi ~lOH
9 A repres~rltatiVE of the Catholic Marriaie Advisory Council
10 amp 11 Re~)resentatives of che Family Planning Association 12 6 13 M~mbers or the Publi~
14 Diector Family Planning Program MOH - Secretary
Olj The Population CQtJrdJ hal three roles (a) policymaking ll) I rogralil formulation and evaitllt1()l and (c) providing general direction fllr program implementation Its composition is designed to ensure (a) intershydapamiddottmental coordination withill the (overnment (b) coordination between the ( Ole-nment program and the activi ties of voluntary agencies and (c) rapport vith pblic opinion
05 The Population Council is assisted in the task of program formushyIation by a numbe of committees ~thich are so constituted as to draw upon Ihe ex lertse avalIahI wi tlin the Government as well as outside Pre-eminent arnorg heseuro commictees s lhE lati()nal tH Program fnLMulation committee ihi(h technically speakirg is not a committee of the Council but a commitshytee of the MOH It inter-meshes with the Council since it is the policy of the Government to integrate family planning services with MCH services delivered through the network or health centersoffices of the Ministry of Health This committee is headed by the Principal Medical Officer of the MOH in dnrge oE Integrateci 2~edicil Care now restyled as Community Services
- 3 shy
which COlT bull Se 11CH anii IIgt sxvl(s I1H~ other committees are Community Educaior and Publidty Cvrm] ttec Research and Evaluation Committee Family
~du aton Comrnirii ~~e(i] CCimittee and inance Committee
OS i~ n1eptUd~ i p Ni ~runi t 1 an advisory body and as such itus 10 execl1lt)ltjmiddot n p-actice the Office of the Family Planning Prog) am e tabisLecl wirgtmiddotcn tilt2 middotlnitry of Health functions not only as the ecr ~tc dat of lIC )hiCJl but also as the instrument for carrying out lis lirEctvls Furtiie ch GOtdcCU has concerned itself nomiddott merely with broal i~ SUIS f10Hc out also vL detailed implementation The majority of t le r emmiddoters of rhe Council are in favor of Umi ting the Councils role to tile givlng of broad direction to the Program
20i The Office of thl~ Fitli1y Planning PrO~rall1 is comprised as follows
Dlrcct0r (Incant) Medilal OfHceuror (Famtly Planning) Nm-~If Offieer St~tistical afficer Health Educator 2 lield Workers (for follow up)
(OIlE positor vacant)
8CCiHWlcnt 2 clexks 2 typists 1 driver 2 proj ctionis 15 and 1 messenger
T- ~ g af f of the Office of the Famly Planning Program is under the discipline of thttinistry of Health since the Population Council is nei ther a departshymfntal unit nor a separate legal entity with its own fund
2 OB The places of )nrm1 atton Council and the Office of the Family p ~anr ins Program wi thi n the Minis try of Health as conceived originally by tile Government may be seen in the abbreviated version of the chart appearing hI different official documents and reproduced at the end of the report
~ 09 In April i973 at the time of the consultants visit there was In aCIDc)sphere of uncertainty about the administration of the family planning l)rogram as a result of changes in some of the top positions As a result of t c~binet reshuffle the portfolio of Health had changed hands The Permanent euroctet lry who is the princ~al ad~liser to the Minister was new as lras the r-i c al Yedic1l Officer h charge of Commurity Health Services (Mel[ and Pam ly Pl1nnhg) The Dtnct0 of family Planning who was managing the Office of middothe Family Planning Program and also serving as the Secretary of the PoshypUlition Council had reCiTed in March 1973 and a successor had not yet been named Meanwhile the Medical Officer for Family Planning (a part-time employee) was carrying out the functions of the Director in addition to her OWT Wi thin the Population Council the advisory agency for policy-making
and ccord~n8tionJ there was a groHinr feeling among the members that the ouncl1 510t1d shed thE respOJ1sibili ty for implementing the program a funeL on j ch nad heuroe added on to its advisory role with the passage of time
iO the 1 ~lp~1 the lines 0 responsibili cy were not clcay (e ned and Li1 refioal system was not fully functioning The post of Re ior 3 Director crth VIas vacant The policy seems to be to strengthen the 1St tu ion of Pt()1ic Flealth Office as an 3ency for the supervi-middot sion)pound ne district sflVices (health centers health offices and school servi ces ~l thin the ccnmty
II I PRES EN STATUS OF THE PROGRAM
301 ~he adl1linistrt~ivE changes narrated in para 209 have come about at fl tin e IJhen the P1ogram has entered a phase of declining performance as is 11 Jpal en from th colloHing figures taken from a report submitted to the Populaton Council
YrUL 10C7 ~j8 1969 1970 1971 1972
--- -- ------------~~ --~ - shy----shy
Ne Acceptors 3696 2731 16207 9997 9898
(End of October)
7560
Slur~e Family PlAnnto Program Report (no date)----AsII1Ulilg that th6 ttlrollmant of new acceptors during November-December 1972 prclrd at the 8ame rate as during the ten~onth period January-October
- 9i2the total enrollmslt in 1972 would be lebullbull than 8500
3(12 lhe total number of leW i-iCCeptors for 1971 shown in the foregoing tal11e 1s at variance with the following data from the 1971 Allnual Report
- 5 shy
~ev C~~ Contraceptive Method and Agency
nm Other Advice Total New Cases
Aeny
GovrrmenC ProEllil ___~zZ(lt1____ 97____2Lbull499___~528~___4i_750~_
Farr Uy Planning Association 2814 315 607 76
Catholic MarriaAdis1ry COLnc_H____
ge
74 88 162
otal 31[10 692 8724
_--__------------------shySOlrce Natio
1973 nal p
Fam29
ily Planning Program 1971 Annual Report April
NevmiddotrneJl~ss) the declining trend in annual performance after 1969 is manifest ana conpaes unsatisfactodly to the following targets set for the Program
Targets for Contraceptive Users - 1968-72
New Accep tots Old Cases Total
1968 20noO 20 000 lO noo
1969 20000 40 000 60000
1970 20000 60000 80000
1971 20000 80000 100000
-----__shySource National Family Planning Program
p i9
------------------------------------
- F shy
3JJ3 Ttl flient recrvitTrent has fallen off since 1969 in spite of a signif Icar t xpansinn ir the number of Government health facilities providing family paarin~ services FrCli1 7Hr to year Starting from scratch the number oE GovE(nment health irlstitl1tions delivering family planning services in isollL(Od ~ily pltJfAill~I ~J in c)lchiratinn ~7ith MCa services has lWW risEn t 4 lhis ie --tdt)p to t cii1ics organized by the Family Plannin Asce1ation bull U2 by tile Catholic Marriage Advisory Council which offers the ~h)lthm meti1middot1 nT
304 1i ciecli ne d~ d re11~m2nt of new acceptors coincidentally w-Lth th~ eXlsioH uf s-crLce facilities needs to be studied to identify the factors responsible for it eg the quality of services offered the strategy of commmic at~on and motivation and management and supervision One obvious gap is he abgtence of an agercy for promotion and extension of demand for family lal 111 If services -gt tLe field reliance being placed mainly on clinic counseUn H1d generaUzmiddotd mass media publicity The need for a field promoshytional agelcy is underscored by the dropout rate In 11 draft paper prepared by the Hed_cal Offic(1r for FIrnilv Planning it is stated that by the end of 1972 t ile Heuroe approxiclt ji rHJC cun~ent users of contraceptive methods and 33 per ert dropouts
305 rht~ program is cot merely clinic-centered but also female-oriented Recent Iy mellsages aimed at m11es and stressing joint male-female responsibishyIi ty l gtT j ecillc CImt-J 1 i~gtVt~ b~~in )7cn 1n0 the cOTul1mication activity sUf1 tv) c nts Em he 2iucaccw i milc8 and che distribution of condoms to them illVC he ~n or n~d iD r GJvefl1nenC s(~ctor The Family Planning Association has a130E~k11 the irti U3 1V~ to reis ter males ln industrial employment Tllese are steps in the ri)n dtrect1ongt but the size of the problem indicates the n~ ed OI a concerted effort en a much large r scale
306 Tre Program relies largely on the use of oral contraceptives as shown in the following table
Oral Other Advice Contraceptlves IUDs Methods Only Totals ( 100)
19)9 76 20 16207 ( 100)
1970 316 63 9997 ( 100)
1971 50n 4n 365 79 8724 (100)
Family Planning Association unpublished report
----
- 7 -
Althougr amJnp the neH acceptors in 1971 the users of oral pills were only 509 ~mon~ the old cases the figure was 119 The percentage of IUD users has remiined stagnant at an insignificant level this may be partly due to consume prefErence and pctrtly outng to lack of trained staff to undertake IlTD i1srti l7U There h hOHever a visible shi ft towards the uSe of othe~ ilettods (npchani81 and chemical) attributable to a scare about the side efects nf oral connaceptives Among these conventional methods the condom s 11 os popular
307 J t )resent fami ly planning services have been extended to 48 out of 106 hellth centersoffices run by the Government and the objective is to C)Vel t1e remaining health centersoffices within a short span of time so that adice and facilities for the practice of family planning are conshyvenient Ly wa nable to the people in all parts of the country By ann large sepanit e fITti ly planning eli nics are held on specified days as an addition to norrral lealth work Besides doctor sessions at the clinics supply sessions are rur by health visitors and nllrses assisted by clerks The nurses are authorjzed tc issue oral contraceptives for a period not exceeding three months ani the acceptor is required to attend a doctor session for advice during thi jnterval In 1971 the numbers of full-timepart-time staff in Gov~rtmnf centers renderinp family planning services were
Full-time Part-time
1elical Officers 14 8
NUseMidwives 35 19
Cl~rks 3 17
Now tile low~rnment -gtbjective is to integrate family planning services into MOl services and use the same staff being used for the delivery of both types of erlices at multi-purpose sessions However so far only 1A centers have interated family planntng with Men or gpoundmeral hpalth care sessions
3011 The Family Planning Association has eight unf-purpose centers where famil) pLmring services are available ftve days a week The Association employs tilrEe full-time and ttJO part-time doctors a complement of 14 nurSeS (who llave been trained to do pelvic examinations) and 11 other clinic staff membels The Association also has a number of voluntary workers in the clinics The CithoUt Marriage Advisory Council has three clinics but their contri shybution in terms of enrallment of acceptors is not signiflcant
3)9 A Post-PartumPost-ALortal Program was started in 1969 It is state I tlat about 14 percent of the patients reached attend a family planning clini~ 1iTj thin six weeks of the interview in the wards IhiR is qui te a low figur In 1970 when a system of home visits was tried under the Family Planning Aide Project in 7 clinics the rate of acceptance doubled in three clinils rose by 50 percent in two clinics and increased by 24 percent in one clini (No change was noticeable in the seventh clinic) No decision has been Inad~ tmiddot) continue extend or modify this Project
A Po~ulaton Council ~-----------
401 he fu~ura ro~ Lh~ ~~~01ati0n Council has to be considered in theli1 A the tasK t~ lL ahead of the ~ational Family Planning Program At pesent tile officil~r(QSrJ1Tl is prirnarily concentrating on two objectives (a) tIlE excpound1sinrt of fmd plannin~ services to tie remaining 58 health centen cLJs as rapi(ily as possible and (b) the integration of family planniT g VI tr MCH services Thus thG administration of family planning serviCHJ will be merged into and become part of the Community Health Services Since t is ()rganizationally undesirable to disturb unity of command a separa1e elteecutive agency for the administration of family planning services is preempted within the existing policy framework An executive role for thp Pcnulc tinn Council is there fore ruled out on this consideration
402 If the Population Council is to function as an advisory body at the p()Lic~ aId progra1l pLilnni-l level snd not to concern itself with the minutile If program execution there wonld be no advantage in giving it a statutory stltuS But if it were the policy of the Government to set up a verticll )middotro~ram for family planning ii th a field organization separate and distir~tOroll the HeaHh administration it would be quite appropriate to establish an autonOiTiOUS statut()y a~fgtny ntside the departmental setup of the MinisiY of Health d~b a budi~t md staff of its own commensurate vith the rE spo lsi hi Ii ty to be rEs j Freed from the usual departmental conshystrailts ~n the matters Cif sp(ndlng a1d hiring and firing of personnel such an aglncy c(uld move faster than a heavy-footed departmental formation wi thin a Mins trl bull Hovever a hody of this eharacter would need to be cas t in a cliffe ent m(ld than the present Population Council The shape that it would take lrould be more like a Board of Management with a full-time Chairman or Execuive Director and with more functional expertise than representational charater But an advisory council with an autonomous status and no responsishybilit f( r lrogrrun eXIGulion iould be a source of friction
403 r~e existence of the Population Council as an organ of policy advici has certain advantages Firstly it is a forum for developing a national poLicy in which officials and non-officials participate Secondly it pr )vi bulles a focus to ti1e official program vhich it otherwise may tend to lose as ~ontraceptive services are merged into the general health services Thirc lymiddot- and this is important -- the Ministry has extra-departmental advice availabL to it~ but the Ministers constitutional responsibility for the condl ct )f the national progl~lt~ le1lains unimpaired
404 ls an advisory Q(dy the Population Council should be more broanshybase( than it is at present For instance it should include representatives of tile organizations of employers and vorkers associations of the medical nursngmct teaching professions and organizations for womens welfare The Counil should also haye a social scientis t on it On the official side the
- 9 -
Permane It Secetary and the P1O (fen and FP) should be brought into the Council he inclusion of the Permenent Secretary would open a channel of communi~aton with the MOR ae the highest policy level next to the Minister and would (ontribute administrative expertise to the deliberations of the Cou1ci1 ~m f icili tali 5 (pleuenrti)D of th~ recommendations of the Council within the -rni and in OUltL depa-cments The inclusions of the PMO (MCH and FP) wOlld el) emphasi ~2 hs responsibi lity toward the family planninR program Some officrs of the HOH (eg Chief Health Educator Principal Nursin~ Office e) may 111 ea~e to be members though they may attend as requirE d nmiddot the agenda before the Council A representative of the Ministry of Fin nee stQuId be inc~uded in the Population Council This would make for a lettr appreciation of the needs of the Program in that Ministry and fadIi ate fj nancial sanct ions
B A~tatutory Council
40S In the foregotng Pgraphs the view has been expressed that within th edsting policy framework an advisory Population Council would be more tli)prcpriate than a COlincil wi th executive functions and powers that an advisory rOUlcil would not gain by having a statutory status and that if a statl1tory body 5s to be set up in lieu of the existing Council it would need tC b structured more Iiice a Board of Management than a council wi th a repre13entttional charact~( n the latter event the statutory council should have fu 1- time Executive Chairman or failing that an Executive Director functj oni1g undel- a Chairman trno can devote considerable time to the business of tlw COlncil
406 T1e Statutory Council should have its own budget with full operashytiona pOlo1ers It should have the authority to appoint its own staff and regulLte their conditions of service If it is constitutionally possible the Couner1 shollld be outside the jurisdiction of the Public Service Commission in pesornel matters
407 As an instrument of Government the Council should be subject to such ~eUfral or specific directives that the Ministry of Health may issue to it frcffi ime to time This should be written into the statute under which the Cmntil is set UD
408 The composition of the Council ould depend on the functions assig1ed to it It is suggested that the Council should not concern itself wl th the delivery of cliric selVices in the field The Ministry of Health may (ont nue to administer rampmily planning services at Government hospitals health cmters and health offices and the voluntary agencies should run thei] OWl ~rogram The following functions may be handled by the Council
- to shy
s rrogram plannin and target-setting
b proram monitoring and evalllation
c wiL of d 1ci(JTIdnCf by inspections
d Qrg8lizatim 0 es and marketing of contraceptive J~1J-s BLl (iV es at subs idi zed rates through es tablished 1 2 d(~ channel
e information mass media communication and audiovisual ublicity in the field
f prorrotion of famil~r plannIng acceptance through face-to-face cotlmunication by poundi eld workers in domiciliary visi ts
g trIining of personnel
II pr )motion of -esearch enJ
i financial support to voluntary agencies providing family planning services
409 n Statutory CCii1cil may corsi5t or an eminent non-official vith a comri tm ~~1t towacds foJlily plailninf nd the fol1owin~ members
I ~ bull Pfrmanent Secretary ltl-tIlH
Chief Hedical Officer HOH
i Principal ~ecHcal Office ~mH
d Pilhlic RellltionB OfJte(middotmiddot Prtm~ Ministere Office
A represen ta ti V~1 of the Ministry of Education
f ~ representative of the Ministry of Finance
g A representa~ive of the FPA
h A representative ot the C1AC
i H social scientist fcum tle University of the ~Jest Indies
j Three non-officials with experience in management and administration and the
k Director of the Family Planning Program - Secretary
- 11 shy
The COUlcil ITIltW constitute cOlClmittees for Finance - Accounts Personnel and Sup lies nd Stores ir~whi ch )nly members may be included Other commitles sc1h as those 01 training info1nation and education and researCl ara ~valuation r1ili also include experts from outside
410 he Off1ce raquo) cc im Panning Program which at present forms part of th ~Hnis try or [i n should be placed under the Council and its staff strelgtl ilcn~ii2 i~ r181 it may cease to depend upon the services of the Mir is t y of H~alth
C Office of the Family Planning Program
4 11ollwther the Offic~ of the Family Planning Program remains a part of the Mirisry of Health or is transferred under a statutory council if one is set uP i needs to be strengthened to meet the requirements of an expAndshying pr )gn m At present the following sys terns need to be ins ti tuted in this Office
a a 3ystem of setting annual targets for the enrollment of acceptors and the projection of service fadli ties in relation to these targets
I Ci ~ystem oE V)glC loHitoring (the monthly statistics flowing from the clini~s c~iiiain unproc(~s5erl for months)
a system of program evaluation eg demographic effect of tte program cost studies
1 an overall design for media communication based on a study of the reach a~d cost effectiveness of different media and the effect of the meflBsge content and
e a m88t~r plan for training which would comprise an assessment of the training needK of the existing staff and future reshycruits and a long-term plan divided into annual programs
412 Th2 Prograll afiie s~lould have the services of a demographer and a meeia expert A training adviser is expected to be provided by the PARO
413 1be Program Office should evolve schedules of field tours to overliee field operatio1s E~1eh health cente heal th office should be visi ted peridicaLy by the Milt~dical fElce- the Nursing Officer and the Health EduCltoI who should guide and assis t the local staff in carrying out the progam Their tour notes should go into separate dossiers for each institushytion and ~ach dossier should have basic demographic data about the area coveled by each institution These dossiers would be a useful record for revilwing l)errOmance The staff of the Program Office should be augmented to Ol)erte this control procedure
- 12 shy
D Decentralization of Powers
414 ~hete is a concentration of administrative and financial powers in the 11in s try of Health I-JllJCi1 results in an accumulation of references in the Miristl) and delays n field operations Specific powers should be delegated ~o (a) the PliO concerned with MCH and family planningmiddot (b) the Directcr o the Program Office (c) the Regional Director and (d) the County Medica1 Oficecs The Ministry should invite suggestions from these officers and wOlk 01t a schedule of delegated powers
415 A tdgh priority in the matter of delegation of powers is to arm the Regiond Directors with sufficient administrative and financial authority to implement with expedition the health and family planning programs of the Ministmiddoty 1 thin the areas in their jurisdictions
E Integration of Family Planning wi th Haternal and Child Health Services
416 At present family planning services are being provided at 48 Goverrnent hospitals health centers and health offices by using the full shytime E taf cf these institutions and employing part-time (sessional) doctors nurse~ anI clerks where necessary At 29 of these institutions separate famil cl~nics are held on specified days in the weck some being doctor sessi(ms mel others supply sessions run hy nurses and clerks At the remaining 18 imtit1tions family planning services are combined with antenatal child healtL cr postnatal services The Family Planning Association runs 8 unishypurpoe f am ly planning centers which provide daily services and contribute a 11 t le less than half the total number of new acceptors per year
417 N assessment has b~en marie of the effect of integrated MOl and famil~ p~ nnning services an the recrl1i tment of acceptors nor were ~ data readily avallable for this purpose It may be observed however that in a situation of shortages of trained personnel for health services utilization of the existing health staff and facilitieR for family planning is inevitable parU cllLrl y in the interior where such shortages are more pronounced This underlines the need of evaluation of the integrated xai and family planning progtam for its impact on the number of acceptors Also a study needs to be made of che utilization of medical and pilramedical manpower so that it leads to bdter ~llocation of duties and optimUJl utilization of personnel
418 ile integration of faMily planning into Mcn services has certain advalltages as well as attendant risks The advantages are
a Lbe association of family planning with the care of mothers and children helps project a benevolent image of family planning as a program of family welfare This creates a
- 13 shy
1imate favorab~e to the acceptance of family planning aa lt p-)si tL1e il-Eare rreasure rather than a negative program cE limiting c~ildren
h t elps erlist ~r2tion tf doctars and nurses who as c -~ass enjo tft~ Y)er)et~ a~d confidf~nce of the communities i712~ Eerve
c ~ieD of contact with women
d luni-purposa clhlics for ~lCH and family planning services are onenient for motn~rs who would have to travel considerable (listances to the clinics
e hete is better utilizat1on of Acarce heAlth manpower
419 he limitatio$ of integrating family planning with MCH servicesI
are the posiOili ties of loss of focus on family planning as a high priori ty prograrr ald the diffusion of pol1sibility for its implementation These could tlow ve r he safegurded agaifls t by adopting the following measures
a 11e job descriptions of doctors and nurses should be rewritten 0 include the family planning function
b hE perf0rt1iai1ce of ctoltors and nurses should be judged as much )y tbeir inteceq t in planning ~vork as in maternal and ~hjld care and this should he lade known to them
c )octors and nurses involved in ~CH services should be given middot)rj entation and traIning in famj ly planning and their interest 3UEtained by refresher courses seminars meetings and supplies of literature
d Thl techrical (xpert~ in the Office of the Family Planninl Program should maintain liaison with and guide the field agencies in implementing the family plannin~ program For this purpose schedules shoul d be marle out for periodic field inspections
420 It is suggested that the working of half-a-dozen centers where family plbnnLng services have been integrated wi th MCH sessions should be studiei for ehe purpose of standardizing the methodology of delivery of servicl~ Such a study should include staff strength patient load recoril shykeepills 10middot of patents in the clinic timing and frequency of clinic sesaios ani convenience vf patients
F Voluntary Organizations
421 I i~ internrticri31 expedence that the birth control movement is pion aTC tt volunh[~ JilC S Qltl that hen the national governments step in wi tl cmbi ti 019 prjhns wi thin the sLate welfare system voluntary bodies ieh tteir limited ilsrluces restrict their service activities and shift the emplasi i 0 educedgt (f the community training research and contracepshytive Sf vic not 1l7gtilflblr in he official program or in areas not reached by it In nagni tude and expanse the of ficial program in Trinidad and Tobago has alrad~ orertak~n Ce 101umary program Increasingly it will become the domLnart tartner in the total national program while the voluntary agencies will cOltirlU1~ to receive financial support and encouragement to set up high standaeis If service and explore new areas thus acting as a stimulus and an additi_e tl the official program
G FrOB-ram Infomation
422 Thre is no concurrent evaluation or monitoring of the Program The daa or lq72 flowing in from the clinics month by month have r8Jllsined unprocss~d tn the Program Office The official Annual Report - 1971 Sums up th~ poition as fcllo~s
ITThe Research and Evaluation component continued to be the weakest in the Population Program Although a systen of evaluation had been built into the program the follow-up procedures for analyzing the data and for correcting inshyconsistencies are inadequate Requests were made to extend the staff to establish a more viable unit but by the end of the year no chllnges had been made
423 T1e recording and riporting jJrocedures were revised effective Januery 1972 and there has been a further change recently at the instance of t1e Evaluation Adviser Under the system now established the clinics are lequ Lreurod to maintain the following records
a Family Planning Clinic Case Card - New Cases This was introduced on January 1 1972 and has thirty-one entries giving age parity contraceptive listory pregnancies socio-economic background ource of family planning information and agency for notvat ion bull (Annex 2) The case card is made out in duplicate for each new acceptor and a copy sent to the Program Office
b Daily Regis ter This fs a ne~gt1 form recently introduced in replacement of the old regis ter and is preparen
- 15 shy
ie) ruplicate the original to be transmitted to the Program (fHce and the carbon copy to be retained in the clinic Th~ is a very 121zborute form requiring 36 entries to be aa~ for each Chse nel and old attending a session includin~ (ntries to cit L to contTaceptive supplies issued
AijCleX 3 T~13e fcnnG are required to be sent to the Program lffce in i7JO balches every month the first batch for the i IS fif~eeL days and the second for the remaining part of hE month The trtention is that the data appearing in the ~EZlic daily legis ter forms should be compiled in the Program Office and fed back to the clinics Although it is claimed that this new form has been pretested and is workable ex)erience alone will show whether the majority of clinic cL~rks are able to cope with it in a busy session
bull o now-Ho Card TIlis card is intended to keep track of ac ceptor--It has entries for name addresfI and month fcr which a visit is due for each year
bull Aphabe tical Index This is a card index of clients with aidresses
Each i)at en is given a simple clinic card on which the dates of further appo~utnli rc3 an~ indicated A special fonT[ has been devised for the reporting ot cases unler the Post-IartumPost-Abortal Education and Referral Program
424 J system of monitoring progrRm performance from month to month need to bE develQped as a high priori ty The problem is not so much reshycord ng mc transmission of data by the clinics but its aggregation and proclssi ng in the Program Office every month which at present takes a long time The Statistical Officer should have a statistical assistant to help him Ln I he taflk Monthly progress reports should be available to the Mini H t~ n H(llllth and A11 offt eerlil of the ProKrnm Office so that remedial ac tl m I lAY h(~ tuk~n n rll1u- WhOnh1f ~Hfl(AlJtlaTY
42 For the analysis of data and evaluation the Program office shouln haVE th(~ full-time services of a trained demographer
H Field Workers
42) Tie Program nemiddotis tne services of a cadre of field workers to enr)ll neii aceeptoTs follow up acceptors in their homes and revive the int 2remiddott of dropouts Such a category of workers could also be utilizerl for pr1fficting other health programs such as the VD campaign and the inmuni~ation program
47 As an experimental measure one field ~]orker may be assigned to a emi l~ of Hi 000 population This would mean 100 field workers in all
- 16 shy
Earh of the workers should preferably have harl a higher secondary education otherwLe 1gt junior secondalY education They should be married persons with middoti1ltt mot tl-an two or tlree children recruited from the locali ty in which they armiddot~ requlred to function Only persons who have the capaci ty to comnunl at~ and or6anl~e should c chosen A months ini tial orientation
slcu1d enable them to start functioning in the field though reshyfresher CO rSeS tvould be necesslt1ry in due course In Port-of-Spain married mer~ a1C women may be employed on a part-time basis
I Hanagement Study
428 A nanagement study of the Family Planning Program should include a sctu iny of the top m~nagement Atructure (Population Council - Office of the Fanil) PLanning Program - Principal Medical Officer for MCH and Family Planni Ig fetices) the field structure for the delivery of family planning servics (Re0ional Director - District Health Services) including the utilizlti(n if medical and paramedical personnel for adding the function of del ve y )f family planning services and the control and communication proCed1reF Lfnking the top management with the field structure
429 The management consultants may study the functioning of the Popul tio I Council and advise whether it adequately serves the purpose of givini po Licy direction to the Program and if not what changes in its compo itt m and operating procedures may be introduced without altering its bsic craracter as an advisory agency The consultants may suggest an alern at ve form of organizati)n and utilization of personnel which in thir p nion may be better adapted to the needs of the Program
430 Irrespective of whether the Population Council is maintained or it is replaced by an agency of a different character a formation like the Offic of be Family Planning Program would be necessary for the administrashytion i)f 1 he program a task for which i 1 appears inadequately equipped at preselt Its obvious requirements are in the areas of program monitoring and el7alnation program supervision communication and training The manag ememiddotlt consultants may study the structure and procedures of this form~ tio Gnd make suggestions with regard to the augmentation of professional and ~ upp)rt lng staffgt and modification of operating procedures
431 The linkage of the Office of the Family Planning Program with the Miniutry of Health (Central Office) and the District Health Services should be sudied In view of the policy of the Government to integrate MCH and faI11iLy rlallning services it should be examined whether the Principal Medi al Officer for Communi ty Heal th Services (MCH and Family Planning) should be agtpoj nt~d as the Chief of the Office of the Family Planning Program and an adTlilistrative officer of a suitable level inducted in that Office to assist him TIle implication of this suggestion is that the head of the Family PlanJling Program would control the District Health Services
- 17 shy
432 rf 1e management consultants should examine the delegation of adminshyistratiie Bld financial powers of the Ministry of Health to different levels of Progam aclrlirdstration viz bull PMO Program Office Regional Director and County ~djca~ Officers
l33 he system of 01 af Togram information from the clinlcs to the Pr()~ra1 O~fice and tOile processing and use of information in the latter office iholld )e studied
434 he working procedures at the integrated McP and family planning clinics shnuLl be studied This would involve a study of each stage which a clien tpcticmt has to go through from the point of entry to the point of exit after receiving advice service or supplies This study shoulci lead to star dartization of procedures and functions and evolution of -lork norms CognatE st tdies of the working procedures at uni-purpose family planning clinics and su~ply SEssions should also be undertaken An essential component of these ~ tad ~es would be to examine Nhich functions currently performed by docshytors lealh visitors nurses and midives respectively hav~ become so roushytinize ttl it they can he relegated (0 the next 10Her level
435 Reated to working procedures is the problem of job description of medcal 8nd parrunedical personnel involved in family planning from the centra i tc the field level This job description needs to be studied wi th a vie VIW8Id txaminiDg the uttlization of skills and allocation of time by the staff lcc(rd~ng to the functional prj ori ties
436 frV management consultants should study the workings of the curren slralgements fOJ family planning counselling under the Post-Partul11 Post-Abortal Education and Referral Program at the Port-of-Spain and San Fenaldo General Hospitals
437 SU1ect to the ItBrcement of the Gove1nment the management conshy8ultal ts ~hOLlld undertake a study of th requirement of field workers (home vinitcru) in tmtlUI of are nnd population cov(ra~e
ANNEX 1
Names of Persons Met
Ii Mr T C Taitt Pem1(H~nt 3~crtarY) Ministry of Health
2 Dr M n Henry Chitd Medical Officer Ministry of Health
Ellubeth Quam a Prindpal Medical Officer (1S)
4 Mr G Z Jaine ~ uJiector Population Council
5 Dr Norma Andrews Medical Officer Population Council
6 Mr Jc~n Coury~ Evaluation Adviser Population Council
7 Mr A Jriseph Principal Statistical Officer Population Council
8 Dr C 0 Colman Country Representative Pan American Health )rg ni~ation
9 Mr ranca Kippel Health Education Specialist Ministry of Iea th
10 (1 bullbullines Principal Nursing Officer Ministry of Health
11 Dr Mx won (formerlyHinistry of Health)
12 M3 late Carops Ex-Chairman of Population Council
--
4i 1_ middotIIlt F-ntCWclOotf_Y v OJ t tl
GOVIIlHMEIgt(I OF TINIOAD AND TOampAGQ - NNISTJY OF HIALftf AIJIE1 2NATIONAL FAMilY PLANNING PROGRAMME
F MIL Y PLANNING CUNIC CASE CARD - NEW CASES - NFPPl
li ~~___ 1 ________
~ ecll-U
-- --------------------- shy~) ~~middot~------------------~~~~~~---CIJ------ middot~ii--middot-middot----middot-middot---middot--------- shy
ltv Writt N_ 01(111________________
a ~4itiJtmiddotl_____ ilIIIltIoI~____~____~-__----- shybull ~4
fie l$ - JO tDql IIfIA- tr-JMimiddot _ iJ 1 Odoor o
14aorielaquol_ _~ 0 lio witIleo-La ~ 01 bull - OJ ( _01 1~ltgt1lh o bull- 0$
AacJcu 0 2 CIIriIWA 0 J Os 0
Yv~MONTH ltnollOf~nfIGHTI
Undu 1100U$ Utgtdn 5SCI Undu 11200 01 ~ 50 - 9949 amp100 - 1199 02UlOO - nn9E~ (
0)~ 10- $99 SiOO -- U9~ lOO -- U99 12400 - 1359)-------_-r----shy ~l)o SIS n600 - Hm1300 -- 019 OJ200 il~9 ~------ 99~ a 1)0 m Os1)00 -- l99 1400 -shy $4100 -- 1S999r--- shy
1500 donl S6000aad O399 - lt499I~- I 0lt
ltII
IJ -IC _~tltlioltgti lS
02 IaampJIIocI OJ 04 laM Os
w Oltwio I_-l(~u IrIaa U
h~~ ~Clubl 01 OJ
IS ~C-n 01 toSIitDI 02
Ji poundI on 01 IriIIIuy M ur 02 IV OJ
WU 10 pltIoII~ llaMtl 411 cIIiId 01 Ol it fIolto ~ do~ _14 rou IIlgtJo 1Ia1 ___~_ shy
40
It _ I 00 ~bull FPIiIJ 1
OJ 02 OJ 06
)0 III- iy wOWcf ~1
aMIIl Os
11 T 1gtlt ( h _______ 4)~
06
04 (MIbullbull middot bIrlI ~___~__~_ (-fIJI ~- -~-- (1HJ 49middot SJ
U 10k 01( 1__ raquo$-4
iU1) DOl F ToWotfOlnC DOl 001 or Do [IP 006 001 OIIgtu___Spltclty DOll Nltmo 010
U1Mo I orcpmiddot laquo55middot16
1lD 001 Foam Toblelf_ICim DOl Condom DOl CoomS~ 004 oe Oos WlttuJn 1J OIkr DSpody) 101~ ~Iu 006 Rhylhm 001 DOG OJO
no wI~lmm 4 cd
(I 0) 1110 01 Condor 03 (lorn bull l S~muoidIl 04 Faa TabioolfIIltr- Os RhyUlm 01 lnJrl tible O Advico 090 06
la slt 1)0 19 loti ~rltnlt) ([)sl or 1llOn) ____ --__ bullbully-J n SV - ~JcdS
v~ Cl NCI 0 30 OJI_O I Wr blJ1h 0 I ~ OJ 1 ~ (fOOd V 01 No 02 laquo 6) Cf4
WIiI 1 172
004 001
j D middotmiddot middot
1 ~
r
~
bull I
bullI I I
r c i
ANNEX 3 Pagemiddot 1 of 5
0 raquo rshy -lt l)J ~ 111 t G) 5 shy (J) ~ -
fT1u
i
MINISTTY OF Ho1TH
NTIONl F~ILY LNNING PR-GRbullbullM-tE
~~5tructions to C11nic ClerKa
How to co~ploto the Daily Rogister
~~ ~~v1sd Daily Rosi8ter replnc~D tho one which is now in use tb$ Monthly PC~ri rOt~ arti tho 01( Ci() Dod PollJ j f m It is a pre-coded form and 1411 cl~1p Jd tl a1I6iniul-mIHvn Oel Clinic nctivi~y
110 )rm rollt biJ coupJot)d lrl cupLtcoto using a o(roon shoot Tho top aheot or oriinai ~ust bl) 6(Ult to tho CQgt1tral O[[lCO and tho carbon copy retained in the Gliaic rilo dll the for6a that ar uD~d betwoen the 1st 4nd the 15th of the oIIollth aut bo subClittud tocho office 35 Lnc blttch Those oomp1cted betwoon tho 16th _lid tqemc of tho month must bo ~cnt in a secJnll batch
P lOvLior hns boon Illllde for 25 clients on cZlch forlll new forlll must b IIlied f r poundh 50[810n2 whothur or not ono or lIIore session are hoIdiit the clinic on he sarne day
I th ro alO more htl 25 clionta 1n attondnnco at tho session the additi shyOhAl m~bOl of clionts 10 clients nu~ber 26 27 etc sh0u1l be ontered on the next Imiddotrlll ~i ttout a1tpoundring the numbtlrs in the cvlumn hond Series
51 ppOfil th~ number of aUcnts lQr that session ws 5 this would mean thllt two rJlS ~ lst be 6ubllIitt~dl the first filled uF 1 tltgt 25 And the laquoIncond 1 to 10 Th~ cal bon ofies should bo st~plod togother at thu t0P l~rt h4nd corner of the torm ard ktpt in the Clinic filo lou IIlU6t stapl~ the originftls in the 8~~ monnshyer for lIub~ssion to the ofticl
ie h~ ll idontiflctior- (cc 1 - )
0 lot Ji 9 anythin~ hGro poundhia is int(mdClc for tha computer code
2 ~~pound~ - Print clOflrly tho name of your Clinic
C1Lic Huml or - (cc 4 - 8) Evar1 Clinic Numbor has 5 digits Virite each dig t il a t$purate box
It Pai~_thllsectgdllion (00 lt) -1 1) - Dl monll 10M
lw) bolte IlrO proY140d fetr olAoh pr 01 thQ dISh Enter tho dA) ldns a R
d16ih
emiddot5middot (0 11 I for 115t ( 0 21 for 5th etc Treat month the am pay
e ~ 10 ~ I for I-hrch 0 [2] for September Tho y~nr must be (into ad
I Z I ~ I I 71 q etc
Take as in IixulIple tho dOlte 3rd tllrch 1973 7~ie must bo written
[0131 LSLDI[7l3JDny Month Ye~r
5middot 1~J $~~ - Irom ~-------- To --------shytntol hOI II the time the Clinic 111118 in SW5sion emiddot8middot
(i) 11011 500 lm To 1200 non
(11) Frclt 100 pm To 400 pm
(iii ) IX-OG OO pllI To 6~00 pm
f
2
ADEJ ) Paae ) of S
6 Eov
_ 1hA 1gtIpoundC iIIUlt be nu~o7Ifd tler1ally 1 throurh n lU tbey Are Wled In ~1l8ellJ IInel 1301 tlU 1 Orcl 1 Wled tor a o5038ioll - -I 2 tonY tho _boul~ b I1WJbtl 1 and 2
hlrlll are 25 linos OIl the fOnl Ilnd thoae muet be UBtleS for 25 clients 9 one ior bullbull 01 I ini
ot ~h lc II ol1cM lOlivpound til e linic before soeinc DurOI or doc tor ilnc ii hox rristrltltion nUlJbet had alrearll been recorded on the Dai 1y Roiuter then n line ~hollld be drawn through that entry an1 the eliort nust not 06 includttd in tho totals tor that 0eDion
1lw Ileifitration Num)~r of cueh client must be IiIritten IS n 5-dlrlt oode ClhnC IH11IlElr 315 1IIU8 tborotore be enterod 18J010117]5]
~ Clt ZOt
Coda 1 Codo
10 ~tl c 2t j co 21)
~w elSe - Coda 1 0) d CltaEl - Code 2 Revislt Code 3
Only pound1 01 theBe coiles may be usod
11 prol-O~ ~Eil~1 (cc 22)
If ma climt was L drop-out IIho haoS returned now to the Clinio tor tho first no linmiddot bullwin lt1ro1eo o t he or she should be given CCe 1 It this do 5 II It nprlly leu this colWlln blank
u Hothod middothisllill loe 23)
NOh til t otly ~ Cod 16 tp he ontered in 2lpound of the columna oven thOUGh 10 co11lllJlB 10 provided on the torm The Codes llrol-
Oral Contraceptive Code 0 1 U D Code 1 Condom plUD Codo Z Condor (only) Code 3 Foum tAblets cream Code it DitphrClGJII Code 5 Rhythm Cde 6 Injectible Code 7 Advice Code 8 Other Code 9
It for middotDo-le 1 client rlllll ji yen cclldorls ord foam or creall Iou Qust entor Coole i (condom plulJ) in the appropri~te column This Quat be the only lIotmiddot) tarcie If an in the cnse of a tlnle clinic I the client is Bup)lieu lith COIlOrW only you rmot entEr CorlQ 3 (cpndolll) Do not use a ticII ~ tho (odo Nwber
It is CUi tomary fur 11 cliont 110 is beine put on the oral contraceptive for the first tiT1o and even on other occasionn be issued condoms and 11 crelle or foam a Ilell rI3 a pgtcket of pilla In such Cllses when the piDQ Ilre Ilctually iouou you tlust record Orll (Co~e 0) 08 tho onll metbod ilo othor ntry sll0uld ho nnrlo
Uovever n SJC~ canas vucru condoms and fOHa ~rc eiven but no pilJa (even thoJRh _t _n the intention to issue pills nt the noxt vioit) than the Mothol Th5 ifli t ohoulcl be recorded uo Condor Plus (Code 2)
13 Seen Bybullbullbullbullbull
~rot S-1 SO l
Doctor (Dr) - Code 1 j Nurse (Nul ) - Code 2
Clark (Olk-) - Code If tho Clhnt is vcen hy both tho llootor tlnd the Nurse enter Code 1 t Doctor It 6~61l by the Nurso only arite Code 2 Cod bullbull Cerk is l)llnt for FA Cllnica Clerks in tho Government Cli1t hiwo Llttoll istructed not to i56uo supplios on their own volition
14 fl221~
lhio S~tiCl of -Ie fvrtl t~ke 16 (llrci coluMna (cc 25-+0) nnd 10 tho only part at th iOIQ in llich iore thAn one cod is Zlccoptl1blo Tho purpoco of the )ecton is to 0 able to arrive nt the Cjunntity of 6tock dilltlitJutshyed YOI IIlUdt writo in the CllllOjH-iata colulna the nUllbJr of Il1ch 4rtic1o i~JSu~d ~lo e ha I Oral Contrcilpti vea are aub-di vi dod into types ae_ 3 PIllCKC 9 0 Elynnn LlUot be entered Codo in card column 25
If tor eXllrplc t l cliunt is iosued wi th packots of Zucynon nnd aJ(1 ~ivn 1 conuotll (8inoloo) you ouot enter in oard column 25 and 11 It
cnrd col~8 )2 and J (io 1 in card colucn 2 nnd 2 1n card coluun 33) Nota C)lldoIlU ale to b(t ruoordod individually not os packots of throo) Should n ne LlondoClo be isoued thil3 is to be rc-Qed as 09
If It clint 6 t~ot isoued Blly lIupplies thon you must writo Codo 1 in CQllAlilD 41
It Q eli nt isite the clinic to check on her LUD or her Diaphra~t IUId ro DI W 6 ppl ills nre ispounducd then Code 1 1s wri t ten in column 40
In the FA clinios here a variety ot orll contraceptiveo in orer~l tho elerll wilmiddot~ bJ provided with a specill code shoot The idontifyin coo will b wiittn in Column 29 nnd the nUlber of packets iosued in colwm )0
lralaer-In Code 1 lrllllsie r~ut Coda 2 leIllPQrArr Trnnsfer-In Codo gt
In the cao of n 2ratl8fcr-In I you lUot n160 cOrlpleto coluons 42-51
In the cllU J of A ~~emporary TranGfor-1n (an individual who i8 only v1citing fur clinic tor some epecial trcatcont hna who will bo rdnlnin
~middot(II~~~fO~l~SIl~I3~nn~~~h~rO~nh~1~~190~~nll 2-46 and ler rei IItrntion numbu in colullnll41-51
It the oli( nt i iNt a CrllnoforwIu - Out or loClporu1 tMn loave oolumn 1 blank
16 lr4nst(gtr-tl2~~morrry TilJnder-In (co 42-51) Forl1ltl CUn E1~ (cc 112-46)
hen you rei iatlr L irllsfcrln or Il TJlporary Trnnsfer-In you IIIUBt write I ere the five-digit clinio nucbor of the Clinic iraQ which tho ltlient Me (uIlO
2mer ]letr ~2n ~ (cc 47-51)
frlta fllao Clo r-~itrlltion Nuc~Er ot the client in the Former Clinic (i c bullbull th 1 Sis rnmiddotion ~UlIlh()r which the client carrics 1n the tormor clinio) bull
It tho Forrltl Ho( ist rntion Number iIJ not readily wnilnble you tluct oocpluto thtl epcciol [orlll Transfer-In Not Identifiod Dy Forrlcr RCGi(trn~ t10n Nwlbvr Or ~ flt)rCl is to be cOlplctcd for och cnso nnd th forlJO Ilubmi tted to thu )opllntion Prorrnnme Of fice tOGether with tho Dily Ro~iBtors lhwev~r should the clork leuTI of tho clint B FormlI Uocintra tion lUlllb r )0[(10 Cubmi ttinft the D1ily IOCI otro t hen the nUQbcr shoulo bo -ri ton in colucns 47-51 lna the special foro should lJo deotroyotl
l7 bullbullbullbullbull
r lt bull bull
ADXI ) Pap S ot S
11 UD LV~ (cc 525)
It tb( cliont io ~ivQn An IUD tor the firot tl~o then you should Sri to Codo 1 Inuort ill colurJI 52
It tho olimiddotsnt ia rvinGgtrtltld i th An I UD bullbull tben wse Coda 2 RelnDltlrt shyin (01Uil11 52
It the clLmt is ~tte~~dint chnic beruse her IUD CflClQ out by Haol (cxpll Iion i ~hcn fir te todo ~- UIlllrli1 53~
If c-ltr IU fj IIIS reov in -ne cllnic by tho doctor or nurso t~on vlritI Codec in column 5
II the eli nt otends eiLlie tld explin[l th(lt she rccovcd the IUD tlllleel nen write Coda H in Colwlm 53
It the IUD jr still within the uterus nd the WOIraquoI1 1 11rc6llJlnt thon lIrite 1gt40 4 in Column 53
lZ np h5t (ce 54) It 0 Pull 5mor ie t~ken durin thi visit tben Codo 1 ehould be ampDtere4 in ColWlln 54 Should he c110nt lltt rQ(uircd to rttturn to clin1c for a rogtol1t Pnl) t06t then CoLe 2 llhould bo middotwrittcn in column 54
It no Pllp Scou io taken tde visit Itove colUQn 54 blank
Iraferti1lli (CQ 55)
Ii the e liett io nl1 infortili tr eaoe use Cor1o Ill in colUQn 55
If tbia 1000 not tlpl lonve column 55 blonk
20 Totaltll
CO~1ploete the [)ldegO 1gty puti YI tne totals betweon the double lines nt tu b()ttctl Carrj colUlllnc 20 21 nd gt4 Must hlve tho Bnoe JllIIber and thiG Would coreslonc to the numocr ir attencbnco
Writ$ th to1ul nUlllior of Drop-Outs returned (c022)
Urito 41eo tb totnls fOJ each card column 0 to 9 under tho h(adinu Method thiB Vioit Show tho tote L fgtr OlCl type of contraceptive issued (cc 25-40)
1)0 Dot wrLte 1111 totll lUl(Ier Card Columns 15-19 29 41-51
21 COPmllh bull ~lt h~t~ Monthly ROilort
OQ thG DaLl oCator forlll thnt ccrrOspOldB to tho 1(8t 1$06610n lt 0
oth yo Olllt (vwlgtleto the items nt the botto of the [orampl This is tour ontll~1 n(olt nnd includcD tho totll lumber of sesions Ilntl tho total Iluolcr ( r crop-outs durinr the Qonth
An tiUlsilt n drir which n doctor liB in nttcndnncc is a doctor sOfll~1on and shoulc 00 re(liGtcnd in coltns 56-57 All other sessions 1116 conlliid~recl supply stllciona and thtlY 1110 rocordod in columns 58-59
the total Ilum)nl Jf drop-outo ld the drop-outs by method durinc the onth nre 10 bu oltorou in the inrlicllted boxes
72 Chad Your ~
Milke I ura th t all thE fijul4gtu rre c101r -tNever writo our nutlUQrS 50 InrjEl that they oxtend out of tho
ap~rotr1ato ~ox
Cheek to BoJa tht 1111 numuors 1110 in tho correct boxes -- CJslHloially when Writi1 the totlB
Mllxe Cirtc O thmiddott t1e infoT1I1ntion i6 clear on the corbon COllY before sep rmiddotinr the sheets
Jitn the Fomiddotl lien tly sien YOUl nr me 1t the bot tOil right hnnd corner btl forc subol ttinG it Keep tle CL rb n copy for your rocordn
i
-l ________~~---------~
I _1
Adminiatr-atlve SKVieu
P inba ~~~l1cal lrlnbin~~eltltcal -1 te~ra t~~rvicc (lnatittloaa)
--1- - shy -1------------_-L_ l-r-aJiil- shy _-L_tet1lal d
PlIinm1tJ8 atdUon DetalMid H8Il1tb ~ ________bull Care
-----~ Office of i
the FlIily _IPlill3 roarshy
1- - - -------RegiatUll urnr
ltIi 1 Drelttor Rcgicaat Director Souta Tabqo tacallortb ~ counu gt____ ~ (4 ouottet)
Off1ce of the Res10nal Diractoc L
r----- _L_ -- shy i I bull IREgional Ipitl I
District IIttaltb I bull Othn RelOl ond Hcpital CenteIntt itlt j In 1__ _shy-~- ---- -_j
J r Ii~lth
C~nlef
L
I Ihnlth lie I th Offlcu (1ft lc~
Coullty 1I0p1ta1
Henlth tentet
I

- 2 shy
202 In pursuance of t l= foregoiny decision the following terms of refer nce were framed for the Po1)ulation Council
10 i~vll ditcoction to a Family Planning Program fo Y ltdd cHl T0bagn d th Ii view among other things to eo ~ ~c n lfllonrdnr activities in the
203 A PTOlllH~ f(cibor nf ttl rredical profession was appointed as Chailman llei the lill~1L y h2 jiamily Progran Ministry of Health as the Secrltar r (r th C~-ur~ ihe membership of the council comprised officials of tle t-instry of He3ltii and other departments representatives of the volultary agencies operating family planning services and leaders of opinion the present Chairman of the Council is an eminent gynecologist in privmiddotte practice and a former Minister of Health the members are as foIl 08
1- Chief Medicnl Officer MOR -l Spcclliflt ~middotjJ3C Officei- General Hospital
3 A rEpr~senative of the Ministry of Planning and Developneut
4 A represehtacive of the Central Statistical Office 5 Public Tidaions Officer Prime Ministers Office 6 ~ PrilLj~d t1lt dq Officer NOH 1 ~e( CL bull ~clmiddot ~~t)pulati on Program H Chid ~ea~h Educatoi ~lOH
9 A repres~rltatiVE of the Catholic Marriaie Advisory Council
10 amp 11 Re~)resentatives of che Family Planning Association 12 6 13 M~mbers or the Publi~
14 Diector Family Planning Program MOH - Secretary
Olj The Population CQtJrdJ hal three roles (a) policymaking ll) I rogralil formulation and evaitllt1()l and (c) providing general direction fllr program implementation Its composition is designed to ensure (a) intershydapamiddottmental coordination withill the (overnment (b) coordination between the ( Ole-nment program and the activi ties of voluntary agencies and (c) rapport vith pblic opinion
05 The Population Council is assisted in the task of program formushyIation by a numbe of committees ~thich are so constituted as to draw upon Ihe ex lertse avalIahI wi tlin the Government as well as outside Pre-eminent arnorg heseuro commictees s lhE lati()nal tH Program fnLMulation committee ihi(h technically speakirg is not a committee of the Council but a commitshytee of the MOH It inter-meshes with the Council since it is the policy of the Government to integrate family planning services with MCH services delivered through the network or health centersoffices of the Ministry of Health This committee is headed by the Principal Medical Officer of the MOH in dnrge oE Integrateci 2~edicil Care now restyled as Community Services
- 3 shy
which COlT bull Se 11CH anii IIgt sxvl(s I1H~ other committees are Community Educaior and Publidty Cvrm] ttec Research and Evaluation Committee Family
~du aton Comrnirii ~~e(i] CCimittee and inance Committee
OS i~ n1eptUd~ i p Ni ~runi t 1 an advisory body and as such itus 10 execl1lt)ltjmiddot n p-actice the Office of the Family Planning Prog) am e tabisLecl wirgtmiddotcn tilt2 middotlnitry of Health functions not only as the ecr ~tc dat of lIC )hiCJl but also as the instrument for carrying out lis lirEctvls Furtiie ch GOtdcCU has concerned itself nomiddott merely with broal i~ SUIS f10Hc out also vL detailed implementation The majority of t le r emmiddoters of rhe Council are in favor of Umi ting the Councils role to tile givlng of broad direction to the Program
20i The Office of thl~ Fitli1y Planning PrO~rall1 is comprised as follows
Dlrcct0r (Incant) Medilal OfHceuror (Famtly Planning) Nm-~If Offieer St~tistical afficer Health Educator 2 lield Workers (for follow up)
(OIlE positor vacant)
8CCiHWlcnt 2 clexks 2 typists 1 driver 2 proj ctionis 15 and 1 messenger
T- ~ g af f of the Office of the Famly Planning Program is under the discipline of thttinistry of Health since the Population Council is nei ther a departshymfntal unit nor a separate legal entity with its own fund
2 OB The places of )nrm1 atton Council and the Office of the Family p ~anr ins Program wi thi n the Minis try of Health as conceived originally by tile Government may be seen in the abbreviated version of the chart appearing hI different official documents and reproduced at the end of the report
~ 09 In April i973 at the time of the consultants visit there was In aCIDc)sphere of uncertainty about the administration of the family planning l)rogram as a result of changes in some of the top positions As a result of t c~binet reshuffle the portfolio of Health had changed hands The Permanent euroctet lry who is the princ~al ad~liser to the Minister was new as lras the r-i c al Yedic1l Officer h charge of Commurity Health Services (Mel[ and Pam ly Pl1nnhg) The Dtnct0 of family Planning who was managing the Office of middothe Family Planning Program and also serving as the Secretary of the PoshypUlition Council had reCiTed in March 1973 and a successor had not yet been named Meanwhile the Medical Officer for Family Planning (a part-time employee) was carrying out the functions of the Director in addition to her OWT Wi thin the Population Council the advisory agency for policy-making
and ccord~n8tionJ there was a groHinr feeling among the members that the ouncl1 510t1d shed thE respOJ1sibili ty for implementing the program a funeL on j ch nad heuroe added on to its advisory role with the passage of time
iO the 1 ~lp~1 the lines 0 responsibili cy were not clcay (e ned and Li1 refioal system was not fully functioning The post of Re ior 3 Director crth VIas vacant The policy seems to be to strengthen the 1St tu ion of Pt()1ic Flealth Office as an 3ency for the supervi-middot sion)pound ne district sflVices (health centers health offices and school servi ces ~l thin the ccnmty
II I PRES EN STATUS OF THE PROGRAM
301 ~he adl1linistrt~ivE changes narrated in para 209 have come about at fl tin e IJhen the P1ogram has entered a phase of declining performance as is 11 Jpal en from th colloHing figures taken from a report submitted to the Populaton Council
YrUL 10C7 ~j8 1969 1970 1971 1972
--- -- ------------~~ --~ - shy----shy
Ne Acceptors 3696 2731 16207 9997 9898
(End of October)
7560
Slur~e Family PlAnnto Program Report (no date)----AsII1Ulilg that th6 ttlrollmant of new acceptors during November-December 1972 prclrd at the 8ame rate as during the ten~onth period January-October
- 9i2the total enrollmslt in 1972 would be lebullbull than 8500
3(12 lhe total number of leW i-iCCeptors for 1971 shown in the foregoing tal11e 1s at variance with the following data from the 1971 Allnual Report
- 5 shy
~ev C~~ Contraceptive Method and Agency
nm Other Advice Total New Cases
Aeny
GovrrmenC ProEllil ___~zZ(lt1____ 97____2Lbull499___~528~___4i_750~_
Farr Uy Planning Association 2814 315 607 76
Catholic MarriaAdis1ry COLnc_H____
ge
74 88 162
otal 31[10 692 8724
_--__------------------shySOlrce Natio
1973 nal p
Fam29
ily Planning Program 1971 Annual Report April
NevmiddotrneJl~ss) the declining trend in annual performance after 1969 is manifest ana conpaes unsatisfactodly to the following targets set for the Program
Targets for Contraceptive Users - 1968-72
New Accep tots Old Cases Total
1968 20noO 20 000 lO noo
1969 20000 40 000 60000
1970 20000 60000 80000
1971 20000 80000 100000
-----__shySource National Family Planning Program
p i9
------------------------------------
- F shy
3JJ3 Ttl flient recrvitTrent has fallen off since 1969 in spite of a signif Icar t xpansinn ir the number of Government health facilities providing family paarin~ services FrCli1 7Hr to year Starting from scratch the number oE GovE(nment health irlstitl1tions delivering family planning services in isollL(Od ~ily pltJfAill~I ~J in c)lchiratinn ~7ith MCa services has lWW risEn t 4 lhis ie --tdt)p to t cii1ics organized by the Family Plannin Asce1ation bull U2 by tile Catholic Marriage Advisory Council which offers the ~h)lthm meti1middot1 nT
304 1i ciecli ne d~ d re11~m2nt of new acceptors coincidentally w-Lth th~ eXlsioH uf s-crLce facilities needs to be studied to identify the factors responsible for it eg the quality of services offered the strategy of commmic at~on and motivation and management and supervision One obvious gap is he abgtence of an agercy for promotion and extension of demand for family lal 111 If services -gt tLe field reliance being placed mainly on clinic counseUn H1d generaUzmiddotd mass media publicity The need for a field promoshytional agelcy is underscored by the dropout rate In 11 draft paper prepared by the Hed_cal Offic(1r for FIrnilv Planning it is stated that by the end of 1972 t ile Heuroe approxiclt ji rHJC cun~ent users of contraceptive methods and 33 per ert dropouts
305 rht~ program is cot merely clinic-centered but also female-oriented Recent Iy mellsages aimed at m11es and stressing joint male-female responsibishyIi ty l gtT j ecillc CImt-J 1 i~gtVt~ b~~in )7cn 1n0 the cOTul1mication activity sUf1 tv) c nts Em he 2iucaccw i milc8 and che distribution of condoms to them illVC he ~n or n~d iD r GJvefl1nenC s(~ctor The Family Planning Association has a130E~k11 the irti U3 1V~ to reis ter males ln industrial employment Tllese are steps in the ri)n dtrect1ongt but the size of the problem indicates the n~ ed OI a concerted effort en a much large r scale
306 Tre Program relies largely on the use of oral contraceptives as shown in the following table
Oral Other Advice Contraceptlves IUDs Methods Only Totals ( 100)
19)9 76 20 16207 ( 100)
1970 316 63 9997 ( 100)
1971 50n 4n 365 79 8724 (100)
Family Planning Association unpublished report
----
- 7 -
Althougr amJnp the neH acceptors in 1971 the users of oral pills were only 509 ~mon~ the old cases the figure was 119 The percentage of IUD users has remiined stagnant at an insignificant level this may be partly due to consume prefErence and pctrtly outng to lack of trained staff to undertake IlTD i1srti l7U There h hOHever a visible shi ft towards the uSe of othe~ ilettods (npchani81 and chemical) attributable to a scare about the side efects nf oral connaceptives Among these conventional methods the condom s 11 os popular
307 J t )resent fami ly planning services have been extended to 48 out of 106 hellth centersoffices run by the Government and the objective is to C)Vel t1e remaining health centersoffices within a short span of time so that adice and facilities for the practice of family planning are conshyvenient Ly wa nable to the people in all parts of the country By ann large sepanit e fITti ly planning eli nics are held on specified days as an addition to norrral lealth work Besides doctor sessions at the clinics supply sessions are rur by health visitors and nllrses assisted by clerks The nurses are authorjzed tc issue oral contraceptives for a period not exceeding three months ani the acceptor is required to attend a doctor session for advice during thi jnterval In 1971 the numbers of full-timepart-time staff in Gov~rtmnf centers renderinp family planning services were
Full-time Part-time
1elical Officers 14 8
NUseMidwives 35 19
Cl~rks 3 17
Now tile low~rnment -gtbjective is to integrate family planning services into MOl services and use the same staff being used for the delivery of both types of erlices at multi-purpose sessions However so far only 1A centers have interated family planntng with Men or gpoundmeral hpalth care sessions
3011 The Family Planning Association has eight unf-purpose centers where famil) pLmring services are available ftve days a week The Association employs tilrEe full-time and ttJO part-time doctors a complement of 14 nurSeS (who llave been trained to do pelvic examinations) and 11 other clinic staff membels The Association also has a number of voluntary workers in the clinics The CithoUt Marriage Advisory Council has three clinics but their contri shybution in terms of enrallment of acceptors is not signiflcant
3)9 A Post-PartumPost-ALortal Program was started in 1969 It is state I tlat about 14 percent of the patients reached attend a family planning clini~ 1iTj thin six weeks of the interview in the wards IhiR is qui te a low figur In 1970 when a system of home visits was tried under the Family Planning Aide Project in 7 clinics the rate of acceptance doubled in three clinils rose by 50 percent in two clinics and increased by 24 percent in one clini (No change was noticeable in the seventh clinic) No decision has been Inad~ tmiddot) continue extend or modify this Project
A Po~ulaton Council ~-----------
401 he fu~ura ro~ Lh~ ~~~01ati0n Council has to be considered in theli1 A the tasK t~ lL ahead of the ~ational Family Planning Program At pesent tile officil~r(QSrJ1Tl is prirnarily concentrating on two objectives (a) tIlE excpound1sinrt of fmd plannin~ services to tie remaining 58 health centen cLJs as rapi(ily as possible and (b) the integration of family planniT g VI tr MCH services Thus thG administration of family planning serviCHJ will be merged into and become part of the Community Health Services Since t is ()rganizationally undesirable to disturb unity of command a separa1e elteecutive agency for the administration of family planning services is preempted within the existing policy framework An executive role for thp Pcnulc tinn Council is there fore ruled out on this consideration
402 If the Population Council is to function as an advisory body at the p()Lic~ aId progra1l pLilnni-l level snd not to concern itself with the minutile If program execution there wonld be no advantage in giving it a statutory stltuS But if it were the policy of the Government to set up a verticll )middotro~ram for family planning ii th a field organization separate and distir~tOroll the HeaHh administration it would be quite appropriate to establish an autonOiTiOUS statut()y a~fgtny ntside the departmental setup of the MinisiY of Health d~b a budi~t md staff of its own commensurate vith the rE spo lsi hi Ii ty to be rEs j Freed from the usual departmental conshystrailts ~n the matters Cif sp(ndlng a1d hiring and firing of personnel such an aglncy c(uld move faster than a heavy-footed departmental formation wi thin a Mins trl bull Hovever a hody of this eharacter would need to be cas t in a cliffe ent m(ld than the present Population Council The shape that it would take lrould be more like a Board of Management with a full-time Chairman or Execuive Director and with more functional expertise than representational charater But an advisory council with an autonomous status and no responsishybilit f( r lrogrrun eXIGulion iould be a source of friction
403 r~e existence of the Population Council as an organ of policy advici has certain advantages Firstly it is a forum for developing a national poLicy in which officials and non-officials participate Secondly it pr )vi bulles a focus to ti1e official program vhich it otherwise may tend to lose as ~ontraceptive services are merged into the general health services Thirc lymiddot- and this is important -- the Ministry has extra-departmental advice availabL to it~ but the Ministers constitutional responsibility for the condl ct )f the national progl~lt~ le1lains unimpaired
404 ls an advisory Q(dy the Population Council should be more broanshybase( than it is at present For instance it should include representatives of tile organizations of employers and vorkers associations of the medical nursngmct teaching professions and organizations for womens welfare The Counil should also haye a social scientis t on it On the official side the
- 9 -
Permane It Secetary and the P1O (fen and FP) should be brought into the Council he inclusion of the Permenent Secretary would open a channel of communi~aton with the MOR ae the highest policy level next to the Minister and would (ontribute administrative expertise to the deliberations of the Cou1ci1 ~m f icili tali 5 (pleuenrti)D of th~ recommendations of the Council within the -rni and in OUltL depa-cments The inclusions of the PMO (MCH and FP) wOlld el) emphasi ~2 hs responsibi lity toward the family planninR program Some officrs of the HOH (eg Chief Health Educator Principal Nursin~ Office e) may 111 ea~e to be members though they may attend as requirE d nmiddot the agenda before the Council A representative of the Ministry of Fin nee stQuId be inc~uded in the Population Council This would make for a lettr appreciation of the needs of the Program in that Ministry and fadIi ate fj nancial sanct ions
B A~tatutory Council
40S In the foregotng Pgraphs the view has been expressed that within th edsting policy framework an advisory Population Council would be more tli)prcpriate than a COlincil wi th executive functions and powers that an advisory rOUlcil would not gain by having a statutory status and that if a statl1tory body 5s to be set up in lieu of the existing Council it would need tC b structured more Iiice a Board of Management than a council wi th a repre13entttional charact~( n the latter event the statutory council should have fu 1- time Executive Chairman or failing that an Executive Director functj oni1g undel- a Chairman trno can devote considerable time to the business of tlw COlncil
406 T1e Statutory Council should have its own budget with full operashytiona pOlo1ers It should have the authority to appoint its own staff and regulLte their conditions of service If it is constitutionally possible the Couner1 shollld be outside the jurisdiction of the Public Service Commission in pesornel matters
407 As an instrument of Government the Council should be subject to such ~eUfral or specific directives that the Ministry of Health may issue to it frcffi ime to time This should be written into the statute under which the Cmntil is set UD
408 The composition of the Council ould depend on the functions assig1ed to it It is suggested that the Council should not concern itself wl th the delivery of cliric selVices in the field The Ministry of Health may (ont nue to administer rampmily planning services at Government hospitals health cmters and health offices and the voluntary agencies should run thei] OWl ~rogram The following functions may be handled by the Council
- to shy
s rrogram plannin and target-setting
b proram monitoring and evalllation
c wiL of d 1ci(JTIdnCf by inspections
d Qrg8lizatim 0 es and marketing of contraceptive J~1J-s BLl (iV es at subs idi zed rates through es tablished 1 2 d(~ channel
e information mass media communication and audiovisual ublicity in the field
f prorrotion of famil~r plannIng acceptance through face-to-face cotlmunication by poundi eld workers in domiciliary visi ts
g trIining of personnel
II pr )motion of -esearch enJ
i financial support to voluntary agencies providing family planning services
409 n Statutory CCii1cil may corsi5t or an eminent non-official vith a comri tm ~~1t towacds foJlily plailninf nd the fol1owin~ members
I ~ bull Pfrmanent Secretary ltl-tIlH
Chief Hedical Officer HOH
i Principal ~ecHcal Office ~mH
d Pilhlic RellltionB OfJte(middotmiddot Prtm~ Ministere Office
A represen ta ti V~1 of the Ministry of Education
f ~ representative of the Ministry of Finance
g A representa~ive of the FPA
h A representative ot the C1AC
i H social scientist fcum tle University of the ~Jest Indies
j Three non-officials with experience in management and administration and the
k Director of the Family Planning Program - Secretary
- 11 shy
The COUlcil ITIltW constitute cOlClmittees for Finance - Accounts Personnel and Sup lies nd Stores ir~whi ch )nly members may be included Other commitles sc1h as those 01 training info1nation and education and researCl ara ~valuation r1ili also include experts from outside
410 he Off1ce raquo) cc im Panning Program which at present forms part of th ~Hnis try or [i n should be placed under the Council and its staff strelgtl ilcn~ii2 i~ r181 it may cease to depend upon the services of the Mir is t y of H~alth
C Office of the Family Planning Program
4 11ollwther the Offic~ of the Family Planning Program remains a part of the Mirisry of Health or is transferred under a statutory council if one is set uP i needs to be strengthened to meet the requirements of an expAndshying pr )gn m At present the following sys terns need to be ins ti tuted in this Office
a a 3ystem of setting annual targets for the enrollment of acceptors and the projection of service fadli ties in relation to these targets
I Ci ~ystem oE V)glC loHitoring (the monthly statistics flowing from the clini~s c~iiiain unproc(~s5erl for months)
a system of program evaluation eg demographic effect of tte program cost studies
1 an overall design for media communication based on a study of the reach a~d cost effectiveness of different media and the effect of the meflBsge content and
e a m88t~r plan for training which would comprise an assessment of the training needK of the existing staff and future reshycruits and a long-term plan divided into annual programs
412 Th2 Prograll afiie s~lould have the services of a demographer and a meeia expert A training adviser is expected to be provided by the PARO
413 1be Program Office should evolve schedules of field tours to overliee field operatio1s E~1eh health cente heal th office should be visi ted peridicaLy by the Milt~dical fElce- the Nursing Officer and the Health EduCltoI who should guide and assis t the local staff in carrying out the progam Their tour notes should go into separate dossiers for each institushytion and ~ach dossier should have basic demographic data about the area coveled by each institution These dossiers would be a useful record for revilwing l)errOmance The staff of the Program Office should be augmented to Ol)erte this control procedure
- 12 shy
D Decentralization of Powers
414 ~hete is a concentration of administrative and financial powers in the 11in s try of Health I-JllJCi1 results in an accumulation of references in the Miristl) and delays n field operations Specific powers should be delegated ~o (a) the PliO concerned with MCH and family planningmiddot (b) the Directcr o the Program Office (c) the Regional Director and (d) the County Medica1 Oficecs The Ministry should invite suggestions from these officers and wOlk 01t a schedule of delegated powers
415 A tdgh priority in the matter of delegation of powers is to arm the Regiond Directors with sufficient administrative and financial authority to implement with expedition the health and family planning programs of the Ministmiddoty 1 thin the areas in their jurisdictions
E Integration of Family Planning wi th Haternal and Child Health Services
416 At present family planning services are being provided at 48 Goverrnent hospitals health centers and health offices by using the full shytime E taf cf these institutions and employing part-time (sessional) doctors nurse~ anI clerks where necessary At 29 of these institutions separate famil cl~nics are held on specified days in the weck some being doctor sessi(ms mel others supply sessions run hy nurses and clerks At the remaining 18 imtit1tions family planning services are combined with antenatal child healtL cr postnatal services The Family Planning Association runs 8 unishypurpoe f am ly planning centers which provide daily services and contribute a 11 t le less than half the total number of new acceptors per year
417 N assessment has b~en marie of the effect of integrated MOl and famil~ p~ nnning services an the recrl1i tment of acceptors nor were ~ data readily avallable for this purpose It may be observed however that in a situation of shortages of trained personnel for health services utilization of the existing health staff and facilitieR for family planning is inevitable parU cllLrl y in the interior where such shortages are more pronounced This underlines the need of evaluation of the integrated xai and family planning progtam for its impact on the number of acceptors Also a study needs to be made of che utilization of medical and pilramedical manpower so that it leads to bdter ~llocation of duties and optimUJl utilization of personnel
418 ile integration of faMily planning into Mcn services has certain advalltages as well as attendant risks The advantages are
a Lbe association of family planning with the care of mothers and children helps project a benevolent image of family planning as a program of family welfare This creates a
- 13 shy
1imate favorab~e to the acceptance of family planning aa lt p-)si tL1e il-Eare rreasure rather than a negative program cE limiting c~ildren
h t elps erlist ~r2tion tf doctars and nurses who as c -~ass enjo tft~ Y)er)et~ a~d confidf~nce of the communities i712~ Eerve
c ~ieD of contact with women
d luni-purposa clhlics for ~lCH and family planning services are onenient for motn~rs who would have to travel considerable (listances to the clinics
e hete is better utilizat1on of Acarce heAlth manpower
419 he limitatio$ of integrating family planning with MCH servicesI
are the posiOili ties of loss of focus on family planning as a high priori ty prograrr ald the diffusion of pol1sibility for its implementation These could tlow ve r he safegurded agaifls t by adopting the following measures
a 11e job descriptions of doctors and nurses should be rewritten 0 include the family planning function
b hE perf0rt1iai1ce of ctoltors and nurses should be judged as much )y tbeir inteceq t in planning ~vork as in maternal and ~hjld care and this should he lade known to them
c )octors and nurses involved in ~CH services should be given middot)rj entation and traIning in famj ly planning and their interest 3UEtained by refresher courses seminars meetings and supplies of literature
d Thl techrical (xpert~ in the Office of the Family Planninl Program should maintain liaison with and guide the field agencies in implementing the family plannin~ program For this purpose schedules shoul d be marle out for periodic field inspections
420 It is suggested that the working of half-a-dozen centers where family plbnnLng services have been integrated wi th MCH sessions should be studiei for ehe purpose of standardizing the methodology of delivery of servicl~ Such a study should include staff strength patient load recoril shykeepills 10middot of patents in the clinic timing and frequency of clinic sesaios ani convenience vf patients
F Voluntary Organizations
421 I i~ internrticri31 expedence that the birth control movement is pion aTC tt volunh[~ JilC S Qltl that hen the national governments step in wi tl cmbi ti 019 prjhns wi thin the sLate welfare system voluntary bodies ieh tteir limited ilsrluces restrict their service activities and shift the emplasi i 0 educedgt (f the community training research and contracepshytive Sf vic not 1l7gtilflblr in he official program or in areas not reached by it In nagni tude and expanse the of ficial program in Trinidad and Tobago has alrad~ orertak~n Ce 101umary program Increasingly it will become the domLnart tartner in the total national program while the voluntary agencies will cOltirlU1~ to receive financial support and encouragement to set up high standaeis If service and explore new areas thus acting as a stimulus and an additi_e tl the official program
G FrOB-ram Infomation
422 Thre is no concurrent evaluation or monitoring of the Program The daa or lq72 flowing in from the clinics month by month have r8Jllsined unprocss~d tn the Program Office The official Annual Report - 1971 Sums up th~ poition as fcllo~s
ITThe Research and Evaluation component continued to be the weakest in the Population Program Although a systen of evaluation had been built into the program the follow-up procedures for analyzing the data and for correcting inshyconsistencies are inadequate Requests were made to extend the staff to establish a more viable unit but by the end of the year no chllnges had been made
423 T1e recording and riporting jJrocedures were revised effective Januery 1972 and there has been a further change recently at the instance of t1e Evaluation Adviser Under the system now established the clinics are lequ Lreurod to maintain the following records
a Family Planning Clinic Case Card - New Cases This was introduced on January 1 1972 and has thirty-one entries giving age parity contraceptive listory pregnancies socio-economic background ource of family planning information and agency for notvat ion bull (Annex 2) The case card is made out in duplicate for each new acceptor and a copy sent to the Program Office
b Daily Regis ter This fs a ne~gt1 form recently introduced in replacement of the old regis ter and is preparen
- 15 shy
ie) ruplicate the original to be transmitted to the Program (fHce and the carbon copy to be retained in the clinic Th~ is a very 121zborute form requiring 36 entries to be aa~ for each Chse nel and old attending a session includin~ (ntries to cit L to contTaceptive supplies issued
AijCleX 3 T~13e fcnnG are required to be sent to the Program lffce in i7JO balches every month the first batch for the i IS fif~eeL days and the second for the remaining part of hE month The trtention is that the data appearing in the ~EZlic daily legis ter forms should be compiled in the Program Office and fed back to the clinics Although it is claimed that this new form has been pretested and is workable ex)erience alone will show whether the majority of clinic cL~rks are able to cope with it in a busy session
bull o now-Ho Card TIlis card is intended to keep track of ac ceptor--It has entries for name addresfI and month fcr which a visit is due for each year
bull Aphabe tical Index This is a card index of clients with aidresses
Each i)at en is given a simple clinic card on which the dates of further appo~utnli rc3 an~ indicated A special fonT[ has been devised for the reporting ot cases unler the Post-IartumPost-Abortal Education and Referral Program
424 J system of monitoring progrRm performance from month to month need to bE develQped as a high priori ty The problem is not so much reshycord ng mc transmission of data by the clinics but its aggregation and proclssi ng in the Program Office every month which at present takes a long time The Statistical Officer should have a statistical assistant to help him Ln I he taflk Monthly progress reports should be available to the Mini H t~ n H(llllth and A11 offt eerlil of the ProKrnm Office so that remedial ac tl m I lAY h(~ tuk~n n rll1u- WhOnh1f ~Hfl(AlJtlaTY
42 For the analysis of data and evaluation the Program office shouln haVE th(~ full-time services of a trained demographer
H Field Workers
42) Tie Program nemiddotis tne services of a cadre of field workers to enr)ll neii aceeptoTs follow up acceptors in their homes and revive the int 2remiddott of dropouts Such a category of workers could also be utilizerl for pr1fficting other health programs such as the VD campaign and the inmuni~ation program
47 As an experimental measure one field ~]orker may be assigned to a emi l~ of Hi 000 population This would mean 100 field workers in all
- 16 shy
Earh of the workers should preferably have harl a higher secondary education otherwLe 1gt junior secondalY education They should be married persons with middoti1ltt mot tl-an two or tlree children recruited from the locali ty in which they armiddot~ requlred to function Only persons who have the capaci ty to comnunl at~ and or6anl~e should c chosen A months ini tial orientation
slcu1d enable them to start functioning in the field though reshyfresher CO rSeS tvould be necesslt1ry in due course In Port-of-Spain married mer~ a1C women may be employed on a part-time basis
I Hanagement Study
428 A nanagement study of the Family Planning Program should include a sctu iny of the top m~nagement Atructure (Population Council - Office of the Fanil) PLanning Program - Principal Medical Officer for MCH and Family Planni Ig fetices) the field structure for the delivery of family planning servics (Re0ional Director - District Health Services) including the utilizlti(n if medical and paramedical personnel for adding the function of del ve y )f family planning services and the control and communication proCed1reF Lfnking the top management with the field structure
429 The management consultants may study the functioning of the Popul tio I Council and advise whether it adequately serves the purpose of givini po Licy direction to the Program and if not what changes in its compo itt m and operating procedures may be introduced without altering its bsic craracter as an advisory agency The consultants may suggest an alern at ve form of organizati)n and utilization of personnel which in thir p nion may be better adapted to the needs of the Program
430 Irrespective of whether the Population Council is maintained or it is replaced by an agency of a different character a formation like the Offic of be Family Planning Program would be necessary for the administrashytion i)f 1 he program a task for which i 1 appears inadequately equipped at preselt Its obvious requirements are in the areas of program monitoring and el7alnation program supervision communication and training The manag ememiddotlt consultants may study the structure and procedures of this form~ tio Gnd make suggestions with regard to the augmentation of professional and ~ upp)rt lng staffgt and modification of operating procedures
431 The linkage of the Office of the Family Planning Program with the Miniutry of Health (Central Office) and the District Health Services should be sudied In view of the policy of the Government to integrate MCH and faI11iLy rlallning services it should be examined whether the Principal Medi al Officer for Communi ty Heal th Services (MCH and Family Planning) should be agtpoj nt~d as the Chief of the Office of the Family Planning Program and an adTlilistrative officer of a suitable level inducted in that Office to assist him TIle implication of this suggestion is that the head of the Family PlanJling Program would control the District Health Services
- 17 shy
432 rf 1e management consultants should examine the delegation of adminshyistratiie Bld financial powers of the Ministry of Health to different levels of Progam aclrlirdstration viz bull PMO Program Office Regional Director and County ~djca~ Officers
l33 he system of 01 af Togram information from the clinlcs to the Pr()~ra1 O~fice and tOile processing and use of information in the latter office iholld )e studied
434 he working procedures at the integrated McP and family planning clinics shnuLl be studied This would involve a study of each stage which a clien tpcticmt has to go through from the point of entry to the point of exit after receiving advice service or supplies This study shoulci lead to star dartization of procedures and functions and evolution of -lork norms CognatE st tdies of the working procedures at uni-purpose family planning clinics and su~ply SEssions should also be undertaken An essential component of these ~ tad ~es would be to examine Nhich functions currently performed by docshytors lealh visitors nurses and midives respectively hav~ become so roushytinize ttl it they can he relegated (0 the next 10Her level
435 Reated to working procedures is the problem of job description of medcal 8nd parrunedical personnel involved in family planning from the centra i tc the field level This job description needs to be studied wi th a vie VIW8Id txaminiDg the uttlization of skills and allocation of time by the staff lcc(rd~ng to the functional prj ori ties
436 frV management consultants should study the workings of the curren slralgements fOJ family planning counselling under the Post-Partul11 Post-Abortal Education and Referral Program at the Port-of-Spain and San Fenaldo General Hospitals
437 SU1ect to the ItBrcement of the Gove1nment the management conshy8ultal ts ~hOLlld undertake a study of th requirement of field workers (home vinitcru) in tmtlUI of are nnd population cov(ra~e
ANNEX 1
Names of Persons Met
Ii Mr T C Taitt Pem1(H~nt 3~crtarY) Ministry of Health
2 Dr M n Henry Chitd Medical Officer Ministry of Health
Ellubeth Quam a Prindpal Medical Officer (1S)
4 Mr G Z Jaine ~ uJiector Population Council
5 Dr Norma Andrews Medical Officer Population Council
6 Mr Jc~n Coury~ Evaluation Adviser Population Council
7 Mr A Jriseph Principal Statistical Officer Population Council
8 Dr C 0 Colman Country Representative Pan American Health )rg ni~ation
9 Mr ranca Kippel Health Education Specialist Ministry of Iea th
10 (1 bullbullines Principal Nursing Officer Ministry of Health
11 Dr Mx won (formerlyHinistry of Health)
12 M3 late Carops Ex-Chairman of Population Council
--
4i 1_ middotIIlt F-ntCWclOotf_Y v OJ t tl
GOVIIlHMEIgt(I OF TINIOAD AND TOampAGQ - NNISTJY OF HIALftf AIJIE1 2NATIONAL FAMilY PLANNING PROGRAMME
F MIL Y PLANNING CUNIC CASE CARD - NEW CASES - NFPPl
li ~~___ 1 ________
~ ecll-U
-- --------------------- shy~) ~~middot~------------------~~~~~~---CIJ------ middot~ii--middot-middot----middot-middot---middot--------- shy
ltv Writt N_ 01(111________________
a ~4itiJtmiddotl_____ ilIIIltIoI~____~____~-__----- shybull ~4
fie l$ - JO tDql IIfIA- tr-JMimiddot _ iJ 1 Odoor o
14aorielaquol_ _~ 0 lio witIleo-La ~ 01 bull - OJ ( _01 1~ltgt1lh o bull- 0$
AacJcu 0 2 CIIriIWA 0 J Os 0
Yv~MONTH ltnollOf~nfIGHTI
Undu 1100U$ Utgtdn 5SCI Undu 11200 01 ~ 50 - 9949 amp100 - 1199 02UlOO - nn9E~ (
0)~ 10- $99 SiOO -- U9~ lOO -- U99 12400 - 1359)-------_-r----shy ~l)o SIS n600 - Hm1300 -- 019 OJ200 il~9 ~------ 99~ a 1)0 m Os1)00 -- l99 1400 -shy $4100 -- 1S999r--- shy
1500 donl S6000aad O399 - lt499I~- I 0lt
ltII
IJ -IC _~tltlioltgti lS
02 IaampJIIocI OJ 04 laM Os
w Oltwio I_-l(~u IrIaa U
h~~ ~Clubl 01 OJ
IS ~C-n 01 toSIitDI 02
Ji poundI on 01 IriIIIuy M ur 02 IV OJ
WU 10 pltIoII~ llaMtl 411 cIIiId 01 Ol it fIolto ~ do~ _14 rou IIlgtJo 1Ia1 ___~_ shy
40
It _ I 00 ~bull FPIiIJ 1
OJ 02 OJ 06
)0 III- iy wOWcf ~1
aMIIl Os
11 T 1gtlt ( h _______ 4)~
06
04 (MIbullbull middot bIrlI ~___~__~_ (-fIJI ~- -~-- (1HJ 49middot SJ
U 10k 01( 1__ raquo$-4
iU1) DOl F ToWotfOlnC DOl 001 or Do [IP 006 001 OIIgtu___Spltclty DOll Nltmo 010
U1Mo I orcpmiddot laquo55middot16
1lD 001 Foam Toblelf_ICim DOl Condom DOl CoomS~ 004 oe Oos WlttuJn 1J OIkr DSpody) 101~ ~Iu 006 Rhylhm 001 DOG OJO
no wI~lmm 4 cd
(I 0) 1110 01 Condor 03 (lorn bull l S~muoidIl 04 Faa TabioolfIIltr- Os RhyUlm 01 lnJrl tible O Advico 090 06
la slt 1)0 19 loti ~rltnlt) ([)sl or 1llOn) ____ --__ bullbully-J n SV - ~JcdS
v~ Cl NCI 0 30 OJI_O I Wr blJ1h 0 I ~ OJ 1 ~ (fOOd V 01 No 02 laquo 6) Cf4
WIiI 1 172
004 001
j D middotmiddot middot
1 ~
r
~
bull I
bullI I I
r c i
ANNEX 3 Pagemiddot 1 of 5
0 raquo rshy -lt l)J ~ 111 t G) 5 shy (J) ~ -
fT1u
i
MINISTTY OF Ho1TH
NTIONl F~ILY LNNING PR-GRbullbullM-tE
~~5tructions to C11nic ClerKa
How to co~ploto the Daily Rogister
~~ ~~v1sd Daily Rosi8ter replnc~D tho one which is now in use tb$ Monthly PC~ri rOt~ arti tho 01( Ci() Dod PollJ j f m It is a pre-coded form and 1411 cl~1p Jd tl a1I6iniul-mIHvn Oel Clinic nctivi~y
110 )rm rollt biJ coupJot)d lrl cupLtcoto using a o(roon shoot Tho top aheot or oriinai ~ust bl) 6(Ult to tho CQgt1tral O[[lCO and tho carbon copy retained in the Gliaic rilo dll the for6a that ar uD~d betwoen the 1st 4nd the 15th of the oIIollth aut bo subClittud tocho office 35 Lnc blttch Those oomp1cted betwoon tho 16th _lid tqemc of tho month must bo ~cnt in a secJnll batch
P lOvLior hns boon Illllde for 25 clients on cZlch forlll new forlll must b IIlied f r poundh 50[810n2 whothur or not ono or lIIore session are hoIdiit the clinic on he sarne day
I th ro alO more htl 25 clionta 1n attondnnco at tho session the additi shyOhAl m~bOl of clionts 10 clients nu~ber 26 27 etc sh0u1l be ontered on the next Imiddotrlll ~i ttout a1tpoundring the numbtlrs in the cvlumn hond Series
51 ppOfil th~ number of aUcnts lQr that session ws 5 this would mean thllt two rJlS ~ lst be 6ubllIitt~dl the first filled uF 1 tltgt 25 And the laquoIncond 1 to 10 Th~ cal bon ofies should bo st~plod togother at thu t0P l~rt h4nd corner of the torm ard ktpt in the Clinic filo lou IIlU6t stapl~ the originftls in the 8~~ monnshyer for lIub~ssion to the ofticl
ie h~ ll idontiflctior- (cc 1 - )
0 lot Ji 9 anythin~ hGro poundhia is int(mdClc for tha computer code
2 ~~pound~ - Print clOflrly tho name of your Clinic
C1Lic Huml or - (cc 4 - 8) Evar1 Clinic Numbor has 5 digits Virite each dig t il a t$purate box
It Pai~_thllsectgdllion (00 lt) -1 1) - Dl monll 10M
lw) bolte IlrO proY140d fetr olAoh pr 01 thQ dISh Enter tho dA) ldns a R
d16ih
emiddot5middot (0 11 I for 115t ( 0 21 for 5th etc Treat month the am pay
e ~ 10 ~ I for I-hrch 0 [2] for September Tho y~nr must be (into ad
I Z I ~ I I 71 q etc
Take as in IixulIple tho dOlte 3rd tllrch 1973 7~ie must bo written
[0131 LSLDI[7l3JDny Month Ye~r
5middot 1~J $~~ - Irom ~-------- To --------shytntol hOI II the time the Clinic 111118 in SW5sion emiddot8middot
(i) 11011 500 lm To 1200 non
(11) Frclt 100 pm To 400 pm
(iii ) IX-OG OO pllI To 6~00 pm
f
2
ADEJ ) Paae ) of S
6 Eov
_ 1hA 1gtIpoundC iIIUlt be nu~o7Ifd tler1ally 1 throurh n lU tbey Are Wled In ~1l8ellJ IInel 1301 tlU 1 Orcl 1 Wled tor a o5038ioll - -I 2 tonY tho _boul~ b I1WJbtl 1 and 2
hlrlll are 25 linos OIl the fOnl Ilnd thoae muet be UBtleS for 25 clients 9 one ior bullbull 01 I ini
ot ~h lc II ol1cM lOlivpound til e linic before soeinc DurOI or doc tor ilnc ii hox rristrltltion nUlJbet had alrearll been recorded on the Dai 1y Roiuter then n line ~hollld be drawn through that entry an1 the eliort nust not 06 includttd in tho totals tor that 0eDion
1lw Ileifitration Num)~r of cueh client must be IiIritten IS n 5-dlrlt oode ClhnC IH11IlElr 315 1IIU8 tborotore be enterod 18J010117]5]
~ Clt ZOt
Coda 1 Codo
10 ~tl c 2t j co 21)
~w elSe - Coda 1 0) d CltaEl - Code 2 Revislt Code 3
Only pound1 01 theBe coiles may be usod
11 prol-O~ ~Eil~1 (cc 22)
If ma climt was L drop-out IIho haoS returned now to the Clinio tor tho first no linmiddot bullwin lt1ro1eo o t he or she should be given CCe 1 It this do 5 II It nprlly leu this colWlln blank
u Hothod middothisllill loe 23)
NOh til t otly ~ Cod 16 tp he ontered in 2lpound of the columna oven thOUGh 10 co11lllJlB 10 provided on the torm The Codes llrol-
Oral Contraceptive Code 0 1 U D Code 1 Condom plUD Codo Z Condor (only) Code 3 Foum tAblets cream Code it DitphrClGJII Code 5 Rhythm Cde 6 Injectible Code 7 Advice Code 8 Other Code 9
It for middotDo-le 1 client rlllll ji yen cclldorls ord foam or creall Iou Qust entor Coole i (condom plulJ) in the appropri~te column This Quat be the only lIotmiddot) tarcie If an in the cnse of a tlnle clinic I the client is Bup)lieu lith COIlOrW only you rmot entEr CorlQ 3 (cpndolll) Do not use a ticII ~ tho (odo Nwber
It is CUi tomary fur 11 cliont 110 is beine put on the oral contraceptive for the first tiT1o and even on other occasionn be issued condoms and 11 crelle or foam a Ilell rI3 a pgtcket of pilla In such Cllses when the piDQ Ilre Ilctually iouou you tlust record Orll (Co~e 0) 08 tho onll metbod ilo othor ntry sll0uld ho nnrlo
Uovever n SJC~ canas vucru condoms and fOHa ~rc eiven but no pilJa (even thoJRh _t _n the intention to issue pills nt the noxt vioit) than the Mothol Th5 ifli t ohoulcl be recorded uo Condor Plus (Code 2)
13 Seen Bybullbullbullbullbull
~rot S-1 SO l
Doctor (Dr) - Code 1 j Nurse (Nul ) - Code 2
Clark (Olk-) - Code If tho Clhnt is vcen hy both tho llootor tlnd the Nurse enter Code 1 t Doctor It 6~61l by the Nurso only arite Code 2 Cod bullbull Cerk is l)llnt for FA Cllnica Clerks in tho Government Cli1t hiwo Llttoll istructed not to i56uo supplios on their own volition
14 fl221~
lhio S~tiCl of -Ie fvrtl t~ke 16 (llrci coluMna (cc 25-+0) nnd 10 tho only part at th iOIQ in llich iore thAn one cod is Zlccoptl1blo Tho purpoco of the )ecton is to 0 able to arrive nt the Cjunntity of 6tock dilltlitJutshyed YOI IIlUdt writo in the CllllOjH-iata colulna the nUllbJr of Il1ch 4rtic1o i~JSu~d ~lo e ha I Oral Contrcilpti vea are aub-di vi dod into types ae_ 3 PIllCKC 9 0 Elynnn LlUot be entered Codo in card column 25
If tor eXllrplc t l cliunt is iosued wi th packots of Zucynon nnd aJ(1 ~ivn 1 conuotll (8inoloo) you ouot enter in oard column 25 and 11 It
cnrd col~8 )2 and J (io 1 in card colucn 2 nnd 2 1n card coluun 33) Nota C)lldoIlU ale to b(t ruoordod individually not os packots of throo) Should n ne LlondoClo be isoued thil3 is to be rc-Qed as 09
If It clint 6 t~ot isoued Blly lIupplies thon you must writo Codo 1 in CQllAlilD 41
It Q eli nt isite the clinic to check on her LUD or her Diaphra~t IUId ro DI W 6 ppl ills nre ispounducd then Code 1 1s wri t ten in column 40
In the FA clinios here a variety ot orll contraceptiveo in orer~l tho elerll wilmiddot~ bJ provided with a specill code shoot The idontifyin coo will b wiittn in Column 29 nnd the nUlber of packets iosued in colwm )0
lralaer-In Code 1 lrllllsie r~ut Coda 2 leIllPQrArr Trnnsfer-In Codo gt
In the cao of n 2ratl8fcr-In I you lUot n160 cOrlpleto coluons 42-51
In the cllU J of A ~~emporary TranGfor-1n (an individual who i8 only v1citing fur clinic tor some epecial trcatcont hna who will bo rdnlnin
~middot(II~~~fO~l~SIl~I3~nn~~~h~rO~nh~1~~190~~nll 2-46 and ler rei IItrntion numbu in colullnll41-51
It the oli( nt i iNt a CrllnoforwIu - Out or loClporu1 tMn loave oolumn 1 blank
16 lr4nst(gtr-tl2~~morrry TilJnder-In (co 42-51) Forl1ltl CUn E1~ (cc 112-46)
hen you rei iatlr L irllsfcrln or Il TJlporary Trnnsfer-In you IIIUBt write I ere the five-digit clinio nucbor of the Clinic iraQ which tho ltlient Me (uIlO
2mer ]letr ~2n ~ (cc 47-51)
frlta fllao Clo r-~itrlltion Nuc~Er ot the client in the Former Clinic (i c bullbull th 1 Sis rnmiddotion ~UlIlh()r which the client carrics 1n the tormor clinio) bull
It tho Forrltl Ho( ist rntion Number iIJ not readily wnilnble you tluct oocpluto thtl epcciol [orlll Transfer-In Not Identifiod Dy Forrlcr RCGi(trn~ t10n Nwlbvr Or ~ flt)rCl is to be cOlplctcd for och cnso nnd th forlJO Ilubmi tted to thu )opllntion Prorrnnme Of fice tOGether with tho Dily Ro~iBtors lhwev~r should the clork leuTI of tho clint B FormlI Uocintra tion lUlllb r )0[(10 Cubmi ttinft the D1ily IOCI otro t hen the nUQbcr shoulo bo -ri ton in colucns 47-51 lna the special foro should lJo deotroyotl
l7 bullbullbullbullbull
r lt bull bull
ADXI ) Pap S ot S
11 UD LV~ (cc 525)
It tb( cliont io ~ivQn An IUD tor the firot tl~o then you should Sri to Codo 1 Inuort ill colurJI 52
It tho olimiddotsnt ia rvinGgtrtltld i th An I UD bullbull tben wse Coda 2 RelnDltlrt shyin (01Uil11 52
It the clLmt is ~tte~~dint chnic beruse her IUD CflClQ out by Haol (cxpll Iion i ~hcn fir te todo ~- UIlllrli1 53~
If c-ltr IU fj IIIS reov in -ne cllnic by tho doctor or nurso t~on vlritI Codec in column 5
II the eli nt otends eiLlie tld explin[l th(lt she rccovcd the IUD tlllleel nen write Coda H in Colwlm 53
It the IUD jr still within the uterus nd the WOIraquoI1 1 11rc6llJlnt thon lIrite 1gt40 4 in Column 53
lZ np h5t (ce 54) It 0 Pull 5mor ie t~ken durin thi visit tben Codo 1 ehould be ampDtere4 in ColWlln 54 Should he c110nt lltt rQ(uircd to rttturn to clin1c for a rogtol1t Pnl) t06t then CoLe 2 llhould bo middotwrittcn in column 54
It no Pllp Scou io taken tde visit Itove colUQn 54 blank
Iraferti1lli (CQ 55)
Ii the e liett io nl1 infortili tr eaoe use Cor1o Ill in colUQn 55
If tbia 1000 not tlpl lonve column 55 blonk
20 Totaltll
CO~1ploete the [)ldegO 1gty puti YI tne totals betweon the double lines nt tu b()ttctl Carrj colUlllnc 20 21 nd gt4 Must hlve tho Bnoe JllIIber and thiG Would coreslonc to the numocr ir attencbnco
Writ$ th to1ul nUlllior of Drop-Outs returned (c022)
Urito 41eo tb totnls fOJ each card column 0 to 9 under tho h(adinu Method thiB Vioit Show tho tote L fgtr OlCl type of contraceptive issued (cc 25-40)
1)0 Dot wrLte 1111 totll lUl(Ier Card Columns 15-19 29 41-51
21 COPmllh bull ~lt h~t~ Monthly ROilort
OQ thG DaLl oCator forlll thnt ccrrOspOldB to tho 1(8t 1$06610n lt 0
oth yo Olllt (vwlgtleto the items nt the botto of the [orampl This is tour ontll~1 n(olt nnd includcD tho totll lumber of sesions Ilntl tho total Iluolcr ( r crop-outs durinr the Qonth
An tiUlsilt n drir which n doctor liB in nttcndnncc is a doctor sOfll~1on and shoulc 00 re(liGtcnd in coltns 56-57 All other sessions 1116 conlliid~recl supply stllciona and thtlY 1110 rocordod in columns 58-59
the total Ilum)nl Jf drop-outo ld the drop-outs by method durinc the onth nre 10 bu oltorou in the inrlicllted boxes
72 Chad Your ~
Milke I ura th t all thE fijul4gtu rre c101r -tNever writo our nutlUQrS 50 InrjEl that they oxtend out of tho
ap~rotr1ato ~ox
Cheek to BoJa tht 1111 numuors 1110 in tho correct boxes -- CJslHloially when Writi1 the totlB
Mllxe Cirtc O thmiddott t1e infoT1I1ntion i6 clear on the corbon COllY before sep rmiddotinr the sheets
Jitn the Fomiddotl lien tly sien YOUl nr me 1t the bot tOil right hnnd corner btl forc subol ttinG it Keep tle CL rb n copy for your rocordn
i
-l ________~~---------~
I _1
Adminiatr-atlve SKVieu
P inba ~~~l1cal lrlnbin~~eltltcal -1 te~ra t~~rvicc (lnatittloaa)
--1- - shy -1------------_-L_ l-r-aJiil- shy _-L_tet1lal d
PlIinm1tJ8 atdUon DetalMid H8Il1tb ~ ________bull Care
-----~ Office of i
the FlIily _IPlill3 roarshy
1- - - -------RegiatUll urnr
ltIi 1 Drelttor Rcgicaat Director Souta Tabqo tacallortb ~ counu gt____ ~ (4 ouottet)
Off1ce of the Res10nal Diractoc L
r----- _L_ -- shy i I bull IREgional Ipitl I
District IIttaltb I bull Othn RelOl ond Hcpital CenteIntt itlt j In 1__ _shy-~- ---- -_j
J r Ii~lth
C~nlef
L
I Ihnlth lie I th Offlcu (1ft lc~
Coullty 1I0p1ta1
Henlth tentet
I

- 3 shy
which COlT bull Se 11CH anii IIgt sxvl(s I1H~ other committees are Community Educaior and Publidty Cvrm] ttec Research and Evaluation Committee Family
~du aton Comrnirii ~~e(i] CCimittee and inance Committee
OS i~ n1eptUd~ i p Ni ~runi t 1 an advisory body and as such itus 10 execl1lt)ltjmiddot n p-actice the Office of the Family Planning Prog) am e tabisLecl wirgtmiddotcn tilt2 middotlnitry of Health functions not only as the ecr ~tc dat of lIC )hiCJl but also as the instrument for carrying out lis lirEctvls Furtiie ch GOtdcCU has concerned itself nomiddott merely with broal i~ SUIS f10Hc out also vL detailed implementation The majority of t le r emmiddoters of rhe Council are in favor of Umi ting the Councils role to tile givlng of broad direction to the Program
20i The Office of thl~ Fitli1y Planning PrO~rall1 is comprised as follows
Dlrcct0r (Incant) Medilal OfHceuror (Famtly Planning) Nm-~If Offieer St~tistical afficer Health Educator 2 lield Workers (for follow up)
(OIlE positor vacant)
8CCiHWlcnt 2 clexks 2 typists 1 driver 2 proj ctionis 15 and 1 messenger
T- ~ g af f of the Office of the Famly Planning Program is under the discipline of thttinistry of Health since the Population Council is nei ther a departshymfntal unit nor a separate legal entity with its own fund
2 OB The places of )nrm1 atton Council and the Office of the Family p ~anr ins Program wi thi n the Minis try of Health as conceived originally by tile Government may be seen in the abbreviated version of the chart appearing hI different official documents and reproduced at the end of the report
~ 09 In April i973 at the time of the consultants visit there was In aCIDc)sphere of uncertainty about the administration of the family planning l)rogram as a result of changes in some of the top positions As a result of t c~binet reshuffle the portfolio of Health had changed hands The Permanent euroctet lry who is the princ~al ad~liser to the Minister was new as lras the r-i c al Yedic1l Officer h charge of Commurity Health Services (Mel[ and Pam ly Pl1nnhg) The Dtnct0 of family Planning who was managing the Office of middothe Family Planning Program and also serving as the Secretary of the PoshypUlition Council had reCiTed in March 1973 and a successor had not yet been named Meanwhile the Medical Officer for Family Planning (a part-time employee) was carrying out the functions of the Director in addition to her OWT Wi thin the Population Council the advisory agency for policy-making
and ccord~n8tionJ there was a groHinr feeling among the members that the ouncl1 510t1d shed thE respOJ1sibili ty for implementing the program a funeL on j ch nad heuroe added on to its advisory role with the passage of time
iO the 1 ~lp~1 the lines 0 responsibili cy were not clcay (e ned and Li1 refioal system was not fully functioning The post of Re ior 3 Director crth VIas vacant The policy seems to be to strengthen the 1St tu ion of Pt()1ic Flealth Office as an 3ency for the supervi-middot sion)pound ne district sflVices (health centers health offices and school servi ces ~l thin the ccnmty
II I PRES EN STATUS OF THE PROGRAM
301 ~he adl1linistrt~ivE changes narrated in para 209 have come about at fl tin e IJhen the P1ogram has entered a phase of declining performance as is 11 Jpal en from th colloHing figures taken from a report submitted to the Populaton Council
YrUL 10C7 ~j8 1969 1970 1971 1972
--- -- ------------~~ --~ - shy----shy
Ne Acceptors 3696 2731 16207 9997 9898
(End of October)
7560
Slur~e Family PlAnnto Program Report (no date)----AsII1Ulilg that th6 ttlrollmant of new acceptors during November-December 1972 prclrd at the 8ame rate as during the ten~onth period January-October
- 9i2the total enrollmslt in 1972 would be lebullbull than 8500
3(12 lhe total number of leW i-iCCeptors for 1971 shown in the foregoing tal11e 1s at variance with the following data from the 1971 Allnual Report
- 5 shy
~ev C~~ Contraceptive Method and Agency
nm Other Advice Total New Cases
Aeny
GovrrmenC ProEllil ___~zZ(lt1____ 97____2Lbull499___~528~___4i_750~_
Farr Uy Planning Association 2814 315 607 76
Catholic MarriaAdis1ry COLnc_H____
ge
74 88 162
otal 31[10 692 8724
_--__------------------shySOlrce Natio
1973 nal p
Fam29
ily Planning Program 1971 Annual Report April
NevmiddotrneJl~ss) the declining trend in annual performance after 1969 is manifest ana conpaes unsatisfactodly to the following targets set for the Program
Targets for Contraceptive Users - 1968-72
New Accep tots Old Cases Total
1968 20noO 20 000 lO noo
1969 20000 40 000 60000
1970 20000 60000 80000
1971 20000 80000 100000
-----__shySource National Family Planning Program
p i9
------------------------------------
- F shy
3JJ3 Ttl flient recrvitTrent has fallen off since 1969 in spite of a signif Icar t xpansinn ir the number of Government health facilities providing family paarin~ services FrCli1 7Hr to year Starting from scratch the number oE GovE(nment health irlstitl1tions delivering family planning services in isollL(Od ~ily pltJfAill~I ~J in c)lchiratinn ~7ith MCa services has lWW risEn t 4 lhis ie --tdt)p to t cii1ics organized by the Family Plannin Asce1ation bull U2 by tile Catholic Marriage Advisory Council which offers the ~h)lthm meti1middot1 nT
304 1i ciecli ne d~ d re11~m2nt of new acceptors coincidentally w-Lth th~ eXlsioH uf s-crLce facilities needs to be studied to identify the factors responsible for it eg the quality of services offered the strategy of commmic at~on and motivation and management and supervision One obvious gap is he abgtence of an agercy for promotion and extension of demand for family lal 111 If services -gt tLe field reliance being placed mainly on clinic counseUn H1d generaUzmiddotd mass media publicity The need for a field promoshytional agelcy is underscored by the dropout rate In 11 draft paper prepared by the Hed_cal Offic(1r for FIrnilv Planning it is stated that by the end of 1972 t ile Heuroe approxiclt ji rHJC cun~ent users of contraceptive methods and 33 per ert dropouts
305 rht~ program is cot merely clinic-centered but also female-oriented Recent Iy mellsages aimed at m11es and stressing joint male-female responsibishyIi ty l gtT j ecillc CImt-J 1 i~gtVt~ b~~in )7cn 1n0 the cOTul1mication activity sUf1 tv) c nts Em he 2iucaccw i milc8 and che distribution of condoms to them illVC he ~n or n~d iD r GJvefl1nenC s(~ctor The Family Planning Association has a130E~k11 the irti U3 1V~ to reis ter males ln industrial employment Tllese are steps in the ri)n dtrect1ongt but the size of the problem indicates the n~ ed OI a concerted effort en a much large r scale
306 Tre Program relies largely on the use of oral contraceptives as shown in the following table
Oral Other Advice Contraceptlves IUDs Methods Only Totals ( 100)
19)9 76 20 16207 ( 100)
1970 316 63 9997 ( 100)
1971 50n 4n 365 79 8724 (100)
Family Planning Association unpublished report
----
- 7 -
Althougr amJnp the neH acceptors in 1971 the users of oral pills were only 509 ~mon~ the old cases the figure was 119 The percentage of IUD users has remiined stagnant at an insignificant level this may be partly due to consume prefErence and pctrtly outng to lack of trained staff to undertake IlTD i1srti l7U There h hOHever a visible shi ft towards the uSe of othe~ ilettods (npchani81 and chemical) attributable to a scare about the side efects nf oral connaceptives Among these conventional methods the condom s 11 os popular
307 J t )resent fami ly planning services have been extended to 48 out of 106 hellth centersoffices run by the Government and the objective is to C)Vel t1e remaining health centersoffices within a short span of time so that adice and facilities for the practice of family planning are conshyvenient Ly wa nable to the people in all parts of the country By ann large sepanit e fITti ly planning eli nics are held on specified days as an addition to norrral lealth work Besides doctor sessions at the clinics supply sessions are rur by health visitors and nllrses assisted by clerks The nurses are authorjzed tc issue oral contraceptives for a period not exceeding three months ani the acceptor is required to attend a doctor session for advice during thi jnterval In 1971 the numbers of full-timepart-time staff in Gov~rtmnf centers renderinp family planning services were
Full-time Part-time
1elical Officers 14 8
NUseMidwives 35 19
Cl~rks 3 17
Now tile low~rnment -gtbjective is to integrate family planning services into MOl services and use the same staff being used for the delivery of both types of erlices at multi-purpose sessions However so far only 1A centers have interated family planntng with Men or gpoundmeral hpalth care sessions
3011 The Family Planning Association has eight unf-purpose centers where famil) pLmring services are available ftve days a week The Association employs tilrEe full-time and ttJO part-time doctors a complement of 14 nurSeS (who llave been trained to do pelvic examinations) and 11 other clinic staff membels The Association also has a number of voluntary workers in the clinics The CithoUt Marriage Advisory Council has three clinics but their contri shybution in terms of enrallment of acceptors is not signiflcant
3)9 A Post-PartumPost-ALortal Program was started in 1969 It is state I tlat about 14 percent of the patients reached attend a family planning clini~ 1iTj thin six weeks of the interview in the wards IhiR is qui te a low figur In 1970 when a system of home visits was tried under the Family Planning Aide Project in 7 clinics the rate of acceptance doubled in three clinils rose by 50 percent in two clinics and increased by 24 percent in one clini (No change was noticeable in the seventh clinic) No decision has been Inad~ tmiddot) continue extend or modify this Project
A Po~ulaton Council ~-----------
401 he fu~ura ro~ Lh~ ~~~01ati0n Council has to be considered in theli1 A the tasK t~ lL ahead of the ~ational Family Planning Program At pesent tile officil~r(QSrJ1Tl is prirnarily concentrating on two objectives (a) tIlE excpound1sinrt of fmd plannin~ services to tie remaining 58 health centen cLJs as rapi(ily as possible and (b) the integration of family planniT g VI tr MCH services Thus thG administration of family planning serviCHJ will be merged into and become part of the Community Health Services Since t is ()rganizationally undesirable to disturb unity of command a separa1e elteecutive agency for the administration of family planning services is preempted within the existing policy framework An executive role for thp Pcnulc tinn Council is there fore ruled out on this consideration
402 If the Population Council is to function as an advisory body at the p()Lic~ aId progra1l pLilnni-l level snd not to concern itself with the minutile If program execution there wonld be no advantage in giving it a statutory stltuS But if it were the policy of the Government to set up a verticll )middotro~ram for family planning ii th a field organization separate and distir~tOroll the HeaHh administration it would be quite appropriate to establish an autonOiTiOUS statut()y a~fgtny ntside the departmental setup of the MinisiY of Health d~b a budi~t md staff of its own commensurate vith the rE spo lsi hi Ii ty to be rEs j Freed from the usual departmental conshystrailts ~n the matters Cif sp(ndlng a1d hiring and firing of personnel such an aglncy c(uld move faster than a heavy-footed departmental formation wi thin a Mins trl bull Hovever a hody of this eharacter would need to be cas t in a cliffe ent m(ld than the present Population Council The shape that it would take lrould be more like a Board of Management with a full-time Chairman or Execuive Director and with more functional expertise than representational charater But an advisory council with an autonomous status and no responsishybilit f( r lrogrrun eXIGulion iould be a source of friction
403 r~e existence of the Population Council as an organ of policy advici has certain advantages Firstly it is a forum for developing a national poLicy in which officials and non-officials participate Secondly it pr )vi bulles a focus to ti1e official program vhich it otherwise may tend to lose as ~ontraceptive services are merged into the general health services Thirc lymiddot- and this is important -- the Ministry has extra-departmental advice availabL to it~ but the Ministers constitutional responsibility for the condl ct )f the national progl~lt~ le1lains unimpaired
404 ls an advisory Q(dy the Population Council should be more broanshybase( than it is at present For instance it should include representatives of tile organizations of employers and vorkers associations of the medical nursngmct teaching professions and organizations for womens welfare The Counil should also haye a social scientis t on it On the official side the
- 9 -
Permane It Secetary and the P1O (fen and FP) should be brought into the Council he inclusion of the Permenent Secretary would open a channel of communi~aton with the MOR ae the highest policy level next to the Minister and would (ontribute administrative expertise to the deliberations of the Cou1ci1 ~m f icili tali 5 (pleuenrti)D of th~ recommendations of the Council within the -rni and in OUltL depa-cments The inclusions of the PMO (MCH and FP) wOlld el) emphasi ~2 hs responsibi lity toward the family planninR program Some officrs of the HOH (eg Chief Health Educator Principal Nursin~ Office e) may 111 ea~e to be members though they may attend as requirE d nmiddot the agenda before the Council A representative of the Ministry of Fin nee stQuId be inc~uded in the Population Council This would make for a lettr appreciation of the needs of the Program in that Ministry and fadIi ate fj nancial sanct ions
B A~tatutory Council
40S In the foregotng Pgraphs the view has been expressed that within th edsting policy framework an advisory Population Council would be more tli)prcpriate than a COlincil wi th executive functions and powers that an advisory rOUlcil would not gain by having a statutory status and that if a statl1tory body 5s to be set up in lieu of the existing Council it would need tC b structured more Iiice a Board of Management than a council wi th a repre13entttional charact~( n the latter event the statutory council should have fu 1- time Executive Chairman or failing that an Executive Director functj oni1g undel- a Chairman trno can devote considerable time to the business of tlw COlncil
406 T1e Statutory Council should have its own budget with full operashytiona pOlo1ers It should have the authority to appoint its own staff and regulLte their conditions of service If it is constitutionally possible the Couner1 shollld be outside the jurisdiction of the Public Service Commission in pesornel matters
407 As an instrument of Government the Council should be subject to such ~eUfral or specific directives that the Ministry of Health may issue to it frcffi ime to time This should be written into the statute under which the Cmntil is set UD
408 The composition of the Council ould depend on the functions assig1ed to it It is suggested that the Council should not concern itself wl th the delivery of cliric selVices in the field The Ministry of Health may (ont nue to administer rampmily planning services at Government hospitals health cmters and health offices and the voluntary agencies should run thei] OWl ~rogram The following functions may be handled by the Council
- to shy
s rrogram plannin and target-setting
b proram monitoring and evalllation
c wiL of d 1ci(JTIdnCf by inspections
d Qrg8lizatim 0 es and marketing of contraceptive J~1J-s BLl (iV es at subs idi zed rates through es tablished 1 2 d(~ channel
e information mass media communication and audiovisual ublicity in the field
f prorrotion of famil~r plannIng acceptance through face-to-face cotlmunication by poundi eld workers in domiciliary visi ts
g trIining of personnel
II pr )motion of -esearch enJ
i financial support to voluntary agencies providing family planning services
409 n Statutory CCii1cil may corsi5t or an eminent non-official vith a comri tm ~~1t towacds foJlily plailninf nd the fol1owin~ members
I ~ bull Pfrmanent Secretary ltl-tIlH
Chief Hedical Officer HOH
i Principal ~ecHcal Office ~mH
d Pilhlic RellltionB OfJte(middotmiddot Prtm~ Ministere Office
A represen ta ti V~1 of the Ministry of Education
f ~ representative of the Ministry of Finance
g A representa~ive of the FPA
h A representative ot the C1AC
i H social scientist fcum tle University of the ~Jest Indies
j Three non-officials with experience in management and administration and the
k Director of the Family Planning Program - Secretary
- 11 shy
The COUlcil ITIltW constitute cOlClmittees for Finance - Accounts Personnel and Sup lies nd Stores ir~whi ch )nly members may be included Other commitles sc1h as those 01 training info1nation and education and researCl ara ~valuation r1ili also include experts from outside
410 he Off1ce raquo) cc im Panning Program which at present forms part of th ~Hnis try or [i n should be placed under the Council and its staff strelgtl ilcn~ii2 i~ r181 it may cease to depend upon the services of the Mir is t y of H~alth
C Office of the Family Planning Program
4 11ollwther the Offic~ of the Family Planning Program remains a part of the Mirisry of Health or is transferred under a statutory council if one is set uP i needs to be strengthened to meet the requirements of an expAndshying pr )gn m At present the following sys terns need to be ins ti tuted in this Office
a a 3ystem of setting annual targets for the enrollment of acceptors and the projection of service fadli ties in relation to these targets
I Ci ~ystem oE V)glC loHitoring (the monthly statistics flowing from the clini~s c~iiiain unproc(~s5erl for months)
a system of program evaluation eg demographic effect of tte program cost studies
1 an overall design for media communication based on a study of the reach a~d cost effectiveness of different media and the effect of the meflBsge content and
e a m88t~r plan for training which would comprise an assessment of the training needK of the existing staff and future reshycruits and a long-term plan divided into annual programs
412 Th2 Prograll afiie s~lould have the services of a demographer and a meeia expert A training adviser is expected to be provided by the PARO
413 1be Program Office should evolve schedules of field tours to overliee field operatio1s E~1eh health cente heal th office should be visi ted peridicaLy by the Milt~dical fElce- the Nursing Officer and the Health EduCltoI who should guide and assis t the local staff in carrying out the progam Their tour notes should go into separate dossiers for each institushytion and ~ach dossier should have basic demographic data about the area coveled by each institution These dossiers would be a useful record for revilwing l)errOmance The staff of the Program Office should be augmented to Ol)erte this control procedure
- 12 shy
D Decentralization of Powers
414 ~hete is a concentration of administrative and financial powers in the 11in s try of Health I-JllJCi1 results in an accumulation of references in the Miristl) and delays n field operations Specific powers should be delegated ~o (a) the PliO concerned with MCH and family planningmiddot (b) the Directcr o the Program Office (c) the Regional Director and (d) the County Medica1 Oficecs The Ministry should invite suggestions from these officers and wOlk 01t a schedule of delegated powers
415 A tdgh priority in the matter of delegation of powers is to arm the Regiond Directors with sufficient administrative and financial authority to implement with expedition the health and family planning programs of the Ministmiddoty 1 thin the areas in their jurisdictions
E Integration of Family Planning wi th Haternal and Child Health Services
416 At present family planning services are being provided at 48 Goverrnent hospitals health centers and health offices by using the full shytime E taf cf these institutions and employing part-time (sessional) doctors nurse~ anI clerks where necessary At 29 of these institutions separate famil cl~nics are held on specified days in the weck some being doctor sessi(ms mel others supply sessions run hy nurses and clerks At the remaining 18 imtit1tions family planning services are combined with antenatal child healtL cr postnatal services The Family Planning Association runs 8 unishypurpoe f am ly planning centers which provide daily services and contribute a 11 t le less than half the total number of new acceptors per year
417 N assessment has b~en marie of the effect of integrated MOl and famil~ p~ nnning services an the recrl1i tment of acceptors nor were ~ data readily avallable for this purpose It may be observed however that in a situation of shortages of trained personnel for health services utilization of the existing health staff and facilitieR for family planning is inevitable parU cllLrl y in the interior where such shortages are more pronounced This underlines the need of evaluation of the integrated xai and family planning progtam for its impact on the number of acceptors Also a study needs to be made of che utilization of medical and pilramedical manpower so that it leads to bdter ~llocation of duties and optimUJl utilization of personnel
418 ile integration of faMily planning into Mcn services has certain advalltages as well as attendant risks The advantages are
a Lbe association of family planning with the care of mothers and children helps project a benevolent image of family planning as a program of family welfare This creates a
- 13 shy
1imate favorab~e to the acceptance of family planning aa lt p-)si tL1e il-Eare rreasure rather than a negative program cE limiting c~ildren
h t elps erlist ~r2tion tf doctars and nurses who as c -~ass enjo tft~ Y)er)et~ a~d confidf~nce of the communities i712~ Eerve
c ~ieD of contact with women
d luni-purposa clhlics for ~lCH and family planning services are onenient for motn~rs who would have to travel considerable (listances to the clinics
e hete is better utilizat1on of Acarce heAlth manpower
419 he limitatio$ of integrating family planning with MCH servicesI
are the posiOili ties of loss of focus on family planning as a high priori ty prograrr ald the diffusion of pol1sibility for its implementation These could tlow ve r he safegurded agaifls t by adopting the following measures
a 11e job descriptions of doctors and nurses should be rewritten 0 include the family planning function
b hE perf0rt1iai1ce of ctoltors and nurses should be judged as much )y tbeir inteceq t in planning ~vork as in maternal and ~hjld care and this should he lade known to them
c )octors and nurses involved in ~CH services should be given middot)rj entation and traIning in famj ly planning and their interest 3UEtained by refresher courses seminars meetings and supplies of literature
d Thl techrical (xpert~ in the Office of the Family Planninl Program should maintain liaison with and guide the field agencies in implementing the family plannin~ program For this purpose schedules shoul d be marle out for periodic field inspections
420 It is suggested that the working of half-a-dozen centers where family plbnnLng services have been integrated wi th MCH sessions should be studiei for ehe purpose of standardizing the methodology of delivery of servicl~ Such a study should include staff strength patient load recoril shykeepills 10middot of patents in the clinic timing and frequency of clinic sesaios ani convenience vf patients
F Voluntary Organizations
421 I i~ internrticri31 expedence that the birth control movement is pion aTC tt volunh[~ JilC S Qltl that hen the national governments step in wi tl cmbi ti 019 prjhns wi thin the sLate welfare system voluntary bodies ieh tteir limited ilsrluces restrict their service activities and shift the emplasi i 0 educedgt (f the community training research and contracepshytive Sf vic not 1l7gtilflblr in he official program or in areas not reached by it In nagni tude and expanse the of ficial program in Trinidad and Tobago has alrad~ orertak~n Ce 101umary program Increasingly it will become the domLnart tartner in the total national program while the voluntary agencies will cOltirlU1~ to receive financial support and encouragement to set up high standaeis If service and explore new areas thus acting as a stimulus and an additi_e tl the official program
G FrOB-ram Infomation
422 Thre is no concurrent evaluation or monitoring of the Program The daa or lq72 flowing in from the clinics month by month have r8Jllsined unprocss~d tn the Program Office The official Annual Report - 1971 Sums up th~ poition as fcllo~s
ITThe Research and Evaluation component continued to be the weakest in the Population Program Although a systen of evaluation had been built into the program the follow-up procedures for analyzing the data and for correcting inshyconsistencies are inadequate Requests were made to extend the staff to establish a more viable unit but by the end of the year no chllnges had been made
423 T1e recording and riporting jJrocedures were revised effective Januery 1972 and there has been a further change recently at the instance of t1e Evaluation Adviser Under the system now established the clinics are lequ Lreurod to maintain the following records
a Family Planning Clinic Case Card - New Cases This was introduced on January 1 1972 and has thirty-one entries giving age parity contraceptive listory pregnancies socio-economic background ource of family planning information and agency for notvat ion bull (Annex 2) The case card is made out in duplicate for each new acceptor and a copy sent to the Program Office
b Daily Regis ter This fs a ne~gt1 form recently introduced in replacement of the old regis ter and is preparen
- 15 shy
ie) ruplicate the original to be transmitted to the Program (fHce and the carbon copy to be retained in the clinic Th~ is a very 121zborute form requiring 36 entries to be aa~ for each Chse nel and old attending a session includin~ (ntries to cit L to contTaceptive supplies issued
AijCleX 3 T~13e fcnnG are required to be sent to the Program lffce in i7JO balches every month the first batch for the i IS fif~eeL days and the second for the remaining part of hE month The trtention is that the data appearing in the ~EZlic daily legis ter forms should be compiled in the Program Office and fed back to the clinics Although it is claimed that this new form has been pretested and is workable ex)erience alone will show whether the majority of clinic cL~rks are able to cope with it in a busy session
bull o now-Ho Card TIlis card is intended to keep track of ac ceptor--It has entries for name addresfI and month fcr which a visit is due for each year
bull Aphabe tical Index This is a card index of clients with aidresses
Each i)at en is given a simple clinic card on which the dates of further appo~utnli rc3 an~ indicated A special fonT[ has been devised for the reporting ot cases unler the Post-IartumPost-Abortal Education and Referral Program
424 J system of monitoring progrRm performance from month to month need to bE develQped as a high priori ty The problem is not so much reshycord ng mc transmission of data by the clinics but its aggregation and proclssi ng in the Program Office every month which at present takes a long time The Statistical Officer should have a statistical assistant to help him Ln I he taflk Monthly progress reports should be available to the Mini H t~ n H(llllth and A11 offt eerlil of the ProKrnm Office so that remedial ac tl m I lAY h(~ tuk~n n rll1u- WhOnh1f ~Hfl(AlJtlaTY
42 For the analysis of data and evaluation the Program office shouln haVE th(~ full-time services of a trained demographer
H Field Workers
42) Tie Program nemiddotis tne services of a cadre of field workers to enr)ll neii aceeptoTs follow up acceptors in their homes and revive the int 2remiddott of dropouts Such a category of workers could also be utilizerl for pr1fficting other health programs such as the VD campaign and the inmuni~ation program
47 As an experimental measure one field ~]orker may be assigned to a emi l~ of Hi 000 population This would mean 100 field workers in all
- 16 shy
Earh of the workers should preferably have harl a higher secondary education otherwLe 1gt junior secondalY education They should be married persons with middoti1ltt mot tl-an two or tlree children recruited from the locali ty in which they armiddot~ requlred to function Only persons who have the capaci ty to comnunl at~ and or6anl~e should c chosen A months ini tial orientation
slcu1d enable them to start functioning in the field though reshyfresher CO rSeS tvould be necesslt1ry in due course In Port-of-Spain married mer~ a1C women may be employed on a part-time basis
I Hanagement Study
428 A nanagement study of the Family Planning Program should include a sctu iny of the top m~nagement Atructure (Population Council - Office of the Fanil) PLanning Program - Principal Medical Officer for MCH and Family Planni Ig fetices) the field structure for the delivery of family planning servics (Re0ional Director - District Health Services) including the utilizlti(n if medical and paramedical personnel for adding the function of del ve y )f family planning services and the control and communication proCed1reF Lfnking the top management with the field structure
429 The management consultants may study the functioning of the Popul tio I Council and advise whether it adequately serves the purpose of givini po Licy direction to the Program and if not what changes in its compo itt m and operating procedures may be introduced without altering its bsic craracter as an advisory agency The consultants may suggest an alern at ve form of organizati)n and utilization of personnel which in thir p nion may be better adapted to the needs of the Program
430 Irrespective of whether the Population Council is maintained or it is replaced by an agency of a different character a formation like the Offic of be Family Planning Program would be necessary for the administrashytion i)f 1 he program a task for which i 1 appears inadequately equipped at preselt Its obvious requirements are in the areas of program monitoring and el7alnation program supervision communication and training The manag ememiddotlt consultants may study the structure and procedures of this form~ tio Gnd make suggestions with regard to the augmentation of professional and ~ upp)rt lng staffgt and modification of operating procedures
431 The linkage of the Office of the Family Planning Program with the Miniutry of Health (Central Office) and the District Health Services should be sudied In view of the policy of the Government to integrate MCH and faI11iLy rlallning services it should be examined whether the Principal Medi al Officer for Communi ty Heal th Services (MCH and Family Planning) should be agtpoj nt~d as the Chief of the Office of the Family Planning Program and an adTlilistrative officer of a suitable level inducted in that Office to assist him TIle implication of this suggestion is that the head of the Family PlanJling Program would control the District Health Services
- 17 shy
432 rf 1e management consultants should examine the delegation of adminshyistratiie Bld financial powers of the Ministry of Health to different levels of Progam aclrlirdstration viz bull PMO Program Office Regional Director and County ~djca~ Officers
l33 he system of 01 af Togram information from the clinlcs to the Pr()~ra1 O~fice and tOile processing and use of information in the latter office iholld )e studied
434 he working procedures at the integrated McP and family planning clinics shnuLl be studied This would involve a study of each stage which a clien tpcticmt has to go through from the point of entry to the point of exit after receiving advice service or supplies This study shoulci lead to star dartization of procedures and functions and evolution of -lork norms CognatE st tdies of the working procedures at uni-purpose family planning clinics and su~ply SEssions should also be undertaken An essential component of these ~ tad ~es would be to examine Nhich functions currently performed by docshytors lealh visitors nurses and midives respectively hav~ become so roushytinize ttl it they can he relegated (0 the next 10Her level
435 Reated to working procedures is the problem of job description of medcal 8nd parrunedical personnel involved in family planning from the centra i tc the field level This job description needs to be studied wi th a vie VIW8Id txaminiDg the uttlization of skills and allocation of time by the staff lcc(rd~ng to the functional prj ori ties
436 frV management consultants should study the workings of the curren slralgements fOJ family planning counselling under the Post-Partul11 Post-Abortal Education and Referral Program at the Port-of-Spain and San Fenaldo General Hospitals
437 SU1ect to the ItBrcement of the Gove1nment the management conshy8ultal ts ~hOLlld undertake a study of th requirement of field workers (home vinitcru) in tmtlUI of are nnd population cov(ra~e
ANNEX 1
Names of Persons Met
Ii Mr T C Taitt Pem1(H~nt 3~crtarY) Ministry of Health
2 Dr M n Henry Chitd Medical Officer Ministry of Health
Ellubeth Quam a Prindpal Medical Officer (1S)
4 Mr G Z Jaine ~ uJiector Population Council
5 Dr Norma Andrews Medical Officer Population Council
6 Mr Jc~n Coury~ Evaluation Adviser Population Council
7 Mr A Jriseph Principal Statistical Officer Population Council
8 Dr C 0 Colman Country Representative Pan American Health )rg ni~ation
9 Mr ranca Kippel Health Education Specialist Ministry of Iea th
10 (1 bullbullines Principal Nursing Officer Ministry of Health
11 Dr Mx won (formerlyHinistry of Health)
12 M3 late Carops Ex-Chairman of Population Council
--
4i 1_ middotIIlt F-ntCWclOotf_Y v OJ t tl
GOVIIlHMEIgt(I OF TINIOAD AND TOampAGQ - NNISTJY OF HIALftf AIJIE1 2NATIONAL FAMilY PLANNING PROGRAMME
F MIL Y PLANNING CUNIC CASE CARD - NEW CASES - NFPPl
li ~~___ 1 ________
~ ecll-U
-- --------------------- shy~) ~~middot~------------------~~~~~~---CIJ------ middot~ii--middot-middot----middot-middot---middot--------- shy
ltv Writt N_ 01(111________________
a ~4itiJtmiddotl_____ ilIIIltIoI~____~____~-__----- shybull ~4
fie l$ - JO tDql IIfIA- tr-JMimiddot _ iJ 1 Odoor o
14aorielaquol_ _~ 0 lio witIleo-La ~ 01 bull - OJ ( _01 1~ltgt1lh o bull- 0$
AacJcu 0 2 CIIriIWA 0 J Os 0
Yv~MONTH ltnollOf~nfIGHTI
Undu 1100U$ Utgtdn 5SCI Undu 11200 01 ~ 50 - 9949 amp100 - 1199 02UlOO - nn9E~ (
0)~ 10- $99 SiOO -- U9~ lOO -- U99 12400 - 1359)-------_-r----shy ~l)o SIS n600 - Hm1300 -- 019 OJ200 il~9 ~------ 99~ a 1)0 m Os1)00 -- l99 1400 -shy $4100 -- 1S999r--- shy
1500 donl S6000aad O399 - lt499I~- I 0lt
ltII
IJ -IC _~tltlioltgti lS
02 IaampJIIocI OJ 04 laM Os
w Oltwio I_-l(~u IrIaa U
h~~ ~Clubl 01 OJ
IS ~C-n 01 toSIitDI 02
Ji poundI on 01 IriIIIuy M ur 02 IV OJ
WU 10 pltIoII~ llaMtl 411 cIIiId 01 Ol it fIolto ~ do~ _14 rou IIlgtJo 1Ia1 ___~_ shy
40
It _ I 00 ~bull FPIiIJ 1
OJ 02 OJ 06
)0 III- iy wOWcf ~1
aMIIl Os
11 T 1gtlt ( h _______ 4)~
06
04 (MIbullbull middot bIrlI ~___~__~_ (-fIJI ~- -~-- (1HJ 49middot SJ
U 10k 01( 1__ raquo$-4
iU1) DOl F ToWotfOlnC DOl 001 or Do [IP 006 001 OIIgtu___Spltclty DOll Nltmo 010
U1Mo I orcpmiddot laquo55middot16
1lD 001 Foam Toblelf_ICim DOl Condom DOl CoomS~ 004 oe Oos WlttuJn 1J OIkr DSpody) 101~ ~Iu 006 Rhylhm 001 DOG OJO
no wI~lmm 4 cd
(I 0) 1110 01 Condor 03 (lorn bull l S~muoidIl 04 Faa TabioolfIIltr- Os RhyUlm 01 lnJrl tible O Advico 090 06
la slt 1)0 19 loti ~rltnlt) ([)sl or 1llOn) ____ --__ bullbully-J n SV - ~JcdS
v~ Cl NCI 0 30 OJI_O I Wr blJ1h 0 I ~ OJ 1 ~ (fOOd V 01 No 02 laquo 6) Cf4
WIiI 1 172
004 001
j D middotmiddot middot
1 ~
r
~
bull I
bullI I I
r c i
ANNEX 3 Pagemiddot 1 of 5
0 raquo rshy -lt l)J ~ 111 t G) 5 shy (J) ~ -
fT1u
i
MINISTTY OF Ho1TH
NTIONl F~ILY LNNING PR-GRbullbullM-tE
~~5tructions to C11nic ClerKa
How to co~ploto the Daily Rogister
~~ ~~v1sd Daily Rosi8ter replnc~D tho one which is now in use tb$ Monthly PC~ri rOt~ arti tho 01( Ci() Dod PollJ j f m It is a pre-coded form and 1411 cl~1p Jd tl a1I6iniul-mIHvn Oel Clinic nctivi~y
110 )rm rollt biJ coupJot)d lrl cupLtcoto using a o(roon shoot Tho top aheot or oriinai ~ust bl) 6(Ult to tho CQgt1tral O[[lCO and tho carbon copy retained in the Gliaic rilo dll the for6a that ar uD~d betwoen the 1st 4nd the 15th of the oIIollth aut bo subClittud tocho office 35 Lnc blttch Those oomp1cted betwoon tho 16th _lid tqemc of tho month must bo ~cnt in a secJnll batch
P lOvLior hns boon Illllde for 25 clients on cZlch forlll new forlll must b IIlied f r poundh 50[810n2 whothur or not ono or lIIore session are hoIdiit the clinic on he sarne day
I th ro alO more htl 25 clionta 1n attondnnco at tho session the additi shyOhAl m~bOl of clionts 10 clients nu~ber 26 27 etc sh0u1l be ontered on the next Imiddotrlll ~i ttout a1tpoundring the numbtlrs in the cvlumn hond Series
51 ppOfil th~ number of aUcnts lQr that session ws 5 this would mean thllt two rJlS ~ lst be 6ubllIitt~dl the first filled uF 1 tltgt 25 And the laquoIncond 1 to 10 Th~ cal bon ofies should bo st~plod togother at thu t0P l~rt h4nd corner of the torm ard ktpt in the Clinic filo lou IIlU6t stapl~ the originftls in the 8~~ monnshyer for lIub~ssion to the ofticl
ie h~ ll idontiflctior- (cc 1 - )
0 lot Ji 9 anythin~ hGro poundhia is int(mdClc for tha computer code
2 ~~pound~ - Print clOflrly tho name of your Clinic
C1Lic Huml or - (cc 4 - 8) Evar1 Clinic Numbor has 5 digits Virite each dig t il a t$purate box
It Pai~_thllsectgdllion (00 lt) -1 1) - Dl monll 10M
lw) bolte IlrO proY140d fetr olAoh pr 01 thQ dISh Enter tho dA) ldns a R
d16ih
emiddot5middot (0 11 I for 115t ( 0 21 for 5th etc Treat month the am pay
e ~ 10 ~ I for I-hrch 0 [2] for September Tho y~nr must be (into ad
I Z I ~ I I 71 q etc
Take as in IixulIple tho dOlte 3rd tllrch 1973 7~ie must bo written
[0131 LSLDI[7l3JDny Month Ye~r
5middot 1~J $~~ - Irom ~-------- To --------shytntol hOI II the time the Clinic 111118 in SW5sion emiddot8middot
(i) 11011 500 lm To 1200 non
(11) Frclt 100 pm To 400 pm
(iii ) IX-OG OO pllI To 6~00 pm
f
2
ADEJ ) Paae ) of S
6 Eov
_ 1hA 1gtIpoundC iIIUlt be nu~o7Ifd tler1ally 1 throurh n lU tbey Are Wled In ~1l8ellJ IInel 1301 tlU 1 Orcl 1 Wled tor a o5038ioll - -I 2 tonY tho _boul~ b I1WJbtl 1 and 2
hlrlll are 25 linos OIl the fOnl Ilnd thoae muet be UBtleS for 25 clients 9 one ior bullbull 01 I ini
ot ~h lc II ol1cM lOlivpound til e linic before soeinc DurOI or doc tor ilnc ii hox rristrltltion nUlJbet had alrearll been recorded on the Dai 1y Roiuter then n line ~hollld be drawn through that entry an1 the eliort nust not 06 includttd in tho totals tor that 0eDion
1lw Ileifitration Num)~r of cueh client must be IiIritten IS n 5-dlrlt oode ClhnC IH11IlElr 315 1IIU8 tborotore be enterod 18J010117]5]
~ Clt ZOt
Coda 1 Codo
10 ~tl c 2t j co 21)
~w elSe - Coda 1 0) d CltaEl - Code 2 Revislt Code 3
Only pound1 01 theBe coiles may be usod
11 prol-O~ ~Eil~1 (cc 22)
If ma climt was L drop-out IIho haoS returned now to the Clinio tor tho first no linmiddot bullwin lt1ro1eo o t he or she should be given CCe 1 It this do 5 II It nprlly leu this colWlln blank
u Hothod middothisllill loe 23)
NOh til t otly ~ Cod 16 tp he ontered in 2lpound of the columna oven thOUGh 10 co11lllJlB 10 provided on the torm The Codes llrol-
Oral Contraceptive Code 0 1 U D Code 1 Condom plUD Codo Z Condor (only) Code 3 Foum tAblets cream Code it DitphrClGJII Code 5 Rhythm Cde 6 Injectible Code 7 Advice Code 8 Other Code 9
It for middotDo-le 1 client rlllll ji yen cclldorls ord foam or creall Iou Qust entor Coole i (condom plulJ) in the appropri~te column This Quat be the only lIotmiddot) tarcie If an in the cnse of a tlnle clinic I the client is Bup)lieu lith COIlOrW only you rmot entEr CorlQ 3 (cpndolll) Do not use a ticII ~ tho (odo Nwber
It is CUi tomary fur 11 cliont 110 is beine put on the oral contraceptive for the first tiT1o and even on other occasionn be issued condoms and 11 crelle or foam a Ilell rI3 a pgtcket of pilla In such Cllses when the piDQ Ilre Ilctually iouou you tlust record Orll (Co~e 0) 08 tho onll metbod ilo othor ntry sll0uld ho nnrlo
Uovever n SJC~ canas vucru condoms and fOHa ~rc eiven but no pilJa (even thoJRh _t _n the intention to issue pills nt the noxt vioit) than the Mothol Th5 ifli t ohoulcl be recorded uo Condor Plus (Code 2)
13 Seen Bybullbullbullbullbull
~rot S-1 SO l
Doctor (Dr) - Code 1 j Nurse (Nul ) - Code 2
Clark (Olk-) - Code If tho Clhnt is vcen hy both tho llootor tlnd the Nurse enter Code 1 t Doctor It 6~61l by the Nurso only arite Code 2 Cod bullbull Cerk is l)llnt for FA Cllnica Clerks in tho Government Cli1t hiwo Llttoll istructed not to i56uo supplios on their own volition
14 fl221~
lhio S~tiCl of -Ie fvrtl t~ke 16 (llrci coluMna (cc 25-+0) nnd 10 tho only part at th iOIQ in llich iore thAn one cod is Zlccoptl1blo Tho purpoco of the )ecton is to 0 able to arrive nt the Cjunntity of 6tock dilltlitJutshyed YOI IIlUdt writo in the CllllOjH-iata colulna the nUllbJr of Il1ch 4rtic1o i~JSu~d ~lo e ha I Oral Contrcilpti vea are aub-di vi dod into types ae_ 3 PIllCKC 9 0 Elynnn LlUot be entered Codo in card column 25
If tor eXllrplc t l cliunt is iosued wi th packots of Zucynon nnd aJ(1 ~ivn 1 conuotll (8inoloo) you ouot enter in oard column 25 and 11 It
cnrd col~8 )2 and J (io 1 in card colucn 2 nnd 2 1n card coluun 33) Nota C)lldoIlU ale to b(t ruoordod individually not os packots of throo) Should n ne LlondoClo be isoued thil3 is to be rc-Qed as 09
If It clint 6 t~ot isoued Blly lIupplies thon you must writo Codo 1 in CQllAlilD 41
It Q eli nt isite the clinic to check on her LUD or her Diaphra~t IUId ro DI W 6 ppl ills nre ispounducd then Code 1 1s wri t ten in column 40
In the FA clinios here a variety ot orll contraceptiveo in orer~l tho elerll wilmiddot~ bJ provided with a specill code shoot The idontifyin coo will b wiittn in Column 29 nnd the nUlber of packets iosued in colwm )0
lralaer-In Code 1 lrllllsie r~ut Coda 2 leIllPQrArr Trnnsfer-In Codo gt
In the cao of n 2ratl8fcr-In I you lUot n160 cOrlpleto coluons 42-51
In the cllU J of A ~~emporary TranGfor-1n (an individual who i8 only v1citing fur clinic tor some epecial trcatcont hna who will bo rdnlnin
~middot(II~~~fO~l~SIl~I3~nn~~~h~rO~nh~1~~190~~nll 2-46 and ler rei IItrntion numbu in colullnll41-51
It the oli( nt i iNt a CrllnoforwIu - Out or loClporu1 tMn loave oolumn 1 blank
16 lr4nst(gtr-tl2~~morrry TilJnder-In (co 42-51) Forl1ltl CUn E1~ (cc 112-46)
hen you rei iatlr L irllsfcrln or Il TJlporary Trnnsfer-In you IIIUBt write I ere the five-digit clinio nucbor of the Clinic iraQ which tho ltlient Me (uIlO
2mer ]letr ~2n ~ (cc 47-51)
frlta fllao Clo r-~itrlltion Nuc~Er ot the client in the Former Clinic (i c bullbull th 1 Sis rnmiddotion ~UlIlh()r which the client carrics 1n the tormor clinio) bull
It tho Forrltl Ho( ist rntion Number iIJ not readily wnilnble you tluct oocpluto thtl epcciol [orlll Transfer-In Not Identifiod Dy Forrlcr RCGi(trn~ t10n Nwlbvr Or ~ flt)rCl is to be cOlplctcd for och cnso nnd th forlJO Ilubmi tted to thu )opllntion Prorrnnme Of fice tOGether with tho Dily Ro~iBtors lhwev~r should the clork leuTI of tho clint B FormlI Uocintra tion lUlllb r )0[(10 Cubmi ttinft the D1ily IOCI otro t hen the nUQbcr shoulo bo -ri ton in colucns 47-51 lna the special foro should lJo deotroyotl
l7 bullbullbullbullbull
r lt bull bull
ADXI ) Pap S ot S
11 UD LV~ (cc 525)
It tb( cliont io ~ivQn An IUD tor the firot tl~o then you should Sri to Codo 1 Inuort ill colurJI 52
It tho olimiddotsnt ia rvinGgtrtltld i th An I UD bullbull tben wse Coda 2 RelnDltlrt shyin (01Uil11 52
It the clLmt is ~tte~~dint chnic beruse her IUD CflClQ out by Haol (cxpll Iion i ~hcn fir te todo ~- UIlllrli1 53~
If c-ltr IU fj IIIS reov in -ne cllnic by tho doctor or nurso t~on vlritI Codec in column 5
II the eli nt otends eiLlie tld explin[l th(lt she rccovcd the IUD tlllleel nen write Coda H in Colwlm 53
It the IUD jr still within the uterus nd the WOIraquoI1 1 11rc6llJlnt thon lIrite 1gt40 4 in Column 53
lZ np h5t (ce 54) It 0 Pull 5mor ie t~ken durin thi visit tben Codo 1 ehould be ampDtere4 in ColWlln 54 Should he c110nt lltt rQ(uircd to rttturn to clin1c for a rogtol1t Pnl) t06t then CoLe 2 llhould bo middotwrittcn in column 54
It no Pllp Scou io taken tde visit Itove colUQn 54 blank
Iraferti1lli (CQ 55)
Ii the e liett io nl1 infortili tr eaoe use Cor1o Ill in colUQn 55
If tbia 1000 not tlpl lonve column 55 blonk
20 Totaltll
CO~1ploete the [)ldegO 1gty puti YI tne totals betweon the double lines nt tu b()ttctl Carrj colUlllnc 20 21 nd gt4 Must hlve tho Bnoe JllIIber and thiG Would coreslonc to the numocr ir attencbnco
Writ$ th to1ul nUlllior of Drop-Outs returned (c022)
Urito 41eo tb totnls fOJ each card column 0 to 9 under tho h(adinu Method thiB Vioit Show tho tote L fgtr OlCl type of contraceptive issued (cc 25-40)
1)0 Dot wrLte 1111 totll lUl(Ier Card Columns 15-19 29 41-51
21 COPmllh bull ~lt h~t~ Monthly ROilort
OQ thG DaLl oCator forlll thnt ccrrOspOldB to tho 1(8t 1$06610n lt 0
oth yo Olllt (vwlgtleto the items nt the botto of the [orampl This is tour ontll~1 n(olt nnd includcD tho totll lumber of sesions Ilntl tho total Iluolcr ( r crop-outs durinr the Qonth
An tiUlsilt n drir which n doctor liB in nttcndnncc is a doctor sOfll~1on and shoulc 00 re(liGtcnd in coltns 56-57 All other sessions 1116 conlliid~recl supply stllciona and thtlY 1110 rocordod in columns 58-59
the total Ilum)nl Jf drop-outo ld the drop-outs by method durinc the onth nre 10 bu oltorou in the inrlicllted boxes
72 Chad Your ~
Milke I ura th t all thE fijul4gtu rre c101r -tNever writo our nutlUQrS 50 InrjEl that they oxtend out of tho
ap~rotr1ato ~ox
Cheek to BoJa tht 1111 numuors 1110 in tho correct boxes -- CJslHloially when Writi1 the totlB
Mllxe Cirtc O thmiddott t1e infoT1I1ntion i6 clear on the corbon COllY before sep rmiddotinr the sheets
Jitn the Fomiddotl lien tly sien YOUl nr me 1t the bot tOil right hnnd corner btl forc subol ttinG it Keep tle CL rb n copy for your rocordn
i
-l ________~~---------~
I _1
Adminiatr-atlve SKVieu
P inba ~~~l1cal lrlnbin~~eltltcal -1 te~ra t~~rvicc (lnatittloaa)
--1- - shy -1------------_-L_ l-r-aJiil- shy _-L_tet1lal d
PlIinm1tJ8 atdUon DetalMid H8Il1tb ~ ________bull Care
-----~ Office of i
the FlIily _IPlill3 roarshy
1- - - -------RegiatUll urnr
ltIi 1 Drelttor Rcgicaat Director Souta Tabqo tacallortb ~ counu gt____ ~ (4 ouottet)
Off1ce of the Res10nal Diractoc L
r----- _L_ -- shy i I bull IREgional Ipitl I
District IIttaltb I bull Othn RelOl ond Hcpital CenteIntt itlt j In 1__ _shy-~- ---- -_j
J r Ii~lth
C~nlef
L
I Ihnlth lie I th Offlcu (1ft lc~
Coullty 1I0p1ta1
Henlth tentet
I

and ccord~n8tionJ there was a groHinr feeling among the members that the ouncl1 510t1d shed thE respOJ1sibili ty for implementing the program a funeL on j ch nad heuroe added on to its advisory role with the passage of time
iO the 1 ~lp~1 the lines 0 responsibili cy were not clcay (e ned and Li1 refioal system was not fully functioning The post of Re ior 3 Director crth VIas vacant The policy seems to be to strengthen the 1St tu ion of Pt()1ic Flealth Office as an 3ency for the supervi-middot sion)pound ne district sflVices (health centers health offices and school servi ces ~l thin the ccnmty
II I PRES EN STATUS OF THE PROGRAM
301 ~he adl1linistrt~ivE changes narrated in para 209 have come about at fl tin e IJhen the P1ogram has entered a phase of declining performance as is 11 Jpal en from th colloHing figures taken from a report submitted to the Populaton Council
YrUL 10C7 ~j8 1969 1970 1971 1972
--- -- ------------~~ --~ - shy----shy
Ne Acceptors 3696 2731 16207 9997 9898
(End of October)
7560
Slur~e Family PlAnnto Program Report (no date)----AsII1Ulilg that th6 ttlrollmant of new acceptors during November-December 1972 prclrd at the 8ame rate as during the ten~onth period January-October
- 9i2the total enrollmslt in 1972 would be lebullbull than 8500
3(12 lhe total number of leW i-iCCeptors for 1971 shown in the foregoing tal11e 1s at variance with the following data from the 1971 Allnual Report
- 5 shy
~ev C~~ Contraceptive Method and Agency
nm Other Advice Total New Cases
Aeny
GovrrmenC ProEllil ___~zZ(lt1____ 97____2Lbull499___~528~___4i_750~_
Farr Uy Planning Association 2814 315 607 76
Catholic MarriaAdis1ry COLnc_H____
ge
74 88 162
otal 31[10 692 8724
_--__------------------shySOlrce Natio
1973 nal p
Fam29
ily Planning Program 1971 Annual Report April
NevmiddotrneJl~ss) the declining trend in annual performance after 1969 is manifest ana conpaes unsatisfactodly to the following targets set for the Program
Targets for Contraceptive Users - 1968-72
New Accep tots Old Cases Total
1968 20noO 20 000 lO noo
1969 20000 40 000 60000
1970 20000 60000 80000
1971 20000 80000 100000
-----__shySource National Family Planning Program
p i9
------------------------------------
- F shy
3JJ3 Ttl flient recrvitTrent has fallen off since 1969 in spite of a signif Icar t xpansinn ir the number of Government health facilities providing family paarin~ services FrCli1 7Hr to year Starting from scratch the number oE GovE(nment health irlstitl1tions delivering family planning services in isollL(Od ~ily pltJfAill~I ~J in c)lchiratinn ~7ith MCa services has lWW risEn t 4 lhis ie --tdt)p to t cii1ics organized by the Family Plannin Asce1ation bull U2 by tile Catholic Marriage Advisory Council which offers the ~h)lthm meti1middot1 nT
304 1i ciecli ne d~ d re11~m2nt of new acceptors coincidentally w-Lth th~ eXlsioH uf s-crLce facilities needs to be studied to identify the factors responsible for it eg the quality of services offered the strategy of commmic at~on and motivation and management and supervision One obvious gap is he abgtence of an agercy for promotion and extension of demand for family lal 111 If services -gt tLe field reliance being placed mainly on clinic counseUn H1d generaUzmiddotd mass media publicity The need for a field promoshytional agelcy is underscored by the dropout rate In 11 draft paper prepared by the Hed_cal Offic(1r for FIrnilv Planning it is stated that by the end of 1972 t ile Heuroe approxiclt ji rHJC cun~ent users of contraceptive methods and 33 per ert dropouts
305 rht~ program is cot merely clinic-centered but also female-oriented Recent Iy mellsages aimed at m11es and stressing joint male-female responsibishyIi ty l gtT j ecillc CImt-J 1 i~gtVt~ b~~in )7cn 1n0 the cOTul1mication activity sUf1 tv) c nts Em he 2iucaccw i milc8 and che distribution of condoms to them illVC he ~n or n~d iD r GJvefl1nenC s(~ctor The Family Planning Association has a130E~k11 the irti U3 1V~ to reis ter males ln industrial employment Tllese are steps in the ri)n dtrect1ongt but the size of the problem indicates the n~ ed OI a concerted effort en a much large r scale
306 Tre Program relies largely on the use of oral contraceptives as shown in the following table
Oral Other Advice Contraceptlves IUDs Methods Only Totals ( 100)
19)9 76 20 16207 ( 100)
1970 316 63 9997 ( 100)
1971 50n 4n 365 79 8724 (100)
Family Planning Association unpublished report
----
- 7 -
Althougr amJnp the neH acceptors in 1971 the users of oral pills were only 509 ~mon~ the old cases the figure was 119 The percentage of IUD users has remiined stagnant at an insignificant level this may be partly due to consume prefErence and pctrtly outng to lack of trained staff to undertake IlTD i1srti l7U There h hOHever a visible shi ft towards the uSe of othe~ ilettods (npchani81 and chemical) attributable to a scare about the side efects nf oral connaceptives Among these conventional methods the condom s 11 os popular
307 J t )resent fami ly planning services have been extended to 48 out of 106 hellth centersoffices run by the Government and the objective is to C)Vel t1e remaining health centersoffices within a short span of time so that adice and facilities for the practice of family planning are conshyvenient Ly wa nable to the people in all parts of the country By ann large sepanit e fITti ly planning eli nics are held on specified days as an addition to norrral lealth work Besides doctor sessions at the clinics supply sessions are rur by health visitors and nllrses assisted by clerks The nurses are authorjzed tc issue oral contraceptives for a period not exceeding three months ani the acceptor is required to attend a doctor session for advice during thi jnterval In 1971 the numbers of full-timepart-time staff in Gov~rtmnf centers renderinp family planning services were
Full-time Part-time
1elical Officers 14 8
NUseMidwives 35 19
Cl~rks 3 17
Now tile low~rnment -gtbjective is to integrate family planning services into MOl services and use the same staff being used for the delivery of both types of erlices at multi-purpose sessions However so far only 1A centers have interated family planntng with Men or gpoundmeral hpalth care sessions
3011 The Family Planning Association has eight unf-purpose centers where famil) pLmring services are available ftve days a week The Association employs tilrEe full-time and ttJO part-time doctors a complement of 14 nurSeS (who llave been trained to do pelvic examinations) and 11 other clinic staff membels The Association also has a number of voluntary workers in the clinics The CithoUt Marriage Advisory Council has three clinics but their contri shybution in terms of enrallment of acceptors is not signiflcant
3)9 A Post-PartumPost-ALortal Program was started in 1969 It is state I tlat about 14 percent of the patients reached attend a family planning clini~ 1iTj thin six weeks of the interview in the wards IhiR is qui te a low figur In 1970 when a system of home visits was tried under the Family Planning Aide Project in 7 clinics the rate of acceptance doubled in three clinils rose by 50 percent in two clinics and increased by 24 percent in one clini (No change was noticeable in the seventh clinic) No decision has been Inad~ tmiddot) continue extend or modify this Project
A Po~ulaton Council ~-----------
401 he fu~ura ro~ Lh~ ~~~01ati0n Council has to be considered in theli1 A the tasK t~ lL ahead of the ~ational Family Planning Program At pesent tile officil~r(QSrJ1Tl is prirnarily concentrating on two objectives (a) tIlE excpound1sinrt of fmd plannin~ services to tie remaining 58 health centen cLJs as rapi(ily as possible and (b) the integration of family planniT g VI tr MCH services Thus thG administration of family planning serviCHJ will be merged into and become part of the Community Health Services Since t is ()rganizationally undesirable to disturb unity of command a separa1e elteecutive agency for the administration of family planning services is preempted within the existing policy framework An executive role for thp Pcnulc tinn Council is there fore ruled out on this consideration
402 If the Population Council is to function as an advisory body at the p()Lic~ aId progra1l pLilnni-l level snd not to concern itself with the minutile If program execution there wonld be no advantage in giving it a statutory stltuS But if it were the policy of the Government to set up a verticll )middotro~ram for family planning ii th a field organization separate and distir~tOroll the HeaHh administration it would be quite appropriate to establish an autonOiTiOUS statut()y a~fgtny ntside the departmental setup of the MinisiY of Health d~b a budi~t md staff of its own commensurate vith the rE spo lsi hi Ii ty to be rEs j Freed from the usual departmental conshystrailts ~n the matters Cif sp(ndlng a1d hiring and firing of personnel such an aglncy c(uld move faster than a heavy-footed departmental formation wi thin a Mins trl bull Hovever a hody of this eharacter would need to be cas t in a cliffe ent m(ld than the present Population Council The shape that it would take lrould be more like a Board of Management with a full-time Chairman or Execuive Director and with more functional expertise than representational charater But an advisory council with an autonomous status and no responsishybilit f( r lrogrrun eXIGulion iould be a source of friction
403 r~e existence of the Population Council as an organ of policy advici has certain advantages Firstly it is a forum for developing a national poLicy in which officials and non-officials participate Secondly it pr )vi bulles a focus to ti1e official program vhich it otherwise may tend to lose as ~ontraceptive services are merged into the general health services Thirc lymiddot- and this is important -- the Ministry has extra-departmental advice availabL to it~ but the Ministers constitutional responsibility for the condl ct )f the national progl~lt~ le1lains unimpaired
404 ls an advisory Q(dy the Population Council should be more broanshybase( than it is at present For instance it should include representatives of tile organizations of employers and vorkers associations of the medical nursngmct teaching professions and organizations for womens welfare The Counil should also haye a social scientis t on it On the official side the
- 9 -
Permane It Secetary and the P1O (fen and FP) should be brought into the Council he inclusion of the Permenent Secretary would open a channel of communi~aton with the MOR ae the highest policy level next to the Minister and would (ontribute administrative expertise to the deliberations of the Cou1ci1 ~m f icili tali 5 (pleuenrti)D of th~ recommendations of the Council within the -rni and in OUltL depa-cments The inclusions of the PMO (MCH and FP) wOlld el) emphasi ~2 hs responsibi lity toward the family planninR program Some officrs of the HOH (eg Chief Health Educator Principal Nursin~ Office e) may 111 ea~e to be members though they may attend as requirE d nmiddot the agenda before the Council A representative of the Ministry of Fin nee stQuId be inc~uded in the Population Council This would make for a lettr appreciation of the needs of the Program in that Ministry and fadIi ate fj nancial sanct ions
B A~tatutory Council
40S In the foregotng Pgraphs the view has been expressed that within th edsting policy framework an advisory Population Council would be more tli)prcpriate than a COlincil wi th executive functions and powers that an advisory rOUlcil would not gain by having a statutory status and that if a statl1tory body 5s to be set up in lieu of the existing Council it would need tC b structured more Iiice a Board of Management than a council wi th a repre13entttional charact~( n the latter event the statutory council should have fu 1- time Executive Chairman or failing that an Executive Director functj oni1g undel- a Chairman trno can devote considerable time to the business of tlw COlncil
406 T1e Statutory Council should have its own budget with full operashytiona pOlo1ers It should have the authority to appoint its own staff and regulLte their conditions of service If it is constitutionally possible the Couner1 shollld be outside the jurisdiction of the Public Service Commission in pesornel matters
407 As an instrument of Government the Council should be subject to such ~eUfral or specific directives that the Ministry of Health may issue to it frcffi ime to time This should be written into the statute under which the Cmntil is set UD
408 The composition of the Council ould depend on the functions assig1ed to it It is suggested that the Council should not concern itself wl th the delivery of cliric selVices in the field The Ministry of Health may (ont nue to administer rampmily planning services at Government hospitals health cmters and health offices and the voluntary agencies should run thei] OWl ~rogram The following functions may be handled by the Council
- to shy
s rrogram plannin and target-setting
b proram monitoring and evalllation
c wiL of d 1ci(JTIdnCf by inspections
d Qrg8lizatim 0 es and marketing of contraceptive J~1J-s BLl (iV es at subs idi zed rates through es tablished 1 2 d(~ channel
e information mass media communication and audiovisual ublicity in the field
f prorrotion of famil~r plannIng acceptance through face-to-face cotlmunication by poundi eld workers in domiciliary visi ts
g trIining of personnel
II pr )motion of -esearch enJ
i financial support to voluntary agencies providing family planning services
409 n Statutory CCii1cil may corsi5t or an eminent non-official vith a comri tm ~~1t towacds foJlily plailninf nd the fol1owin~ members
I ~ bull Pfrmanent Secretary ltl-tIlH
Chief Hedical Officer HOH
i Principal ~ecHcal Office ~mH
d Pilhlic RellltionB OfJte(middotmiddot Prtm~ Ministere Office
A represen ta ti V~1 of the Ministry of Education
f ~ representative of the Ministry of Finance
g A representa~ive of the FPA
h A representative ot the C1AC
i H social scientist fcum tle University of the ~Jest Indies
j Three non-officials with experience in management and administration and the
k Director of the Family Planning Program - Secretary
- 11 shy
The COUlcil ITIltW constitute cOlClmittees for Finance - Accounts Personnel and Sup lies nd Stores ir~whi ch )nly members may be included Other commitles sc1h as those 01 training info1nation and education and researCl ara ~valuation r1ili also include experts from outside
410 he Off1ce raquo) cc im Panning Program which at present forms part of th ~Hnis try or [i n should be placed under the Council and its staff strelgtl ilcn~ii2 i~ r181 it may cease to depend upon the services of the Mir is t y of H~alth
C Office of the Family Planning Program
4 11ollwther the Offic~ of the Family Planning Program remains a part of the Mirisry of Health or is transferred under a statutory council if one is set uP i needs to be strengthened to meet the requirements of an expAndshying pr )gn m At present the following sys terns need to be ins ti tuted in this Office
a a 3ystem of setting annual targets for the enrollment of acceptors and the projection of service fadli ties in relation to these targets
I Ci ~ystem oE V)glC loHitoring (the monthly statistics flowing from the clini~s c~iiiain unproc(~s5erl for months)
a system of program evaluation eg demographic effect of tte program cost studies
1 an overall design for media communication based on a study of the reach a~d cost effectiveness of different media and the effect of the meflBsge content and
e a m88t~r plan for training which would comprise an assessment of the training needK of the existing staff and future reshycruits and a long-term plan divided into annual programs
412 Th2 Prograll afiie s~lould have the services of a demographer and a meeia expert A training adviser is expected to be provided by the PARO
413 1be Program Office should evolve schedules of field tours to overliee field operatio1s E~1eh health cente heal th office should be visi ted peridicaLy by the Milt~dical fElce- the Nursing Officer and the Health EduCltoI who should guide and assis t the local staff in carrying out the progam Their tour notes should go into separate dossiers for each institushytion and ~ach dossier should have basic demographic data about the area coveled by each institution These dossiers would be a useful record for revilwing l)errOmance The staff of the Program Office should be augmented to Ol)erte this control procedure
- 12 shy
D Decentralization of Powers
414 ~hete is a concentration of administrative and financial powers in the 11in s try of Health I-JllJCi1 results in an accumulation of references in the Miristl) and delays n field operations Specific powers should be delegated ~o (a) the PliO concerned with MCH and family planningmiddot (b) the Directcr o the Program Office (c) the Regional Director and (d) the County Medica1 Oficecs The Ministry should invite suggestions from these officers and wOlk 01t a schedule of delegated powers
415 A tdgh priority in the matter of delegation of powers is to arm the Regiond Directors with sufficient administrative and financial authority to implement with expedition the health and family planning programs of the Ministmiddoty 1 thin the areas in their jurisdictions
E Integration of Family Planning wi th Haternal and Child Health Services
416 At present family planning services are being provided at 48 Goverrnent hospitals health centers and health offices by using the full shytime E taf cf these institutions and employing part-time (sessional) doctors nurse~ anI clerks where necessary At 29 of these institutions separate famil cl~nics are held on specified days in the weck some being doctor sessi(ms mel others supply sessions run hy nurses and clerks At the remaining 18 imtit1tions family planning services are combined with antenatal child healtL cr postnatal services The Family Planning Association runs 8 unishypurpoe f am ly planning centers which provide daily services and contribute a 11 t le less than half the total number of new acceptors per year
417 N assessment has b~en marie of the effect of integrated MOl and famil~ p~ nnning services an the recrl1i tment of acceptors nor were ~ data readily avallable for this purpose It may be observed however that in a situation of shortages of trained personnel for health services utilization of the existing health staff and facilitieR for family planning is inevitable parU cllLrl y in the interior where such shortages are more pronounced This underlines the need of evaluation of the integrated xai and family planning progtam for its impact on the number of acceptors Also a study needs to be made of che utilization of medical and pilramedical manpower so that it leads to bdter ~llocation of duties and optimUJl utilization of personnel
418 ile integration of faMily planning into Mcn services has certain advalltages as well as attendant risks The advantages are
a Lbe association of family planning with the care of mothers and children helps project a benevolent image of family planning as a program of family welfare This creates a
- 13 shy
1imate favorab~e to the acceptance of family planning aa lt p-)si tL1e il-Eare rreasure rather than a negative program cE limiting c~ildren
h t elps erlist ~r2tion tf doctars and nurses who as c -~ass enjo tft~ Y)er)et~ a~d confidf~nce of the communities i712~ Eerve
c ~ieD of contact with women
d luni-purposa clhlics for ~lCH and family planning services are onenient for motn~rs who would have to travel considerable (listances to the clinics
e hete is better utilizat1on of Acarce heAlth manpower
419 he limitatio$ of integrating family planning with MCH servicesI
are the posiOili ties of loss of focus on family planning as a high priori ty prograrr ald the diffusion of pol1sibility for its implementation These could tlow ve r he safegurded agaifls t by adopting the following measures
a 11e job descriptions of doctors and nurses should be rewritten 0 include the family planning function
b hE perf0rt1iai1ce of ctoltors and nurses should be judged as much )y tbeir inteceq t in planning ~vork as in maternal and ~hjld care and this should he lade known to them
c )octors and nurses involved in ~CH services should be given middot)rj entation and traIning in famj ly planning and their interest 3UEtained by refresher courses seminars meetings and supplies of literature
d Thl techrical (xpert~ in the Office of the Family Planninl Program should maintain liaison with and guide the field agencies in implementing the family plannin~ program For this purpose schedules shoul d be marle out for periodic field inspections
420 It is suggested that the working of half-a-dozen centers where family plbnnLng services have been integrated wi th MCH sessions should be studiei for ehe purpose of standardizing the methodology of delivery of servicl~ Such a study should include staff strength patient load recoril shykeepills 10middot of patents in the clinic timing and frequency of clinic sesaios ani convenience vf patients
F Voluntary Organizations
421 I i~ internrticri31 expedence that the birth control movement is pion aTC tt volunh[~ JilC S Qltl that hen the national governments step in wi tl cmbi ti 019 prjhns wi thin the sLate welfare system voluntary bodies ieh tteir limited ilsrluces restrict their service activities and shift the emplasi i 0 educedgt (f the community training research and contracepshytive Sf vic not 1l7gtilflblr in he official program or in areas not reached by it In nagni tude and expanse the of ficial program in Trinidad and Tobago has alrad~ orertak~n Ce 101umary program Increasingly it will become the domLnart tartner in the total national program while the voluntary agencies will cOltirlU1~ to receive financial support and encouragement to set up high standaeis If service and explore new areas thus acting as a stimulus and an additi_e tl the official program
G FrOB-ram Infomation
422 Thre is no concurrent evaluation or monitoring of the Program The daa or lq72 flowing in from the clinics month by month have r8Jllsined unprocss~d tn the Program Office The official Annual Report - 1971 Sums up th~ poition as fcllo~s
ITThe Research and Evaluation component continued to be the weakest in the Population Program Although a systen of evaluation had been built into the program the follow-up procedures for analyzing the data and for correcting inshyconsistencies are inadequate Requests were made to extend the staff to establish a more viable unit but by the end of the year no chllnges had been made
423 T1e recording and riporting jJrocedures were revised effective Januery 1972 and there has been a further change recently at the instance of t1e Evaluation Adviser Under the system now established the clinics are lequ Lreurod to maintain the following records
a Family Planning Clinic Case Card - New Cases This was introduced on January 1 1972 and has thirty-one entries giving age parity contraceptive listory pregnancies socio-economic background ource of family planning information and agency for notvat ion bull (Annex 2) The case card is made out in duplicate for each new acceptor and a copy sent to the Program Office
b Daily Regis ter This fs a ne~gt1 form recently introduced in replacement of the old regis ter and is preparen
- 15 shy
ie) ruplicate the original to be transmitted to the Program (fHce and the carbon copy to be retained in the clinic Th~ is a very 121zborute form requiring 36 entries to be aa~ for each Chse nel and old attending a session includin~ (ntries to cit L to contTaceptive supplies issued
AijCleX 3 T~13e fcnnG are required to be sent to the Program lffce in i7JO balches every month the first batch for the i IS fif~eeL days and the second for the remaining part of hE month The trtention is that the data appearing in the ~EZlic daily legis ter forms should be compiled in the Program Office and fed back to the clinics Although it is claimed that this new form has been pretested and is workable ex)erience alone will show whether the majority of clinic cL~rks are able to cope with it in a busy session
bull o now-Ho Card TIlis card is intended to keep track of ac ceptor--It has entries for name addresfI and month fcr which a visit is due for each year
bull Aphabe tical Index This is a card index of clients with aidresses
Each i)at en is given a simple clinic card on which the dates of further appo~utnli rc3 an~ indicated A special fonT[ has been devised for the reporting ot cases unler the Post-IartumPost-Abortal Education and Referral Program
424 J system of monitoring progrRm performance from month to month need to bE develQped as a high priori ty The problem is not so much reshycord ng mc transmission of data by the clinics but its aggregation and proclssi ng in the Program Office every month which at present takes a long time The Statistical Officer should have a statistical assistant to help him Ln I he taflk Monthly progress reports should be available to the Mini H t~ n H(llllth and A11 offt eerlil of the ProKrnm Office so that remedial ac tl m I lAY h(~ tuk~n n rll1u- WhOnh1f ~Hfl(AlJtlaTY
42 For the analysis of data and evaluation the Program office shouln haVE th(~ full-time services of a trained demographer
H Field Workers
42) Tie Program nemiddotis tne services of a cadre of field workers to enr)ll neii aceeptoTs follow up acceptors in their homes and revive the int 2remiddott of dropouts Such a category of workers could also be utilizerl for pr1fficting other health programs such as the VD campaign and the inmuni~ation program
47 As an experimental measure one field ~]orker may be assigned to a emi l~ of Hi 000 population This would mean 100 field workers in all
- 16 shy
Earh of the workers should preferably have harl a higher secondary education otherwLe 1gt junior secondalY education They should be married persons with middoti1ltt mot tl-an two or tlree children recruited from the locali ty in which they armiddot~ requlred to function Only persons who have the capaci ty to comnunl at~ and or6anl~e should c chosen A months ini tial orientation
slcu1d enable them to start functioning in the field though reshyfresher CO rSeS tvould be necesslt1ry in due course In Port-of-Spain married mer~ a1C women may be employed on a part-time basis
I Hanagement Study
428 A nanagement study of the Family Planning Program should include a sctu iny of the top m~nagement Atructure (Population Council - Office of the Fanil) PLanning Program - Principal Medical Officer for MCH and Family Planni Ig fetices) the field structure for the delivery of family planning servics (Re0ional Director - District Health Services) including the utilizlti(n if medical and paramedical personnel for adding the function of del ve y )f family planning services and the control and communication proCed1reF Lfnking the top management with the field structure
429 The management consultants may study the functioning of the Popul tio I Council and advise whether it adequately serves the purpose of givini po Licy direction to the Program and if not what changes in its compo itt m and operating procedures may be introduced without altering its bsic craracter as an advisory agency The consultants may suggest an alern at ve form of organizati)n and utilization of personnel which in thir p nion may be better adapted to the needs of the Program
430 Irrespective of whether the Population Council is maintained or it is replaced by an agency of a different character a formation like the Offic of be Family Planning Program would be necessary for the administrashytion i)f 1 he program a task for which i 1 appears inadequately equipped at preselt Its obvious requirements are in the areas of program monitoring and el7alnation program supervision communication and training The manag ememiddotlt consultants may study the structure and procedures of this form~ tio Gnd make suggestions with regard to the augmentation of professional and ~ upp)rt lng staffgt and modification of operating procedures
431 The linkage of the Office of the Family Planning Program with the Miniutry of Health (Central Office) and the District Health Services should be sudied In view of the policy of the Government to integrate MCH and faI11iLy rlallning services it should be examined whether the Principal Medi al Officer for Communi ty Heal th Services (MCH and Family Planning) should be agtpoj nt~d as the Chief of the Office of the Family Planning Program and an adTlilistrative officer of a suitable level inducted in that Office to assist him TIle implication of this suggestion is that the head of the Family PlanJling Program would control the District Health Services
- 17 shy
432 rf 1e management consultants should examine the delegation of adminshyistratiie Bld financial powers of the Ministry of Health to different levels of Progam aclrlirdstration viz bull PMO Program Office Regional Director and County ~djca~ Officers
l33 he system of 01 af Togram information from the clinlcs to the Pr()~ra1 O~fice and tOile processing and use of information in the latter office iholld )e studied
434 he working procedures at the integrated McP and family planning clinics shnuLl be studied This would involve a study of each stage which a clien tpcticmt has to go through from the point of entry to the point of exit after receiving advice service or supplies This study shoulci lead to star dartization of procedures and functions and evolution of -lork norms CognatE st tdies of the working procedures at uni-purpose family planning clinics and su~ply SEssions should also be undertaken An essential component of these ~ tad ~es would be to examine Nhich functions currently performed by docshytors lealh visitors nurses and midives respectively hav~ become so roushytinize ttl it they can he relegated (0 the next 10Her level
435 Reated to working procedures is the problem of job description of medcal 8nd parrunedical personnel involved in family planning from the centra i tc the field level This job description needs to be studied wi th a vie VIW8Id txaminiDg the uttlization of skills and allocation of time by the staff lcc(rd~ng to the functional prj ori ties
436 frV management consultants should study the workings of the curren slralgements fOJ family planning counselling under the Post-Partul11 Post-Abortal Education and Referral Program at the Port-of-Spain and San Fenaldo General Hospitals
437 SU1ect to the ItBrcement of the Gove1nment the management conshy8ultal ts ~hOLlld undertake a study of th requirement of field workers (home vinitcru) in tmtlUI of are nnd population cov(ra~e
ANNEX 1
Names of Persons Met
Ii Mr T C Taitt Pem1(H~nt 3~crtarY) Ministry of Health
2 Dr M n Henry Chitd Medical Officer Ministry of Health
Ellubeth Quam a Prindpal Medical Officer (1S)
4 Mr G Z Jaine ~ uJiector Population Council
5 Dr Norma Andrews Medical Officer Population Council
6 Mr Jc~n Coury~ Evaluation Adviser Population Council
7 Mr A Jriseph Principal Statistical Officer Population Council
8 Dr C 0 Colman Country Representative Pan American Health )rg ni~ation
9 Mr ranca Kippel Health Education Specialist Ministry of Iea th
10 (1 bullbullines Principal Nursing Officer Ministry of Health
11 Dr Mx won (formerlyHinistry of Health)
12 M3 late Carops Ex-Chairman of Population Council
--
4i 1_ middotIIlt F-ntCWclOotf_Y v OJ t tl
GOVIIlHMEIgt(I OF TINIOAD AND TOampAGQ - NNISTJY OF HIALftf AIJIE1 2NATIONAL FAMilY PLANNING PROGRAMME
F MIL Y PLANNING CUNIC CASE CARD - NEW CASES - NFPPl
li ~~___ 1 ________
~ ecll-U
-- --------------------- shy~) ~~middot~------------------~~~~~~---CIJ------ middot~ii--middot-middot----middot-middot---middot--------- shy
ltv Writt N_ 01(111________________
a ~4itiJtmiddotl_____ ilIIIltIoI~____~____~-__----- shybull ~4
fie l$ - JO tDql IIfIA- tr-JMimiddot _ iJ 1 Odoor o
14aorielaquol_ _~ 0 lio witIleo-La ~ 01 bull - OJ ( _01 1~ltgt1lh o bull- 0$
AacJcu 0 2 CIIriIWA 0 J Os 0
Yv~MONTH ltnollOf~nfIGHTI
Undu 1100U$ Utgtdn 5SCI Undu 11200 01 ~ 50 - 9949 amp100 - 1199 02UlOO - nn9E~ (
0)~ 10- $99 SiOO -- U9~ lOO -- U99 12400 - 1359)-------_-r----shy ~l)o SIS n600 - Hm1300 -- 019 OJ200 il~9 ~------ 99~ a 1)0 m Os1)00 -- l99 1400 -shy $4100 -- 1S999r--- shy
1500 donl S6000aad O399 - lt499I~- I 0lt
ltII
IJ -IC _~tltlioltgti lS
02 IaampJIIocI OJ 04 laM Os
w Oltwio I_-l(~u IrIaa U
h~~ ~Clubl 01 OJ
IS ~C-n 01 toSIitDI 02
Ji poundI on 01 IriIIIuy M ur 02 IV OJ
WU 10 pltIoII~ llaMtl 411 cIIiId 01 Ol it fIolto ~ do~ _14 rou IIlgtJo 1Ia1 ___~_ shy
40
It _ I 00 ~bull FPIiIJ 1
OJ 02 OJ 06
)0 III- iy wOWcf ~1
aMIIl Os
11 T 1gtlt ( h _______ 4)~
06
04 (MIbullbull middot bIrlI ~___~__~_ (-fIJI ~- -~-- (1HJ 49middot SJ
U 10k 01( 1__ raquo$-4
iU1) DOl F ToWotfOlnC DOl 001 or Do [IP 006 001 OIIgtu___Spltclty DOll Nltmo 010
U1Mo I orcpmiddot laquo55middot16
1lD 001 Foam Toblelf_ICim DOl Condom DOl CoomS~ 004 oe Oos WlttuJn 1J OIkr DSpody) 101~ ~Iu 006 Rhylhm 001 DOG OJO
no wI~lmm 4 cd
(I 0) 1110 01 Condor 03 (lorn bull l S~muoidIl 04 Faa TabioolfIIltr- Os RhyUlm 01 lnJrl tible O Advico 090 06
la slt 1)0 19 loti ~rltnlt) ([)sl or 1llOn) ____ --__ bullbully-J n SV - ~JcdS
v~ Cl NCI 0 30 OJI_O I Wr blJ1h 0 I ~ OJ 1 ~ (fOOd V 01 No 02 laquo 6) Cf4
WIiI 1 172
004 001
j D middotmiddot middot
1 ~
r
~
bull I
bullI I I
r c i
ANNEX 3 Pagemiddot 1 of 5
0 raquo rshy -lt l)J ~ 111 t G) 5 shy (J) ~ -
fT1u
i
MINISTTY OF Ho1TH
NTIONl F~ILY LNNING PR-GRbullbullM-tE
~~5tructions to C11nic ClerKa
How to co~ploto the Daily Rogister
~~ ~~v1sd Daily Rosi8ter replnc~D tho one which is now in use tb$ Monthly PC~ri rOt~ arti tho 01( Ci() Dod PollJ j f m It is a pre-coded form and 1411 cl~1p Jd tl a1I6iniul-mIHvn Oel Clinic nctivi~y
110 )rm rollt biJ coupJot)d lrl cupLtcoto using a o(roon shoot Tho top aheot or oriinai ~ust bl) 6(Ult to tho CQgt1tral O[[lCO and tho carbon copy retained in the Gliaic rilo dll the for6a that ar uD~d betwoen the 1st 4nd the 15th of the oIIollth aut bo subClittud tocho office 35 Lnc blttch Those oomp1cted betwoon tho 16th _lid tqemc of tho month must bo ~cnt in a secJnll batch
P lOvLior hns boon Illllde for 25 clients on cZlch forlll new forlll must b IIlied f r poundh 50[810n2 whothur or not ono or lIIore session are hoIdiit the clinic on he sarne day
I th ro alO more htl 25 clionta 1n attondnnco at tho session the additi shyOhAl m~bOl of clionts 10 clients nu~ber 26 27 etc sh0u1l be ontered on the next Imiddotrlll ~i ttout a1tpoundring the numbtlrs in the cvlumn hond Series
51 ppOfil th~ number of aUcnts lQr that session ws 5 this would mean thllt two rJlS ~ lst be 6ubllIitt~dl the first filled uF 1 tltgt 25 And the laquoIncond 1 to 10 Th~ cal bon ofies should bo st~plod togother at thu t0P l~rt h4nd corner of the torm ard ktpt in the Clinic filo lou IIlU6t stapl~ the originftls in the 8~~ monnshyer for lIub~ssion to the ofticl
ie h~ ll idontiflctior- (cc 1 - )
0 lot Ji 9 anythin~ hGro poundhia is int(mdClc for tha computer code
2 ~~pound~ - Print clOflrly tho name of your Clinic
C1Lic Huml or - (cc 4 - 8) Evar1 Clinic Numbor has 5 digits Virite each dig t il a t$purate box
It Pai~_thllsectgdllion (00 lt) -1 1) - Dl monll 10M
lw) bolte IlrO proY140d fetr olAoh pr 01 thQ dISh Enter tho dA) ldns a R
d16ih
emiddot5middot (0 11 I for 115t ( 0 21 for 5th etc Treat month the am pay
e ~ 10 ~ I for I-hrch 0 [2] for September Tho y~nr must be (into ad
I Z I ~ I I 71 q etc
Take as in IixulIple tho dOlte 3rd tllrch 1973 7~ie must bo written
[0131 LSLDI[7l3JDny Month Ye~r
5middot 1~J $~~ - Irom ~-------- To --------shytntol hOI II the time the Clinic 111118 in SW5sion emiddot8middot
(i) 11011 500 lm To 1200 non
(11) Frclt 100 pm To 400 pm
(iii ) IX-OG OO pllI To 6~00 pm
f
2
ADEJ ) Paae ) of S
6 Eov
_ 1hA 1gtIpoundC iIIUlt be nu~o7Ifd tler1ally 1 throurh n lU tbey Are Wled In ~1l8ellJ IInel 1301 tlU 1 Orcl 1 Wled tor a o5038ioll - -I 2 tonY tho _boul~ b I1WJbtl 1 and 2
hlrlll are 25 linos OIl the fOnl Ilnd thoae muet be UBtleS for 25 clients 9 one ior bullbull 01 I ini
ot ~h lc II ol1cM lOlivpound til e linic before soeinc DurOI or doc tor ilnc ii hox rristrltltion nUlJbet had alrearll been recorded on the Dai 1y Roiuter then n line ~hollld be drawn through that entry an1 the eliort nust not 06 includttd in tho totals tor that 0eDion
1lw Ileifitration Num)~r of cueh client must be IiIritten IS n 5-dlrlt oode ClhnC IH11IlElr 315 1IIU8 tborotore be enterod 18J010117]5]
~ Clt ZOt
Coda 1 Codo
10 ~tl c 2t j co 21)
~w elSe - Coda 1 0) d CltaEl - Code 2 Revislt Code 3
Only pound1 01 theBe coiles may be usod
11 prol-O~ ~Eil~1 (cc 22)
If ma climt was L drop-out IIho haoS returned now to the Clinio tor tho first no linmiddot bullwin lt1ro1eo o t he or she should be given CCe 1 It this do 5 II It nprlly leu this colWlln blank
u Hothod middothisllill loe 23)
NOh til t otly ~ Cod 16 tp he ontered in 2lpound of the columna oven thOUGh 10 co11lllJlB 10 provided on the torm The Codes llrol-
Oral Contraceptive Code 0 1 U D Code 1 Condom plUD Codo Z Condor (only) Code 3 Foum tAblets cream Code it DitphrClGJII Code 5 Rhythm Cde 6 Injectible Code 7 Advice Code 8 Other Code 9
It for middotDo-le 1 client rlllll ji yen cclldorls ord foam or creall Iou Qust entor Coole i (condom plulJ) in the appropri~te column This Quat be the only lIotmiddot) tarcie If an in the cnse of a tlnle clinic I the client is Bup)lieu lith COIlOrW only you rmot entEr CorlQ 3 (cpndolll) Do not use a ticII ~ tho (odo Nwber
It is CUi tomary fur 11 cliont 110 is beine put on the oral contraceptive for the first tiT1o and even on other occasionn be issued condoms and 11 crelle or foam a Ilell rI3 a pgtcket of pilla In such Cllses when the piDQ Ilre Ilctually iouou you tlust record Orll (Co~e 0) 08 tho onll metbod ilo othor ntry sll0uld ho nnrlo
Uovever n SJC~ canas vucru condoms and fOHa ~rc eiven but no pilJa (even thoJRh _t _n the intention to issue pills nt the noxt vioit) than the Mothol Th5 ifli t ohoulcl be recorded uo Condor Plus (Code 2)
13 Seen Bybullbullbullbullbull
~rot S-1 SO l
Doctor (Dr) - Code 1 j Nurse (Nul ) - Code 2
Clark (Olk-) - Code If tho Clhnt is vcen hy both tho llootor tlnd the Nurse enter Code 1 t Doctor It 6~61l by the Nurso only arite Code 2 Cod bullbull Cerk is l)llnt for FA Cllnica Clerks in tho Government Cli1t hiwo Llttoll istructed not to i56uo supplios on their own volition
14 fl221~
lhio S~tiCl of -Ie fvrtl t~ke 16 (llrci coluMna (cc 25-+0) nnd 10 tho only part at th iOIQ in llich iore thAn one cod is Zlccoptl1blo Tho purpoco of the )ecton is to 0 able to arrive nt the Cjunntity of 6tock dilltlitJutshyed YOI IIlUdt writo in the CllllOjH-iata colulna the nUllbJr of Il1ch 4rtic1o i~JSu~d ~lo e ha I Oral Contrcilpti vea are aub-di vi dod into types ae_ 3 PIllCKC 9 0 Elynnn LlUot be entered Codo in card column 25
If tor eXllrplc t l cliunt is iosued wi th packots of Zucynon nnd aJ(1 ~ivn 1 conuotll (8inoloo) you ouot enter in oard column 25 and 11 It
cnrd col~8 )2 and J (io 1 in card colucn 2 nnd 2 1n card coluun 33) Nota C)lldoIlU ale to b(t ruoordod individually not os packots of throo) Should n ne LlondoClo be isoued thil3 is to be rc-Qed as 09
If It clint 6 t~ot isoued Blly lIupplies thon you must writo Codo 1 in CQllAlilD 41
It Q eli nt isite the clinic to check on her LUD or her Diaphra~t IUId ro DI W 6 ppl ills nre ispounducd then Code 1 1s wri t ten in column 40
In the FA clinios here a variety ot orll contraceptiveo in orer~l tho elerll wilmiddot~ bJ provided with a specill code shoot The idontifyin coo will b wiittn in Column 29 nnd the nUlber of packets iosued in colwm )0
lralaer-In Code 1 lrllllsie r~ut Coda 2 leIllPQrArr Trnnsfer-In Codo gt
In the cao of n 2ratl8fcr-In I you lUot n160 cOrlpleto coluons 42-51
In the cllU J of A ~~emporary TranGfor-1n (an individual who i8 only v1citing fur clinic tor some epecial trcatcont hna who will bo rdnlnin
~middot(II~~~fO~l~SIl~I3~nn~~~h~rO~nh~1~~190~~nll 2-46 and ler rei IItrntion numbu in colullnll41-51
It the oli( nt i iNt a CrllnoforwIu - Out or loClporu1 tMn loave oolumn 1 blank
16 lr4nst(gtr-tl2~~morrry TilJnder-In (co 42-51) Forl1ltl CUn E1~ (cc 112-46)
hen you rei iatlr L irllsfcrln or Il TJlporary Trnnsfer-In you IIIUBt write I ere the five-digit clinio nucbor of the Clinic iraQ which tho ltlient Me (uIlO
2mer ]letr ~2n ~ (cc 47-51)
frlta fllao Clo r-~itrlltion Nuc~Er ot the client in the Former Clinic (i c bullbull th 1 Sis rnmiddotion ~UlIlh()r which the client carrics 1n the tormor clinio) bull
It tho Forrltl Ho( ist rntion Number iIJ not readily wnilnble you tluct oocpluto thtl epcciol [orlll Transfer-In Not Identifiod Dy Forrlcr RCGi(trn~ t10n Nwlbvr Or ~ flt)rCl is to be cOlplctcd for och cnso nnd th forlJO Ilubmi tted to thu )opllntion Prorrnnme Of fice tOGether with tho Dily Ro~iBtors lhwev~r should the clork leuTI of tho clint B FormlI Uocintra tion lUlllb r )0[(10 Cubmi ttinft the D1ily IOCI otro t hen the nUQbcr shoulo bo -ri ton in colucns 47-51 lna the special foro should lJo deotroyotl
l7 bullbullbullbullbull
r lt bull bull
ADXI ) Pap S ot S
11 UD LV~ (cc 525)
It tb( cliont io ~ivQn An IUD tor the firot tl~o then you should Sri to Codo 1 Inuort ill colurJI 52
It tho olimiddotsnt ia rvinGgtrtltld i th An I UD bullbull tben wse Coda 2 RelnDltlrt shyin (01Uil11 52
It the clLmt is ~tte~~dint chnic beruse her IUD CflClQ out by Haol (cxpll Iion i ~hcn fir te todo ~- UIlllrli1 53~
If c-ltr IU fj IIIS reov in -ne cllnic by tho doctor or nurso t~on vlritI Codec in column 5
II the eli nt otends eiLlie tld explin[l th(lt she rccovcd the IUD tlllleel nen write Coda H in Colwlm 53
It the IUD jr still within the uterus nd the WOIraquoI1 1 11rc6llJlnt thon lIrite 1gt40 4 in Column 53
lZ np h5t (ce 54) It 0 Pull 5mor ie t~ken durin thi visit tben Codo 1 ehould be ampDtere4 in ColWlln 54 Should he c110nt lltt rQ(uircd to rttturn to clin1c for a rogtol1t Pnl) t06t then CoLe 2 llhould bo middotwrittcn in column 54
It no Pllp Scou io taken tde visit Itove colUQn 54 blank
Iraferti1lli (CQ 55)
Ii the e liett io nl1 infortili tr eaoe use Cor1o Ill in colUQn 55
If tbia 1000 not tlpl lonve column 55 blonk
20 Totaltll
CO~1ploete the [)ldegO 1gty puti YI tne totals betweon the double lines nt tu b()ttctl Carrj colUlllnc 20 21 nd gt4 Must hlve tho Bnoe JllIIber and thiG Would coreslonc to the numocr ir attencbnco
Writ$ th to1ul nUlllior of Drop-Outs returned (c022)
Urito 41eo tb totnls fOJ each card column 0 to 9 under tho h(adinu Method thiB Vioit Show tho tote L fgtr OlCl type of contraceptive issued (cc 25-40)
1)0 Dot wrLte 1111 totll lUl(Ier Card Columns 15-19 29 41-51
21 COPmllh bull ~lt h~t~ Monthly ROilort
OQ thG DaLl oCator forlll thnt ccrrOspOldB to tho 1(8t 1$06610n lt 0
oth yo Olllt (vwlgtleto the items nt the botto of the [orampl This is tour ontll~1 n(olt nnd includcD tho totll lumber of sesions Ilntl tho total Iluolcr ( r crop-outs durinr the Qonth
An tiUlsilt n drir which n doctor liB in nttcndnncc is a doctor sOfll~1on and shoulc 00 re(liGtcnd in coltns 56-57 All other sessions 1116 conlliid~recl supply stllciona and thtlY 1110 rocordod in columns 58-59
the total Ilum)nl Jf drop-outo ld the drop-outs by method durinc the onth nre 10 bu oltorou in the inrlicllted boxes
72 Chad Your ~
Milke I ura th t all thE fijul4gtu rre c101r -tNever writo our nutlUQrS 50 InrjEl that they oxtend out of tho
ap~rotr1ato ~ox
Cheek to BoJa tht 1111 numuors 1110 in tho correct boxes -- CJslHloially when Writi1 the totlB
Mllxe Cirtc O thmiddott t1e infoT1I1ntion i6 clear on the corbon COllY before sep rmiddotinr the sheets
Jitn the Fomiddotl lien tly sien YOUl nr me 1t the bot tOil right hnnd corner btl forc subol ttinG it Keep tle CL rb n copy for your rocordn
i
-l ________~~---------~
I _1
Adminiatr-atlve SKVieu
P inba ~~~l1cal lrlnbin~~eltltcal -1 te~ra t~~rvicc (lnatittloaa)
--1- - shy -1------------_-L_ l-r-aJiil- shy _-L_tet1lal d
PlIinm1tJ8 atdUon DetalMid H8Il1tb ~ ________bull Care
-----~ Office of i
the FlIily _IPlill3 roarshy
1- - - -------RegiatUll urnr
ltIi 1 Drelttor Rcgicaat Director Souta Tabqo tacallortb ~ counu gt____ ~ (4 ouottet)
Off1ce of the Res10nal Diractoc L
r----- _L_ -- shy i I bull IREgional Ipitl I
District IIttaltb I bull Othn RelOl ond Hcpital CenteIntt itlt j In 1__ _shy-~- ---- -_j
J r Ii~lth
C~nlef
L
I Ihnlth lie I th Offlcu (1ft lc~
Coullty 1I0p1ta1
Henlth tentet
I

- 5 shy
~ev C~~ Contraceptive Method and Agency
nm Other Advice Total New Cases
Aeny
GovrrmenC ProEllil ___~zZ(lt1____ 97____2Lbull499___~528~___4i_750~_
Farr Uy Planning Association 2814 315 607 76
Catholic MarriaAdis1ry COLnc_H____
ge
74 88 162
otal 31[10 692 8724
_--__------------------shySOlrce Natio
1973 nal p
Fam29
ily Planning Program 1971 Annual Report April
NevmiddotrneJl~ss) the declining trend in annual performance after 1969 is manifest ana conpaes unsatisfactodly to the following targets set for the Program
Targets for Contraceptive Users - 1968-72
New Accep tots Old Cases Total
1968 20noO 20 000 lO noo
1969 20000 40 000 60000
1970 20000 60000 80000
1971 20000 80000 100000
-----__shySource National Family Planning Program
p i9
------------------------------------
- F shy
3JJ3 Ttl flient recrvitTrent has fallen off since 1969 in spite of a signif Icar t xpansinn ir the number of Government health facilities providing family paarin~ services FrCli1 7Hr to year Starting from scratch the number oE GovE(nment health irlstitl1tions delivering family planning services in isollL(Od ~ily pltJfAill~I ~J in c)lchiratinn ~7ith MCa services has lWW risEn t 4 lhis ie --tdt)p to t cii1ics organized by the Family Plannin Asce1ation bull U2 by tile Catholic Marriage Advisory Council which offers the ~h)lthm meti1middot1 nT
304 1i ciecli ne d~ d re11~m2nt of new acceptors coincidentally w-Lth th~ eXlsioH uf s-crLce facilities needs to be studied to identify the factors responsible for it eg the quality of services offered the strategy of commmic at~on and motivation and management and supervision One obvious gap is he abgtence of an agercy for promotion and extension of demand for family lal 111 If services -gt tLe field reliance being placed mainly on clinic counseUn H1d generaUzmiddotd mass media publicity The need for a field promoshytional agelcy is underscored by the dropout rate In 11 draft paper prepared by the Hed_cal Offic(1r for FIrnilv Planning it is stated that by the end of 1972 t ile Heuroe approxiclt ji rHJC cun~ent users of contraceptive methods and 33 per ert dropouts
305 rht~ program is cot merely clinic-centered but also female-oriented Recent Iy mellsages aimed at m11es and stressing joint male-female responsibishyIi ty l gtT j ecillc CImt-J 1 i~gtVt~ b~~in )7cn 1n0 the cOTul1mication activity sUf1 tv) c nts Em he 2iucaccw i milc8 and che distribution of condoms to them illVC he ~n or n~d iD r GJvefl1nenC s(~ctor The Family Planning Association has a130E~k11 the irti U3 1V~ to reis ter males ln industrial employment Tllese are steps in the ri)n dtrect1ongt but the size of the problem indicates the n~ ed OI a concerted effort en a much large r scale
306 Tre Program relies largely on the use of oral contraceptives as shown in the following table
Oral Other Advice Contraceptlves IUDs Methods Only Totals ( 100)
19)9 76 20 16207 ( 100)
1970 316 63 9997 ( 100)
1971 50n 4n 365 79 8724 (100)
Family Planning Association unpublished report
----
- 7 -
Althougr amJnp the neH acceptors in 1971 the users of oral pills were only 509 ~mon~ the old cases the figure was 119 The percentage of IUD users has remiined stagnant at an insignificant level this may be partly due to consume prefErence and pctrtly outng to lack of trained staff to undertake IlTD i1srti l7U There h hOHever a visible shi ft towards the uSe of othe~ ilettods (npchani81 and chemical) attributable to a scare about the side efects nf oral connaceptives Among these conventional methods the condom s 11 os popular
307 J t )resent fami ly planning services have been extended to 48 out of 106 hellth centersoffices run by the Government and the objective is to C)Vel t1e remaining health centersoffices within a short span of time so that adice and facilities for the practice of family planning are conshyvenient Ly wa nable to the people in all parts of the country By ann large sepanit e fITti ly planning eli nics are held on specified days as an addition to norrral lealth work Besides doctor sessions at the clinics supply sessions are rur by health visitors and nllrses assisted by clerks The nurses are authorjzed tc issue oral contraceptives for a period not exceeding three months ani the acceptor is required to attend a doctor session for advice during thi jnterval In 1971 the numbers of full-timepart-time staff in Gov~rtmnf centers renderinp family planning services were
Full-time Part-time
1elical Officers 14 8
NUseMidwives 35 19
Cl~rks 3 17
Now tile low~rnment -gtbjective is to integrate family planning services into MOl services and use the same staff being used for the delivery of both types of erlices at multi-purpose sessions However so far only 1A centers have interated family planntng with Men or gpoundmeral hpalth care sessions
3011 The Family Planning Association has eight unf-purpose centers where famil) pLmring services are available ftve days a week The Association employs tilrEe full-time and ttJO part-time doctors a complement of 14 nurSeS (who llave been trained to do pelvic examinations) and 11 other clinic staff membels The Association also has a number of voluntary workers in the clinics The CithoUt Marriage Advisory Council has three clinics but their contri shybution in terms of enrallment of acceptors is not signiflcant
3)9 A Post-PartumPost-ALortal Program was started in 1969 It is state I tlat about 14 percent of the patients reached attend a family planning clini~ 1iTj thin six weeks of the interview in the wards IhiR is qui te a low figur In 1970 when a system of home visits was tried under the Family Planning Aide Project in 7 clinics the rate of acceptance doubled in three clinils rose by 50 percent in two clinics and increased by 24 percent in one clini (No change was noticeable in the seventh clinic) No decision has been Inad~ tmiddot) continue extend or modify this Project
A Po~ulaton Council ~-----------
401 he fu~ura ro~ Lh~ ~~~01ati0n Council has to be considered in theli1 A the tasK t~ lL ahead of the ~ational Family Planning Program At pesent tile officil~r(QSrJ1Tl is prirnarily concentrating on two objectives (a) tIlE excpound1sinrt of fmd plannin~ services to tie remaining 58 health centen cLJs as rapi(ily as possible and (b) the integration of family planniT g VI tr MCH services Thus thG administration of family planning serviCHJ will be merged into and become part of the Community Health Services Since t is ()rganizationally undesirable to disturb unity of command a separa1e elteecutive agency for the administration of family planning services is preempted within the existing policy framework An executive role for thp Pcnulc tinn Council is there fore ruled out on this consideration
402 If the Population Council is to function as an advisory body at the p()Lic~ aId progra1l pLilnni-l level snd not to concern itself with the minutile If program execution there wonld be no advantage in giving it a statutory stltuS But if it were the policy of the Government to set up a verticll )middotro~ram for family planning ii th a field organization separate and distir~tOroll the HeaHh administration it would be quite appropriate to establish an autonOiTiOUS statut()y a~fgtny ntside the departmental setup of the MinisiY of Health d~b a budi~t md staff of its own commensurate vith the rE spo lsi hi Ii ty to be rEs j Freed from the usual departmental conshystrailts ~n the matters Cif sp(ndlng a1d hiring and firing of personnel such an aglncy c(uld move faster than a heavy-footed departmental formation wi thin a Mins trl bull Hovever a hody of this eharacter would need to be cas t in a cliffe ent m(ld than the present Population Council The shape that it would take lrould be more like a Board of Management with a full-time Chairman or Execuive Director and with more functional expertise than representational charater But an advisory council with an autonomous status and no responsishybilit f( r lrogrrun eXIGulion iould be a source of friction
403 r~e existence of the Population Council as an organ of policy advici has certain advantages Firstly it is a forum for developing a national poLicy in which officials and non-officials participate Secondly it pr )vi bulles a focus to ti1e official program vhich it otherwise may tend to lose as ~ontraceptive services are merged into the general health services Thirc lymiddot- and this is important -- the Ministry has extra-departmental advice availabL to it~ but the Ministers constitutional responsibility for the condl ct )f the national progl~lt~ le1lains unimpaired
404 ls an advisory Q(dy the Population Council should be more broanshybase( than it is at present For instance it should include representatives of tile organizations of employers and vorkers associations of the medical nursngmct teaching professions and organizations for womens welfare The Counil should also haye a social scientis t on it On the official side the
- 9 -
Permane It Secetary and the P1O (fen and FP) should be brought into the Council he inclusion of the Permenent Secretary would open a channel of communi~aton with the MOR ae the highest policy level next to the Minister and would (ontribute administrative expertise to the deliberations of the Cou1ci1 ~m f icili tali 5 (pleuenrti)D of th~ recommendations of the Council within the -rni and in OUltL depa-cments The inclusions of the PMO (MCH and FP) wOlld el) emphasi ~2 hs responsibi lity toward the family planninR program Some officrs of the HOH (eg Chief Health Educator Principal Nursin~ Office e) may 111 ea~e to be members though they may attend as requirE d nmiddot the agenda before the Council A representative of the Ministry of Fin nee stQuId be inc~uded in the Population Council This would make for a lettr appreciation of the needs of the Program in that Ministry and fadIi ate fj nancial sanct ions
B A~tatutory Council
40S In the foregotng Pgraphs the view has been expressed that within th edsting policy framework an advisory Population Council would be more tli)prcpriate than a COlincil wi th executive functions and powers that an advisory rOUlcil would not gain by having a statutory status and that if a statl1tory body 5s to be set up in lieu of the existing Council it would need tC b structured more Iiice a Board of Management than a council wi th a repre13entttional charact~( n the latter event the statutory council should have fu 1- time Executive Chairman or failing that an Executive Director functj oni1g undel- a Chairman trno can devote considerable time to the business of tlw COlncil
406 T1e Statutory Council should have its own budget with full operashytiona pOlo1ers It should have the authority to appoint its own staff and regulLte their conditions of service If it is constitutionally possible the Couner1 shollld be outside the jurisdiction of the Public Service Commission in pesornel matters
407 As an instrument of Government the Council should be subject to such ~eUfral or specific directives that the Ministry of Health may issue to it frcffi ime to time This should be written into the statute under which the Cmntil is set UD
408 The composition of the Council ould depend on the functions assig1ed to it It is suggested that the Council should not concern itself wl th the delivery of cliric selVices in the field The Ministry of Health may (ont nue to administer rampmily planning services at Government hospitals health cmters and health offices and the voluntary agencies should run thei] OWl ~rogram The following functions may be handled by the Council
- to shy
s rrogram plannin and target-setting
b proram monitoring and evalllation
c wiL of d 1ci(JTIdnCf by inspections
d Qrg8lizatim 0 es and marketing of contraceptive J~1J-s BLl (iV es at subs idi zed rates through es tablished 1 2 d(~ channel
e information mass media communication and audiovisual ublicity in the field
f prorrotion of famil~r plannIng acceptance through face-to-face cotlmunication by poundi eld workers in domiciliary visi ts
g trIining of personnel
II pr )motion of -esearch enJ
i financial support to voluntary agencies providing family planning services
409 n Statutory CCii1cil may corsi5t or an eminent non-official vith a comri tm ~~1t towacds foJlily plailninf nd the fol1owin~ members
I ~ bull Pfrmanent Secretary ltl-tIlH
Chief Hedical Officer HOH
i Principal ~ecHcal Office ~mH
d Pilhlic RellltionB OfJte(middotmiddot Prtm~ Ministere Office
A represen ta ti V~1 of the Ministry of Education
f ~ representative of the Ministry of Finance
g A representa~ive of the FPA
h A representative ot the C1AC
i H social scientist fcum tle University of the ~Jest Indies
j Three non-officials with experience in management and administration and the
k Director of the Family Planning Program - Secretary
- 11 shy
The COUlcil ITIltW constitute cOlClmittees for Finance - Accounts Personnel and Sup lies nd Stores ir~whi ch )nly members may be included Other commitles sc1h as those 01 training info1nation and education and researCl ara ~valuation r1ili also include experts from outside
410 he Off1ce raquo) cc im Panning Program which at present forms part of th ~Hnis try or [i n should be placed under the Council and its staff strelgtl ilcn~ii2 i~ r181 it may cease to depend upon the services of the Mir is t y of H~alth
C Office of the Family Planning Program
4 11ollwther the Offic~ of the Family Planning Program remains a part of the Mirisry of Health or is transferred under a statutory council if one is set uP i needs to be strengthened to meet the requirements of an expAndshying pr )gn m At present the following sys terns need to be ins ti tuted in this Office
a a 3ystem of setting annual targets for the enrollment of acceptors and the projection of service fadli ties in relation to these targets
I Ci ~ystem oE V)glC loHitoring (the monthly statistics flowing from the clini~s c~iiiain unproc(~s5erl for months)
a system of program evaluation eg demographic effect of tte program cost studies
1 an overall design for media communication based on a study of the reach a~d cost effectiveness of different media and the effect of the meflBsge content and
e a m88t~r plan for training which would comprise an assessment of the training needK of the existing staff and future reshycruits and a long-term plan divided into annual programs
412 Th2 Prograll afiie s~lould have the services of a demographer and a meeia expert A training adviser is expected to be provided by the PARO
413 1be Program Office should evolve schedules of field tours to overliee field operatio1s E~1eh health cente heal th office should be visi ted peridicaLy by the Milt~dical fElce- the Nursing Officer and the Health EduCltoI who should guide and assis t the local staff in carrying out the progam Their tour notes should go into separate dossiers for each institushytion and ~ach dossier should have basic demographic data about the area coveled by each institution These dossiers would be a useful record for revilwing l)errOmance The staff of the Program Office should be augmented to Ol)erte this control procedure
- 12 shy
D Decentralization of Powers
414 ~hete is a concentration of administrative and financial powers in the 11in s try of Health I-JllJCi1 results in an accumulation of references in the Miristl) and delays n field operations Specific powers should be delegated ~o (a) the PliO concerned with MCH and family planningmiddot (b) the Directcr o the Program Office (c) the Regional Director and (d) the County Medica1 Oficecs The Ministry should invite suggestions from these officers and wOlk 01t a schedule of delegated powers
415 A tdgh priority in the matter of delegation of powers is to arm the Regiond Directors with sufficient administrative and financial authority to implement with expedition the health and family planning programs of the Ministmiddoty 1 thin the areas in their jurisdictions
E Integration of Family Planning wi th Haternal and Child Health Services
416 At present family planning services are being provided at 48 Goverrnent hospitals health centers and health offices by using the full shytime E taf cf these institutions and employing part-time (sessional) doctors nurse~ anI clerks where necessary At 29 of these institutions separate famil cl~nics are held on specified days in the weck some being doctor sessi(ms mel others supply sessions run hy nurses and clerks At the remaining 18 imtit1tions family planning services are combined with antenatal child healtL cr postnatal services The Family Planning Association runs 8 unishypurpoe f am ly planning centers which provide daily services and contribute a 11 t le less than half the total number of new acceptors per year
417 N assessment has b~en marie of the effect of integrated MOl and famil~ p~ nnning services an the recrl1i tment of acceptors nor were ~ data readily avallable for this purpose It may be observed however that in a situation of shortages of trained personnel for health services utilization of the existing health staff and facilitieR for family planning is inevitable parU cllLrl y in the interior where such shortages are more pronounced This underlines the need of evaluation of the integrated xai and family planning progtam for its impact on the number of acceptors Also a study needs to be made of che utilization of medical and pilramedical manpower so that it leads to bdter ~llocation of duties and optimUJl utilization of personnel
418 ile integration of faMily planning into Mcn services has certain advalltages as well as attendant risks The advantages are
a Lbe association of family planning with the care of mothers and children helps project a benevolent image of family planning as a program of family welfare This creates a
- 13 shy
1imate favorab~e to the acceptance of family planning aa lt p-)si tL1e il-Eare rreasure rather than a negative program cE limiting c~ildren
h t elps erlist ~r2tion tf doctars and nurses who as c -~ass enjo tft~ Y)er)et~ a~d confidf~nce of the communities i712~ Eerve
c ~ieD of contact with women
d luni-purposa clhlics for ~lCH and family planning services are onenient for motn~rs who would have to travel considerable (listances to the clinics
e hete is better utilizat1on of Acarce heAlth manpower
419 he limitatio$ of integrating family planning with MCH servicesI
are the posiOili ties of loss of focus on family planning as a high priori ty prograrr ald the diffusion of pol1sibility for its implementation These could tlow ve r he safegurded agaifls t by adopting the following measures
a 11e job descriptions of doctors and nurses should be rewritten 0 include the family planning function
b hE perf0rt1iai1ce of ctoltors and nurses should be judged as much )y tbeir inteceq t in planning ~vork as in maternal and ~hjld care and this should he lade known to them
c )octors and nurses involved in ~CH services should be given middot)rj entation and traIning in famj ly planning and their interest 3UEtained by refresher courses seminars meetings and supplies of literature
d Thl techrical (xpert~ in the Office of the Family Planninl Program should maintain liaison with and guide the field agencies in implementing the family plannin~ program For this purpose schedules shoul d be marle out for periodic field inspections
420 It is suggested that the working of half-a-dozen centers where family plbnnLng services have been integrated wi th MCH sessions should be studiei for ehe purpose of standardizing the methodology of delivery of servicl~ Such a study should include staff strength patient load recoril shykeepills 10middot of patents in the clinic timing and frequency of clinic sesaios ani convenience vf patients
F Voluntary Organizations
421 I i~ internrticri31 expedence that the birth control movement is pion aTC tt volunh[~ JilC S Qltl that hen the national governments step in wi tl cmbi ti 019 prjhns wi thin the sLate welfare system voluntary bodies ieh tteir limited ilsrluces restrict their service activities and shift the emplasi i 0 educedgt (f the community training research and contracepshytive Sf vic not 1l7gtilflblr in he official program or in areas not reached by it In nagni tude and expanse the of ficial program in Trinidad and Tobago has alrad~ orertak~n Ce 101umary program Increasingly it will become the domLnart tartner in the total national program while the voluntary agencies will cOltirlU1~ to receive financial support and encouragement to set up high standaeis If service and explore new areas thus acting as a stimulus and an additi_e tl the official program
G FrOB-ram Infomation
422 Thre is no concurrent evaluation or monitoring of the Program The daa or lq72 flowing in from the clinics month by month have r8Jllsined unprocss~d tn the Program Office The official Annual Report - 1971 Sums up th~ poition as fcllo~s
ITThe Research and Evaluation component continued to be the weakest in the Population Program Although a systen of evaluation had been built into the program the follow-up procedures for analyzing the data and for correcting inshyconsistencies are inadequate Requests were made to extend the staff to establish a more viable unit but by the end of the year no chllnges had been made
423 T1e recording and riporting jJrocedures were revised effective Januery 1972 and there has been a further change recently at the instance of t1e Evaluation Adviser Under the system now established the clinics are lequ Lreurod to maintain the following records
a Family Planning Clinic Case Card - New Cases This was introduced on January 1 1972 and has thirty-one entries giving age parity contraceptive listory pregnancies socio-economic background ource of family planning information and agency for notvat ion bull (Annex 2) The case card is made out in duplicate for each new acceptor and a copy sent to the Program Office
b Daily Regis ter This fs a ne~gt1 form recently introduced in replacement of the old regis ter and is preparen
- 15 shy
ie) ruplicate the original to be transmitted to the Program (fHce and the carbon copy to be retained in the clinic Th~ is a very 121zborute form requiring 36 entries to be aa~ for each Chse nel and old attending a session includin~ (ntries to cit L to contTaceptive supplies issued
AijCleX 3 T~13e fcnnG are required to be sent to the Program lffce in i7JO balches every month the first batch for the i IS fif~eeL days and the second for the remaining part of hE month The trtention is that the data appearing in the ~EZlic daily legis ter forms should be compiled in the Program Office and fed back to the clinics Although it is claimed that this new form has been pretested and is workable ex)erience alone will show whether the majority of clinic cL~rks are able to cope with it in a busy session
bull o now-Ho Card TIlis card is intended to keep track of ac ceptor--It has entries for name addresfI and month fcr which a visit is due for each year
bull Aphabe tical Index This is a card index of clients with aidresses
Each i)at en is given a simple clinic card on which the dates of further appo~utnli rc3 an~ indicated A special fonT[ has been devised for the reporting ot cases unler the Post-IartumPost-Abortal Education and Referral Program
424 J system of monitoring progrRm performance from month to month need to bE develQped as a high priori ty The problem is not so much reshycord ng mc transmission of data by the clinics but its aggregation and proclssi ng in the Program Office every month which at present takes a long time The Statistical Officer should have a statistical assistant to help him Ln I he taflk Monthly progress reports should be available to the Mini H t~ n H(llllth and A11 offt eerlil of the ProKrnm Office so that remedial ac tl m I lAY h(~ tuk~n n rll1u- WhOnh1f ~Hfl(AlJtlaTY
42 For the analysis of data and evaluation the Program office shouln haVE th(~ full-time services of a trained demographer
H Field Workers
42) Tie Program nemiddotis tne services of a cadre of field workers to enr)ll neii aceeptoTs follow up acceptors in their homes and revive the int 2remiddott of dropouts Such a category of workers could also be utilizerl for pr1fficting other health programs such as the VD campaign and the inmuni~ation program
47 As an experimental measure one field ~]orker may be assigned to a emi l~ of Hi 000 population This would mean 100 field workers in all
- 16 shy
Earh of the workers should preferably have harl a higher secondary education otherwLe 1gt junior secondalY education They should be married persons with middoti1ltt mot tl-an two or tlree children recruited from the locali ty in which they armiddot~ requlred to function Only persons who have the capaci ty to comnunl at~ and or6anl~e should c chosen A months ini tial orientation
slcu1d enable them to start functioning in the field though reshyfresher CO rSeS tvould be necesslt1ry in due course In Port-of-Spain married mer~ a1C women may be employed on a part-time basis
I Hanagement Study
428 A nanagement study of the Family Planning Program should include a sctu iny of the top m~nagement Atructure (Population Council - Office of the Fanil) PLanning Program - Principal Medical Officer for MCH and Family Planni Ig fetices) the field structure for the delivery of family planning servics (Re0ional Director - District Health Services) including the utilizlti(n if medical and paramedical personnel for adding the function of del ve y )f family planning services and the control and communication proCed1reF Lfnking the top management with the field structure
429 The management consultants may study the functioning of the Popul tio I Council and advise whether it adequately serves the purpose of givini po Licy direction to the Program and if not what changes in its compo itt m and operating procedures may be introduced without altering its bsic craracter as an advisory agency The consultants may suggest an alern at ve form of organizati)n and utilization of personnel which in thir p nion may be better adapted to the needs of the Program
430 Irrespective of whether the Population Council is maintained or it is replaced by an agency of a different character a formation like the Offic of be Family Planning Program would be necessary for the administrashytion i)f 1 he program a task for which i 1 appears inadequately equipped at preselt Its obvious requirements are in the areas of program monitoring and el7alnation program supervision communication and training The manag ememiddotlt consultants may study the structure and procedures of this form~ tio Gnd make suggestions with regard to the augmentation of professional and ~ upp)rt lng staffgt and modification of operating procedures
431 The linkage of the Office of the Family Planning Program with the Miniutry of Health (Central Office) and the District Health Services should be sudied In view of the policy of the Government to integrate MCH and faI11iLy rlallning services it should be examined whether the Principal Medi al Officer for Communi ty Heal th Services (MCH and Family Planning) should be agtpoj nt~d as the Chief of the Office of the Family Planning Program and an adTlilistrative officer of a suitable level inducted in that Office to assist him TIle implication of this suggestion is that the head of the Family PlanJling Program would control the District Health Services
- 17 shy
432 rf 1e management consultants should examine the delegation of adminshyistratiie Bld financial powers of the Ministry of Health to different levels of Progam aclrlirdstration viz bull PMO Program Office Regional Director and County ~djca~ Officers
l33 he system of 01 af Togram information from the clinlcs to the Pr()~ra1 O~fice and tOile processing and use of information in the latter office iholld )e studied
434 he working procedures at the integrated McP and family planning clinics shnuLl be studied This would involve a study of each stage which a clien tpcticmt has to go through from the point of entry to the point of exit after receiving advice service or supplies This study shoulci lead to star dartization of procedures and functions and evolution of -lork norms CognatE st tdies of the working procedures at uni-purpose family planning clinics and su~ply SEssions should also be undertaken An essential component of these ~ tad ~es would be to examine Nhich functions currently performed by docshytors lealh visitors nurses and midives respectively hav~ become so roushytinize ttl it they can he relegated (0 the next 10Her level
435 Reated to working procedures is the problem of job description of medcal 8nd parrunedical personnel involved in family planning from the centra i tc the field level This job description needs to be studied wi th a vie VIW8Id txaminiDg the uttlization of skills and allocation of time by the staff lcc(rd~ng to the functional prj ori ties
436 frV management consultants should study the workings of the curren slralgements fOJ family planning counselling under the Post-Partul11 Post-Abortal Education and Referral Program at the Port-of-Spain and San Fenaldo General Hospitals
437 SU1ect to the ItBrcement of the Gove1nment the management conshy8ultal ts ~hOLlld undertake a study of th requirement of field workers (home vinitcru) in tmtlUI of are nnd population cov(ra~e
ANNEX 1
Names of Persons Met
Ii Mr T C Taitt Pem1(H~nt 3~crtarY) Ministry of Health
2 Dr M n Henry Chitd Medical Officer Ministry of Health
Ellubeth Quam a Prindpal Medical Officer (1S)
4 Mr G Z Jaine ~ uJiector Population Council
5 Dr Norma Andrews Medical Officer Population Council
6 Mr Jc~n Coury~ Evaluation Adviser Population Council
7 Mr A Jriseph Principal Statistical Officer Population Council
8 Dr C 0 Colman Country Representative Pan American Health )rg ni~ation
9 Mr ranca Kippel Health Education Specialist Ministry of Iea th
10 (1 bullbullines Principal Nursing Officer Ministry of Health
11 Dr Mx won (formerlyHinistry of Health)
12 M3 late Carops Ex-Chairman of Population Council
--
4i 1_ middotIIlt F-ntCWclOotf_Y v OJ t tl
GOVIIlHMEIgt(I OF TINIOAD AND TOampAGQ - NNISTJY OF HIALftf AIJIE1 2NATIONAL FAMilY PLANNING PROGRAMME
F MIL Y PLANNING CUNIC CASE CARD - NEW CASES - NFPPl
li ~~___ 1 ________
~ ecll-U
-- --------------------- shy~) ~~middot~------------------~~~~~~---CIJ------ middot~ii--middot-middot----middot-middot---middot--------- shy
ltv Writt N_ 01(111________________
a ~4itiJtmiddotl_____ ilIIIltIoI~____~____~-__----- shybull ~4
fie l$ - JO tDql IIfIA- tr-JMimiddot _ iJ 1 Odoor o
14aorielaquol_ _~ 0 lio witIleo-La ~ 01 bull - OJ ( _01 1~ltgt1lh o bull- 0$
AacJcu 0 2 CIIriIWA 0 J Os 0
Yv~MONTH ltnollOf~nfIGHTI
Undu 1100U$ Utgtdn 5SCI Undu 11200 01 ~ 50 - 9949 amp100 - 1199 02UlOO - nn9E~ (
0)~ 10- $99 SiOO -- U9~ lOO -- U99 12400 - 1359)-------_-r----shy ~l)o SIS n600 - Hm1300 -- 019 OJ200 il~9 ~------ 99~ a 1)0 m Os1)00 -- l99 1400 -shy $4100 -- 1S999r--- shy
1500 donl S6000aad O399 - lt499I~- I 0lt
ltII
IJ -IC _~tltlioltgti lS
02 IaampJIIocI OJ 04 laM Os
w Oltwio I_-l(~u IrIaa U
h~~ ~Clubl 01 OJ
IS ~C-n 01 toSIitDI 02
Ji poundI on 01 IriIIIuy M ur 02 IV OJ
WU 10 pltIoII~ llaMtl 411 cIIiId 01 Ol it fIolto ~ do~ _14 rou IIlgtJo 1Ia1 ___~_ shy
40
It _ I 00 ~bull FPIiIJ 1
OJ 02 OJ 06
)0 III- iy wOWcf ~1
aMIIl Os
11 T 1gtlt ( h _______ 4)~
06
04 (MIbullbull middot bIrlI ~___~__~_ (-fIJI ~- -~-- (1HJ 49middot SJ
U 10k 01( 1__ raquo$-4
iU1) DOl F ToWotfOlnC DOl 001 or Do [IP 006 001 OIIgtu___Spltclty DOll Nltmo 010
U1Mo I orcpmiddot laquo55middot16
1lD 001 Foam Toblelf_ICim DOl Condom DOl CoomS~ 004 oe Oos WlttuJn 1J OIkr DSpody) 101~ ~Iu 006 Rhylhm 001 DOG OJO
no wI~lmm 4 cd
(I 0) 1110 01 Condor 03 (lorn bull l S~muoidIl 04 Faa TabioolfIIltr- Os RhyUlm 01 lnJrl tible O Advico 090 06
la slt 1)0 19 loti ~rltnlt) ([)sl or 1llOn) ____ --__ bullbully-J n SV - ~JcdS
v~ Cl NCI 0 30 OJI_O I Wr blJ1h 0 I ~ OJ 1 ~ (fOOd V 01 No 02 laquo 6) Cf4
WIiI 1 172
004 001
j D middotmiddot middot
1 ~
r
~
bull I
bullI I I
r c i
ANNEX 3 Pagemiddot 1 of 5
0 raquo rshy -lt l)J ~ 111 t G) 5 shy (J) ~ -
fT1u
i
MINISTTY OF Ho1TH
NTIONl F~ILY LNNING PR-GRbullbullM-tE
~~5tructions to C11nic ClerKa
How to co~ploto the Daily Rogister
~~ ~~v1sd Daily Rosi8ter replnc~D tho one which is now in use tb$ Monthly PC~ri rOt~ arti tho 01( Ci() Dod PollJ j f m It is a pre-coded form and 1411 cl~1p Jd tl a1I6iniul-mIHvn Oel Clinic nctivi~y
110 )rm rollt biJ coupJot)d lrl cupLtcoto using a o(roon shoot Tho top aheot or oriinai ~ust bl) 6(Ult to tho CQgt1tral O[[lCO and tho carbon copy retained in the Gliaic rilo dll the for6a that ar uD~d betwoen the 1st 4nd the 15th of the oIIollth aut bo subClittud tocho office 35 Lnc blttch Those oomp1cted betwoon tho 16th _lid tqemc of tho month must bo ~cnt in a secJnll batch
P lOvLior hns boon Illllde for 25 clients on cZlch forlll new forlll must b IIlied f r poundh 50[810n2 whothur or not ono or lIIore session are hoIdiit the clinic on he sarne day
I th ro alO more htl 25 clionta 1n attondnnco at tho session the additi shyOhAl m~bOl of clionts 10 clients nu~ber 26 27 etc sh0u1l be ontered on the next Imiddotrlll ~i ttout a1tpoundring the numbtlrs in the cvlumn hond Series
51 ppOfil th~ number of aUcnts lQr that session ws 5 this would mean thllt two rJlS ~ lst be 6ubllIitt~dl the first filled uF 1 tltgt 25 And the laquoIncond 1 to 10 Th~ cal bon ofies should bo st~plod togother at thu t0P l~rt h4nd corner of the torm ard ktpt in the Clinic filo lou IIlU6t stapl~ the originftls in the 8~~ monnshyer for lIub~ssion to the ofticl
ie h~ ll idontiflctior- (cc 1 - )
0 lot Ji 9 anythin~ hGro poundhia is int(mdClc for tha computer code
2 ~~pound~ - Print clOflrly tho name of your Clinic
C1Lic Huml or - (cc 4 - 8) Evar1 Clinic Numbor has 5 digits Virite each dig t il a t$purate box
It Pai~_thllsectgdllion (00 lt) -1 1) - Dl monll 10M
lw) bolte IlrO proY140d fetr olAoh pr 01 thQ dISh Enter tho dA) ldns a R
d16ih
emiddot5middot (0 11 I for 115t ( 0 21 for 5th etc Treat month the am pay
e ~ 10 ~ I for I-hrch 0 [2] for September Tho y~nr must be (into ad
I Z I ~ I I 71 q etc
Take as in IixulIple tho dOlte 3rd tllrch 1973 7~ie must bo written
[0131 LSLDI[7l3JDny Month Ye~r
5middot 1~J $~~ - Irom ~-------- To --------shytntol hOI II the time the Clinic 111118 in SW5sion emiddot8middot
(i) 11011 500 lm To 1200 non
(11) Frclt 100 pm To 400 pm
(iii ) IX-OG OO pllI To 6~00 pm
f
2
ADEJ ) Paae ) of S
6 Eov
_ 1hA 1gtIpoundC iIIUlt be nu~o7Ifd tler1ally 1 throurh n lU tbey Are Wled In ~1l8ellJ IInel 1301 tlU 1 Orcl 1 Wled tor a o5038ioll - -I 2 tonY tho _boul~ b I1WJbtl 1 and 2
hlrlll are 25 linos OIl the fOnl Ilnd thoae muet be UBtleS for 25 clients 9 one ior bullbull 01 I ini
ot ~h lc II ol1cM lOlivpound til e linic before soeinc DurOI or doc tor ilnc ii hox rristrltltion nUlJbet had alrearll been recorded on the Dai 1y Roiuter then n line ~hollld be drawn through that entry an1 the eliort nust not 06 includttd in tho totals tor that 0eDion
1lw Ileifitration Num)~r of cueh client must be IiIritten IS n 5-dlrlt oode ClhnC IH11IlElr 315 1IIU8 tborotore be enterod 18J010117]5]
~ Clt ZOt
Coda 1 Codo
10 ~tl c 2t j co 21)
~w elSe - Coda 1 0) d CltaEl - Code 2 Revislt Code 3
Only pound1 01 theBe coiles may be usod
11 prol-O~ ~Eil~1 (cc 22)
If ma climt was L drop-out IIho haoS returned now to the Clinio tor tho first no linmiddot bullwin lt1ro1eo o t he or she should be given CCe 1 It this do 5 II It nprlly leu this colWlln blank
u Hothod middothisllill loe 23)
NOh til t otly ~ Cod 16 tp he ontered in 2lpound of the columna oven thOUGh 10 co11lllJlB 10 provided on the torm The Codes llrol-
Oral Contraceptive Code 0 1 U D Code 1 Condom plUD Codo Z Condor (only) Code 3 Foum tAblets cream Code it DitphrClGJII Code 5 Rhythm Cde 6 Injectible Code 7 Advice Code 8 Other Code 9
It for middotDo-le 1 client rlllll ji yen cclldorls ord foam or creall Iou Qust entor Coole i (condom plulJ) in the appropri~te column This Quat be the only lIotmiddot) tarcie If an in the cnse of a tlnle clinic I the client is Bup)lieu lith COIlOrW only you rmot entEr CorlQ 3 (cpndolll) Do not use a ticII ~ tho (odo Nwber
It is CUi tomary fur 11 cliont 110 is beine put on the oral contraceptive for the first tiT1o and even on other occasionn be issued condoms and 11 crelle or foam a Ilell rI3 a pgtcket of pilla In such Cllses when the piDQ Ilre Ilctually iouou you tlust record Orll (Co~e 0) 08 tho onll metbod ilo othor ntry sll0uld ho nnrlo
Uovever n SJC~ canas vucru condoms and fOHa ~rc eiven but no pilJa (even thoJRh _t _n the intention to issue pills nt the noxt vioit) than the Mothol Th5 ifli t ohoulcl be recorded uo Condor Plus (Code 2)
13 Seen Bybullbullbullbullbull
~rot S-1 SO l
Doctor (Dr) - Code 1 j Nurse (Nul ) - Code 2
Clark (Olk-) - Code If tho Clhnt is vcen hy both tho llootor tlnd the Nurse enter Code 1 t Doctor It 6~61l by the Nurso only arite Code 2 Cod bullbull Cerk is l)llnt for FA Cllnica Clerks in tho Government Cli1t hiwo Llttoll istructed not to i56uo supplios on their own volition
14 fl221~
lhio S~tiCl of -Ie fvrtl t~ke 16 (llrci coluMna (cc 25-+0) nnd 10 tho only part at th iOIQ in llich iore thAn one cod is Zlccoptl1blo Tho purpoco of the )ecton is to 0 able to arrive nt the Cjunntity of 6tock dilltlitJutshyed YOI IIlUdt writo in the CllllOjH-iata colulna the nUllbJr of Il1ch 4rtic1o i~JSu~d ~lo e ha I Oral Contrcilpti vea are aub-di vi dod into types ae_ 3 PIllCKC 9 0 Elynnn LlUot be entered Codo in card column 25
If tor eXllrplc t l cliunt is iosued wi th packots of Zucynon nnd aJ(1 ~ivn 1 conuotll (8inoloo) you ouot enter in oard column 25 and 11 It
cnrd col~8 )2 and J (io 1 in card colucn 2 nnd 2 1n card coluun 33) Nota C)lldoIlU ale to b(t ruoordod individually not os packots of throo) Should n ne LlondoClo be isoued thil3 is to be rc-Qed as 09
If It clint 6 t~ot isoued Blly lIupplies thon you must writo Codo 1 in CQllAlilD 41
It Q eli nt isite the clinic to check on her LUD or her Diaphra~t IUId ro DI W 6 ppl ills nre ispounducd then Code 1 1s wri t ten in column 40
In the FA clinios here a variety ot orll contraceptiveo in orer~l tho elerll wilmiddot~ bJ provided with a specill code shoot The idontifyin coo will b wiittn in Column 29 nnd the nUlber of packets iosued in colwm )0
lralaer-In Code 1 lrllllsie r~ut Coda 2 leIllPQrArr Trnnsfer-In Codo gt
In the cao of n 2ratl8fcr-In I you lUot n160 cOrlpleto coluons 42-51
In the cllU J of A ~~emporary TranGfor-1n (an individual who i8 only v1citing fur clinic tor some epecial trcatcont hna who will bo rdnlnin
~middot(II~~~fO~l~SIl~I3~nn~~~h~rO~nh~1~~190~~nll 2-46 and ler rei IItrntion numbu in colullnll41-51
It the oli( nt i iNt a CrllnoforwIu - Out or loClporu1 tMn loave oolumn 1 blank
16 lr4nst(gtr-tl2~~morrry TilJnder-In (co 42-51) Forl1ltl CUn E1~ (cc 112-46)
hen you rei iatlr L irllsfcrln or Il TJlporary Trnnsfer-In you IIIUBt write I ere the five-digit clinio nucbor of the Clinic iraQ which tho ltlient Me (uIlO
2mer ]letr ~2n ~ (cc 47-51)
frlta fllao Clo r-~itrlltion Nuc~Er ot the client in the Former Clinic (i c bullbull th 1 Sis rnmiddotion ~UlIlh()r which the client carrics 1n the tormor clinio) bull
It tho Forrltl Ho( ist rntion Number iIJ not readily wnilnble you tluct oocpluto thtl epcciol [orlll Transfer-In Not Identifiod Dy Forrlcr RCGi(trn~ t10n Nwlbvr Or ~ flt)rCl is to be cOlplctcd for och cnso nnd th forlJO Ilubmi tted to thu )opllntion Prorrnnme Of fice tOGether with tho Dily Ro~iBtors lhwev~r should the clork leuTI of tho clint B FormlI Uocintra tion lUlllb r )0[(10 Cubmi ttinft the D1ily IOCI otro t hen the nUQbcr shoulo bo -ri ton in colucns 47-51 lna the special foro should lJo deotroyotl
l7 bullbullbullbullbull
r lt bull bull
ADXI ) Pap S ot S
11 UD LV~ (cc 525)
It tb( cliont io ~ivQn An IUD tor the firot tl~o then you should Sri to Codo 1 Inuort ill colurJI 52
It tho olimiddotsnt ia rvinGgtrtltld i th An I UD bullbull tben wse Coda 2 RelnDltlrt shyin (01Uil11 52
It the clLmt is ~tte~~dint chnic beruse her IUD CflClQ out by Haol (cxpll Iion i ~hcn fir te todo ~- UIlllrli1 53~
If c-ltr IU fj IIIS reov in -ne cllnic by tho doctor or nurso t~on vlritI Codec in column 5
II the eli nt otends eiLlie tld explin[l th(lt she rccovcd the IUD tlllleel nen write Coda H in Colwlm 53
It the IUD jr still within the uterus nd the WOIraquoI1 1 11rc6llJlnt thon lIrite 1gt40 4 in Column 53
lZ np h5t (ce 54) It 0 Pull 5mor ie t~ken durin thi visit tben Codo 1 ehould be ampDtere4 in ColWlln 54 Should he c110nt lltt rQ(uircd to rttturn to clin1c for a rogtol1t Pnl) t06t then CoLe 2 llhould bo middotwrittcn in column 54
It no Pllp Scou io taken tde visit Itove colUQn 54 blank
Iraferti1lli (CQ 55)
Ii the e liett io nl1 infortili tr eaoe use Cor1o Ill in colUQn 55
If tbia 1000 not tlpl lonve column 55 blonk
20 Totaltll
CO~1ploete the [)ldegO 1gty puti YI tne totals betweon the double lines nt tu b()ttctl Carrj colUlllnc 20 21 nd gt4 Must hlve tho Bnoe JllIIber and thiG Would coreslonc to the numocr ir attencbnco
Writ$ th to1ul nUlllior of Drop-Outs returned (c022)
Urito 41eo tb totnls fOJ each card column 0 to 9 under tho h(adinu Method thiB Vioit Show tho tote L fgtr OlCl type of contraceptive issued (cc 25-40)
1)0 Dot wrLte 1111 totll lUl(Ier Card Columns 15-19 29 41-51
21 COPmllh bull ~lt h~t~ Monthly ROilort
OQ thG DaLl oCator forlll thnt ccrrOspOldB to tho 1(8t 1$06610n lt 0
oth yo Olllt (vwlgtleto the items nt the botto of the [orampl This is tour ontll~1 n(olt nnd includcD tho totll lumber of sesions Ilntl tho total Iluolcr ( r crop-outs durinr the Qonth
An tiUlsilt n drir which n doctor liB in nttcndnncc is a doctor sOfll~1on and shoulc 00 re(liGtcnd in coltns 56-57 All other sessions 1116 conlliid~recl supply stllciona and thtlY 1110 rocordod in columns 58-59
the total Ilum)nl Jf drop-outo ld the drop-outs by method durinc the onth nre 10 bu oltorou in the inrlicllted boxes
72 Chad Your ~
Milke I ura th t all thE fijul4gtu rre c101r -tNever writo our nutlUQrS 50 InrjEl that they oxtend out of tho
ap~rotr1ato ~ox
Cheek to BoJa tht 1111 numuors 1110 in tho correct boxes -- CJslHloially when Writi1 the totlB
Mllxe Cirtc O thmiddott t1e infoT1I1ntion i6 clear on the corbon COllY before sep rmiddotinr the sheets
Jitn the Fomiddotl lien tly sien YOUl nr me 1t the bot tOil right hnnd corner btl forc subol ttinG it Keep tle CL rb n copy for your rocordn
i
-l ________~~---------~
I _1
Adminiatr-atlve SKVieu
P inba ~~~l1cal lrlnbin~~eltltcal -1 te~ra t~~rvicc (lnatittloaa)
--1- - shy -1------------_-L_ l-r-aJiil- shy _-L_tet1lal d
PlIinm1tJ8 atdUon DetalMid H8Il1tb ~ ________bull Care
-----~ Office of i
the FlIily _IPlill3 roarshy
1- - - -------RegiatUll urnr
ltIi 1 Drelttor Rcgicaat Director Souta Tabqo tacallortb ~ counu gt____ ~ (4 ouottet)
Off1ce of the Res10nal Diractoc L
r----- _L_ -- shy i I bull IREgional Ipitl I
District IIttaltb I bull Othn RelOl ond Hcpital CenteIntt itlt j In 1__ _shy-~- ---- -_j
J r Ii~lth
C~nlef
L
I Ihnlth lie I th Offlcu (1ft lc~
Coullty 1I0p1ta1
Henlth tentet
I

------------------------------------
- F shy
3JJ3 Ttl flient recrvitTrent has fallen off since 1969 in spite of a signif Icar t xpansinn ir the number of Government health facilities providing family paarin~ services FrCli1 7Hr to year Starting from scratch the number oE GovE(nment health irlstitl1tions delivering family planning services in isollL(Od ~ily pltJfAill~I ~J in c)lchiratinn ~7ith MCa services has lWW risEn t 4 lhis ie --tdt)p to t cii1ics organized by the Family Plannin Asce1ation bull U2 by tile Catholic Marriage Advisory Council which offers the ~h)lthm meti1middot1 nT
304 1i ciecli ne d~ d re11~m2nt of new acceptors coincidentally w-Lth th~ eXlsioH uf s-crLce facilities needs to be studied to identify the factors responsible for it eg the quality of services offered the strategy of commmic at~on and motivation and management and supervision One obvious gap is he abgtence of an agercy for promotion and extension of demand for family lal 111 If services -gt tLe field reliance being placed mainly on clinic counseUn H1d generaUzmiddotd mass media publicity The need for a field promoshytional agelcy is underscored by the dropout rate In 11 draft paper prepared by the Hed_cal Offic(1r for FIrnilv Planning it is stated that by the end of 1972 t ile Heuroe approxiclt ji rHJC cun~ent users of contraceptive methods and 33 per ert dropouts
305 rht~ program is cot merely clinic-centered but also female-oriented Recent Iy mellsages aimed at m11es and stressing joint male-female responsibishyIi ty l gtT j ecillc CImt-J 1 i~gtVt~ b~~in )7cn 1n0 the cOTul1mication activity sUf1 tv) c nts Em he 2iucaccw i milc8 and che distribution of condoms to them illVC he ~n or n~d iD r GJvefl1nenC s(~ctor The Family Planning Association has a130E~k11 the irti U3 1V~ to reis ter males ln industrial employment Tllese are steps in the ri)n dtrect1ongt but the size of the problem indicates the n~ ed OI a concerted effort en a much large r scale
306 Tre Program relies largely on the use of oral contraceptives as shown in the following table
Oral Other Advice Contraceptlves IUDs Methods Only Totals ( 100)
19)9 76 20 16207 ( 100)
1970 316 63 9997 ( 100)
1971 50n 4n 365 79 8724 (100)
Family Planning Association unpublished report
----
- 7 -
Althougr amJnp the neH acceptors in 1971 the users of oral pills were only 509 ~mon~ the old cases the figure was 119 The percentage of IUD users has remiined stagnant at an insignificant level this may be partly due to consume prefErence and pctrtly outng to lack of trained staff to undertake IlTD i1srti l7U There h hOHever a visible shi ft towards the uSe of othe~ ilettods (npchani81 and chemical) attributable to a scare about the side efects nf oral connaceptives Among these conventional methods the condom s 11 os popular
307 J t )resent fami ly planning services have been extended to 48 out of 106 hellth centersoffices run by the Government and the objective is to C)Vel t1e remaining health centersoffices within a short span of time so that adice and facilities for the practice of family planning are conshyvenient Ly wa nable to the people in all parts of the country By ann large sepanit e fITti ly planning eli nics are held on specified days as an addition to norrral lealth work Besides doctor sessions at the clinics supply sessions are rur by health visitors and nllrses assisted by clerks The nurses are authorjzed tc issue oral contraceptives for a period not exceeding three months ani the acceptor is required to attend a doctor session for advice during thi jnterval In 1971 the numbers of full-timepart-time staff in Gov~rtmnf centers renderinp family planning services were
Full-time Part-time
1elical Officers 14 8
NUseMidwives 35 19
Cl~rks 3 17
Now tile low~rnment -gtbjective is to integrate family planning services into MOl services and use the same staff being used for the delivery of both types of erlices at multi-purpose sessions However so far only 1A centers have interated family planntng with Men or gpoundmeral hpalth care sessions
3011 The Family Planning Association has eight unf-purpose centers where famil) pLmring services are available ftve days a week The Association employs tilrEe full-time and ttJO part-time doctors a complement of 14 nurSeS (who llave been trained to do pelvic examinations) and 11 other clinic staff membels The Association also has a number of voluntary workers in the clinics The CithoUt Marriage Advisory Council has three clinics but their contri shybution in terms of enrallment of acceptors is not signiflcant
3)9 A Post-PartumPost-ALortal Program was started in 1969 It is state I tlat about 14 percent of the patients reached attend a family planning clini~ 1iTj thin six weeks of the interview in the wards IhiR is qui te a low figur In 1970 when a system of home visits was tried under the Family Planning Aide Project in 7 clinics the rate of acceptance doubled in three clinils rose by 50 percent in two clinics and increased by 24 percent in one clini (No change was noticeable in the seventh clinic) No decision has been Inad~ tmiddot) continue extend or modify this Project
A Po~ulaton Council ~-----------
401 he fu~ura ro~ Lh~ ~~~01ati0n Council has to be considered in theli1 A the tasK t~ lL ahead of the ~ational Family Planning Program At pesent tile officil~r(QSrJ1Tl is prirnarily concentrating on two objectives (a) tIlE excpound1sinrt of fmd plannin~ services to tie remaining 58 health centen cLJs as rapi(ily as possible and (b) the integration of family planniT g VI tr MCH services Thus thG administration of family planning serviCHJ will be merged into and become part of the Community Health Services Since t is ()rganizationally undesirable to disturb unity of command a separa1e elteecutive agency for the administration of family planning services is preempted within the existing policy framework An executive role for thp Pcnulc tinn Council is there fore ruled out on this consideration
402 If the Population Council is to function as an advisory body at the p()Lic~ aId progra1l pLilnni-l level snd not to concern itself with the minutile If program execution there wonld be no advantage in giving it a statutory stltuS But if it were the policy of the Government to set up a verticll )middotro~ram for family planning ii th a field organization separate and distir~tOroll the HeaHh administration it would be quite appropriate to establish an autonOiTiOUS statut()y a~fgtny ntside the departmental setup of the MinisiY of Health d~b a budi~t md staff of its own commensurate vith the rE spo lsi hi Ii ty to be rEs j Freed from the usual departmental conshystrailts ~n the matters Cif sp(ndlng a1d hiring and firing of personnel such an aglncy c(uld move faster than a heavy-footed departmental formation wi thin a Mins trl bull Hovever a hody of this eharacter would need to be cas t in a cliffe ent m(ld than the present Population Council The shape that it would take lrould be more like a Board of Management with a full-time Chairman or Execuive Director and with more functional expertise than representational charater But an advisory council with an autonomous status and no responsishybilit f( r lrogrrun eXIGulion iould be a source of friction
403 r~e existence of the Population Council as an organ of policy advici has certain advantages Firstly it is a forum for developing a national poLicy in which officials and non-officials participate Secondly it pr )vi bulles a focus to ti1e official program vhich it otherwise may tend to lose as ~ontraceptive services are merged into the general health services Thirc lymiddot- and this is important -- the Ministry has extra-departmental advice availabL to it~ but the Ministers constitutional responsibility for the condl ct )f the national progl~lt~ le1lains unimpaired
404 ls an advisory Q(dy the Population Council should be more broanshybase( than it is at present For instance it should include representatives of tile organizations of employers and vorkers associations of the medical nursngmct teaching professions and organizations for womens welfare The Counil should also haye a social scientis t on it On the official side the
- 9 -
Permane It Secetary and the P1O (fen and FP) should be brought into the Council he inclusion of the Permenent Secretary would open a channel of communi~aton with the MOR ae the highest policy level next to the Minister and would (ontribute administrative expertise to the deliberations of the Cou1ci1 ~m f icili tali 5 (pleuenrti)D of th~ recommendations of the Council within the -rni and in OUltL depa-cments The inclusions of the PMO (MCH and FP) wOlld el) emphasi ~2 hs responsibi lity toward the family planninR program Some officrs of the HOH (eg Chief Health Educator Principal Nursin~ Office e) may 111 ea~e to be members though they may attend as requirE d nmiddot the agenda before the Council A representative of the Ministry of Fin nee stQuId be inc~uded in the Population Council This would make for a lettr appreciation of the needs of the Program in that Ministry and fadIi ate fj nancial sanct ions
B A~tatutory Council
40S In the foregotng Pgraphs the view has been expressed that within th edsting policy framework an advisory Population Council would be more tli)prcpriate than a COlincil wi th executive functions and powers that an advisory rOUlcil would not gain by having a statutory status and that if a statl1tory body 5s to be set up in lieu of the existing Council it would need tC b structured more Iiice a Board of Management than a council wi th a repre13entttional charact~( n the latter event the statutory council should have fu 1- time Executive Chairman or failing that an Executive Director functj oni1g undel- a Chairman trno can devote considerable time to the business of tlw COlncil
406 T1e Statutory Council should have its own budget with full operashytiona pOlo1ers It should have the authority to appoint its own staff and regulLte their conditions of service If it is constitutionally possible the Couner1 shollld be outside the jurisdiction of the Public Service Commission in pesornel matters
407 As an instrument of Government the Council should be subject to such ~eUfral or specific directives that the Ministry of Health may issue to it frcffi ime to time This should be written into the statute under which the Cmntil is set UD
408 The composition of the Council ould depend on the functions assig1ed to it It is suggested that the Council should not concern itself wl th the delivery of cliric selVices in the field The Ministry of Health may (ont nue to administer rampmily planning services at Government hospitals health cmters and health offices and the voluntary agencies should run thei] OWl ~rogram The following functions may be handled by the Council
- to shy
s rrogram plannin and target-setting
b proram monitoring and evalllation
c wiL of d 1ci(JTIdnCf by inspections
d Qrg8lizatim 0 es and marketing of contraceptive J~1J-s BLl (iV es at subs idi zed rates through es tablished 1 2 d(~ channel
e information mass media communication and audiovisual ublicity in the field
f prorrotion of famil~r plannIng acceptance through face-to-face cotlmunication by poundi eld workers in domiciliary visi ts
g trIining of personnel
II pr )motion of -esearch enJ
i financial support to voluntary agencies providing family planning services
409 n Statutory CCii1cil may corsi5t or an eminent non-official vith a comri tm ~~1t towacds foJlily plailninf nd the fol1owin~ members
I ~ bull Pfrmanent Secretary ltl-tIlH
Chief Hedical Officer HOH
i Principal ~ecHcal Office ~mH
d Pilhlic RellltionB OfJte(middotmiddot Prtm~ Ministere Office
A represen ta ti V~1 of the Ministry of Education
f ~ representative of the Ministry of Finance
g A representa~ive of the FPA
h A representative ot the C1AC
i H social scientist fcum tle University of the ~Jest Indies
j Three non-officials with experience in management and administration and the
k Director of the Family Planning Program - Secretary
- 11 shy
The COUlcil ITIltW constitute cOlClmittees for Finance - Accounts Personnel and Sup lies nd Stores ir~whi ch )nly members may be included Other commitles sc1h as those 01 training info1nation and education and researCl ara ~valuation r1ili also include experts from outside
410 he Off1ce raquo) cc im Panning Program which at present forms part of th ~Hnis try or [i n should be placed under the Council and its staff strelgtl ilcn~ii2 i~ r181 it may cease to depend upon the services of the Mir is t y of H~alth
C Office of the Family Planning Program
4 11ollwther the Offic~ of the Family Planning Program remains a part of the Mirisry of Health or is transferred under a statutory council if one is set uP i needs to be strengthened to meet the requirements of an expAndshying pr )gn m At present the following sys terns need to be ins ti tuted in this Office
a a 3ystem of setting annual targets for the enrollment of acceptors and the projection of service fadli ties in relation to these targets
I Ci ~ystem oE V)glC loHitoring (the monthly statistics flowing from the clini~s c~iiiain unproc(~s5erl for months)
a system of program evaluation eg demographic effect of tte program cost studies
1 an overall design for media communication based on a study of the reach a~d cost effectiveness of different media and the effect of the meflBsge content and
e a m88t~r plan for training which would comprise an assessment of the training needK of the existing staff and future reshycruits and a long-term plan divided into annual programs
412 Th2 Prograll afiie s~lould have the services of a demographer and a meeia expert A training adviser is expected to be provided by the PARO
413 1be Program Office should evolve schedules of field tours to overliee field operatio1s E~1eh health cente heal th office should be visi ted peridicaLy by the Milt~dical fElce- the Nursing Officer and the Health EduCltoI who should guide and assis t the local staff in carrying out the progam Their tour notes should go into separate dossiers for each institushytion and ~ach dossier should have basic demographic data about the area coveled by each institution These dossiers would be a useful record for revilwing l)errOmance The staff of the Program Office should be augmented to Ol)erte this control procedure
- 12 shy
D Decentralization of Powers
414 ~hete is a concentration of administrative and financial powers in the 11in s try of Health I-JllJCi1 results in an accumulation of references in the Miristl) and delays n field operations Specific powers should be delegated ~o (a) the PliO concerned with MCH and family planningmiddot (b) the Directcr o the Program Office (c) the Regional Director and (d) the County Medica1 Oficecs The Ministry should invite suggestions from these officers and wOlk 01t a schedule of delegated powers
415 A tdgh priority in the matter of delegation of powers is to arm the Regiond Directors with sufficient administrative and financial authority to implement with expedition the health and family planning programs of the Ministmiddoty 1 thin the areas in their jurisdictions
E Integration of Family Planning wi th Haternal and Child Health Services
416 At present family planning services are being provided at 48 Goverrnent hospitals health centers and health offices by using the full shytime E taf cf these institutions and employing part-time (sessional) doctors nurse~ anI clerks where necessary At 29 of these institutions separate famil cl~nics are held on specified days in the weck some being doctor sessi(ms mel others supply sessions run hy nurses and clerks At the remaining 18 imtit1tions family planning services are combined with antenatal child healtL cr postnatal services The Family Planning Association runs 8 unishypurpoe f am ly planning centers which provide daily services and contribute a 11 t le less than half the total number of new acceptors per year
417 N assessment has b~en marie of the effect of integrated MOl and famil~ p~ nnning services an the recrl1i tment of acceptors nor were ~ data readily avallable for this purpose It may be observed however that in a situation of shortages of trained personnel for health services utilization of the existing health staff and facilitieR for family planning is inevitable parU cllLrl y in the interior where such shortages are more pronounced This underlines the need of evaluation of the integrated xai and family planning progtam for its impact on the number of acceptors Also a study needs to be made of che utilization of medical and pilramedical manpower so that it leads to bdter ~llocation of duties and optimUJl utilization of personnel
418 ile integration of faMily planning into Mcn services has certain advalltages as well as attendant risks The advantages are
a Lbe association of family planning with the care of mothers and children helps project a benevolent image of family planning as a program of family welfare This creates a
- 13 shy
1imate favorab~e to the acceptance of family planning aa lt p-)si tL1e il-Eare rreasure rather than a negative program cE limiting c~ildren
h t elps erlist ~r2tion tf doctars and nurses who as c -~ass enjo tft~ Y)er)et~ a~d confidf~nce of the communities i712~ Eerve
c ~ieD of contact with women
d luni-purposa clhlics for ~lCH and family planning services are onenient for motn~rs who would have to travel considerable (listances to the clinics
e hete is better utilizat1on of Acarce heAlth manpower
419 he limitatio$ of integrating family planning with MCH servicesI
are the posiOili ties of loss of focus on family planning as a high priori ty prograrr ald the diffusion of pol1sibility for its implementation These could tlow ve r he safegurded agaifls t by adopting the following measures
a 11e job descriptions of doctors and nurses should be rewritten 0 include the family planning function
b hE perf0rt1iai1ce of ctoltors and nurses should be judged as much )y tbeir inteceq t in planning ~vork as in maternal and ~hjld care and this should he lade known to them
c )octors and nurses involved in ~CH services should be given middot)rj entation and traIning in famj ly planning and their interest 3UEtained by refresher courses seminars meetings and supplies of literature
d Thl techrical (xpert~ in the Office of the Family Planninl Program should maintain liaison with and guide the field agencies in implementing the family plannin~ program For this purpose schedules shoul d be marle out for periodic field inspections
420 It is suggested that the working of half-a-dozen centers where family plbnnLng services have been integrated wi th MCH sessions should be studiei for ehe purpose of standardizing the methodology of delivery of servicl~ Such a study should include staff strength patient load recoril shykeepills 10middot of patents in the clinic timing and frequency of clinic sesaios ani convenience vf patients
F Voluntary Organizations
421 I i~ internrticri31 expedence that the birth control movement is pion aTC tt volunh[~ JilC S Qltl that hen the national governments step in wi tl cmbi ti 019 prjhns wi thin the sLate welfare system voluntary bodies ieh tteir limited ilsrluces restrict their service activities and shift the emplasi i 0 educedgt (f the community training research and contracepshytive Sf vic not 1l7gtilflblr in he official program or in areas not reached by it In nagni tude and expanse the of ficial program in Trinidad and Tobago has alrad~ orertak~n Ce 101umary program Increasingly it will become the domLnart tartner in the total national program while the voluntary agencies will cOltirlU1~ to receive financial support and encouragement to set up high standaeis If service and explore new areas thus acting as a stimulus and an additi_e tl the official program
G FrOB-ram Infomation
422 Thre is no concurrent evaluation or monitoring of the Program The daa or lq72 flowing in from the clinics month by month have r8Jllsined unprocss~d tn the Program Office The official Annual Report - 1971 Sums up th~ poition as fcllo~s
ITThe Research and Evaluation component continued to be the weakest in the Population Program Although a systen of evaluation had been built into the program the follow-up procedures for analyzing the data and for correcting inshyconsistencies are inadequate Requests were made to extend the staff to establish a more viable unit but by the end of the year no chllnges had been made
423 T1e recording and riporting jJrocedures were revised effective Januery 1972 and there has been a further change recently at the instance of t1e Evaluation Adviser Under the system now established the clinics are lequ Lreurod to maintain the following records
a Family Planning Clinic Case Card - New Cases This was introduced on January 1 1972 and has thirty-one entries giving age parity contraceptive listory pregnancies socio-economic background ource of family planning information and agency for notvat ion bull (Annex 2) The case card is made out in duplicate for each new acceptor and a copy sent to the Program Office
b Daily Regis ter This fs a ne~gt1 form recently introduced in replacement of the old regis ter and is preparen
- 15 shy
ie) ruplicate the original to be transmitted to the Program (fHce and the carbon copy to be retained in the clinic Th~ is a very 121zborute form requiring 36 entries to be aa~ for each Chse nel and old attending a session includin~ (ntries to cit L to contTaceptive supplies issued
AijCleX 3 T~13e fcnnG are required to be sent to the Program lffce in i7JO balches every month the first batch for the i IS fif~eeL days and the second for the remaining part of hE month The trtention is that the data appearing in the ~EZlic daily legis ter forms should be compiled in the Program Office and fed back to the clinics Although it is claimed that this new form has been pretested and is workable ex)erience alone will show whether the majority of clinic cL~rks are able to cope with it in a busy session
bull o now-Ho Card TIlis card is intended to keep track of ac ceptor--It has entries for name addresfI and month fcr which a visit is due for each year
bull Aphabe tical Index This is a card index of clients with aidresses
Each i)at en is given a simple clinic card on which the dates of further appo~utnli rc3 an~ indicated A special fonT[ has been devised for the reporting ot cases unler the Post-IartumPost-Abortal Education and Referral Program
424 J system of monitoring progrRm performance from month to month need to bE develQped as a high priori ty The problem is not so much reshycord ng mc transmission of data by the clinics but its aggregation and proclssi ng in the Program Office every month which at present takes a long time The Statistical Officer should have a statistical assistant to help him Ln I he taflk Monthly progress reports should be available to the Mini H t~ n H(llllth and A11 offt eerlil of the ProKrnm Office so that remedial ac tl m I lAY h(~ tuk~n n rll1u- WhOnh1f ~Hfl(AlJtlaTY
42 For the analysis of data and evaluation the Program office shouln haVE th(~ full-time services of a trained demographer
H Field Workers
42) Tie Program nemiddotis tne services of a cadre of field workers to enr)ll neii aceeptoTs follow up acceptors in their homes and revive the int 2remiddott of dropouts Such a category of workers could also be utilizerl for pr1fficting other health programs such as the VD campaign and the inmuni~ation program
47 As an experimental measure one field ~]orker may be assigned to a emi l~ of Hi 000 population This would mean 100 field workers in all
- 16 shy
Earh of the workers should preferably have harl a higher secondary education otherwLe 1gt junior secondalY education They should be married persons with middoti1ltt mot tl-an two or tlree children recruited from the locali ty in which they armiddot~ requlred to function Only persons who have the capaci ty to comnunl at~ and or6anl~e should c chosen A months ini tial orientation
slcu1d enable them to start functioning in the field though reshyfresher CO rSeS tvould be necesslt1ry in due course In Port-of-Spain married mer~ a1C women may be employed on a part-time basis
I Hanagement Study
428 A nanagement study of the Family Planning Program should include a sctu iny of the top m~nagement Atructure (Population Council - Office of the Fanil) PLanning Program - Principal Medical Officer for MCH and Family Planni Ig fetices) the field structure for the delivery of family planning servics (Re0ional Director - District Health Services) including the utilizlti(n if medical and paramedical personnel for adding the function of del ve y )f family planning services and the control and communication proCed1reF Lfnking the top management with the field structure
429 The management consultants may study the functioning of the Popul tio I Council and advise whether it adequately serves the purpose of givini po Licy direction to the Program and if not what changes in its compo itt m and operating procedures may be introduced without altering its bsic craracter as an advisory agency The consultants may suggest an alern at ve form of organizati)n and utilization of personnel which in thir p nion may be better adapted to the needs of the Program
430 Irrespective of whether the Population Council is maintained or it is replaced by an agency of a different character a formation like the Offic of be Family Planning Program would be necessary for the administrashytion i)f 1 he program a task for which i 1 appears inadequately equipped at preselt Its obvious requirements are in the areas of program monitoring and el7alnation program supervision communication and training The manag ememiddotlt consultants may study the structure and procedures of this form~ tio Gnd make suggestions with regard to the augmentation of professional and ~ upp)rt lng staffgt and modification of operating procedures
431 The linkage of the Office of the Family Planning Program with the Miniutry of Health (Central Office) and the District Health Services should be sudied In view of the policy of the Government to integrate MCH and faI11iLy rlallning services it should be examined whether the Principal Medi al Officer for Communi ty Heal th Services (MCH and Family Planning) should be agtpoj nt~d as the Chief of the Office of the Family Planning Program and an adTlilistrative officer of a suitable level inducted in that Office to assist him TIle implication of this suggestion is that the head of the Family PlanJling Program would control the District Health Services
- 17 shy
432 rf 1e management consultants should examine the delegation of adminshyistratiie Bld financial powers of the Ministry of Health to different levels of Progam aclrlirdstration viz bull PMO Program Office Regional Director and County ~djca~ Officers
l33 he system of 01 af Togram information from the clinlcs to the Pr()~ra1 O~fice and tOile processing and use of information in the latter office iholld )e studied
434 he working procedures at the integrated McP and family planning clinics shnuLl be studied This would involve a study of each stage which a clien tpcticmt has to go through from the point of entry to the point of exit after receiving advice service or supplies This study shoulci lead to star dartization of procedures and functions and evolution of -lork norms CognatE st tdies of the working procedures at uni-purpose family planning clinics and su~ply SEssions should also be undertaken An essential component of these ~ tad ~es would be to examine Nhich functions currently performed by docshytors lealh visitors nurses and midives respectively hav~ become so roushytinize ttl it they can he relegated (0 the next 10Her level
435 Reated to working procedures is the problem of job description of medcal 8nd parrunedical personnel involved in family planning from the centra i tc the field level This job description needs to be studied wi th a vie VIW8Id txaminiDg the uttlization of skills and allocation of time by the staff lcc(rd~ng to the functional prj ori ties
436 frV management consultants should study the workings of the curren slralgements fOJ family planning counselling under the Post-Partul11 Post-Abortal Education and Referral Program at the Port-of-Spain and San Fenaldo General Hospitals
437 SU1ect to the ItBrcement of the Gove1nment the management conshy8ultal ts ~hOLlld undertake a study of th requirement of field workers (home vinitcru) in tmtlUI of are nnd population cov(ra~e
ANNEX 1
Names of Persons Met
Ii Mr T C Taitt Pem1(H~nt 3~crtarY) Ministry of Health
2 Dr M n Henry Chitd Medical Officer Ministry of Health
Ellubeth Quam a Prindpal Medical Officer (1S)
4 Mr G Z Jaine ~ uJiector Population Council
5 Dr Norma Andrews Medical Officer Population Council
6 Mr Jc~n Coury~ Evaluation Adviser Population Council
7 Mr A Jriseph Principal Statistical Officer Population Council
8 Dr C 0 Colman Country Representative Pan American Health )rg ni~ation
9 Mr ranca Kippel Health Education Specialist Ministry of Iea th
10 (1 bullbullines Principal Nursing Officer Ministry of Health
11 Dr Mx won (formerlyHinistry of Health)
12 M3 late Carops Ex-Chairman of Population Council
--
4i 1_ middotIIlt F-ntCWclOotf_Y v OJ t tl
GOVIIlHMEIgt(I OF TINIOAD AND TOampAGQ - NNISTJY OF HIALftf AIJIE1 2NATIONAL FAMilY PLANNING PROGRAMME
F MIL Y PLANNING CUNIC CASE CARD - NEW CASES - NFPPl
li ~~___ 1 ________
~ ecll-U
-- --------------------- shy~) ~~middot~------------------~~~~~~---CIJ------ middot~ii--middot-middot----middot-middot---middot--------- shy
ltv Writt N_ 01(111________________
a ~4itiJtmiddotl_____ ilIIIltIoI~____~____~-__----- shybull ~4
fie l$ - JO tDql IIfIA- tr-JMimiddot _ iJ 1 Odoor o
14aorielaquol_ _~ 0 lio witIleo-La ~ 01 bull - OJ ( _01 1~ltgt1lh o bull- 0$
AacJcu 0 2 CIIriIWA 0 J Os 0
Yv~MONTH ltnollOf~nfIGHTI
Undu 1100U$ Utgtdn 5SCI Undu 11200 01 ~ 50 - 9949 amp100 - 1199 02UlOO - nn9E~ (
0)~ 10- $99 SiOO -- U9~ lOO -- U99 12400 - 1359)-------_-r----shy ~l)o SIS n600 - Hm1300 -- 019 OJ200 il~9 ~------ 99~ a 1)0 m Os1)00 -- l99 1400 -shy $4100 -- 1S999r--- shy
1500 donl S6000aad O399 - lt499I~- I 0lt
ltII
IJ -IC _~tltlioltgti lS
02 IaampJIIocI OJ 04 laM Os
w Oltwio I_-l(~u IrIaa U
h~~ ~Clubl 01 OJ
IS ~C-n 01 toSIitDI 02
Ji poundI on 01 IriIIIuy M ur 02 IV OJ
WU 10 pltIoII~ llaMtl 411 cIIiId 01 Ol it fIolto ~ do~ _14 rou IIlgtJo 1Ia1 ___~_ shy
40
It _ I 00 ~bull FPIiIJ 1
OJ 02 OJ 06
)0 III- iy wOWcf ~1
aMIIl Os
11 T 1gtlt ( h _______ 4)~
06
04 (MIbullbull middot bIrlI ~___~__~_ (-fIJI ~- -~-- (1HJ 49middot SJ
U 10k 01( 1__ raquo$-4
iU1) DOl F ToWotfOlnC DOl 001 or Do [IP 006 001 OIIgtu___Spltclty DOll Nltmo 010
U1Mo I orcpmiddot laquo55middot16
1lD 001 Foam Toblelf_ICim DOl Condom DOl CoomS~ 004 oe Oos WlttuJn 1J OIkr DSpody) 101~ ~Iu 006 Rhylhm 001 DOG OJO
no wI~lmm 4 cd
(I 0) 1110 01 Condor 03 (lorn bull l S~muoidIl 04 Faa TabioolfIIltr- Os RhyUlm 01 lnJrl tible O Advico 090 06
la slt 1)0 19 loti ~rltnlt) ([)sl or 1llOn) ____ --__ bullbully-J n SV - ~JcdS
v~ Cl NCI 0 30 OJI_O I Wr blJ1h 0 I ~ OJ 1 ~ (fOOd V 01 No 02 laquo 6) Cf4
WIiI 1 172
004 001
j D middotmiddot middot
1 ~
r
~
bull I
bullI I I
r c i
ANNEX 3 Pagemiddot 1 of 5
0 raquo rshy -lt l)J ~ 111 t G) 5 shy (J) ~ -
fT1u
i
MINISTTY OF Ho1TH
NTIONl F~ILY LNNING PR-GRbullbullM-tE
~~5tructions to C11nic ClerKa
How to co~ploto the Daily Rogister
~~ ~~v1sd Daily Rosi8ter replnc~D tho one which is now in use tb$ Monthly PC~ri rOt~ arti tho 01( Ci() Dod PollJ j f m It is a pre-coded form and 1411 cl~1p Jd tl a1I6iniul-mIHvn Oel Clinic nctivi~y
110 )rm rollt biJ coupJot)d lrl cupLtcoto using a o(roon shoot Tho top aheot or oriinai ~ust bl) 6(Ult to tho CQgt1tral O[[lCO and tho carbon copy retained in the Gliaic rilo dll the for6a that ar uD~d betwoen the 1st 4nd the 15th of the oIIollth aut bo subClittud tocho office 35 Lnc blttch Those oomp1cted betwoon tho 16th _lid tqemc of tho month must bo ~cnt in a secJnll batch
P lOvLior hns boon Illllde for 25 clients on cZlch forlll new forlll must b IIlied f r poundh 50[810n2 whothur or not ono or lIIore session are hoIdiit the clinic on he sarne day
I th ro alO more htl 25 clionta 1n attondnnco at tho session the additi shyOhAl m~bOl of clionts 10 clients nu~ber 26 27 etc sh0u1l be ontered on the next Imiddotrlll ~i ttout a1tpoundring the numbtlrs in the cvlumn hond Series
51 ppOfil th~ number of aUcnts lQr that session ws 5 this would mean thllt two rJlS ~ lst be 6ubllIitt~dl the first filled uF 1 tltgt 25 And the laquoIncond 1 to 10 Th~ cal bon ofies should bo st~plod togother at thu t0P l~rt h4nd corner of the torm ard ktpt in the Clinic filo lou IIlU6t stapl~ the originftls in the 8~~ monnshyer for lIub~ssion to the ofticl
ie h~ ll idontiflctior- (cc 1 - )
0 lot Ji 9 anythin~ hGro poundhia is int(mdClc for tha computer code
2 ~~pound~ - Print clOflrly tho name of your Clinic
C1Lic Huml or - (cc 4 - 8) Evar1 Clinic Numbor has 5 digits Virite each dig t il a t$purate box
It Pai~_thllsectgdllion (00 lt) -1 1) - Dl monll 10M
lw) bolte IlrO proY140d fetr olAoh pr 01 thQ dISh Enter tho dA) ldns a R
d16ih
emiddot5middot (0 11 I for 115t ( 0 21 for 5th etc Treat month the am pay
e ~ 10 ~ I for I-hrch 0 [2] for September Tho y~nr must be (into ad
I Z I ~ I I 71 q etc
Take as in IixulIple tho dOlte 3rd tllrch 1973 7~ie must bo written
[0131 LSLDI[7l3JDny Month Ye~r
5middot 1~J $~~ - Irom ~-------- To --------shytntol hOI II the time the Clinic 111118 in SW5sion emiddot8middot
(i) 11011 500 lm To 1200 non
(11) Frclt 100 pm To 400 pm
(iii ) IX-OG OO pllI To 6~00 pm
f
2
ADEJ ) Paae ) of S
6 Eov
_ 1hA 1gtIpoundC iIIUlt be nu~o7Ifd tler1ally 1 throurh n lU tbey Are Wled In ~1l8ellJ IInel 1301 tlU 1 Orcl 1 Wled tor a o5038ioll - -I 2 tonY tho _boul~ b I1WJbtl 1 and 2
hlrlll are 25 linos OIl the fOnl Ilnd thoae muet be UBtleS for 25 clients 9 one ior bullbull 01 I ini
ot ~h lc II ol1cM lOlivpound til e linic before soeinc DurOI or doc tor ilnc ii hox rristrltltion nUlJbet had alrearll been recorded on the Dai 1y Roiuter then n line ~hollld be drawn through that entry an1 the eliort nust not 06 includttd in tho totals tor that 0eDion
1lw Ileifitration Num)~r of cueh client must be IiIritten IS n 5-dlrlt oode ClhnC IH11IlElr 315 1IIU8 tborotore be enterod 18J010117]5]
~ Clt ZOt
Coda 1 Codo
10 ~tl c 2t j co 21)
~w elSe - Coda 1 0) d CltaEl - Code 2 Revislt Code 3
Only pound1 01 theBe coiles may be usod
11 prol-O~ ~Eil~1 (cc 22)
If ma climt was L drop-out IIho haoS returned now to the Clinio tor tho first no linmiddot bullwin lt1ro1eo o t he or she should be given CCe 1 It this do 5 II It nprlly leu this colWlln blank
u Hothod middothisllill loe 23)
NOh til t otly ~ Cod 16 tp he ontered in 2lpound of the columna oven thOUGh 10 co11lllJlB 10 provided on the torm The Codes llrol-
Oral Contraceptive Code 0 1 U D Code 1 Condom plUD Codo Z Condor (only) Code 3 Foum tAblets cream Code it DitphrClGJII Code 5 Rhythm Cde 6 Injectible Code 7 Advice Code 8 Other Code 9
It for middotDo-le 1 client rlllll ji yen cclldorls ord foam or creall Iou Qust entor Coole i (condom plulJ) in the appropri~te column This Quat be the only lIotmiddot) tarcie If an in the cnse of a tlnle clinic I the client is Bup)lieu lith COIlOrW only you rmot entEr CorlQ 3 (cpndolll) Do not use a ticII ~ tho (odo Nwber
It is CUi tomary fur 11 cliont 110 is beine put on the oral contraceptive for the first tiT1o and even on other occasionn be issued condoms and 11 crelle or foam a Ilell rI3 a pgtcket of pilla In such Cllses when the piDQ Ilre Ilctually iouou you tlust record Orll (Co~e 0) 08 tho onll metbod ilo othor ntry sll0uld ho nnrlo
Uovever n SJC~ canas vucru condoms and fOHa ~rc eiven but no pilJa (even thoJRh _t _n the intention to issue pills nt the noxt vioit) than the Mothol Th5 ifli t ohoulcl be recorded uo Condor Plus (Code 2)
13 Seen Bybullbullbullbullbull
~rot S-1 SO l
Doctor (Dr) - Code 1 j Nurse (Nul ) - Code 2
Clark (Olk-) - Code If tho Clhnt is vcen hy both tho llootor tlnd the Nurse enter Code 1 t Doctor It 6~61l by the Nurso only arite Code 2 Cod bullbull Cerk is l)llnt for FA Cllnica Clerks in tho Government Cli1t hiwo Llttoll istructed not to i56uo supplios on their own volition
14 fl221~
lhio S~tiCl of -Ie fvrtl t~ke 16 (llrci coluMna (cc 25-+0) nnd 10 tho only part at th iOIQ in llich iore thAn one cod is Zlccoptl1blo Tho purpoco of the )ecton is to 0 able to arrive nt the Cjunntity of 6tock dilltlitJutshyed YOI IIlUdt writo in the CllllOjH-iata colulna the nUllbJr of Il1ch 4rtic1o i~JSu~d ~lo e ha I Oral Contrcilpti vea are aub-di vi dod into types ae_ 3 PIllCKC 9 0 Elynnn LlUot be entered Codo in card column 25
If tor eXllrplc t l cliunt is iosued wi th packots of Zucynon nnd aJ(1 ~ivn 1 conuotll (8inoloo) you ouot enter in oard column 25 and 11 It
cnrd col~8 )2 and J (io 1 in card colucn 2 nnd 2 1n card coluun 33) Nota C)lldoIlU ale to b(t ruoordod individually not os packots of throo) Should n ne LlondoClo be isoued thil3 is to be rc-Qed as 09
If It clint 6 t~ot isoued Blly lIupplies thon you must writo Codo 1 in CQllAlilD 41
It Q eli nt isite the clinic to check on her LUD or her Diaphra~t IUId ro DI W 6 ppl ills nre ispounducd then Code 1 1s wri t ten in column 40
In the FA clinios here a variety ot orll contraceptiveo in orer~l tho elerll wilmiddot~ bJ provided with a specill code shoot The idontifyin coo will b wiittn in Column 29 nnd the nUlber of packets iosued in colwm )0
lralaer-In Code 1 lrllllsie r~ut Coda 2 leIllPQrArr Trnnsfer-In Codo gt
In the cao of n 2ratl8fcr-In I you lUot n160 cOrlpleto coluons 42-51
In the cllU J of A ~~emporary TranGfor-1n (an individual who i8 only v1citing fur clinic tor some epecial trcatcont hna who will bo rdnlnin
~middot(II~~~fO~l~SIl~I3~nn~~~h~rO~nh~1~~190~~nll 2-46 and ler rei IItrntion numbu in colullnll41-51
It the oli( nt i iNt a CrllnoforwIu - Out or loClporu1 tMn loave oolumn 1 blank
16 lr4nst(gtr-tl2~~morrry TilJnder-In (co 42-51) Forl1ltl CUn E1~ (cc 112-46)
hen you rei iatlr L irllsfcrln or Il TJlporary Trnnsfer-In you IIIUBt write I ere the five-digit clinio nucbor of the Clinic iraQ which tho ltlient Me (uIlO
2mer ]letr ~2n ~ (cc 47-51)
frlta fllao Clo r-~itrlltion Nuc~Er ot the client in the Former Clinic (i c bullbull th 1 Sis rnmiddotion ~UlIlh()r which the client carrics 1n the tormor clinio) bull
It tho Forrltl Ho( ist rntion Number iIJ not readily wnilnble you tluct oocpluto thtl epcciol [orlll Transfer-In Not Identifiod Dy Forrlcr RCGi(trn~ t10n Nwlbvr Or ~ flt)rCl is to be cOlplctcd for och cnso nnd th forlJO Ilubmi tted to thu )opllntion Prorrnnme Of fice tOGether with tho Dily Ro~iBtors lhwev~r should the clork leuTI of tho clint B FormlI Uocintra tion lUlllb r )0[(10 Cubmi ttinft the D1ily IOCI otro t hen the nUQbcr shoulo bo -ri ton in colucns 47-51 lna the special foro should lJo deotroyotl
l7 bullbullbullbullbull
r lt bull bull
ADXI ) Pap S ot S
11 UD LV~ (cc 525)
It tb( cliont io ~ivQn An IUD tor the firot tl~o then you should Sri to Codo 1 Inuort ill colurJI 52
It tho olimiddotsnt ia rvinGgtrtltld i th An I UD bullbull tben wse Coda 2 RelnDltlrt shyin (01Uil11 52
It the clLmt is ~tte~~dint chnic beruse her IUD CflClQ out by Haol (cxpll Iion i ~hcn fir te todo ~- UIlllrli1 53~
If c-ltr IU fj IIIS reov in -ne cllnic by tho doctor or nurso t~on vlritI Codec in column 5
II the eli nt otends eiLlie tld explin[l th(lt she rccovcd the IUD tlllleel nen write Coda H in Colwlm 53
It the IUD jr still within the uterus nd the WOIraquoI1 1 11rc6llJlnt thon lIrite 1gt40 4 in Column 53
lZ np h5t (ce 54) It 0 Pull 5mor ie t~ken durin thi visit tben Codo 1 ehould be ampDtere4 in ColWlln 54 Should he c110nt lltt rQ(uircd to rttturn to clin1c for a rogtol1t Pnl) t06t then CoLe 2 llhould bo middotwrittcn in column 54
It no Pllp Scou io taken tde visit Itove colUQn 54 blank
Iraferti1lli (CQ 55)
Ii the e liett io nl1 infortili tr eaoe use Cor1o Ill in colUQn 55
If tbia 1000 not tlpl lonve column 55 blonk
20 Totaltll
CO~1ploete the [)ldegO 1gty puti YI tne totals betweon the double lines nt tu b()ttctl Carrj colUlllnc 20 21 nd gt4 Must hlve tho Bnoe JllIIber and thiG Would coreslonc to the numocr ir attencbnco
Writ$ th to1ul nUlllior of Drop-Outs returned (c022)
Urito 41eo tb totnls fOJ each card column 0 to 9 under tho h(adinu Method thiB Vioit Show tho tote L fgtr OlCl type of contraceptive issued (cc 25-40)
1)0 Dot wrLte 1111 totll lUl(Ier Card Columns 15-19 29 41-51
21 COPmllh bull ~lt h~t~ Monthly ROilort
OQ thG DaLl oCator forlll thnt ccrrOspOldB to tho 1(8t 1$06610n lt 0
oth yo Olllt (vwlgtleto the items nt the botto of the [orampl This is tour ontll~1 n(olt nnd includcD tho totll lumber of sesions Ilntl tho total Iluolcr ( r crop-outs durinr the Qonth
An tiUlsilt n drir which n doctor liB in nttcndnncc is a doctor sOfll~1on and shoulc 00 re(liGtcnd in coltns 56-57 All other sessions 1116 conlliid~recl supply stllciona and thtlY 1110 rocordod in columns 58-59
the total Ilum)nl Jf drop-outo ld the drop-outs by method durinc the onth nre 10 bu oltorou in the inrlicllted boxes
72 Chad Your ~
Milke I ura th t all thE fijul4gtu rre c101r -tNever writo our nutlUQrS 50 InrjEl that they oxtend out of tho
ap~rotr1ato ~ox
Cheek to BoJa tht 1111 numuors 1110 in tho correct boxes -- CJslHloially when Writi1 the totlB
Mllxe Cirtc O thmiddott t1e infoT1I1ntion i6 clear on the corbon COllY before sep rmiddotinr the sheets
Jitn the Fomiddotl lien tly sien YOUl nr me 1t the bot tOil right hnnd corner btl forc subol ttinG it Keep tle CL rb n copy for your rocordn
i
-l ________~~---------~
I _1
Adminiatr-atlve SKVieu
P inba ~~~l1cal lrlnbin~~eltltcal -1 te~ra t~~rvicc (lnatittloaa)
--1- - shy -1------------_-L_ l-r-aJiil- shy _-L_tet1lal d
PlIinm1tJ8 atdUon DetalMid H8Il1tb ~ ________bull Care
-----~ Office of i
the FlIily _IPlill3 roarshy
1- - - -------RegiatUll urnr
ltIi 1 Drelttor Rcgicaat Director Souta Tabqo tacallortb ~ counu gt____ ~ (4 ouottet)
Off1ce of the Res10nal Diractoc L
r----- _L_ -- shy i I bull IREgional Ipitl I
District IIttaltb I bull Othn RelOl ond Hcpital CenteIntt itlt j In 1__ _shy-~- ---- -_j
J r Ii~lth
C~nlef
L
I Ihnlth lie I th Offlcu (1ft lc~
Coullty 1I0p1ta1
Henlth tentet
I

----
- 7 -
Althougr amJnp the neH acceptors in 1971 the users of oral pills were only 509 ~mon~ the old cases the figure was 119 The percentage of IUD users has remiined stagnant at an insignificant level this may be partly due to consume prefErence and pctrtly outng to lack of trained staff to undertake IlTD i1srti l7U There h hOHever a visible shi ft towards the uSe of othe~ ilettods (npchani81 and chemical) attributable to a scare about the side efects nf oral connaceptives Among these conventional methods the condom s 11 os popular
307 J t )resent fami ly planning services have been extended to 48 out of 106 hellth centersoffices run by the Government and the objective is to C)Vel t1e remaining health centersoffices within a short span of time so that adice and facilities for the practice of family planning are conshyvenient Ly wa nable to the people in all parts of the country By ann large sepanit e fITti ly planning eli nics are held on specified days as an addition to norrral lealth work Besides doctor sessions at the clinics supply sessions are rur by health visitors and nllrses assisted by clerks The nurses are authorjzed tc issue oral contraceptives for a period not exceeding three months ani the acceptor is required to attend a doctor session for advice during thi jnterval In 1971 the numbers of full-timepart-time staff in Gov~rtmnf centers renderinp family planning services were
Full-time Part-time
1elical Officers 14 8
NUseMidwives 35 19
Cl~rks 3 17
Now tile low~rnment -gtbjective is to integrate family planning services into MOl services and use the same staff being used for the delivery of both types of erlices at multi-purpose sessions However so far only 1A centers have interated family planntng with Men or gpoundmeral hpalth care sessions
3011 The Family Planning Association has eight unf-purpose centers where famil) pLmring services are available ftve days a week The Association employs tilrEe full-time and ttJO part-time doctors a complement of 14 nurSeS (who llave been trained to do pelvic examinations) and 11 other clinic staff membels The Association also has a number of voluntary workers in the clinics The CithoUt Marriage Advisory Council has three clinics but their contri shybution in terms of enrallment of acceptors is not signiflcant
3)9 A Post-PartumPost-ALortal Program was started in 1969 It is state I tlat about 14 percent of the patients reached attend a family planning clini~ 1iTj thin six weeks of the interview in the wards IhiR is qui te a low figur In 1970 when a system of home visits was tried under the Family Planning Aide Project in 7 clinics the rate of acceptance doubled in three clinils rose by 50 percent in two clinics and increased by 24 percent in one clini (No change was noticeable in the seventh clinic) No decision has been Inad~ tmiddot) continue extend or modify this Project
A Po~ulaton Council ~-----------
401 he fu~ura ro~ Lh~ ~~~01ati0n Council has to be considered in theli1 A the tasK t~ lL ahead of the ~ational Family Planning Program At pesent tile officil~r(QSrJ1Tl is prirnarily concentrating on two objectives (a) tIlE excpound1sinrt of fmd plannin~ services to tie remaining 58 health centen cLJs as rapi(ily as possible and (b) the integration of family planniT g VI tr MCH services Thus thG administration of family planning serviCHJ will be merged into and become part of the Community Health Services Since t is ()rganizationally undesirable to disturb unity of command a separa1e elteecutive agency for the administration of family planning services is preempted within the existing policy framework An executive role for thp Pcnulc tinn Council is there fore ruled out on this consideration
402 If the Population Council is to function as an advisory body at the p()Lic~ aId progra1l pLilnni-l level snd not to concern itself with the minutile If program execution there wonld be no advantage in giving it a statutory stltuS But if it were the policy of the Government to set up a verticll )middotro~ram for family planning ii th a field organization separate and distir~tOroll the HeaHh administration it would be quite appropriate to establish an autonOiTiOUS statut()y a~fgtny ntside the departmental setup of the MinisiY of Health d~b a budi~t md staff of its own commensurate vith the rE spo lsi hi Ii ty to be rEs j Freed from the usual departmental conshystrailts ~n the matters Cif sp(ndlng a1d hiring and firing of personnel such an aglncy c(uld move faster than a heavy-footed departmental formation wi thin a Mins trl bull Hovever a hody of this eharacter would need to be cas t in a cliffe ent m(ld than the present Population Council The shape that it would take lrould be more like a Board of Management with a full-time Chairman or Execuive Director and with more functional expertise than representational charater But an advisory council with an autonomous status and no responsishybilit f( r lrogrrun eXIGulion iould be a source of friction
403 r~e existence of the Population Council as an organ of policy advici has certain advantages Firstly it is a forum for developing a national poLicy in which officials and non-officials participate Secondly it pr )vi bulles a focus to ti1e official program vhich it otherwise may tend to lose as ~ontraceptive services are merged into the general health services Thirc lymiddot- and this is important -- the Ministry has extra-departmental advice availabL to it~ but the Ministers constitutional responsibility for the condl ct )f the national progl~lt~ le1lains unimpaired
404 ls an advisory Q(dy the Population Council should be more broanshybase( than it is at present For instance it should include representatives of tile organizations of employers and vorkers associations of the medical nursngmct teaching professions and organizations for womens welfare The Counil should also haye a social scientis t on it On the official side the
- 9 -
Permane It Secetary and the P1O (fen and FP) should be brought into the Council he inclusion of the Permenent Secretary would open a channel of communi~aton with the MOR ae the highest policy level next to the Minister and would (ontribute administrative expertise to the deliberations of the Cou1ci1 ~m f icili tali 5 (pleuenrti)D of th~ recommendations of the Council within the -rni and in OUltL depa-cments The inclusions of the PMO (MCH and FP) wOlld el) emphasi ~2 hs responsibi lity toward the family planninR program Some officrs of the HOH (eg Chief Health Educator Principal Nursin~ Office e) may 111 ea~e to be members though they may attend as requirE d nmiddot the agenda before the Council A representative of the Ministry of Fin nee stQuId be inc~uded in the Population Council This would make for a lettr appreciation of the needs of the Program in that Ministry and fadIi ate fj nancial sanct ions
B A~tatutory Council
40S In the foregotng Pgraphs the view has been expressed that within th edsting policy framework an advisory Population Council would be more tli)prcpriate than a COlincil wi th executive functions and powers that an advisory rOUlcil would not gain by having a statutory status and that if a statl1tory body 5s to be set up in lieu of the existing Council it would need tC b structured more Iiice a Board of Management than a council wi th a repre13entttional charact~( n the latter event the statutory council should have fu 1- time Executive Chairman or failing that an Executive Director functj oni1g undel- a Chairman trno can devote considerable time to the business of tlw COlncil
406 T1e Statutory Council should have its own budget with full operashytiona pOlo1ers It should have the authority to appoint its own staff and regulLte their conditions of service If it is constitutionally possible the Couner1 shollld be outside the jurisdiction of the Public Service Commission in pesornel matters
407 As an instrument of Government the Council should be subject to such ~eUfral or specific directives that the Ministry of Health may issue to it frcffi ime to time This should be written into the statute under which the Cmntil is set UD
408 The composition of the Council ould depend on the functions assig1ed to it It is suggested that the Council should not concern itself wl th the delivery of cliric selVices in the field The Ministry of Health may (ont nue to administer rampmily planning services at Government hospitals health cmters and health offices and the voluntary agencies should run thei] OWl ~rogram The following functions may be handled by the Council
- to shy
s rrogram plannin and target-setting
b proram monitoring and evalllation
c wiL of d 1ci(JTIdnCf by inspections
d Qrg8lizatim 0 es and marketing of contraceptive J~1J-s BLl (iV es at subs idi zed rates through es tablished 1 2 d(~ channel
e information mass media communication and audiovisual ublicity in the field
f prorrotion of famil~r plannIng acceptance through face-to-face cotlmunication by poundi eld workers in domiciliary visi ts
g trIining of personnel
II pr )motion of -esearch enJ
i financial support to voluntary agencies providing family planning services
409 n Statutory CCii1cil may corsi5t or an eminent non-official vith a comri tm ~~1t towacds foJlily plailninf nd the fol1owin~ members
I ~ bull Pfrmanent Secretary ltl-tIlH
Chief Hedical Officer HOH
i Principal ~ecHcal Office ~mH
d Pilhlic RellltionB OfJte(middotmiddot Prtm~ Ministere Office
A represen ta ti V~1 of the Ministry of Education
f ~ representative of the Ministry of Finance
g A representa~ive of the FPA
h A representative ot the C1AC
i H social scientist fcum tle University of the ~Jest Indies
j Three non-officials with experience in management and administration and the
k Director of the Family Planning Program - Secretary
- 11 shy
The COUlcil ITIltW constitute cOlClmittees for Finance - Accounts Personnel and Sup lies nd Stores ir~whi ch )nly members may be included Other commitles sc1h as those 01 training info1nation and education and researCl ara ~valuation r1ili also include experts from outside
410 he Off1ce raquo) cc im Panning Program which at present forms part of th ~Hnis try or [i n should be placed under the Council and its staff strelgtl ilcn~ii2 i~ r181 it may cease to depend upon the services of the Mir is t y of H~alth
C Office of the Family Planning Program
4 11ollwther the Offic~ of the Family Planning Program remains a part of the Mirisry of Health or is transferred under a statutory council if one is set uP i needs to be strengthened to meet the requirements of an expAndshying pr )gn m At present the following sys terns need to be ins ti tuted in this Office
a a 3ystem of setting annual targets for the enrollment of acceptors and the projection of service fadli ties in relation to these targets
I Ci ~ystem oE V)glC loHitoring (the monthly statistics flowing from the clini~s c~iiiain unproc(~s5erl for months)
a system of program evaluation eg demographic effect of tte program cost studies
1 an overall design for media communication based on a study of the reach a~d cost effectiveness of different media and the effect of the meflBsge content and
e a m88t~r plan for training which would comprise an assessment of the training needK of the existing staff and future reshycruits and a long-term plan divided into annual programs
412 Th2 Prograll afiie s~lould have the services of a demographer and a meeia expert A training adviser is expected to be provided by the PARO
413 1be Program Office should evolve schedules of field tours to overliee field operatio1s E~1eh health cente heal th office should be visi ted peridicaLy by the Milt~dical fElce- the Nursing Officer and the Health EduCltoI who should guide and assis t the local staff in carrying out the progam Their tour notes should go into separate dossiers for each institushytion and ~ach dossier should have basic demographic data about the area coveled by each institution These dossiers would be a useful record for revilwing l)errOmance The staff of the Program Office should be augmented to Ol)erte this control procedure
- 12 shy
D Decentralization of Powers
414 ~hete is a concentration of administrative and financial powers in the 11in s try of Health I-JllJCi1 results in an accumulation of references in the Miristl) and delays n field operations Specific powers should be delegated ~o (a) the PliO concerned with MCH and family planningmiddot (b) the Directcr o the Program Office (c) the Regional Director and (d) the County Medica1 Oficecs The Ministry should invite suggestions from these officers and wOlk 01t a schedule of delegated powers
415 A tdgh priority in the matter of delegation of powers is to arm the Regiond Directors with sufficient administrative and financial authority to implement with expedition the health and family planning programs of the Ministmiddoty 1 thin the areas in their jurisdictions
E Integration of Family Planning wi th Haternal and Child Health Services
416 At present family planning services are being provided at 48 Goverrnent hospitals health centers and health offices by using the full shytime E taf cf these institutions and employing part-time (sessional) doctors nurse~ anI clerks where necessary At 29 of these institutions separate famil cl~nics are held on specified days in the weck some being doctor sessi(ms mel others supply sessions run hy nurses and clerks At the remaining 18 imtit1tions family planning services are combined with antenatal child healtL cr postnatal services The Family Planning Association runs 8 unishypurpoe f am ly planning centers which provide daily services and contribute a 11 t le less than half the total number of new acceptors per year
417 N assessment has b~en marie of the effect of integrated MOl and famil~ p~ nnning services an the recrl1i tment of acceptors nor were ~ data readily avallable for this purpose It may be observed however that in a situation of shortages of trained personnel for health services utilization of the existing health staff and facilitieR for family planning is inevitable parU cllLrl y in the interior where such shortages are more pronounced This underlines the need of evaluation of the integrated xai and family planning progtam for its impact on the number of acceptors Also a study needs to be made of che utilization of medical and pilramedical manpower so that it leads to bdter ~llocation of duties and optimUJl utilization of personnel
418 ile integration of faMily planning into Mcn services has certain advalltages as well as attendant risks The advantages are
a Lbe association of family planning with the care of mothers and children helps project a benevolent image of family planning as a program of family welfare This creates a
- 13 shy
1imate favorab~e to the acceptance of family planning aa lt p-)si tL1e il-Eare rreasure rather than a negative program cE limiting c~ildren
h t elps erlist ~r2tion tf doctars and nurses who as c -~ass enjo tft~ Y)er)et~ a~d confidf~nce of the communities i712~ Eerve
c ~ieD of contact with women
d luni-purposa clhlics for ~lCH and family planning services are onenient for motn~rs who would have to travel considerable (listances to the clinics
e hete is better utilizat1on of Acarce heAlth manpower
419 he limitatio$ of integrating family planning with MCH servicesI
are the posiOili ties of loss of focus on family planning as a high priori ty prograrr ald the diffusion of pol1sibility for its implementation These could tlow ve r he safegurded agaifls t by adopting the following measures
a 11e job descriptions of doctors and nurses should be rewritten 0 include the family planning function
b hE perf0rt1iai1ce of ctoltors and nurses should be judged as much )y tbeir inteceq t in planning ~vork as in maternal and ~hjld care and this should he lade known to them
c )octors and nurses involved in ~CH services should be given middot)rj entation and traIning in famj ly planning and their interest 3UEtained by refresher courses seminars meetings and supplies of literature
d Thl techrical (xpert~ in the Office of the Family Planninl Program should maintain liaison with and guide the field agencies in implementing the family plannin~ program For this purpose schedules shoul d be marle out for periodic field inspections
420 It is suggested that the working of half-a-dozen centers where family plbnnLng services have been integrated wi th MCH sessions should be studiei for ehe purpose of standardizing the methodology of delivery of servicl~ Such a study should include staff strength patient load recoril shykeepills 10middot of patents in the clinic timing and frequency of clinic sesaios ani convenience vf patients
F Voluntary Organizations
421 I i~ internrticri31 expedence that the birth control movement is pion aTC tt volunh[~ JilC S Qltl that hen the national governments step in wi tl cmbi ti 019 prjhns wi thin the sLate welfare system voluntary bodies ieh tteir limited ilsrluces restrict their service activities and shift the emplasi i 0 educedgt (f the community training research and contracepshytive Sf vic not 1l7gtilflblr in he official program or in areas not reached by it In nagni tude and expanse the of ficial program in Trinidad and Tobago has alrad~ orertak~n Ce 101umary program Increasingly it will become the domLnart tartner in the total national program while the voluntary agencies will cOltirlU1~ to receive financial support and encouragement to set up high standaeis If service and explore new areas thus acting as a stimulus and an additi_e tl the official program
G FrOB-ram Infomation
422 Thre is no concurrent evaluation or monitoring of the Program The daa or lq72 flowing in from the clinics month by month have r8Jllsined unprocss~d tn the Program Office The official Annual Report - 1971 Sums up th~ poition as fcllo~s
ITThe Research and Evaluation component continued to be the weakest in the Population Program Although a systen of evaluation had been built into the program the follow-up procedures for analyzing the data and for correcting inshyconsistencies are inadequate Requests were made to extend the staff to establish a more viable unit but by the end of the year no chllnges had been made
423 T1e recording and riporting jJrocedures were revised effective Januery 1972 and there has been a further change recently at the instance of t1e Evaluation Adviser Under the system now established the clinics are lequ Lreurod to maintain the following records
a Family Planning Clinic Case Card - New Cases This was introduced on January 1 1972 and has thirty-one entries giving age parity contraceptive listory pregnancies socio-economic background ource of family planning information and agency for notvat ion bull (Annex 2) The case card is made out in duplicate for each new acceptor and a copy sent to the Program Office
b Daily Regis ter This fs a ne~gt1 form recently introduced in replacement of the old regis ter and is preparen
- 15 shy
ie) ruplicate the original to be transmitted to the Program (fHce and the carbon copy to be retained in the clinic Th~ is a very 121zborute form requiring 36 entries to be aa~ for each Chse nel and old attending a session includin~ (ntries to cit L to contTaceptive supplies issued
AijCleX 3 T~13e fcnnG are required to be sent to the Program lffce in i7JO balches every month the first batch for the i IS fif~eeL days and the second for the remaining part of hE month The trtention is that the data appearing in the ~EZlic daily legis ter forms should be compiled in the Program Office and fed back to the clinics Although it is claimed that this new form has been pretested and is workable ex)erience alone will show whether the majority of clinic cL~rks are able to cope with it in a busy session
bull o now-Ho Card TIlis card is intended to keep track of ac ceptor--It has entries for name addresfI and month fcr which a visit is due for each year
bull Aphabe tical Index This is a card index of clients with aidresses
Each i)at en is given a simple clinic card on which the dates of further appo~utnli rc3 an~ indicated A special fonT[ has been devised for the reporting ot cases unler the Post-IartumPost-Abortal Education and Referral Program
424 J system of monitoring progrRm performance from month to month need to bE develQped as a high priori ty The problem is not so much reshycord ng mc transmission of data by the clinics but its aggregation and proclssi ng in the Program Office every month which at present takes a long time The Statistical Officer should have a statistical assistant to help him Ln I he taflk Monthly progress reports should be available to the Mini H t~ n H(llllth and A11 offt eerlil of the ProKrnm Office so that remedial ac tl m I lAY h(~ tuk~n n rll1u- WhOnh1f ~Hfl(AlJtlaTY
42 For the analysis of data and evaluation the Program office shouln haVE th(~ full-time services of a trained demographer
H Field Workers
42) Tie Program nemiddotis tne services of a cadre of field workers to enr)ll neii aceeptoTs follow up acceptors in their homes and revive the int 2remiddott of dropouts Such a category of workers could also be utilizerl for pr1fficting other health programs such as the VD campaign and the inmuni~ation program
47 As an experimental measure one field ~]orker may be assigned to a emi l~ of Hi 000 population This would mean 100 field workers in all
- 16 shy
Earh of the workers should preferably have harl a higher secondary education otherwLe 1gt junior secondalY education They should be married persons with middoti1ltt mot tl-an two or tlree children recruited from the locali ty in which they armiddot~ requlred to function Only persons who have the capaci ty to comnunl at~ and or6anl~e should c chosen A months ini tial orientation
slcu1d enable them to start functioning in the field though reshyfresher CO rSeS tvould be necesslt1ry in due course In Port-of-Spain married mer~ a1C women may be employed on a part-time basis
I Hanagement Study
428 A nanagement study of the Family Planning Program should include a sctu iny of the top m~nagement Atructure (Population Council - Office of the Fanil) PLanning Program - Principal Medical Officer for MCH and Family Planni Ig fetices) the field structure for the delivery of family planning servics (Re0ional Director - District Health Services) including the utilizlti(n if medical and paramedical personnel for adding the function of del ve y )f family planning services and the control and communication proCed1reF Lfnking the top management with the field structure
429 The management consultants may study the functioning of the Popul tio I Council and advise whether it adequately serves the purpose of givini po Licy direction to the Program and if not what changes in its compo itt m and operating procedures may be introduced without altering its bsic craracter as an advisory agency The consultants may suggest an alern at ve form of organizati)n and utilization of personnel which in thir p nion may be better adapted to the needs of the Program
430 Irrespective of whether the Population Council is maintained or it is replaced by an agency of a different character a formation like the Offic of be Family Planning Program would be necessary for the administrashytion i)f 1 he program a task for which i 1 appears inadequately equipped at preselt Its obvious requirements are in the areas of program monitoring and el7alnation program supervision communication and training The manag ememiddotlt consultants may study the structure and procedures of this form~ tio Gnd make suggestions with regard to the augmentation of professional and ~ upp)rt lng staffgt and modification of operating procedures
431 The linkage of the Office of the Family Planning Program with the Miniutry of Health (Central Office) and the District Health Services should be sudied In view of the policy of the Government to integrate MCH and faI11iLy rlallning services it should be examined whether the Principal Medi al Officer for Communi ty Heal th Services (MCH and Family Planning) should be agtpoj nt~d as the Chief of the Office of the Family Planning Program and an adTlilistrative officer of a suitable level inducted in that Office to assist him TIle implication of this suggestion is that the head of the Family PlanJling Program would control the District Health Services
- 17 shy
432 rf 1e management consultants should examine the delegation of adminshyistratiie Bld financial powers of the Ministry of Health to different levels of Progam aclrlirdstration viz bull PMO Program Office Regional Director and County ~djca~ Officers
l33 he system of 01 af Togram information from the clinlcs to the Pr()~ra1 O~fice and tOile processing and use of information in the latter office iholld )e studied
434 he working procedures at the integrated McP and family planning clinics shnuLl be studied This would involve a study of each stage which a clien tpcticmt has to go through from the point of entry to the point of exit after receiving advice service or supplies This study shoulci lead to star dartization of procedures and functions and evolution of -lork norms CognatE st tdies of the working procedures at uni-purpose family planning clinics and su~ply SEssions should also be undertaken An essential component of these ~ tad ~es would be to examine Nhich functions currently performed by docshytors lealh visitors nurses and midives respectively hav~ become so roushytinize ttl it they can he relegated (0 the next 10Her level
435 Reated to working procedures is the problem of job description of medcal 8nd parrunedical personnel involved in family planning from the centra i tc the field level This job description needs to be studied wi th a vie VIW8Id txaminiDg the uttlization of skills and allocation of time by the staff lcc(rd~ng to the functional prj ori ties
436 frV management consultants should study the workings of the curren slralgements fOJ family planning counselling under the Post-Partul11 Post-Abortal Education and Referral Program at the Port-of-Spain and San Fenaldo General Hospitals
437 SU1ect to the ItBrcement of the Gove1nment the management conshy8ultal ts ~hOLlld undertake a study of th requirement of field workers (home vinitcru) in tmtlUI of are nnd population cov(ra~e
ANNEX 1
Names of Persons Met
Ii Mr T C Taitt Pem1(H~nt 3~crtarY) Ministry of Health
2 Dr M n Henry Chitd Medical Officer Ministry of Health
Ellubeth Quam a Prindpal Medical Officer (1S)
4 Mr G Z Jaine ~ uJiector Population Council
5 Dr Norma Andrews Medical Officer Population Council
6 Mr Jc~n Coury~ Evaluation Adviser Population Council
7 Mr A Jriseph Principal Statistical Officer Population Council
8 Dr C 0 Colman Country Representative Pan American Health )rg ni~ation
9 Mr ranca Kippel Health Education Specialist Ministry of Iea th
10 (1 bullbullines Principal Nursing Officer Ministry of Health
11 Dr Mx won (formerlyHinistry of Health)
12 M3 late Carops Ex-Chairman of Population Council
--
4i 1_ middotIIlt F-ntCWclOotf_Y v OJ t tl
GOVIIlHMEIgt(I OF TINIOAD AND TOampAGQ - NNISTJY OF HIALftf AIJIE1 2NATIONAL FAMilY PLANNING PROGRAMME
F MIL Y PLANNING CUNIC CASE CARD - NEW CASES - NFPPl
li ~~___ 1 ________
~ ecll-U
-- --------------------- shy~) ~~middot~------------------~~~~~~---CIJ------ middot~ii--middot-middot----middot-middot---middot--------- shy
ltv Writt N_ 01(111________________
a ~4itiJtmiddotl_____ ilIIIltIoI~____~____~-__----- shybull ~4
fie l$ - JO tDql IIfIA- tr-JMimiddot _ iJ 1 Odoor o
14aorielaquol_ _~ 0 lio witIleo-La ~ 01 bull - OJ ( _01 1~ltgt1lh o bull- 0$
AacJcu 0 2 CIIriIWA 0 J Os 0
Yv~MONTH ltnollOf~nfIGHTI
Undu 1100U$ Utgtdn 5SCI Undu 11200 01 ~ 50 - 9949 amp100 - 1199 02UlOO - nn9E~ (
0)~ 10- $99 SiOO -- U9~ lOO -- U99 12400 - 1359)-------_-r----shy ~l)o SIS n600 - Hm1300 -- 019 OJ200 il~9 ~------ 99~ a 1)0 m Os1)00 -- l99 1400 -shy $4100 -- 1S999r--- shy
1500 donl S6000aad O399 - lt499I~- I 0lt
ltII
IJ -IC _~tltlioltgti lS
02 IaampJIIocI OJ 04 laM Os
w Oltwio I_-l(~u IrIaa U
h~~ ~Clubl 01 OJ
IS ~C-n 01 toSIitDI 02
Ji poundI on 01 IriIIIuy M ur 02 IV OJ
WU 10 pltIoII~ llaMtl 411 cIIiId 01 Ol it fIolto ~ do~ _14 rou IIlgtJo 1Ia1 ___~_ shy
40
It _ I 00 ~bull FPIiIJ 1
OJ 02 OJ 06
)0 III- iy wOWcf ~1
aMIIl Os
11 T 1gtlt ( h _______ 4)~
06
04 (MIbullbull middot bIrlI ~___~__~_ (-fIJI ~- -~-- (1HJ 49middot SJ
U 10k 01( 1__ raquo$-4
iU1) DOl F ToWotfOlnC DOl 001 or Do [IP 006 001 OIIgtu___Spltclty DOll Nltmo 010
U1Mo I orcpmiddot laquo55middot16
1lD 001 Foam Toblelf_ICim DOl Condom DOl CoomS~ 004 oe Oos WlttuJn 1J OIkr DSpody) 101~ ~Iu 006 Rhylhm 001 DOG OJO
no wI~lmm 4 cd
(I 0) 1110 01 Condor 03 (lorn bull l S~muoidIl 04 Faa TabioolfIIltr- Os RhyUlm 01 lnJrl tible O Advico 090 06
la slt 1)0 19 loti ~rltnlt) ([)sl or 1llOn) ____ --__ bullbully-J n SV - ~JcdS
v~ Cl NCI 0 30 OJI_O I Wr blJ1h 0 I ~ OJ 1 ~ (fOOd V 01 No 02 laquo 6) Cf4
WIiI 1 172
004 001
j D middotmiddot middot
1 ~
r
~
bull I
bullI I I
r c i
ANNEX 3 Pagemiddot 1 of 5
0 raquo rshy -lt l)J ~ 111 t G) 5 shy (J) ~ -
fT1u
i
MINISTTY OF Ho1TH
NTIONl F~ILY LNNING PR-GRbullbullM-tE
~~5tructions to C11nic ClerKa
How to co~ploto the Daily Rogister
~~ ~~v1sd Daily Rosi8ter replnc~D tho one which is now in use tb$ Monthly PC~ri rOt~ arti tho 01( Ci() Dod PollJ j f m It is a pre-coded form and 1411 cl~1p Jd tl a1I6iniul-mIHvn Oel Clinic nctivi~y
110 )rm rollt biJ coupJot)d lrl cupLtcoto using a o(roon shoot Tho top aheot or oriinai ~ust bl) 6(Ult to tho CQgt1tral O[[lCO and tho carbon copy retained in the Gliaic rilo dll the for6a that ar uD~d betwoen the 1st 4nd the 15th of the oIIollth aut bo subClittud tocho office 35 Lnc blttch Those oomp1cted betwoon tho 16th _lid tqemc of tho month must bo ~cnt in a secJnll batch
P lOvLior hns boon Illllde for 25 clients on cZlch forlll new forlll must b IIlied f r poundh 50[810n2 whothur or not ono or lIIore session are hoIdiit the clinic on he sarne day
I th ro alO more htl 25 clionta 1n attondnnco at tho session the additi shyOhAl m~bOl of clionts 10 clients nu~ber 26 27 etc sh0u1l be ontered on the next Imiddotrlll ~i ttout a1tpoundring the numbtlrs in the cvlumn hond Series
51 ppOfil th~ number of aUcnts lQr that session ws 5 this would mean thllt two rJlS ~ lst be 6ubllIitt~dl the first filled uF 1 tltgt 25 And the laquoIncond 1 to 10 Th~ cal bon ofies should bo st~plod togother at thu t0P l~rt h4nd corner of the torm ard ktpt in the Clinic filo lou IIlU6t stapl~ the originftls in the 8~~ monnshyer for lIub~ssion to the ofticl
ie h~ ll idontiflctior- (cc 1 - )
0 lot Ji 9 anythin~ hGro poundhia is int(mdClc for tha computer code
2 ~~pound~ - Print clOflrly tho name of your Clinic
C1Lic Huml or - (cc 4 - 8) Evar1 Clinic Numbor has 5 digits Virite each dig t il a t$purate box
It Pai~_thllsectgdllion (00 lt) -1 1) - Dl monll 10M
lw) bolte IlrO proY140d fetr olAoh pr 01 thQ dISh Enter tho dA) ldns a R
d16ih
emiddot5middot (0 11 I for 115t ( 0 21 for 5th etc Treat month the am pay
e ~ 10 ~ I for I-hrch 0 [2] for September Tho y~nr must be (into ad
I Z I ~ I I 71 q etc
Take as in IixulIple tho dOlte 3rd tllrch 1973 7~ie must bo written
[0131 LSLDI[7l3JDny Month Ye~r
5middot 1~J $~~ - Irom ~-------- To --------shytntol hOI II the time the Clinic 111118 in SW5sion emiddot8middot
(i) 11011 500 lm To 1200 non
(11) Frclt 100 pm To 400 pm
(iii ) IX-OG OO pllI To 6~00 pm
f
2
ADEJ ) Paae ) of S
6 Eov
_ 1hA 1gtIpoundC iIIUlt be nu~o7Ifd tler1ally 1 throurh n lU tbey Are Wled In ~1l8ellJ IInel 1301 tlU 1 Orcl 1 Wled tor a o5038ioll - -I 2 tonY tho _boul~ b I1WJbtl 1 and 2
hlrlll are 25 linos OIl the fOnl Ilnd thoae muet be UBtleS for 25 clients 9 one ior bullbull 01 I ini
ot ~h lc II ol1cM lOlivpound til e linic before soeinc DurOI or doc tor ilnc ii hox rristrltltion nUlJbet had alrearll been recorded on the Dai 1y Roiuter then n line ~hollld be drawn through that entry an1 the eliort nust not 06 includttd in tho totals tor that 0eDion
1lw Ileifitration Num)~r of cueh client must be IiIritten IS n 5-dlrlt oode ClhnC IH11IlElr 315 1IIU8 tborotore be enterod 18J010117]5]
~ Clt ZOt
Coda 1 Codo
10 ~tl c 2t j co 21)
~w elSe - Coda 1 0) d CltaEl - Code 2 Revislt Code 3
Only pound1 01 theBe coiles may be usod
11 prol-O~ ~Eil~1 (cc 22)
If ma climt was L drop-out IIho haoS returned now to the Clinio tor tho first no linmiddot bullwin lt1ro1eo o t he or she should be given CCe 1 It this do 5 II It nprlly leu this colWlln blank
u Hothod middothisllill loe 23)
NOh til t otly ~ Cod 16 tp he ontered in 2lpound of the columna oven thOUGh 10 co11lllJlB 10 provided on the torm The Codes llrol-
Oral Contraceptive Code 0 1 U D Code 1 Condom plUD Codo Z Condor (only) Code 3 Foum tAblets cream Code it DitphrClGJII Code 5 Rhythm Cde 6 Injectible Code 7 Advice Code 8 Other Code 9
It for middotDo-le 1 client rlllll ji yen cclldorls ord foam or creall Iou Qust entor Coole i (condom plulJ) in the appropri~te column This Quat be the only lIotmiddot) tarcie If an in the cnse of a tlnle clinic I the client is Bup)lieu lith COIlOrW only you rmot entEr CorlQ 3 (cpndolll) Do not use a ticII ~ tho (odo Nwber
It is CUi tomary fur 11 cliont 110 is beine put on the oral contraceptive for the first tiT1o and even on other occasionn be issued condoms and 11 crelle or foam a Ilell rI3 a pgtcket of pilla In such Cllses when the piDQ Ilre Ilctually iouou you tlust record Orll (Co~e 0) 08 tho onll metbod ilo othor ntry sll0uld ho nnrlo
Uovever n SJC~ canas vucru condoms and fOHa ~rc eiven but no pilJa (even thoJRh _t _n the intention to issue pills nt the noxt vioit) than the Mothol Th5 ifli t ohoulcl be recorded uo Condor Plus (Code 2)
13 Seen Bybullbullbullbullbull
~rot S-1 SO l
Doctor (Dr) - Code 1 j Nurse (Nul ) - Code 2
Clark (Olk-) - Code If tho Clhnt is vcen hy both tho llootor tlnd the Nurse enter Code 1 t Doctor It 6~61l by the Nurso only arite Code 2 Cod bullbull Cerk is l)llnt for FA Cllnica Clerks in tho Government Cli1t hiwo Llttoll istructed not to i56uo supplios on their own volition
14 fl221~
lhio S~tiCl of -Ie fvrtl t~ke 16 (llrci coluMna (cc 25-+0) nnd 10 tho only part at th iOIQ in llich iore thAn one cod is Zlccoptl1blo Tho purpoco of the )ecton is to 0 able to arrive nt the Cjunntity of 6tock dilltlitJutshyed YOI IIlUdt writo in the CllllOjH-iata colulna the nUllbJr of Il1ch 4rtic1o i~JSu~d ~lo e ha I Oral Contrcilpti vea are aub-di vi dod into types ae_ 3 PIllCKC 9 0 Elynnn LlUot be entered Codo in card column 25
If tor eXllrplc t l cliunt is iosued wi th packots of Zucynon nnd aJ(1 ~ivn 1 conuotll (8inoloo) you ouot enter in oard column 25 and 11 It
cnrd col~8 )2 and J (io 1 in card colucn 2 nnd 2 1n card coluun 33) Nota C)lldoIlU ale to b(t ruoordod individually not os packots of throo) Should n ne LlondoClo be isoued thil3 is to be rc-Qed as 09
If It clint 6 t~ot isoued Blly lIupplies thon you must writo Codo 1 in CQllAlilD 41
It Q eli nt isite the clinic to check on her LUD or her Diaphra~t IUId ro DI W 6 ppl ills nre ispounducd then Code 1 1s wri t ten in column 40
In the FA clinios here a variety ot orll contraceptiveo in orer~l tho elerll wilmiddot~ bJ provided with a specill code shoot The idontifyin coo will b wiittn in Column 29 nnd the nUlber of packets iosued in colwm )0
lralaer-In Code 1 lrllllsie r~ut Coda 2 leIllPQrArr Trnnsfer-In Codo gt
In the cao of n 2ratl8fcr-In I you lUot n160 cOrlpleto coluons 42-51
In the cllU J of A ~~emporary TranGfor-1n (an individual who i8 only v1citing fur clinic tor some epecial trcatcont hna who will bo rdnlnin
~middot(II~~~fO~l~SIl~I3~nn~~~h~rO~nh~1~~190~~nll 2-46 and ler rei IItrntion numbu in colullnll41-51
It the oli( nt i iNt a CrllnoforwIu - Out or loClporu1 tMn loave oolumn 1 blank
16 lr4nst(gtr-tl2~~morrry TilJnder-In (co 42-51) Forl1ltl CUn E1~ (cc 112-46)
hen you rei iatlr L irllsfcrln or Il TJlporary Trnnsfer-In you IIIUBt write I ere the five-digit clinio nucbor of the Clinic iraQ which tho ltlient Me (uIlO
2mer ]letr ~2n ~ (cc 47-51)
frlta fllao Clo r-~itrlltion Nuc~Er ot the client in the Former Clinic (i c bullbull th 1 Sis rnmiddotion ~UlIlh()r which the client carrics 1n the tormor clinio) bull
It tho Forrltl Ho( ist rntion Number iIJ not readily wnilnble you tluct oocpluto thtl epcciol [orlll Transfer-In Not Identifiod Dy Forrlcr RCGi(trn~ t10n Nwlbvr Or ~ flt)rCl is to be cOlplctcd for och cnso nnd th forlJO Ilubmi tted to thu )opllntion Prorrnnme Of fice tOGether with tho Dily Ro~iBtors lhwev~r should the clork leuTI of tho clint B FormlI Uocintra tion lUlllb r )0[(10 Cubmi ttinft the D1ily IOCI otro t hen the nUQbcr shoulo bo -ri ton in colucns 47-51 lna the special foro should lJo deotroyotl
l7 bullbullbullbullbull
r lt bull bull
ADXI ) Pap S ot S
11 UD LV~ (cc 525)
It tb( cliont io ~ivQn An IUD tor the firot tl~o then you should Sri to Codo 1 Inuort ill colurJI 52
It tho olimiddotsnt ia rvinGgtrtltld i th An I UD bullbull tben wse Coda 2 RelnDltlrt shyin (01Uil11 52
It the clLmt is ~tte~~dint chnic beruse her IUD CflClQ out by Haol (cxpll Iion i ~hcn fir te todo ~- UIlllrli1 53~
If c-ltr IU fj IIIS reov in -ne cllnic by tho doctor or nurso t~on vlritI Codec in column 5
II the eli nt otends eiLlie tld explin[l th(lt she rccovcd the IUD tlllleel nen write Coda H in Colwlm 53
It the IUD jr still within the uterus nd the WOIraquoI1 1 11rc6llJlnt thon lIrite 1gt40 4 in Column 53
lZ np h5t (ce 54) It 0 Pull 5mor ie t~ken durin thi visit tben Codo 1 ehould be ampDtere4 in ColWlln 54 Should he c110nt lltt rQ(uircd to rttturn to clin1c for a rogtol1t Pnl) t06t then CoLe 2 llhould bo middotwrittcn in column 54
It no Pllp Scou io taken tde visit Itove colUQn 54 blank
Iraferti1lli (CQ 55)
Ii the e liett io nl1 infortili tr eaoe use Cor1o Ill in colUQn 55
If tbia 1000 not tlpl lonve column 55 blonk
20 Totaltll
CO~1ploete the [)ldegO 1gty puti YI tne totals betweon the double lines nt tu b()ttctl Carrj colUlllnc 20 21 nd gt4 Must hlve tho Bnoe JllIIber and thiG Would coreslonc to the numocr ir attencbnco
Writ$ th to1ul nUlllior of Drop-Outs returned (c022)
Urito 41eo tb totnls fOJ each card column 0 to 9 under tho h(adinu Method thiB Vioit Show tho tote L fgtr OlCl type of contraceptive issued (cc 25-40)
1)0 Dot wrLte 1111 totll lUl(Ier Card Columns 15-19 29 41-51
21 COPmllh bull ~lt h~t~ Monthly ROilort
OQ thG DaLl oCator forlll thnt ccrrOspOldB to tho 1(8t 1$06610n lt 0
oth yo Olllt (vwlgtleto the items nt the botto of the [orampl This is tour ontll~1 n(olt nnd includcD tho totll lumber of sesions Ilntl tho total Iluolcr ( r crop-outs durinr the Qonth
An tiUlsilt n drir which n doctor liB in nttcndnncc is a doctor sOfll~1on and shoulc 00 re(liGtcnd in coltns 56-57 All other sessions 1116 conlliid~recl supply stllciona and thtlY 1110 rocordod in columns 58-59
the total Ilum)nl Jf drop-outo ld the drop-outs by method durinc the onth nre 10 bu oltorou in the inrlicllted boxes
72 Chad Your ~
Milke I ura th t all thE fijul4gtu rre c101r -tNever writo our nutlUQrS 50 InrjEl that they oxtend out of tho
ap~rotr1ato ~ox
Cheek to BoJa tht 1111 numuors 1110 in tho correct boxes -- CJslHloially when Writi1 the totlB
Mllxe Cirtc O thmiddott t1e infoT1I1ntion i6 clear on the corbon COllY before sep rmiddotinr the sheets
Jitn the Fomiddotl lien tly sien YOUl nr me 1t the bot tOil right hnnd corner btl forc subol ttinG it Keep tle CL rb n copy for your rocordn
i
-l ________~~---------~
I _1
Adminiatr-atlve SKVieu
P inba ~~~l1cal lrlnbin~~eltltcal -1 te~ra t~~rvicc (lnatittloaa)
--1- - shy -1------------_-L_ l-r-aJiil- shy _-L_tet1lal d
PlIinm1tJ8 atdUon DetalMid H8Il1tb ~ ________bull Care
-----~ Office of i
the FlIily _IPlill3 roarshy
1- - - -------RegiatUll urnr
ltIi 1 Drelttor Rcgicaat Director Souta Tabqo tacallortb ~ counu gt____ ~ (4 ouottet)
Off1ce of the Res10nal Diractoc L
r----- _L_ -- shy i I bull IREgional Ipitl I
District IIttaltb I bull Othn RelOl ond Hcpital CenteIntt itlt j In 1__ _shy-~- ---- -_j
J r Ii~lth
C~nlef
L
I Ihnlth lie I th Offlcu (1ft lc~
Coullty 1I0p1ta1
Henlth tentet
I

A Po~ulaton Council ~-----------
401 he fu~ura ro~ Lh~ ~~~01ati0n Council has to be considered in theli1 A the tasK t~ lL ahead of the ~ational Family Planning Program At pesent tile officil~r(QSrJ1Tl is prirnarily concentrating on two objectives (a) tIlE excpound1sinrt of fmd plannin~ services to tie remaining 58 health centen cLJs as rapi(ily as possible and (b) the integration of family planniT g VI tr MCH services Thus thG administration of family planning serviCHJ will be merged into and become part of the Community Health Services Since t is ()rganizationally undesirable to disturb unity of command a separa1e elteecutive agency for the administration of family planning services is preempted within the existing policy framework An executive role for thp Pcnulc tinn Council is there fore ruled out on this consideration
402 If the Population Council is to function as an advisory body at the p()Lic~ aId progra1l pLilnni-l level snd not to concern itself with the minutile If program execution there wonld be no advantage in giving it a statutory stltuS But if it were the policy of the Government to set up a verticll )middotro~ram for family planning ii th a field organization separate and distir~tOroll the HeaHh administration it would be quite appropriate to establish an autonOiTiOUS statut()y a~fgtny ntside the departmental setup of the MinisiY of Health d~b a budi~t md staff of its own commensurate vith the rE spo lsi hi Ii ty to be rEs j Freed from the usual departmental conshystrailts ~n the matters Cif sp(ndlng a1d hiring and firing of personnel such an aglncy c(uld move faster than a heavy-footed departmental formation wi thin a Mins trl bull Hovever a hody of this eharacter would need to be cas t in a cliffe ent m(ld than the present Population Council The shape that it would take lrould be more like a Board of Management with a full-time Chairman or Execuive Director and with more functional expertise than representational charater But an advisory council with an autonomous status and no responsishybilit f( r lrogrrun eXIGulion iould be a source of friction
403 r~e existence of the Population Council as an organ of policy advici has certain advantages Firstly it is a forum for developing a national poLicy in which officials and non-officials participate Secondly it pr )vi bulles a focus to ti1e official program vhich it otherwise may tend to lose as ~ontraceptive services are merged into the general health services Thirc lymiddot- and this is important -- the Ministry has extra-departmental advice availabL to it~ but the Ministers constitutional responsibility for the condl ct )f the national progl~lt~ le1lains unimpaired
404 ls an advisory Q(dy the Population Council should be more broanshybase( than it is at present For instance it should include representatives of tile organizations of employers and vorkers associations of the medical nursngmct teaching professions and organizations for womens welfare The Counil should also haye a social scientis t on it On the official side the
- 9 -
Permane It Secetary and the P1O (fen and FP) should be brought into the Council he inclusion of the Permenent Secretary would open a channel of communi~aton with the MOR ae the highest policy level next to the Minister and would (ontribute administrative expertise to the deliberations of the Cou1ci1 ~m f icili tali 5 (pleuenrti)D of th~ recommendations of the Council within the -rni and in OUltL depa-cments The inclusions of the PMO (MCH and FP) wOlld el) emphasi ~2 hs responsibi lity toward the family planninR program Some officrs of the HOH (eg Chief Health Educator Principal Nursin~ Office e) may 111 ea~e to be members though they may attend as requirE d nmiddot the agenda before the Council A representative of the Ministry of Fin nee stQuId be inc~uded in the Population Council This would make for a lettr appreciation of the needs of the Program in that Ministry and fadIi ate fj nancial sanct ions
B A~tatutory Council
40S In the foregotng Pgraphs the view has been expressed that within th edsting policy framework an advisory Population Council would be more tli)prcpriate than a COlincil wi th executive functions and powers that an advisory rOUlcil would not gain by having a statutory status and that if a statl1tory body 5s to be set up in lieu of the existing Council it would need tC b structured more Iiice a Board of Management than a council wi th a repre13entttional charact~( n the latter event the statutory council should have fu 1- time Executive Chairman or failing that an Executive Director functj oni1g undel- a Chairman trno can devote considerable time to the business of tlw COlncil
406 T1e Statutory Council should have its own budget with full operashytiona pOlo1ers It should have the authority to appoint its own staff and regulLte their conditions of service If it is constitutionally possible the Couner1 shollld be outside the jurisdiction of the Public Service Commission in pesornel matters
407 As an instrument of Government the Council should be subject to such ~eUfral or specific directives that the Ministry of Health may issue to it frcffi ime to time This should be written into the statute under which the Cmntil is set UD
408 The composition of the Council ould depend on the functions assig1ed to it It is suggested that the Council should not concern itself wl th the delivery of cliric selVices in the field The Ministry of Health may (ont nue to administer rampmily planning services at Government hospitals health cmters and health offices and the voluntary agencies should run thei] OWl ~rogram The following functions may be handled by the Council
- to shy
s rrogram plannin and target-setting
b proram monitoring and evalllation
c wiL of d 1ci(JTIdnCf by inspections
d Qrg8lizatim 0 es and marketing of contraceptive J~1J-s BLl (iV es at subs idi zed rates through es tablished 1 2 d(~ channel
e information mass media communication and audiovisual ublicity in the field
f prorrotion of famil~r plannIng acceptance through face-to-face cotlmunication by poundi eld workers in domiciliary visi ts
g trIining of personnel
II pr )motion of -esearch enJ
i financial support to voluntary agencies providing family planning services
409 n Statutory CCii1cil may corsi5t or an eminent non-official vith a comri tm ~~1t towacds foJlily plailninf nd the fol1owin~ members
I ~ bull Pfrmanent Secretary ltl-tIlH
Chief Hedical Officer HOH
i Principal ~ecHcal Office ~mH
d Pilhlic RellltionB OfJte(middotmiddot Prtm~ Ministere Office
A represen ta ti V~1 of the Ministry of Education
f ~ representative of the Ministry of Finance
g A representa~ive of the FPA
h A representative ot the C1AC
i H social scientist fcum tle University of the ~Jest Indies
j Three non-officials with experience in management and administration and the
k Director of the Family Planning Program - Secretary
- 11 shy
The COUlcil ITIltW constitute cOlClmittees for Finance - Accounts Personnel and Sup lies nd Stores ir~whi ch )nly members may be included Other commitles sc1h as those 01 training info1nation and education and researCl ara ~valuation r1ili also include experts from outside
410 he Off1ce raquo) cc im Panning Program which at present forms part of th ~Hnis try or [i n should be placed under the Council and its staff strelgtl ilcn~ii2 i~ r181 it may cease to depend upon the services of the Mir is t y of H~alth
C Office of the Family Planning Program
4 11ollwther the Offic~ of the Family Planning Program remains a part of the Mirisry of Health or is transferred under a statutory council if one is set uP i needs to be strengthened to meet the requirements of an expAndshying pr )gn m At present the following sys terns need to be ins ti tuted in this Office
a a 3ystem of setting annual targets for the enrollment of acceptors and the projection of service fadli ties in relation to these targets
I Ci ~ystem oE V)glC loHitoring (the monthly statistics flowing from the clini~s c~iiiain unproc(~s5erl for months)
a system of program evaluation eg demographic effect of tte program cost studies
1 an overall design for media communication based on a study of the reach a~d cost effectiveness of different media and the effect of the meflBsge content and
e a m88t~r plan for training which would comprise an assessment of the training needK of the existing staff and future reshycruits and a long-term plan divided into annual programs
412 Th2 Prograll afiie s~lould have the services of a demographer and a meeia expert A training adviser is expected to be provided by the PARO
413 1be Program Office should evolve schedules of field tours to overliee field operatio1s E~1eh health cente heal th office should be visi ted peridicaLy by the Milt~dical fElce- the Nursing Officer and the Health EduCltoI who should guide and assis t the local staff in carrying out the progam Their tour notes should go into separate dossiers for each institushytion and ~ach dossier should have basic demographic data about the area coveled by each institution These dossiers would be a useful record for revilwing l)errOmance The staff of the Program Office should be augmented to Ol)erte this control procedure
- 12 shy
D Decentralization of Powers
414 ~hete is a concentration of administrative and financial powers in the 11in s try of Health I-JllJCi1 results in an accumulation of references in the Miristl) and delays n field operations Specific powers should be delegated ~o (a) the PliO concerned with MCH and family planningmiddot (b) the Directcr o the Program Office (c) the Regional Director and (d) the County Medica1 Oficecs The Ministry should invite suggestions from these officers and wOlk 01t a schedule of delegated powers
415 A tdgh priority in the matter of delegation of powers is to arm the Regiond Directors with sufficient administrative and financial authority to implement with expedition the health and family planning programs of the Ministmiddoty 1 thin the areas in their jurisdictions
E Integration of Family Planning wi th Haternal and Child Health Services
416 At present family planning services are being provided at 48 Goverrnent hospitals health centers and health offices by using the full shytime E taf cf these institutions and employing part-time (sessional) doctors nurse~ anI clerks where necessary At 29 of these institutions separate famil cl~nics are held on specified days in the weck some being doctor sessi(ms mel others supply sessions run hy nurses and clerks At the remaining 18 imtit1tions family planning services are combined with antenatal child healtL cr postnatal services The Family Planning Association runs 8 unishypurpoe f am ly planning centers which provide daily services and contribute a 11 t le less than half the total number of new acceptors per year
417 N assessment has b~en marie of the effect of integrated MOl and famil~ p~ nnning services an the recrl1i tment of acceptors nor were ~ data readily avallable for this purpose It may be observed however that in a situation of shortages of trained personnel for health services utilization of the existing health staff and facilitieR for family planning is inevitable parU cllLrl y in the interior where such shortages are more pronounced This underlines the need of evaluation of the integrated xai and family planning progtam for its impact on the number of acceptors Also a study needs to be made of che utilization of medical and pilramedical manpower so that it leads to bdter ~llocation of duties and optimUJl utilization of personnel
418 ile integration of faMily planning into Mcn services has certain advalltages as well as attendant risks The advantages are
a Lbe association of family planning with the care of mothers and children helps project a benevolent image of family planning as a program of family welfare This creates a
- 13 shy
1imate favorab~e to the acceptance of family planning aa lt p-)si tL1e il-Eare rreasure rather than a negative program cE limiting c~ildren
h t elps erlist ~r2tion tf doctars and nurses who as c -~ass enjo tft~ Y)er)et~ a~d confidf~nce of the communities i712~ Eerve
c ~ieD of contact with women
d luni-purposa clhlics for ~lCH and family planning services are onenient for motn~rs who would have to travel considerable (listances to the clinics
e hete is better utilizat1on of Acarce heAlth manpower
419 he limitatio$ of integrating family planning with MCH servicesI
are the posiOili ties of loss of focus on family planning as a high priori ty prograrr ald the diffusion of pol1sibility for its implementation These could tlow ve r he safegurded agaifls t by adopting the following measures
a 11e job descriptions of doctors and nurses should be rewritten 0 include the family planning function
b hE perf0rt1iai1ce of ctoltors and nurses should be judged as much )y tbeir inteceq t in planning ~vork as in maternal and ~hjld care and this should he lade known to them
c )octors and nurses involved in ~CH services should be given middot)rj entation and traIning in famj ly planning and their interest 3UEtained by refresher courses seminars meetings and supplies of literature
d Thl techrical (xpert~ in the Office of the Family Planninl Program should maintain liaison with and guide the field agencies in implementing the family plannin~ program For this purpose schedules shoul d be marle out for periodic field inspections
420 It is suggested that the working of half-a-dozen centers where family plbnnLng services have been integrated wi th MCH sessions should be studiei for ehe purpose of standardizing the methodology of delivery of servicl~ Such a study should include staff strength patient load recoril shykeepills 10middot of patents in the clinic timing and frequency of clinic sesaios ani convenience vf patients
F Voluntary Organizations
421 I i~ internrticri31 expedence that the birth control movement is pion aTC tt volunh[~ JilC S Qltl that hen the national governments step in wi tl cmbi ti 019 prjhns wi thin the sLate welfare system voluntary bodies ieh tteir limited ilsrluces restrict their service activities and shift the emplasi i 0 educedgt (f the community training research and contracepshytive Sf vic not 1l7gtilflblr in he official program or in areas not reached by it In nagni tude and expanse the of ficial program in Trinidad and Tobago has alrad~ orertak~n Ce 101umary program Increasingly it will become the domLnart tartner in the total national program while the voluntary agencies will cOltirlU1~ to receive financial support and encouragement to set up high standaeis If service and explore new areas thus acting as a stimulus and an additi_e tl the official program
G FrOB-ram Infomation
422 Thre is no concurrent evaluation or monitoring of the Program The daa or lq72 flowing in from the clinics month by month have r8Jllsined unprocss~d tn the Program Office The official Annual Report - 1971 Sums up th~ poition as fcllo~s
ITThe Research and Evaluation component continued to be the weakest in the Population Program Although a systen of evaluation had been built into the program the follow-up procedures for analyzing the data and for correcting inshyconsistencies are inadequate Requests were made to extend the staff to establish a more viable unit but by the end of the year no chllnges had been made
423 T1e recording and riporting jJrocedures were revised effective Januery 1972 and there has been a further change recently at the instance of t1e Evaluation Adviser Under the system now established the clinics are lequ Lreurod to maintain the following records
a Family Planning Clinic Case Card - New Cases This was introduced on January 1 1972 and has thirty-one entries giving age parity contraceptive listory pregnancies socio-economic background ource of family planning information and agency for notvat ion bull (Annex 2) The case card is made out in duplicate for each new acceptor and a copy sent to the Program Office
b Daily Regis ter This fs a ne~gt1 form recently introduced in replacement of the old regis ter and is preparen
- 15 shy
ie) ruplicate the original to be transmitted to the Program (fHce and the carbon copy to be retained in the clinic Th~ is a very 121zborute form requiring 36 entries to be aa~ for each Chse nel and old attending a session includin~ (ntries to cit L to contTaceptive supplies issued
AijCleX 3 T~13e fcnnG are required to be sent to the Program lffce in i7JO balches every month the first batch for the i IS fif~eeL days and the second for the remaining part of hE month The trtention is that the data appearing in the ~EZlic daily legis ter forms should be compiled in the Program Office and fed back to the clinics Although it is claimed that this new form has been pretested and is workable ex)erience alone will show whether the majority of clinic cL~rks are able to cope with it in a busy session
bull o now-Ho Card TIlis card is intended to keep track of ac ceptor--It has entries for name addresfI and month fcr which a visit is due for each year
bull Aphabe tical Index This is a card index of clients with aidresses
Each i)at en is given a simple clinic card on which the dates of further appo~utnli rc3 an~ indicated A special fonT[ has been devised for the reporting ot cases unler the Post-IartumPost-Abortal Education and Referral Program
424 J system of monitoring progrRm performance from month to month need to bE develQped as a high priori ty The problem is not so much reshycord ng mc transmission of data by the clinics but its aggregation and proclssi ng in the Program Office every month which at present takes a long time The Statistical Officer should have a statistical assistant to help him Ln I he taflk Monthly progress reports should be available to the Mini H t~ n H(llllth and A11 offt eerlil of the ProKrnm Office so that remedial ac tl m I lAY h(~ tuk~n n rll1u- WhOnh1f ~Hfl(AlJtlaTY
42 For the analysis of data and evaluation the Program office shouln haVE th(~ full-time services of a trained demographer
H Field Workers
42) Tie Program nemiddotis tne services of a cadre of field workers to enr)ll neii aceeptoTs follow up acceptors in their homes and revive the int 2remiddott of dropouts Such a category of workers could also be utilizerl for pr1fficting other health programs such as the VD campaign and the inmuni~ation program
47 As an experimental measure one field ~]orker may be assigned to a emi l~ of Hi 000 population This would mean 100 field workers in all
- 16 shy
Earh of the workers should preferably have harl a higher secondary education otherwLe 1gt junior secondalY education They should be married persons with middoti1ltt mot tl-an two or tlree children recruited from the locali ty in which they armiddot~ requlred to function Only persons who have the capaci ty to comnunl at~ and or6anl~e should c chosen A months ini tial orientation
slcu1d enable them to start functioning in the field though reshyfresher CO rSeS tvould be necesslt1ry in due course In Port-of-Spain married mer~ a1C women may be employed on a part-time basis
I Hanagement Study
428 A nanagement study of the Family Planning Program should include a sctu iny of the top m~nagement Atructure (Population Council - Office of the Fanil) PLanning Program - Principal Medical Officer for MCH and Family Planni Ig fetices) the field structure for the delivery of family planning servics (Re0ional Director - District Health Services) including the utilizlti(n if medical and paramedical personnel for adding the function of del ve y )f family planning services and the control and communication proCed1reF Lfnking the top management with the field structure
429 The management consultants may study the functioning of the Popul tio I Council and advise whether it adequately serves the purpose of givini po Licy direction to the Program and if not what changes in its compo itt m and operating procedures may be introduced without altering its bsic craracter as an advisory agency The consultants may suggest an alern at ve form of organizati)n and utilization of personnel which in thir p nion may be better adapted to the needs of the Program
430 Irrespective of whether the Population Council is maintained or it is replaced by an agency of a different character a formation like the Offic of be Family Planning Program would be necessary for the administrashytion i)f 1 he program a task for which i 1 appears inadequately equipped at preselt Its obvious requirements are in the areas of program monitoring and el7alnation program supervision communication and training The manag ememiddotlt consultants may study the structure and procedures of this form~ tio Gnd make suggestions with regard to the augmentation of professional and ~ upp)rt lng staffgt and modification of operating procedures
431 The linkage of the Office of the Family Planning Program with the Miniutry of Health (Central Office) and the District Health Services should be sudied In view of the policy of the Government to integrate MCH and faI11iLy rlallning services it should be examined whether the Principal Medi al Officer for Communi ty Heal th Services (MCH and Family Planning) should be agtpoj nt~d as the Chief of the Office of the Family Planning Program and an adTlilistrative officer of a suitable level inducted in that Office to assist him TIle implication of this suggestion is that the head of the Family PlanJling Program would control the District Health Services
- 17 shy
432 rf 1e management consultants should examine the delegation of adminshyistratiie Bld financial powers of the Ministry of Health to different levels of Progam aclrlirdstration viz bull PMO Program Office Regional Director and County ~djca~ Officers
l33 he system of 01 af Togram information from the clinlcs to the Pr()~ra1 O~fice and tOile processing and use of information in the latter office iholld )e studied
434 he working procedures at the integrated McP and family planning clinics shnuLl be studied This would involve a study of each stage which a clien tpcticmt has to go through from the point of entry to the point of exit after receiving advice service or supplies This study shoulci lead to star dartization of procedures and functions and evolution of -lork norms CognatE st tdies of the working procedures at uni-purpose family planning clinics and su~ply SEssions should also be undertaken An essential component of these ~ tad ~es would be to examine Nhich functions currently performed by docshytors lealh visitors nurses and midives respectively hav~ become so roushytinize ttl it they can he relegated (0 the next 10Her level
435 Reated to working procedures is the problem of job description of medcal 8nd parrunedical personnel involved in family planning from the centra i tc the field level This job description needs to be studied wi th a vie VIW8Id txaminiDg the uttlization of skills and allocation of time by the staff lcc(rd~ng to the functional prj ori ties
436 frV management consultants should study the workings of the curren slralgements fOJ family planning counselling under the Post-Partul11 Post-Abortal Education and Referral Program at the Port-of-Spain and San Fenaldo General Hospitals
437 SU1ect to the ItBrcement of the Gove1nment the management conshy8ultal ts ~hOLlld undertake a study of th requirement of field workers (home vinitcru) in tmtlUI of are nnd population cov(ra~e
ANNEX 1
Names of Persons Met
Ii Mr T C Taitt Pem1(H~nt 3~crtarY) Ministry of Health
2 Dr M n Henry Chitd Medical Officer Ministry of Health
Ellubeth Quam a Prindpal Medical Officer (1S)
4 Mr G Z Jaine ~ uJiector Population Council
5 Dr Norma Andrews Medical Officer Population Council
6 Mr Jc~n Coury~ Evaluation Adviser Population Council
7 Mr A Jriseph Principal Statistical Officer Population Council
8 Dr C 0 Colman Country Representative Pan American Health )rg ni~ation
9 Mr ranca Kippel Health Education Specialist Ministry of Iea th
10 (1 bullbullines Principal Nursing Officer Ministry of Health
11 Dr Mx won (formerlyHinistry of Health)
12 M3 late Carops Ex-Chairman of Population Council
--
4i 1_ middotIIlt F-ntCWclOotf_Y v OJ t tl
GOVIIlHMEIgt(I OF TINIOAD AND TOampAGQ - NNISTJY OF HIALftf AIJIE1 2NATIONAL FAMilY PLANNING PROGRAMME
F MIL Y PLANNING CUNIC CASE CARD - NEW CASES - NFPPl
li ~~___ 1 ________
~ ecll-U
-- --------------------- shy~) ~~middot~------------------~~~~~~---CIJ------ middot~ii--middot-middot----middot-middot---middot--------- shy
ltv Writt N_ 01(111________________
a ~4itiJtmiddotl_____ ilIIIltIoI~____~____~-__----- shybull ~4
fie l$ - JO tDql IIfIA- tr-JMimiddot _ iJ 1 Odoor o
14aorielaquol_ _~ 0 lio witIleo-La ~ 01 bull - OJ ( _01 1~ltgt1lh o bull- 0$
AacJcu 0 2 CIIriIWA 0 J Os 0
Yv~MONTH ltnollOf~nfIGHTI
Undu 1100U$ Utgtdn 5SCI Undu 11200 01 ~ 50 - 9949 amp100 - 1199 02UlOO - nn9E~ (
0)~ 10- $99 SiOO -- U9~ lOO -- U99 12400 - 1359)-------_-r----shy ~l)o SIS n600 - Hm1300 -- 019 OJ200 il~9 ~------ 99~ a 1)0 m Os1)00 -- l99 1400 -shy $4100 -- 1S999r--- shy
1500 donl S6000aad O399 - lt499I~- I 0lt
ltII
IJ -IC _~tltlioltgti lS
02 IaampJIIocI OJ 04 laM Os
w Oltwio I_-l(~u IrIaa U
h~~ ~Clubl 01 OJ
IS ~C-n 01 toSIitDI 02
Ji poundI on 01 IriIIIuy M ur 02 IV OJ
WU 10 pltIoII~ llaMtl 411 cIIiId 01 Ol it fIolto ~ do~ _14 rou IIlgtJo 1Ia1 ___~_ shy
40
It _ I 00 ~bull FPIiIJ 1
OJ 02 OJ 06
)0 III- iy wOWcf ~1
aMIIl Os
11 T 1gtlt ( h _______ 4)~
06
04 (MIbullbull middot bIrlI ~___~__~_ (-fIJI ~- -~-- (1HJ 49middot SJ
U 10k 01( 1__ raquo$-4
iU1) DOl F ToWotfOlnC DOl 001 or Do [IP 006 001 OIIgtu___Spltclty DOll Nltmo 010
U1Mo I orcpmiddot laquo55middot16
1lD 001 Foam Toblelf_ICim DOl Condom DOl CoomS~ 004 oe Oos WlttuJn 1J OIkr DSpody) 101~ ~Iu 006 Rhylhm 001 DOG OJO
no wI~lmm 4 cd
(I 0) 1110 01 Condor 03 (lorn bull l S~muoidIl 04 Faa TabioolfIIltr- Os RhyUlm 01 lnJrl tible O Advico 090 06
la slt 1)0 19 loti ~rltnlt) ([)sl or 1llOn) ____ --__ bullbully-J n SV - ~JcdS
v~ Cl NCI 0 30 OJI_O I Wr blJ1h 0 I ~ OJ 1 ~ (fOOd V 01 No 02 laquo 6) Cf4
WIiI 1 172
004 001
j D middotmiddot middot
1 ~
r
~
bull I
bullI I I
r c i
ANNEX 3 Pagemiddot 1 of 5
0 raquo rshy -lt l)J ~ 111 t G) 5 shy (J) ~ -
fT1u
i
MINISTTY OF Ho1TH
NTIONl F~ILY LNNING PR-GRbullbullM-tE
~~5tructions to C11nic ClerKa
How to co~ploto the Daily Rogister
~~ ~~v1sd Daily Rosi8ter replnc~D tho one which is now in use tb$ Monthly PC~ri rOt~ arti tho 01( Ci() Dod PollJ j f m It is a pre-coded form and 1411 cl~1p Jd tl a1I6iniul-mIHvn Oel Clinic nctivi~y
110 )rm rollt biJ coupJot)d lrl cupLtcoto using a o(roon shoot Tho top aheot or oriinai ~ust bl) 6(Ult to tho CQgt1tral O[[lCO and tho carbon copy retained in the Gliaic rilo dll the for6a that ar uD~d betwoen the 1st 4nd the 15th of the oIIollth aut bo subClittud tocho office 35 Lnc blttch Those oomp1cted betwoon tho 16th _lid tqemc of tho month must bo ~cnt in a secJnll batch
P lOvLior hns boon Illllde for 25 clients on cZlch forlll new forlll must b IIlied f r poundh 50[810n2 whothur or not ono or lIIore session are hoIdiit the clinic on he sarne day
I th ro alO more htl 25 clionta 1n attondnnco at tho session the additi shyOhAl m~bOl of clionts 10 clients nu~ber 26 27 etc sh0u1l be ontered on the next Imiddotrlll ~i ttout a1tpoundring the numbtlrs in the cvlumn hond Series
51 ppOfil th~ number of aUcnts lQr that session ws 5 this would mean thllt two rJlS ~ lst be 6ubllIitt~dl the first filled uF 1 tltgt 25 And the laquoIncond 1 to 10 Th~ cal bon ofies should bo st~plod togother at thu t0P l~rt h4nd corner of the torm ard ktpt in the Clinic filo lou IIlU6t stapl~ the originftls in the 8~~ monnshyer for lIub~ssion to the ofticl
ie h~ ll idontiflctior- (cc 1 - )
0 lot Ji 9 anythin~ hGro poundhia is int(mdClc for tha computer code
2 ~~pound~ - Print clOflrly tho name of your Clinic
C1Lic Huml or - (cc 4 - 8) Evar1 Clinic Numbor has 5 digits Virite each dig t il a t$purate box
It Pai~_thllsectgdllion (00 lt) -1 1) - Dl monll 10M
lw) bolte IlrO proY140d fetr olAoh pr 01 thQ dISh Enter tho dA) ldns a R
d16ih
emiddot5middot (0 11 I for 115t ( 0 21 for 5th etc Treat month the am pay
e ~ 10 ~ I for I-hrch 0 [2] for September Tho y~nr must be (into ad
I Z I ~ I I 71 q etc
Take as in IixulIple tho dOlte 3rd tllrch 1973 7~ie must bo written
[0131 LSLDI[7l3JDny Month Ye~r
5middot 1~J $~~ - Irom ~-------- To --------shytntol hOI II the time the Clinic 111118 in SW5sion emiddot8middot
(i) 11011 500 lm To 1200 non
(11) Frclt 100 pm To 400 pm
(iii ) IX-OG OO pllI To 6~00 pm
f
2
ADEJ ) Paae ) of S
6 Eov
_ 1hA 1gtIpoundC iIIUlt be nu~o7Ifd tler1ally 1 throurh n lU tbey Are Wled In ~1l8ellJ IInel 1301 tlU 1 Orcl 1 Wled tor a o5038ioll - -I 2 tonY tho _boul~ b I1WJbtl 1 and 2
hlrlll are 25 linos OIl the fOnl Ilnd thoae muet be UBtleS for 25 clients 9 one ior bullbull 01 I ini
ot ~h lc II ol1cM lOlivpound til e linic before soeinc DurOI or doc tor ilnc ii hox rristrltltion nUlJbet had alrearll been recorded on the Dai 1y Roiuter then n line ~hollld be drawn through that entry an1 the eliort nust not 06 includttd in tho totals tor that 0eDion
1lw Ileifitration Num)~r of cueh client must be IiIritten IS n 5-dlrlt oode ClhnC IH11IlElr 315 1IIU8 tborotore be enterod 18J010117]5]
~ Clt ZOt
Coda 1 Codo
10 ~tl c 2t j co 21)
~w elSe - Coda 1 0) d CltaEl - Code 2 Revislt Code 3
Only pound1 01 theBe coiles may be usod
11 prol-O~ ~Eil~1 (cc 22)
If ma climt was L drop-out IIho haoS returned now to the Clinio tor tho first no linmiddot bullwin lt1ro1eo o t he or she should be given CCe 1 It this do 5 II It nprlly leu this colWlln blank
u Hothod middothisllill loe 23)
NOh til t otly ~ Cod 16 tp he ontered in 2lpound of the columna oven thOUGh 10 co11lllJlB 10 provided on the torm The Codes llrol-
Oral Contraceptive Code 0 1 U D Code 1 Condom plUD Codo Z Condor (only) Code 3 Foum tAblets cream Code it DitphrClGJII Code 5 Rhythm Cde 6 Injectible Code 7 Advice Code 8 Other Code 9
It for middotDo-le 1 client rlllll ji yen cclldorls ord foam or creall Iou Qust entor Coole i (condom plulJ) in the appropri~te column This Quat be the only lIotmiddot) tarcie If an in the cnse of a tlnle clinic I the client is Bup)lieu lith COIlOrW only you rmot entEr CorlQ 3 (cpndolll) Do not use a ticII ~ tho (odo Nwber
It is CUi tomary fur 11 cliont 110 is beine put on the oral contraceptive for the first tiT1o and even on other occasionn be issued condoms and 11 crelle or foam a Ilell rI3 a pgtcket of pilla In such Cllses when the piDQ Ilre Ilctually iouou you tlust record Orll (Co~e 0) 08 tho onll metbod ilo othor ntry sll0uld ho nnrlo
Uovever n SJC~ canas vucru condoms and fOHa ~rc eiven but no pilJa (even thoJRh _t _n the intention to issue pills nt the noxt vioit) than the Mothol Th5 ifli t ohoulcl be recorded uo Condor Plus (Code 2)
13 Seen Bybullbullbullbullbull
~rot S-1 SO l
Doctor (Dr) - Code 1 j Nurse (Nul ) - Code 2
Clark (Olk-) - Code If tho Clhnt is vcen hy both tho llootor tlnd the Nurse enter Code 1 t Doctor It 6~61l by the Nurso only arite Code 2 Cod bullbull Cerk is l)llnt for FA Cllnica Clerks in tho Government Cli1t hiwo Llttoll istructed not to i56uo supplios on their own volition
14 fl221~
lhio S~tiCl of -Ie fvrtl t~ke 16 (llrci coluMna (cc 25-+0) nnd 10 tho only part at th iOIQ in llich iore thAn one cod is Zlccoptl1blo Tho purpoco of the )ecton is to 0 able to arrive nt the Cjunntity of 6tock dilltlitJutshyed YOI IIlUdt writo in the CllllOjH-iata colulna the nUllbJr of Il1ch 4rtic1o i~JSu~d ~lo e ha I Oral Contrcilpti vea are aub-di vi dod into types ae_ 3 PIllCKC 9 0 Elynnn LlUot be entered Codo in card column 25
If tor eXllrplc t l cliunt is iosued wi th packots of Zucynon nnd aJ(1 ~ivn 1 conuotll (8inoloo) you ouot enter in oard column 25 and 11 It
cnrd col~8 )2 and J (io 1 in card colucn 2 nnd 2 1n card coluun 33) Nota C)lldoIlU ale to b(t ruoordod individually not os packots of throo) Should n ne LlondoClo be isoued thil3 is to be rc-Qed as 09
If It clint 6 t~ot isoued Blly lIupplies thon you must writo Codo 1 in CQllAlilD 41
It Q eli nt isite the clinic to check on her LUD or her Diaphra~t IUId ro DI W 6 ppl ills nre ispounducd then Code 1 1s wri t ten in column 40
In the FA clinios here a variety ot orll contraceptiveo in orer~l tho elerll wilmiddot~ bJ provided with a specill code shoot The idontifyin coo will b wiittn in Column 29 nnd the nUlber of packets iosued in colwm )0
lralaer-In Code 1 lrllllsie r~ut Coda 2 leIllPQrArr Trnnsfer-In Codo gt
In the cao of n 2ratl8fcr-In I you lUot n160 cOrlpleto coluons 42-51
In the cllU J of A ~~emporary TranGfor-1n (an individual who i8 only v1citing fur clinic tor some epecial trcatcont hna who will bo rdnlnin
~middot(II~~~fO~l~SIl~I3~nn~~~h~rO~nh~1~~190~~nll 2-46 and ler rei IItrntion numbu in colullnll41-51
It the oli( nt i iNt a CrllnoforwIu - Out or loClporu1 tMn loave oolumn 1 blank
16 lr4nst(gtr-tl2~~morrry TilJnder-In (co 42-51) Forl1ltl CUn E1~ (cc 112-46)
hen you rei iatlr L irllsfcrln or Il TJlporary Trnnsfer-In you IIIUBt write I ere the five-digit clinio nucbor of the Clinic iraQ which tho ltlient Me (uIlO
2mer ]letr ~2n ~ (cc 47-51)
frlta fllao Clo r-~itrlltion Nuc~Er ot the client in the Former Clinic (i c bullbull th 1 Sis rnmiddotion ~UlIlh()r which the client carrics 1n the tormor clinio) bull
It tho Forrltl Ho( ist rntion Number iIJ not readily wnilnble you tluct oocpluto thtl epcciol [orlll Transfer-In Not Identifiod Dy Forrlcr RCGi(trn~ t10n Nwlbvr Or ~ flt)rCl is to be cOlplctcd for och cnso nnd th forlJO Ilubmi tted to thu )opllntion Prorrnnme Of fice tOGether with tho Dily Ro~iBtors lhwev~r should the clork leuTI of tho clint B FormlI Uocintra tion lUlllb r )0[(10 Cubmi ttinft the D1ily IOCI otro t hen the nUQbcr shoulo bo -ri ton in colucns 47-51 lna the special foro should lJo deotroyotl
l7 bullbullbullbullbull
r lt bull bull
ADXI ) Pap S ot S
11 UD LV~ (cc 525)
It tb( cliont io ~ivQn An IUD tor the firot tl~o then you should Sri to Codo 1 Inuort ill colurJI 52
It tho olimiddotsnt ia rvinGgtrtltld i th An I UD bullbull tben wse Coda 2 RelnDltlrt shyin (01Uil11 52
It the clLmt is ~tte~~dint chnic beruse her IUD CflClQ out by Haol (cxpll Iion i ~hcn fir te todo ~- UIlllrli1 53~
If c-ltr IU fj IIIS reov in -ne cllnic by tho doctor or nurso t~on vlritI Codec in column 5
II the eli nt otends eiLlie tld explin[l th(lt she rccovcd the IUD tlllleel nen write Coda H in Colwlm 53
It the IUD jr still within the uterus nd the WOIraquoI1 1 11rc6llJlnt thon lIrite 1gt40 4 in Column 53
lZ np h5t (ce 54) It 0 Pull 5mor ie t~ken durin thi visit tben Codo 1 ehould be ampDtere4 in ColWlln 54 Should he c110nt lltt rQ(uircd to rttturn to clin1c for a rogtol1t Pnl) t06t then CoLe 2 llhould bo middotwrittcn in column 54
It no Pllp Scou io taken tde visit Itove colUQn 54 blank
Iraferti1lli (CQ 55)
Ii the e liett io nl1 infortili tr eaoe use Cor1o Ill in colUQn 55
If tbia 1000 not tlpl lonve column 55 blonk
20 Totaltll
CO~1ploete the [)ldegO 1gty puti YI tne totals betweon the double lines nt tu b()ttctl Carrj colUlllnc 20 21 nd gt4 Must hlve tho Bnoe JllIIber and thiG Would coreslonc to the numocr ir attencbnco
Writ$ th to1ul nUlllior of Drop-Outs returned (c022)
Urito 41eo tb totnls fOJ each card column 0 to 9 under tho h(adinu Method thiB Vioit Show tho tote L fgtr OlCl type of contraceptive issued (cc 25-40)
1)0 Dot wrLte 1111 totll lUl(Ier Card Columns 15-19 29 41-51
21 COPmllh bull ~lt h~t~ Monthly ROilort
OQ thG DaLl oCator forlll thnt ccrrOspOldB to tho 1(8t 1$06610n lt 0
oth yo Olllt (vwlgtleto the items nt the botto of the [orampl This is tour ontll~1 n(olt nnd includcD tho totll lumber of sesions Ilntl tho total Iluolcr ( r crop-outs durinr the Qonth
An tiUlsilt n drir which n doctor liB in nttcndnncc is a doctor sOfll~1on and shoulc 00 re(liGtcnd in coltns 56-57 All other sessions 1116 conlliid~recl supply stllciona and thtlY 1110 rocordod in columns 58-59
the total Ilum)nl Jf drop-outo ld the drop-outs by method durinc the onth nre 10 bu oltorou in the inrlicllted boxes
72 Chad Your ~
Milke I ura th t all thE fijul4gtu rre c101r -tNever writo our nutlUQrS 50 InrjEl that they oxtend out of tho
ap~rotr1ato ~ox
Cheek to BoJa tht 1111 numuors 1110 in tho correct boxes -- CJslHloially when Writi1 the totlB
Mllxe Cirtc O thmiddott t1e infoT1I1ntion i6 clear on the corbon COllY before sep rmiddotinr the sheets
Jitn the Fomiddotl lien tly sien YOUl nr me 1t the bot tOil right hnnd corner btl forc subol ttinG it Keep tle CL rb n copy for your rocordn
i
-l ________~~---------~
I _1
Adminiatr-atlve SKVieu
P inba ~~~l1cal lrlnbin~~eltltcal -1 te~ra t~~rvicc (lnatittloaa)
--1- - shy -1------------_-L_ l-r-aJiil- shy _-L_tet1lal d
PlIinm1tJ8 atdUon DetalMid H8Il1tb ~ ________bull Care
-----~ Office of i
the FlIily _IPlill3 roarshy
1- - - -------RegiatUll urnr
ltIi 1 Drelttor Rcgicaat Director Souta Tabqo tacallortb ~ counu gt____ ~ (4 ouottet)
Off1ce of the Res10nal Diractoc L
r----- _L_ -- shy i I bull IREgional Ipitl I
District IIttaltb I bull Othn RelOl ond Hcpital CenteIntt itlt j In 1__ _shy-~- ---- -_j
J r Ii~lth
C~nlef
L
I Ihnlth lie I th Offlcu (1ft lc~
Coullty 1I0p1ta1
Henlth tentet
I

- 9 -
Permane It Secetary and the P1O (fen and FP) should be brought into the Council he inclusion of the Permenent Secretary would open a channel of communi~aton with the MOR ae the highest policy level next to the Minister and would (ontribute administrative expertise to the deliberations of the Cou1ci1 ~m f icili tali 5 (pleuenrti)D of th~ recommendations of the Council within the -rni and in OUltL depa-cments The inclusions of the PMO (MCH and FP) wOlld el) emphasi ~2 hs responsibi lity toward the family planninR program Some officrs of the HOH (eg Chief Health Educator Principal Nursin~ Office e) may 111 ea~e to be members though they may attend as requirE d nmiddot the agenda before the Council A representative of the Ministry of Fin nee stQuId be inc~uded in the Population Council This would make for a lettr appreciation of the needs of the Program in that Ministry and fadIi ate fj nancial sanct ions
B A~tatutory Council
40S In the foregotng Pgraphs the view has been expressed that within th edsting policy framework an advisory Population Council would be more tli)prcpriate than a COlincil wi th executive functions and powers that an advisory rOUlcil would not gain by having a statutory status and that if a statl1tory body 5s to be set up in lieu of the existing Council it would need tC b structured more Iiice a Board of Management than a council wi th a repre13entttional charact~( n the latter event the statutory council should have fu 1- time Executive Chairman or failing that an Executive Director functj oni1g undel- a Chairman trno can devote considerable time to the business of tlw COlncil
406 T1e Statutory Council should have its own budget with full operashytiona pOlo1ers It should have the authority to appoint its own staff and regulLte their conditions of service If it is constitutionally possible the Couner1 shollld be outside the jurisdiction of the Public Service Commission in pesornel matters
407 As an instrument of Government the Council should be subject to such ~eUfral or specific directives that the Ministry of Health may issue to it frcffi ime to time This should be written into the statute under which the Cmntil is set UD
408 The composition of the Council ould depend on the functions assig1ed to it It is suggested that the Council should not concern itself wl th the delivery of cliric selVices in the field The Ministry of Health may (ont nue to administer rampmily planning services at Government hospitals health cmters and health offices and the voluntary agencies should run thei] OWl ~rogram The following functions may be handled by the Council
- to shy
s rrogram plannin and target-setting
b proram monitoring and evalllation
c wiL of d 1ci(JTIdnCf by inspections
d Qrg8lizatim 0 es and marketing of contraceptive J~1J-s BLl (iV es at subs idi zed rates through es tablished 1 2 d(~ channel
e information mass media communication and audiovisual ublicity in the field
f prorrotion of famil~r plannIng acceptance through face-to-face cotlmunication by poundi eld workers in domiciliary visi ts
g trIining of personnel
II pr )motion of -esearch enJ
i financial support to voluntary agencies providing family planning services
409 n Statutory CCii1cil may corsi5t or an eminent non-official vith a comri tm ~~1t towacds foJlily plailninf nd the fol1owin~ members
I ~ bull Pfrmanent Secretary ltl-tIlH
Chief Hedical Officer HOH
i Principal ~ecHcal Office ~mH
d Pilhlic RellltionB OfJte(middotmiddot Prtm~ Ministere Office
A represen ta ti V~1 of the Ministry of Education
f ~ representative of the Ministry of Finance
g A representa~ive of the FPA
h A representative ot the C1AC
i H social scientist fcum tle University of the ~Jest Indies
j Three non-officials with experience in management and administration and the
k Director of the Family Planning Program - Secretary
- 11 shy
The COUlcil ITIltW constitute cOlClmittees for Finance - Accounts Personnel and Sup lies nd Stores ir~whi ch )nly members may be included Other commitles sc1h as those 01 training info1nation and education and researCl ara ~valuation r1ili also include experts from outside
410 he Off1ce raquo) cc im Panning Program which at present forms part of th ~Hnis try or [i n should be placed under the Council and its staff strelgtl ilcn~ii2 i~ r181 it may cease to depend upon the services of the Mir is t y of H~alth
C Office of the Family Planning Program
4 11ollwther the Offic~ of the Family Planning Program remains a part of the Mirisry of Health or is transferred under a statutory council if one is set uP i needs to be strengthened to meet the requirements of an expAndshying pr )gn m At present the following sys terns need to be ins ti tuted in this Office
a a 3ystem of setting annual targets for the enrollment of acceptors and the projection of service fadli ties in relation to these targets
I Ci ~ystem oE V)glC loHitoring (the monthly statistics flowing from the clini~s c~iiiain unproc(~s5erl for months)
a system of program evaluation eg demographic effect of tte program cost studies
1 an overall design for media communication based on a study of the reach a~d cost effectiveness of different media and the effect of the meflBsge content and
e a m88t~r plan for training which would comprise an assessment of the training needK of the existing staff and future reshycruits and a long-term plan divided into annual programs
412 Th2 Prograll afiie s~lould have the services of a demographer and a meeia expert A training adviser is expected to be provided by the PARO
413 1be Program Office should evolve schedules of field tours to overliee field operatio1s E~1eh health cente heal th office should be visi ted peridicaLy by the Milt~dical fElce- the Nursing Officer and the Health EduCltoI who should guide and assis t the local staff in carrying out the progam Their tour notes should go into separate dossiers for each institushytion and ~ach dossier should have basic demographic data about the area coveled by each institution These dossiers would be a useful record for revilwing l)errOmance The staff of the Program Office should be augmented to Ol)erte this control procedure
- 12 shy
D Decentralization of Powers
414 ~hete is a concentration of administrative and financial powers in the 11in s try of Health I-JllJCi1 results in an accumulation of references in the Miristl) and delays n field operations Specific powers should be delegated ~o (a) the PliO concerned with MCH and family planningmiddot (b) the Directcr o the Program Office (c) the Regional Director and (d) the County Medica1 Oficecs The Ministry should invite suggestions from these officers and wOlk 01t a schedule of delegated powers
415 A tdgh priority in the matter of delegation of powers is to arm the Regiond Directors with sufficient administrative and financial authority to implement with expedition the health and family planning programs of the Ministmiddoty 1 thin the areas in their jurisdictions
E Integration of Family Planning wi th Haternal and Child Health Services
416 At present family planning services are being provided at 48 Goverrnent hospitals health centers and health offices by using the full shytime E taf cf these institutions and employing part-time (sessional) doctors nurse~ anI clerks where necessary At 29 of these institutions separate famil cl~nics are held on specified days in the weck some being doctor sessi(ms mel others supply sessions run hy nurses and clerks At the remaining 18 imtit1tions family planning services are combined with antenatal child healtL cr postnatal services The Family Planning Association runs 8 unishypurpoe f am ly planning centers which provide daily services and contribute a 11 t le less than half the total number of new acceptors per year
417 N assessment has b~en marie of the effect of integrated MOl and famil~ p~ nnning services an the recrl1i tment of acceptors nor were ~ data readily avallable for this purpose It may be observed however that in a situation of shortages of trained personnel for health services utilization of the existing health staff and facilitieR for family planning is inevitable parU cllLrl y in the interior where such shortages are more pronounced This underlines the need of evaluation of the integrated xai and family planning progtam for its impact on the number of acceptors Also a study needs to be made of che utilization of medical and pilramedical manpower so that it leads to bdter ~llocation of duties and optimUJl utilization of personnel
418 ile integration of faMily planning into Mcn services has certain advalltages as well as attendant risks The advantages are
a Lbe association of family planning with the care of mothers and children helps project a benevolent image of family planning as a program of family welfare This creates a
- 13 shy
1imate favorab~e to the acceptance of family planning aa lt p-)si tL1e il-Eare rreasure rather than a negative program cE limiting c~ildren
h t elps erlist ~r2tion tf doctars and nurses who as c -~ass enjo tft~ Y)er)et~ a~d confidf~nce of the communities i712~ Eerve
c ~ieD of contact with women
d luni-purposa clhlics for ~lCH and family planning services are onenient for motn~rs who would have to travel considerable (listances to the clinics
e hete is better utilizat1on of Acarce heAlth manpower
419 he limitatio$ of integrating family planning with MCH servicesI
are the posiOili ties of loss of focus on family planning as a high priori ty prograrr ald the diffusion of pol1sibility for its implementation These could tlow ve r he safegurded agaifls t by adopting the following measures
a 11e job descriptions of doctors and nurses should be rewritten 0 include the family planning function
b hE perf0rt1iai1ce of ctoltors and nurses should be judged as much )y tbeir inteceq t in planning ~vork as in maternal and ~hjld care and this should he lade known to them
c )octors and nurses involved in ~CH services should be given middot)rj entation and traIning in famj ly planning and their interest 3UEtained by refresher courses seminars meetings and supplies of literature
d Thl techrical (xpert~ in the Office of the Family Planninl Program should maintain liaison with and guide the field agencies in implementing the family plannin~ program For this purpose schedules shoul d be marle out for periodic field inspections
420 It is suggested that the working of half-a-dozen centers where family plbnnLng services have been integrated wi th MCH sessions should be studiei for ehe purpose of standardizing the methodology of delivery of servicl~ Such a study should include staff strength patient load recoril shykeepills 10middot of patents in the clinic timing and frequency of clinic sesaios ani convenience vf patients
F Voluntary Organizations
421 I i~ internrticri31 expedence that the birth control movement is pion aTC tt volunh[~ JilC S Qltl that hen the national governments step in wi tl cmbi ti 019 prjhns wi thin the sLate welfare system voluntary bodies ieh tteir limited ilsrluces restrict their service activities and shift the emplasi i 0 educedgt (f the community training research and contracepshytive Sf vic not 1l7gtilflblr in he official program or in areas not reached by it In nagni tude and expanse the of ficial program in Trinidad and Tobago has alrad~ orertak~n Ce 101umary program Increasingly it will become the domLnart tartner in the total national program while the voluntary agencies will cOltirlU1~ to receive financial support and encouragement to set up high standaeis If service and explore new areas thus acting as a stimulus and an additi_e tl the official program
G FrOB-ram Infomation
422 Thre is no concurrent evaluation or monitoring of the Program The daa or lq72 flowing in from the clinics month by month have r8Jllsined unprocss~d tn the Program Office The official Annual Report - 1971 Sums up th~ poition as fcllo~s
ITThe Research and Evaluation component continued to be the weakest in the Population Program Although a systen of evaluation had been built into the program the follow-up procedures for analyzing the data and for correcting inshyconsistencies are inadequate Requests were made to extend the staff to establish a more viable unit but by the end of the year no chllnges had been made
423 T1e recording and riporting jJrocedures were revised effective Januery 1972 and there has been a further change recently at the instance of t1e Evaluation Adviser Under the system now established the clinics are lequ Lreurod to maintain the following records
a Family Planning Clinic Case Card - New Cases This was introduced on January 1 1972 and has thirty-one entries giving age parity contraceptive listory pregnancies socio-economic background ource of family planning information and agency for notvat ion bull (Annex 2) The case card is made out in duplicate for each new acceptor and a copy sent to the Program Office
b Daily Regis ter This fs a ne~gt1 form recently introduced in replacement of the old regis ter and is preparen
- 15 shy
ie) ruplicate the original to be transmitted to the Program (fHce and the carbon copy to be retained in the clinic Th~ is a very 121zborute form requiring 36 entries to be aa~ for each Chse nel and old attending a session includin~ (ntries to cit L to contTaceptive supplies issued
AijCleX 3 T~13e fcnnG are required to be sent to the Program lffce in i7JO balches every month the first batch for the i IS fif~eeL days and the second for the remaining part of hE month The trtention is that the data appearing in the ~EZlic daily legis ter forms should be compiled in the Program Office and fed back to the clinics Although it is claimed that this new form has been pretested and is workable ex)erience alone will show whether the majority of clinic cL~rks are able to cope with it in a busy session
bull o now-Ho Card TIlis card is intended to keep track of ac ceptor--It has entries for name addresfI and month fcr which a visit is due for each year
bull Aphabe tical Index This is a card index of clients with aidresses
Each i)at en is given a simple clinic card on which the dates of further appo~utnli rc3 an~ indicated A special fonT[ has been devised for the reporting ot cases unler the Post-IartumPost-Abortal Education and Referral Program
424 J system of monitoring progrRm performance from month to month need to bE develQped as a high priori ty The problem is not so much reshycord ng mc transmission of data by the clinics but its aggregation and proclssi ng in the Program Office every month which at present takes a long time The Statistical Officer should have a statistical assistant to help him Ln I he taflk Monthly progress reports should be available to the Mini H t~ n H(llllth and A11 offt eerlil of the ProKrnm Office so that remedial ac tl m I lAY h(~ tuk~n n rll1u- WhOnh1f ~Hfl(AlJtlaTY
42 For the analysis of data and evaluation the Program office shouln haVE th(~ full-time services of a trained demographer
H Field Workers
42) Tie Program nemiddotis tne services of a cadre of field workers to enr)ll neii aceeptoTs follow up acceptors in their homes and revive the int 2remiddott of dropouts Such a category of workers could also be utilizerl for pr1fficting other health programs such as the VD campaign and the inmuni~ation program
47 As an experimental measure one field ~]orker may be assigned to a emi l~ of Hi 000 population This would mean 100 field workers in all
- 16 shy
Earh of the workers should preferably have harl a higher secondary education otherwLe 1gt junior secondalY education They should be married persons with middoti1ltt mot tl-an two or tlree children recruited from the locali ty in which they armiddot~ requlred to function Only persons who have the capaci ty to comnunl at~ and or6anl~e should c chosen A months ini tial orientation
slcu1d enable them to start functioning in the field though reshyfresher CO rSeS tvould be necesslt1ry in due course In Port-of-Spain married mer~ a1C women may be employed on a part-time basis
I Hanagement Study
428 A nanagement study of the Family Planning Program should include a sctu iny of the top m~nagement Atructure (Population Council - Office of the Fanil) PLanning Program - Principal Medical Officer for MCH and Family Planni Ig fetices) the field structure for the delivery of family planning servics (Re0ional Director - District Health Services) including the utilizlti(n if medical and paramedical personnel for adding the function of del ve y )f family planning services and the control and communication proCed1reF Lfnking the top management with the field structure
429 The management consultants may study the functioning of the Popul tio I Council and advise whether it adequately serves the purpose of givini po Licy direction to the Program and if not what changes in its compo itt m and operating procedures may be introduced without altering its bsic craracter as an advisory agency The consultants may suggest an alern at ve form of organizati)n and utilization of personnel which in thir p nion may be better adapted to the needs of the Program
430 Irrespective of whether the Population Council is maintained or it is replaced by an agency of a different character a formation like the Offic of be Family Planning Program would be necessary for the administrashytion i)f 1 he program a task for which i 1 appears inadequately equipped at preselt Its obvious requirements are in the areas of program monitoring and el7alnation program supervision communication and training The manag ememiddotlt consultants may study the structure and procedures of this form~ tio Gnd make suggestions with regard to the augmentation of professional and ~ upp)rt lng staffgt and modification of operating procedures
431 The linkage of the Office of the Family Planning Program with the Miniutry of Health (Central Office) and the District Health Services should be sudied In view of the policy of the Government to integrate MCH and faI11iLy rlallning services it should be examined whether the Principal Medi al Officer for Communi ty Heal th Services (MCH and Family Planning) should be agtpoj nt~d as the Chief of the Office of the Family Planning Program and an adTlilistrative officer of a suitable level inducted in that Office to assist him TIle implication of this suggestion is that the head of the Family PlanJling Program would control the District Health Services
- 17 shy
432 rf 1e management consultants should examine the delegation of adminshyistratiie Bld financial powers of the Ministry of Health to different levels of Progam aclrlirdstration viz bull PMO Program Office Regional Director and County ~djca~ Officers
l33 he system of 01 af Togram information from the clinlcs to the Pr()~ra1 O~fice and tOile processing and use of information in the latter office iholld )e studied
434 he working procedures at the integrated McP and family planning clinics shnuLl be studied This would involve a study of each stage which a clien tpcticmt has to go through from the point of entry to the point of exit after receiving advice service or supplies This study shoulci lead to star dartization of procedures and functions and evolution of -lork norms CognatE st tdies of the working procedures at uni-purpose family planning clinics and su~ply SEssions should also be undertaken An essential component of these ~ tad ~es would be to examine Nhich functions currently performed by docshytors lealh visitors nurses and midives respectively hav~ become so roushytinize ttl it they can he relegated (0 the next 10Her level
435 Reated to working procedures is the problem of job description of medcal 8nd parrunedical personnel involved in family planning from the centra i tc the field level This job description needs to be studied wi th a vie VIW8Id txaminiDg the uttlization of skills and allocation of time by the staff lcc(rd~ng to the functional prj ori ties
436 frV management consultants should study the workings of the curren slralgements fOJ family planning counselling under the Post-Partul11 Post-Abortal Education and Referral Program at the Port-of-Spain and San Fenaldo General Hospitals
437 SU1ect to the ItBrcement of the Gove1nment the management conshy8ultal ts ~hOLlld undertake a study of th requirement of field workers (home vinitcru) in tmtlUI of are nnd population cov(ra~e
ANNEX 1
Names of Persons Met
Ii Mr T C Taitt Pem1(H~nt 3~crtarY) Ministry of Health
2 Dr M n Henry Chitd Medical Officer Ministry of Health
Ellubeth Quam a Prindpal Medical Officer (1S)
4 Mr G Z Jaine ~ uJiector Population Council
5 Dr Norma Andrews Medical Officer Population Council
6 Mr Jc~n Coury~ Evaluation Adviser Population Council
7 Mr A Jriseph Principal Statistical Officer Population Council
8 Dr C 0 Colman Country Representative Pan American Health )rg ni~ation
9 Mr ranca Kippel Health Education Specialist Ministry of Iea th
10 (1 bullbullines Principal Nursing Officer Ministry of Health
11 Dr Mx won (formerlyHinistry of Health)
12 M3 late Carops Ex-Chairman of Population Council
--
4i 1_ middotIIlt F-ntCWclOotf_Y v OJ t tl
GOVIIlHMEIgt(I OF TINIOAD AND TOampAGQ - NNISTJY OF HIALftf AIJIE1 2NATIONAL FAMilY PLANNING PROGRAMME
F MIL Y PLANNING CUNIC CASE CARD - NEW CASES - NFPPl
li ~~___ 1 ________
~ ecll-U
-- --------------------- shy~) ~~middot~------------------~~~~~~---CIJ------ middot~ii--middot-middot----middot-middot---middot--------- shy
ltv Writt N_ 01(111________________
a ~4itiJtmiddotl_____ ilIIIltIoI~____~____~-__----- shybull ~4
fie l$ - JO tDql IIfIA- tr-JMimiddot _ iJ 1 Odoor o
14aorielaquol_ _~ 0 lio witIleo-La ~ 01 bull - OJ ( _01 1~ltgt1lh o bull- 0$
AacJcu 0 2 CIIriIWA 0 J Os 0
Yv~MONTH ltnollOf~nfIGHTI
Undu 1100U$ Utgtdn 5SCI Undu 11200 01 ~ 50 - 9949 amp100 - 1199 02UlOO - nn9E~ (
0)~ 10- $99 SiOO -- U9~ lOO -- U99 12400 - 1359)-------_-r----shy ~l)o SIS n600 - Hm1300 -- 019 OJ200 il~9 ~------ 99~ a 1)0 m Os1)00 -- l99 1400 -shy $4100 -- 1S999r--- shy
1500 donl S6000aad O399 - lt499I~- I 0lt
ltII
IJ -IC _~tltlioltgti lS
02 IaampJIIocI OJ 04 laM Os
w Oltwio I_-l(~u IrIaa U
h~~ ~Clubl 01 OJ
IS ~C-n 01 toSIitDI 02
Ji poundI on 01 IriIIIuy M ur 02 IV OJ
WU 10 pltIoII~ llaMtl 411 cIIiId 01 Ol it fIolto ~ do~ _14 rou IIlgtJo 1Ia1 ___~_ shy
40
It _ I 00 ~bull FPIiIJ 1
OJ 02 OJ 06
)0 III- iy wOWcf ~1
aMIIl Os
11 T 1gtlt ( h _______ 4)~
06
04 (MIbullbull middot bIrlI ~___~__~_ (-fIJI ~- -~-- (1HJ 49middot SJ
U 10k 01( 1__ raquo$-4
iU1) DOl F ToWotfOlnC DOl 001 or Do [IP 006 001 OIIgtu___Spltclty DOll Nltmo 010
U1Mo I orcpmiddot laquo55middot16
1lD 001 Foam Toblelf_ICim DOl Condom DOl CoomS~ 004 oe Oos WlttuJn 1J OIkr DSpody) 101~ ~Iu 006 Rhylhm 001 DOG OJO
no wI~lmm 4 cd
(I 0) 1110 01 Condor 03 (lorn bull l S~muoidIl 04 Faa TabioolfIIltr- Os RhyUlm 01 lnJrl tible O Advico 090 06
la slt 1)0 19 loti ~rltnlt) ([)sl or 1llOn) ____ --__ bullbully-J n SV - ~JcdS
v~ Cl NCI 0 30 OJI_O I Wr blJ1h 0 I ~ OJ 1 ~ (fOOd V 01 No 02 laquo 6) Cf4
WIiI 1 172
004 001
j D middotmiddot middot
1 ~
r
~
bull I
bullI I I
r c i
ANNEX 3 Pagemiddot 1 of 5
0 raquo rshy -lt l)J ~ 111 t G) 5 shy (J) ~ -
fT1u
i
MINISTTY OF Ho1TH
NTIONl F~ILY LNNING PR-GRbullbullM-tE
~~5tructions to C11nic ClerKa
How to co~ploto the Daily Rogister
~~ ~~v1sd Daily Rosi8ter replnc~D tho one which is now in use tb$ Monthly PC~ri rOt~ arti tho 01( Ci() Dod PollJ j f m It is a pre-coded form and 1411 cl~1p Jd tl a1I6iniul-mIHvn Oel Clinic nctivi~y
110 )rm rollt biJ coupJot)d lrl cupLtcoto using a o(roon shoot Tho top aheot or oriinai ~ust bl) 6(Ult to tho CQgt1tral O[[lCO and tho carbon copy retained in the Gliaic rilo dll the for6a that ar uD~d betwoen the 1st 4nd the 15th of the oIIollth aut bo subClittud tocho office 35 Lnc blttch Those oomp1cted betwoon tho 16th _lid tqemc of tho month must bo ~cnt in a secJnll batch
P lOvLior hns boon Illllde for 25 clients on cZlch forlll new forlll must b IIlied f r poundh 50[810n2 whothur or not ono or lIIore session are hoIdiit the clinic on he sarne day
I th ro alO more htl 25 clionta 1n attondnnco at tho session the additi shyOhAl m~bOl of clionts 10 clients nu~ber 26 27 etc sh0u1l be ontered on the next Imiddotrlll ~i ttout a1tpoundring the numbtlrs in the cvlumn hond Series
51 ppOfil th~ number of aUcnts lQr that session ws 5 this would mean thllt two rJlS ~ lst be 6ubllIitt~dl the first filled uF 1 tltgt 25 And the laquoIncond 1 to 10 Th~ cal bon ofies should bo st~plod togother at thu t0P l~rt h4nd corner of the torm ard ktpt in the Clinic filo lou IIlU6t stapl~ the originftls in the 8~~ monnshyer for lIub~ssion to the ofticl
ie h~ ll idontiflctior- (cc 1 - )
0 lot Ji 9 anythin~ hGro poundhia is int(mdClc for tha computer code
2 ~~pound~ - Print clOflrly tho name of your Clinic
C1Lic Huml or - (cc 4 - 8) Evar1 Clinic Numbor has 5 digits Virite each dig t il a t$purate box
It Pai~_thllsectgdllion (00 lt) -1 1) - Dl monll 10M
lw) bolte IlrO proY140d fetr olAoh pr 01 thQ dISh Enter tho dA) ldns a R
d16ih
emiddot5middot (0 11 I for 115t ( 0 21 for 5th etc Treat month the am pay
e ~ 10 ~ I for I-hrch 0 [2] for September Tho y~nr must be (into ad
I Z I ~ I I 71 q etc
Take as in IixulIple tho dOlte 3rd tllrch 1973 7~ie must bo written
[0131 LSLDI[7l3JDny Month Ye~r
5middot 1~J $~~ - Irom ~-------- To --------shytntol hOI II the time the Clinic 111118 in SW5sion emiddot8middot
(i) 11011 500 lm To 1200 non
(11) Frclt 100 pm To 400 pm
(iii ) IX-OG OO pllI To 6~00 pm
f
2
ADEJ ) Paae ) of S
6 Eov
_ 1hA 1gtIpoundC iIIUlt be nu~o7Ifd tler1ally 1 throurh n lU tbey Are Wled In ~1l8ellJ IInel 1301 tlU 1 Orcl 1 Wled tor a o5038ioll - -I 2 tonY tho _boul~ b I1WJbtl 1 and 2
hlrlll are 25 linos OIl the fOnl Ilnd thoae muet be UBtleS for 25 clients 9 one ior bullbull 01 I ini
ot ~h lc II ol1cM lOlivpound til e linic before soeinc DurOI or doc tor ilnc ii hox rristrltltion nUlJbet had alrearll been recorded on the Dai 1y Roiuter then n line ~hollld be drawn through that entry an1 the eliort nust not 06 includttd in tho totals tor that 0eDion
1lw Ileifitration Num)~r of cueh client must be IiIritten IS n 5-dlrlt oode ClhnC IH11IlElr 315 1IIU8 tborotore be enterod 18J010117]5]
~ Clt ZOt
Coda 1 Codo
10 ~tl c 2t j co 21)
~w elSe - Coda 1 0) d CltaEl - Code 2 Revislt Code 3
Only pound1 01 theBe coiles may be usod
11 prol-O~ ~Eil~1 (cc 22)
If ma climt was L drop-out IIho haoS returned now to the Clinio tor tho first no linmiddot bullwin lt1ro1eo o t he or she should be given CCe 1 It this do 5 II It nprlly leu this colWlln blank
u Hothod middothisllill loe 23)
NOh til t otly ~ Cod 16 tp he ontered in 2lpound of the columna oven thOUGh 10 co11lllJlB 10 provided on the torm The Codes llrol-
Oral Contraceptive Code 0 1 U D Code 1 Condom plUD Codo Z Condor (only) Code 3 Foum tAblets cream Code it DitphrClGJII Code 5 Rhythm Cde 6 Injectible Code 7 Advice Code 8 Other Code 9
It for middotDo-le 1 client rlllll ji yen cclldorls ord foam or creall Iou Qust entor Coole i (condom plulJ) in the appropri~te column This Quat be the only lIotmiddot) tarcie If an in the cnse of a tlnle clinic I the client is Bup)lieu lith COIlOrW only you rmot entEr CorlQ 3 (cpndolll) Do not use a ticII ~ tho (odo Nwber
It is CUi tomary fur 11 cliont 110 is beine put on the oral contraceptive for the first tiT1o and even on other occasionn be issued condoms and 11 crelle or foam a Ilell rI3 a pgtcket of pilla In such Cllses when the piDQ Ilre Ilctually iouou you tlust record Orll (Co~e 0) 08 tho onll metbod ilo othor ntry sll0uld ho nnrlo
Uovever n SJC~ canas vucru condoms and fOHa ~rc eiven but no pilJa (even thoJRh _t _n the intention to issue pills nt the noxt vioit) than the Mothol Th5 ifli t ohoulcl be recorded uo Condor Plus (Code 2)
13 Seen Bybullbullbullbullbull
~rot S-1 SO l
Doctor (Dr) - Code 1 j Nurse (Nul ) - Code 2
Clark (Olk-) - Code If tho Clhnt is vcen hy both tho llootor tlnd the Nurse enter Code 1 t Doctor It 6~61l by the Nurso only arite Code 2 Cod bullbull Cerk is l)llnt for FA Cllnica Clerks in tho Government Cli1t hiwo Llttoll istructed not to i56uo supplios on their own volition
14 fl221~
lhio S~tiCl of -Ie fvrtl t~ke 16 (llrci coluMna (cc 25-+0) nnd 10 tho only part at th iOIQ in llich iore thAn one cod is Zlccoptl1blo Tho purpoco of the )ecton is to 0 able to arrive nt the Cjunntity of 6tock dilltlitJutshyed YOI IIlUdt writo in the CllllOjH-iata colulna the nUllbJr of Il1ch 4rtic1o i~JSu~d ~lo e ha I Oral Contrcilpti vea are aub-di vi dod into types ae_ 3 PIllCKC 9 0 Elynnn LlUot be entered Codo in card column 25
If tor eXllrplc t l cliunt is iosued wi th packots of Zucynon nnd aJ(1 ~ivn 1 conuotll (8inoloo) you ouot enter in oard column 25 and 11 It
cnrd col~8 )2 and J (io 1 in card colucn 2 nnd 2 1n card coluun 33) Nota C)lldoIlU ale to b(t ruoordod individually not os packots of throo) Should n ne LlondoClo be isoued thil3 is to be rc-Qed as 09
If It clint 6 t~ot isoued Blly lIupplies thon you must writo Codo 1 in CQllAlilD 41
It Q eli nt isite the clinic to check on her LUD or her Diaphra~t IUId ro DI W 6 ppl ills nre ispounducd then Code 1 1s wri t ten in column 40
In the FA clinios here a variety ot orll contraceptiveo in orer~l tho elerll wilmiddot~ bJ provided with a specill code shoot The idontifyin coo will b wiittn in Column 29 nnd the nUlber of packets iosued in colwm )0
lralaer-In Code 1 lrllllsie r~ut Coda 2 leIllPQrArr Trnnsfer-In Codo gt
In the cao of n 2ratl8fcr-In I you lUot n160 cOrlpleto coluons 42-51
In the cllU J of A ~~emporary TranGfor-1n (an individual who i8 only v1citing fur clinic tor some epecial trcatcont hna who will bo rdnlnin
~middot(II~~~fO~l~SIl~I3~nn~~~h~rO~nh~1~~190~~nll 2-46 and ler rei IItrntion numbu in colullnll41-51
It the oli( nt i iNt a CrllnoforwIu - Out or loClporu1 tMn loave oolumn 1 blank
16 lr4nst(gtr-tl2~~morrry TilJnder-In (co 42-51) Forl1ltl CUn E1~ (cc 112-46)
hen you rei iatlr L irllsfcrln or Il TJlporary Trnnsfer-In you IIIUBt write I ere the five-digit clinio nucbor of the Clinic iraQ which tho ltlient Me (uIlO
2mer ]letr ~2n ~ (cc 47-51)
frlta fllao Clo r-~itrlltion Nuc~Er ot the client in the Former Clinic (i c bullbull th 1 Sis rnmiddotion ~UlIlh()r which the client carrics 1n the tormor clinio) bull
It tho Forrltl Ho( ist rntion Number iIJ not readily wnilnble you tluct oocpluto thtl epcciol [orlll Transfer-In Not Identifiod Dy Forrlcr RCGi(trn~ t10n Nwlbvr Or ~ flt)rCl is to be cOlplctcd for och cnso nnd th forlJO Ilubmi tted to thu )opllntion Prorrnnme Of fice tOGether with tho Dily Ro~iBtors lhwev~r should the clork leuTI of tho clint B FormlI Uocintra tion lUlllb r )0[(10 Cubmi ttinft the D1ily IOCI otro t hen the nUQbcr shoulo bo -ri ton in colucns 47-51 lna the special foro should lJo deotroyotl
l7 bullbullbullbullbull
r lt bull bull
ADXI ) Pap S ot S
11 UD LV~ (cc 525)
It tb( cliont io ~ivQn An IUD tor the firot tl~o then you should Sri to Codo 1 Inuort ill colurJI 52
It tho olimiddotsnt ia rvinGgtrtltld i th An I UD bullbull tben wse Coda 2 RelnDltlrt shyin (01Uil11 52
It the clLmt is ~tte~~dint chnic beruse her IUD CflClQ out by Haol (cxpll Iion i ~hcn fir te todo ~- UIlllrli1 53~
If c-ltr IU fj IIIS reov in -ne cllnic by tho doctor or nurso t~on vlritI Codec in column 5
II the eli nt otends eiLlie tld explin[l th(lt she rccovcd the IUD tlllleel nen write Coda H in Colwlm 53
It the IUD jr still within the uterus nd the WOIraquoI1 1 11rc6llJlnt thon lIrite 1gt40 4 in Column 53
lZ np h5t (ce 54) It 0 Pull 5mor ie t~ken durin thi visit tben Codo 1 ehould be ampDtere4 in ColWlln 54 Should he c110nt lltt rQ(uircd to rttturn to clin1c for a rogtol1t Pnl) t06t then CoLe 2 llhould bo middotwrittcn in column 54
It no Pllp Scou io taken tde visit Itove colUQn 54 blank
Iraferti1lli (CQ 55)
Ii the e liett io nl1 infortili tr eaoe use Cor1o Ill in colUQn 55
If tbia 1000 not tlpl lonve column 55 blonk
20 Totaltll
CO~1ploete the [)ldegO 1gty puti YI tne totals betweon the double lines nt tu b()ttctl Carrj colUlllnc 20 21 nd gt4 Must hlve tho Bnoe JllIIber and thiG Would coreslonc to the numocr ir attencbnco
Writ$ th to1ul nUlllior of Drop-Outs returned (c022)
Urito 41eo tb totnls fOJ each card column 0 to 9 under tho h(adinu Method thiB Vioit Show tho tote L fgtr OlCl type of contraceptive issued (cc 25-40)
1)0 Dot wrLte 1111 totll lUl(Ier Card Columns 15-19 29 41-51
21 COPmllh bull ~lt h~t~ Monthly ROilort
OQ thG DaLl oCator forlll thnt ccrrOspOldB to tho 1(8t 1$06610n lt 0
oth yo Olllt (vwlgtleto the items nt the botto of the [orampl This is tour ontll~1 n(olt nnd includcD tho totll lumber of sesions Ilntl tho total Iluolcr ( r crop-outs durinr the Qonth
An tiUlsilt n drir which n doctor liB in nttcndnncc is a doctor sOfll~1on and shoulc 00 re(liGtcnd in coltns 56-57 All other sessions 1116 conlliid~recl supply stllciona and thtlY 1110 rocordod in columns 58-59
the total Ilum)nl Jf drop-outo ld the drop-outs by method durinc the onth nre 10 bu oltorou in the inrlicllted boxes
72 Chad Your ~
Milke I ura th t all thE fijul4gtu rre c101r -tNever writo our nutlUQrS 50 InrjEl that they oxtend out of tho
ap~rotr1ato ~ox
Cheek to BoJa tht 1111 numuors 1110 in tho correct boxes -- CJslHloially when Writi1 the totlB
Mllxe Cirtc O thmiddott t1e infoT1I1ntion i6 clear on the corbon COllY before sep rmiddotinr the sheets
Jitn the Fomiddotl lien tly sien YOUl nr me 1t the bot tOil right hnnd corner btl forc subol ttinG it Keep tle CL rb n copy for your rocordn
i
-l ________~~---------~
I _1
Adminiatr-atlve SKVieu
P inba ~~~l1cal lrlnbin~~eltltcal -1 te~ra t~~rvicc (lnatittloaa)
--1- - shy -1------------_-L_ l-r-aJiil- shy _-L_tet1lal d
PlIinm1tJ8 atdUon DetalMid H8Il1tb ~ ________bull Care
-----~ Office of i
the FlIily _IPlill3 roarshy
1- - - -------RegiatUll urnr
ltIi 1 Drelttor Rcgicaat Director Souta Tabqo tacallortb ~ counu gt____ ~ (4 ouottet)
Off1ce of the Res10nal Diractoc L
r----- _L_ -- shy i I bull IREgional Ipitl I
District IIttaltb I bull Othn RelOl ond Hcpital CenteIntt itlt j In 1__ _shy-~- ---- -_j
J r Ii~lth
C~nlef
L
I Ihnlth lie I th Offlcu (1ft lc~
Coullty 1I0p1ta1
Henlth tentet
I

- to shy
s rrogram plannin and target-setting
b proram monitoring and evalllation
c wiL of d 1ci(JTIdnCf by inspections
d Qrg8lizatim 0 es and marketing of contraceptive J~1J-s BLl (iV es at subs idi zed rates through es tablished 1 2 d(~ channel
e information mass media communication and audiovisual ublicity in the field
f prorrotion of famil~r plannIng acceptance through face-to-face cotlmunication by poundi eld workers in domiciliary visi ts
g trIining of personnel
II pr )motion of -esearch enJ
i financial support to voluntary agencies providing family planning services
409 n Statutory CCii1cil may corsi5t or an eminent non-official vith a comri tm ~~1t towacds foJlily plailninf nd the fol1owin~ members
I ~ bull Pfrmanent Secretary ltl-tIlH
Chief Hedical Officer HOH
i Principal ~ecHcal Office ~mH
d Pilhlic RellltionB OfJte(middotmiddot Prtm~ Ministere Office
A represen ta ti V~1 of the Ministry of Education
f ~ representative of the Ministry of Finance
g A representa~ive of the FPA
h A representative ot the C1AC
i H social scientist fcum tle University of the ~Jest Indies
j Three non-officials with experience in management and administration and the
k Director of the Family Planning Program - Secretary
- 11 shy
The COUlcil ITIltW constitute cOlClmittees for Finance - Accounts Personnel and Sup lies nd Stores ir~whi ch )nly members may be included Other commitles sc1h as those 01 training info1nation and education and researCl ara ~valuation r1ili also include experts from outside
410 he Off1ce raquo) cc im Panning Program which at present forms part of th ~Hnis try or [i n should be placed under the Council and its staff strelgtl ilcn~ii2 i~ r181 it may cease to depend upon the services of the Mir is t y of H~alth
C Office of the Family Planning Program
4 11ollwther the Offic~ of the Family Planning Program remains a part of the Mirisry of Health or is transferred under a statutory council if one is set uP i needs to be strengthened to meet the requirements of an expAndshying pr )gn m At present the following sys terns need to be ins ti tuted in this Office
a a 3ystem of setting annual targets for the enrollment of acceptors and the projection of service fadli ties in relation to these targets
I Ci ~ystem oE V)glC loHitoring (the monthly statistics flowing from the clini~s c~iiiain unproc(~s5erl for months)
a system of program evaluation eg demographic effect of tte program cost studies
1 an overall design for media communication based on a study of the reach a~d cost effectiveness of different media and the effect of the meflBsge content and
e a m88t~r plan for training which would comprise an assessment of the training needK of the existing staff and future reshycruits and a long-term plan divided into annual programs
412 Th2 Prograll afiie s~lould have the services of a demographer and a meeia expert A training adviser is expected to be provided by the PARO
413 1be Program Office should evolve schedules of field tours to overliee field operatio1s E~1eh health cente heal th office should be visi ted peridicaLy by the Milt~dical fElce- the Nursing Officer and the Health EduCltoI who should guide and assis t the local staff in carrying out the progam Their tour notes should go into separate dossiers for each institushytion and ~ach dossier should have basic demographic data about the area coveled by each institution These dossiers would be a useful record for revilwing l)errOmance The staff of the Program Office should be augmented to Ol)erte this control procedure
- 12 shy
D Decentralization of Powers
414 ~hete is a concentration of administrative and financial powers in the 11in s try of Health I-JllJCi1 results in an accumulation of references in the Miristl) and delays n field operations Specific powers should be delegated ~o (a) the PliO concerned with MCH and family planningmiddot (b) the Directcr o the Program Office (c) the Regional Director and (d) the County Medica1 Oficecs The Ministry should invite suggestions from these officers and wOlk 01t a schedule of delegated powers
415 A tdgh priority in the matter of delegation of powers is to arm the Regiond Directors with sufficient administrative and financial authority to implement with expedition the health and family planning programs of the Ministmiddoty 1 thin the areas in their jurisdictions
E Integration of Family Planning wi th Haternal and Child Health Services
416 At present family planning services are being provided at 48 Goverrnent hospitals health centers and health offices by using the full shytime E taf cf these institutions and employing part-time (sessional) doctors nurse~ anI clerks where necessary At 29 of these institutions separate famil cl~nics are held on specified days in the weck some being doctor sessi(ms mel others supply sessions run hy nurses and clerks At the remaining 18 imtit1tions family planning services are combined with antenatal child healtL cr postnatal services The Family Planning Association runs 8 unishypurpoe f am ly planning centers which provide daily services and contribute a 11 t le less than half the total number of new acceptors per year
417 N assessment has b~en marie of the effect of integrated MOl and famil~ p~ nnning services an the recrl1i tment of acceptors nor were ~ data readily avallable for this purpose It may be observed however that in a situation of shortages of trained personnel for health services utilization of the existing health staff and facilitieR for family planning is inevitable parU cllLrl y in the interior where such shortages are more pronounced This underlines the need of evaluation of the integrated xai and family planning progtam for its impact on the number of acceptors Also a study needs to be made of che utilization of medical and pilramedical manpower so that it leads to bdter ~llocation of duties and optimUJl utilization of personnel
418 ile integration of faMily planning into Mcn services has certain advalltages as well as attendant risks The advantages are
a Lbe association of family planning with the care of mothers and children helps project a benevolent image of family planning as a program of family welfare This creates a
- 13 shy
1imate favorab~e to the acceptance of family planning aa lt p-)si tL1e il-Eare rreasure rather than a negative program cE limiting c~ildren
h t elps erlist ~r2tion tf doctars and nurses who as c -~ass enjo tft~ Y)er)et~ a~d confidf~nce of the communities i712~ Eerve
c ~ieD of contact with women
d luni-purposa clhlics for ~lCH and family planning services are onenient for motn~rs who would have to travel considerable (listances to the clinics
e hete is better utilizat1on of Acarce heAlth manpower
419 he limitatio$ of integrating family planning with MCH servicesI
are the posiOili ties of loss of focus on family planning as a high priori ty prograrr ald the diffusion of pol1sibility for its implementation These could tlow ve r he safegurded agaifls t by adopting the following measures
a 11e job descriptions of doctors and nurses should be rewritten 0 include the family planning function
b hE perf0rt1iai1ce of ctoltors and nurses should be judged as much )y tbeir inteceq t in planning ~vork as in maternal and ~hjld care and this should he lade known to them
c )octors and nurses involved in ~CH services should be given middot)rj entation and traIning in famj ly planning and their interest 3UEtained by refresher courses seminars meetings and supplies of literature
d Thl techrical (xpert~ in the Office of the Family Planninl Program should maintain liaison with and guide the field agencies in implementing the family plannin~ program For this purpose schedules shoul d be marle out for periodic field inspections
420 It is suggested that the working of half-a-dozen centers where family plbnnLng services have been integrated wi th MCH sessions should be studiei for ehe purpose of standardizing the methodology of delivery of servicl~ Such a study should include staff strength patient load recoril shykeepills 10middot of patents in the clinic timing and frequency of clinic sesaios ani convenience vf patients
F Voluntary Organizations
421 I i~ internrticri31 expedence that the birth control movement is pion aTC tt volunh[~ JilC S Qltl that hen the national governments step in wi tl cmbi ti 019 prjhns wi thin the sLate welfare system voluntary bodies ieh tteir limited ilsrluces restrict their service activities and shift the emplasi i 0 educedgt (f the community training research and contracepshytive Sf vic not 1l7gtilflblr in he official program or in areas not reached by it In nagni tude and expanse the of ficial program in Trinidad and Tobago has alrad~ orertak~n Ce 101umary program Increasingly it will become the domLnart tartner in the total national program while the voluntary agencies will cOltirlU1~ to receive financial support and encouragement to set up high standaeis If service and explore new areas thus acting as a stimulus and an additi_e tl the official program
G FrOB-ram Infomation
422 Thre is no concurrent evaluation or monitoring of the Program The daa or lq72 flowing in from the clinics month by month have r8Jllsined unprocss~d tn the Program Office The official Annual Report - 1971 Sums up th~ poition as fcllo~s
ITThe Research and Evaluation component continued to be the weakest in the Population Program Although a systen of evaluation had been built into the program the follow-up procedures for analyzing the data and for correcting inshyconsistencies are inadequate Requests were made to extend the staff to establish a more viable unit but by the end of the year no chllnges had been made
423 T1e recording and riporting jJrocedures were revised effective Januery 1972 and there has been a further change recently at the instance of t1e Evaluation Adviser Under the system now established the clinics are lequ Lreurod to maintain the following records
a Family Planning Clinic Case Card - New Cases This was introduced on January 1 1972 and has thirty-one entries giving age parity contraceptive listory pregnancies socio-economic background ource of family planning information and agency for notvat ion bull (Annex 2) The case card is made out in duplicate for each new acceptor and a copy sent to the Program Office
b Daily Regis ter This fs a ne~gt1 form recently introduced in replacement of the old regis ter and is preparen
- 15 shy
ie) ruplicate the original to be transmitted to the Program (fHce and the carbon copy to be retained in the clinic Th~ is a very 121zborute form requiring 36 entries to be aa~ for each Chse nel and old attending a session includin~ (ntries to cit L to contTaceptive supplies issued
AijCleX 3 T~13e fcnnG are required to be sent to the Program lffce in i7JO balches every month the first batch for the i IS fif~eeL days and the second for the remaining part of hE month The trtention is that the data appearing in the ~EZlic daily legis ter forms should be compiled in the Program Office and fed back to the clinics Although it is claimed that this new form has been pretested and is workable ex)erience alone will show whether the majority of clinic cL~rks are able to cope with it in a busy session
bull o now-Ho Card TIlis card is intended to keep track of ac ceptor--It has entries for name addresfI and month fcr which a visit is due for each year
bull Aphabe tical Index This is a card index of clients with aidresses
Each i)at en is given a simple clinic card on which the dates of further appo~utnli rc3 an~ indicated A special fonT[ has been devised for the reporting ot cases unler the Post-IartumPost-Abortal Education and Referral Program
424 J system of monitoring progrRm performance from month to month need to bE develQped as a high priori ty The problem is not so much reshycord ng mc transmission of data by the clinics but its aggregation and proclssi ng in the Program Office every month which at present takes a long time The Statistical Officer should have a statistical assistant to help him Ln I he taflk Monthly progress reports should be available to the Mini H t~ n H(llllth and A11 offt eerlil of the ProKrnm Office so that remedial ac tl m I lAY h(~ tuk~n n rll1u- WhOnh1f ~Hfl(AlJtlaTY
42 For the analysis of data and evaluation the Program office shouln haVE th(~ full-time services of a trained demographer
H Field Workers
42) Tie Program nemiddotis tne services of a cadre of field workers to enr)ll neii aceeptoTs follow up acceptors in their homes and revive the int 2remiddott of dropouts Such a category of workers could also be utilizerl for pr1fficting other health programs such as the VD campaign and the inmuni~ation program
47 As an experimental measure one field ~]orker may be assigned to a emi l~ of Hi 000 population This would mean 100 field workers in all
- 16 shy
Earh of the workers should preferably have harl a higher secondary education otherwLe 1gt junior secondalY education They should be married persons with middoti1ltt mot tl-an two or tlree children recruited from the locali ty in which they armiddot~ requlred to function Only persons who have the capaci ty to comnunl at~ and or6anl~e should c chosen A months ini tial orientation
slcu1d enable them to start functioning in the field though reshyfresher CO rSeS tvould be necesslt1ry in due course In Port-of-Spain married mer~ a1C women may be employed on a part-time basis
I Hanagement Study
428 A nanagement study of the Family Planning Program should include a sctu iny of the top m~nagement Atructure (Population Council - Office of the Fanil) PLanning Program - Principal Medical Officer for MCH and Family Planni Ig fetices) the field structure for the delivery of family planning servics (Re0ional Director - District Health Services) including the utilizlti(n if medical and paramedical personnel for adding the function of del ve y )f family planning services and the control and communication proCed1reF Lfnking the top management with the field structure
429 The management consultants may study the functioning of the Popul tio I Council and advise whether it adequately serves the purpose of givini po Licy direction to the Program and if not what changes in its compo itt m and operating procedures may be introduced without altering its bsic craracter as an advisory agency The consultants may suggest an alern at ve form of organizati)n and utilization of personnel which in thir p nion may be better adapted to the needs of the Program
430 Irrespective of whether the Population Council is maintained or it is replaced by an agency of a different character a formation like the Offic of be Family Planning Program would be necessary for the administrashytion i)f 1 he program a task for which i 1 appears inadequately equipped at preselt Its obvious requirements are in the areas of program monitoring and el7alnation program supervision communication and training The manag ememiddotlt consultants may study the structure and procedures of this form~ tio Gnd make suggestions with regard to the augmentation of professional and ~ upp)rt lng staffgt and modification of operating procedures
431 The linkage of the Office of the Family Planning Program with the Miniutry of Health (Central Office) and the District Health Services should be sudied In view of the policy of the Government to integrate MCH and faI11iLy rlallning services it should be examined whether the Principal Medi al Officer for Communi ty Heal th Services (MCH and Family Planning) should be agtpoj nt~d as the Chief of the Office of the Family Planning Program and an adTlilistrative officer of a suitable level inducted in that Office to assist him TIle implication of this suggestion is that the head of the Family PlanJling Program would control the District Health Services
- 17 shy
432 rf 1e management consultants should examine the delegation of adminshyistratiie Bld financial powers of the Ministry of Health to different levels of Progam aclrlirdstration viz bull PMO Program Office Regional Director and County ~djca~ Officers
l33 he system of 01 af Togram information from the clinlcs to the Pr()~ra1 O~fice and tOile processing and use of information in the latter office iholld )e studied
434 he working procedures at the integrated McP and family planning clinics shnuLl be studied This would involve a study of each stage which a clien tpcticmt has to go through from the point of entry to the point of exit after receiving advice service or supplies This study shoulci lead to star dartization of procedures and functions and evolution of -lork norms CognatE st tdies of the working procedures at uni-purpose family planning clinics and su~ply SEssions should also be undertaken An essential component of these ~ tad ~es would be to examine Nhich functions currently performed by docshytors lealh visitors nurses and midives respectively hav~ become so roushytinize ttl it they can he relegated (0 the next 10Her level
435 Reated to working procedures is the problem of job description of medcal 8nd parrunedical personnel involved in family planning from the centra i tc the field level This job description needs to be studied wi th a vie VIW8Id txaminiDg the uttlization of skills and allocation of time by the staff lcc(rd~ng to the functional prj ori ties
436 frV management consultants should study the workings of the curren slralgements fOJ family planning counselling under the Post-Partul11 Post-Abortal Education and Referral Program at the Port-of-Spain and San Fenaldo General Hospitals
437 SU1ect to the ItBrcement of the Gove1nment the management conshy8ultal ts ~hOLlld undertake a study of th requirement of field workers (home vinitcru) in tmtlUI of are nnd population cov(ra~e
ANNEX 1
Names of Persons Met
Ii Mr T C Taitt Pem1(H~nt 3~crtarY) Ministry of Health
2 Dr M n Henry Chitd Medical Officer Ministry of Health
Ellubeth Quam a Prindpal Medical Officer (1S)
4 Mr G Z Jaine ~ uJiector Population Council
5 Dr Norma Andrews Medical Officer Population Council
6 Mr Jc~n Coury~ Evaluation Adviser Population Council
7 Mr A Jriseph Principal Statistical Officer Population Council
8 Dr C 0 Colman Country Representative Pan American Health )rg ni~ation
9 Mr ranca Kippel Health Education Specialist Ministry of Iea th
10 (1 bullbullines Principal Nursing Officer Ministry of Health
11 Dr Mx won (formerlyHinistry of Health)
12 M3 late Carops Ex-Chairman of Population Council
--
4i 1_ middotIIlt F-ntCWclOotf_Y v OJ t tl
GOVIIlHMEIgt(I OF TINIOAD AND TOampAGQ - NNISTJY OF HIALftf AIJIE1 2NATIONAL FAMilY PLANNING PROGRAMME
F MIL Y PLANNING CUNIC CASE CARD - NEW CASES - NFPPl
li ~~___ 1 ________
~ ecll-U
-- --------------------- shy~) ~~middot~------------------~~~~~~---CIJ------ middot~ii--middot-middot----middot-middot---middot--------- shy
ltv Writt N_ 01(111________________
a ~4itiJtmiddotl_____ ilIIIltIoI~____~____~-__----- shybull ~4
fie l$ - JO tDql IIfIA- tr-JMimiddot _ iJ 1 Odoor o
14aorielaquol_ _~ 0 lio witIleo-La ~ 01 bull - OJ ( _01 1~ltgt1lh o bull- 0$
AacJcu 0 2 CIIriIWA 0 J Os 0
Yv~MONTH ltnollOf~nfIGHTI
Undu 1100U$ Utgtdn 5SCI Undu 11200 01 ~ 50 - 9949 amp100 - 1199 02UlOO - nn9E~ (
0)~ 10- $99 SiOO -- U9~ lOO -- U99 12400 - 1359)-------_-r----shy ~l)o SIS n600 - Hm1300 -- 019 OJ200 il~9 ~------ 99~ a 1)0 m Os1)00 -- l99 1400 -shy $4100 -- 1S999r--- shy
1500 donl S6000aad O399 - lt499I~- I 0lt
ltII
IJ -IC _~tltlioltgti lS
02 IaampJIIocI OJ 04 laM Os
w Oltwio I_-l(~u IrIaa U
h~~ ~Clubl 01 OJ
IS ~C-n 01 toSIitDI 02
Ji poundI on 01 IriIIIuy M ur 02 IV OJ
WU 10 pltIoII~ llaMtl 411 cIIiId 01 Ol it fIolto ~ do~ _14 rou IIlgtJo 1Ia1 ___~_ shy
40
It _ I 00 ~bull FPIiIJ 1
OJ 02 OJ 06
)0 III- iy wOWcf ~1
aMIIl Os
11 T 1gtlt ( h _______ 4)~
06
04 (MIbullbull middot bIrlI ~___~__~_ (-fIJI ~- -~-- (1HJ 49middot SJ
U 10k 01( 1__ raquo$-4
iU1) DOl F ToWotfOlnC DOl 001 or Do [IP 006 001 OIIgtu___Spltclty DOll Nltmo 010
U1Mo I orcpmiddot laquo55middot16
1lD 001 Foam Toblelf_ICim DOl Condom DOl CoomS~ 004 oe Oos WlttuJn 1J OIkr DSpody) 101~ ~Iu 006 Rhylhm 001 DOG OJO
no wI~lmm 4 cd
(I 0) 1110 01 Condor 03 (lorn bull l S~muoidIl 04 Faa TabioolfIIltr- Os RhyUlm 01 lnJrl tible O Advico 090 06
la slt 1)0 19 loti ~rltnlt) ([)sl or 1llOn) ____ --__ bullbully-J n SV - ~JcdS
v~ Cl NCI 0 30 OJI_O I Wr blJ1h 0 I ~ OJ 1 ~ (fOOd V 01 No 02 laquo 6) Cf4
WIiI 1 172
004 001
j D middotmiddot middot
1 ~
r
~
bull I
bullI I I
r c i
ANNEX 3 Pagemiddot 1 of 5
0 raquo rshy -lt l)J ~ 111 t G) 5 shy (J) ~ -
fT1u
i
MINISTTY OF Ho1TH
NTIONl F~ILY LNNING PR-GRbullbullM-tE
~~5tructions to C11nic ClerKa
How to co~ploto the Daily Rogister
~~ ~~v1sd Daily Rosi8ter replnc~D tho one which is now in use tb$ Monthly PC~ri rOt~ arti tho 01( Ci() Dod PollJ j f m It is a pre-coded form and 1411 cl~1p Jd tl a1I6iniul-mIHvn Oel Clinic nctivi~y
110 )rm rollt biJ coupJot)d lrl cupLtcoto using a o(roon shoot Tho top aheot or oriinai ~ust bl) 6(Ult to tho CQgt1tral O[[lCO and tho carbon copy retained in the Gliaic rilo dll the for6a that ar uD~d betwoen the 1st 4nd the 15th of the oIIollth aut bo subClittud tocho office 35 Lnc blttch Those oomp1cted betwoon tho 16th _lid tqemc of tho month must bo ~cnt in a secJnll batch
P lOvLior hns boon Illllde for 25 clients on cZlch forlll new forlll must b IIlied f r poundh 50[810n2 whothur or not ono or lIIore session are hoIdiit the clinic on he sarne day
I th ro alO more htl 25 clionta 1n attondnnco at tho session the additi shyOhAl m~bOl of clionts 10 clients nu~ber 26 27 etc sh0u1l be ontered on the next Imiddotrlll ~i ttout a1tpoundring the numbtlrs in the cvlumn hond Series
51 ppOfil th~ number of aUcnts lQr that session ws 5 this would mean thllt two rJlS ~ lst be 6ubllIitt~dl the first filled uF 1 tltgt 25 And the laquoIncond 1 to 10 Th~ cal bon ofies should bo st~plod togother at thu t0P l~rt h4nd corner of the torm ard ktpt in the Clinic filo lou IIlU6t stapl~ the originftls in the 8~~ monnshyer for lIub~ssion to the ofticl
ie h~ ll idontiflctior- (cc 1 - )
0 lot Ji 9 anythin~ hGro poundhia is int(mdClc for tha computer code
2 ~~pound~ - Print clOflrly tho name of your Clinic
C1Lic Huml or - (cc 4 - 8) Evar1 Clinic Numbor has 5 digits Virite each dig t il a t$purate box
It Pai~_thllsectgdllion (00 lt) -1 1) - Dl monll 10M
lw) bolte IlrO proY140d fetr olAoh pr 01 thQ dISh Enter tho dA) ldns a R
d16ih
emiddot5middot (0 11 I for 115t ( 0 21 for 5th etc Treat month the am pay
e ~ 10 ~ I for I-hrch 0 [2] for September Tho y~nr must be (into ad
I Z I ~ I I 71 q etc
Take as in IixulIple tho dOlte 3rd tllrch 1973 7~ie must bo written
[0131 LSLDI[7l3JDny Month Ye~r
5middot 1~J $~~ - Irom ~-------- To --------shytntol hOI II the time the Clinic 111118 in SW5sion emiddot8middot
(i) 11011 500 lm To 1200 non
(11) Frclt 100 pm To 400 pm
(iii ) IX-OG OO pllI To 6~00 pm
f
2
ADEJ ) Paae ) of S
6 Eov
_ 1hA 1gtIpoundC iIIUlt be nu~o7Ifd tler1ally 1 throurh n lU tbey Are Wled In ~1l8ellJ IInel 1301 tlU 1 Orcl 1 Wled tor a o5038ioll - -I 2 tonY tho _boul~ b I1WJbtl 1 and 2
hlrlll are 25 linos OIl the fOnl Ilnd thoae muet be UBtleS for 25 clients 9 one ior bullbull 01 I ini
ot ~h lc II ol1cM lOlivpound til e linic before soeinc DurOI or doc tor ilnc ii hox rristrltltion nUlJbet had alrearll been recorded on the Dai 1y Roiuter then n line ~hollld be drawn through that entry an1 the eliort nust not 06 includttd in tho totals tor that 0eDion
1lw Ileifitration Num)~r of cueh client must be IiIritten IS n 5-dlrlt oode ClhnC IH11IlElr 315 1IIU8 tborotore be enterod 18J010117]5]
~ Clt ZOt
Coda 1 Codo
10 ~tl c 2t j co 21)
~w elSe - Coda 1 0) d CltaEl - Code 2 Revislt Code 3
Only pound1 01 theBe coiles may be usod
11 prol-O~ ~Eil~1 (cc 22)
If ma climt was L drop-out IIho haoS returned now to the Clinio tor tho first no linmiddot bullwin lt1ro1eo o t he or she should be given CCe 1 It this do 5 II It nprlly leu this colWlln blank
u Hothod middothisllill loe 23)
NOh til t otly ~ Cod 16 tp he ontered in 2lpound of the columna oven thOUGh 10 co11lllJlB 10 provided on the torm The Codes llrol-
Oral Contraceptive Code 0 1 U D Code 1 Condom plUD Codo Z Condor (only) Code 3 Foum tAblets cream Code it DitphrClGJII Code 5 Rhythm Cde 6 Injectible Code 7 Advice Code 8 Other Code 9
It for middotDo-le 1 client rlllll ji yen cclldorls ord foam or creall Iou Qust entor Coole i (condom plulJ) in the appropri~te column This Quat be the only lIotmiddot) tarcie If an in the cnse of a tlnle clinic I the client is Bup)lieu lith COIlOrW only you rmot entEr CorlQ 3 (cpndolll) Do not use a ticII ~ tho (odo Nwber
It is CUi tomary fur 11 cliont 110 is beine put on the oral contraceptive for the first tiT1o and even on other occasionn be issued condoms and 11 crelle or foam a Ilell rI3 a pgtcket of pilla In such Cllses when the piDQ Ilre Ilctually iouou you tlust record Orll (Co~e 0) 08 tho onll metbod ilo othor ntry sll0uld ho nnrlo
Uovever n SJC~ canas vucru condoms and fOHa ~rc eiven but no pilJa (even thoJRh _t _n the intention to issue pills nt the noxt vioit) than the Mothol Th5 ifli t ohoulcl be recorded uo Condor Plus (Code 2)
13 Seen Bybullbullbullbullbull
~rot S-1 SO l
Doctor (Dr) - Code 1 j Nurse (Nul ) - Code 2
Clark (Olk-) - Code If tho Clhnt is vcen hy both tho llootor tlnd the Nurse enter Code 1 t Doctor It 6~61l by the Nurso only arite Code 2 Cod bullbull Cerk is l)llnt for FA Cllnica Clerks in tho Government Cli1t hiwo Llttoll istructed not to i56uo supplios on their own volition
14 fl221~
lhio S~tiCl of -Ie fvrtl t~ke 16 (llrci coluMna (cc 25-+0) nnd 10 tho only part at th iOIQ in llich iore thAn one cod is Zlccoptl1blo Tho purpoco of the )ecton is to 0 able to arrive nt the Cjunntity of 6tock dilltlitJutshyed YOI IIlUdt writo in the CllllOjH-iata colulna the nUllbJr of Il1ch 4rtic1o i~JSu~d ~lo e ha I Oral Contrcilpti vea are aub-di vi dod into types ae_ 3 PIllCKC 9 0 Elynnn LlUot be entered Codo in card column 25
If tor eXllrplc t l cliunt is iosued wi th packots of Zucynon nnd aJ(1 ~ivn 1 conuotll (8inoloo) you ouot enter in oard column 25 and 11 It
cnrd col~8 )2 and J (io 1 in card colucn 2 nnd 2 1n card coluun 33) Nota C)lldoIlU ale to b(t ruoordod individually not os packots of throo) Should n ne LlondoClo be isoued thil3 is to be rc-Qed as 09
If It clint 6 t~ot isoued Blly lIupplies thon you must writo Codo 1 in CQllAlilD 41
It Q eli nt isite the clinic to check on her LUD or her Diaphra~t IUId ro DI W 6 ppl ills nre ispounducd then Code 1 1s wri t ten in column 40
In the FA clinios here a variety ot orll contraceptiveo in orer~l tho elerll wilmiddot~ bJ provided with a specill code shoot The idontifyin coo will b wiittn in Column 29 nnd the nUlber of packets iosued in colwm )0
lralaer-In Code 1 lrllllsie r~ut Coda 2 leIllPQrArr Trnnsfer-In Codo gt
In the cao of n 2ratl8fcr-In I you lUot n160 cOrlpleto coluons 42-51
In the cllU J of A ~~emporary TranGfor-1n (an individual who i8 only v1citing fur clinic tor some epecial trcatcont hna who will bo rdnlnin
~middot(II~~~fO~l~SIl~I3~nn~~~h~rO~nh~1~~190~~nll 2-46 and ler rei IItrntion numbu in colullnll41-51
It the oli( nt i iNt a CrllnoforwIu - Out or loClporu1 tMn loave oolumn 1 blank
16 lr4nst(gtr-tl2~~morrry TilJnder-In (co 42-51) Forl1ltl CUn E1~ (cc 112-46)
hen you rei iatlr L irllsfcrln or Il TJlporary Trnnsfer-In you IIIUBt write I ere the five-digit clinio nucbor of the Clinic iraQ which tho ltlient Me (uIlO
2mer ]letr ~2n ~ (cc 47-51)
frlta fllao Clo r-~itrlltion Nuc~Er ot the client in the Former Clinic (i c bullbull th 1 Sis rnmiddotion ~UlIlh()r which the client carrics 1n the tormor clinio) bull
It tho Forrltl Ho( ist rntion Number iIJ not readily wnilnble you tluct oocpluto thtl epcciol [orlll Transfer-In Not Identifiod Dy Forrlcr RCGi(trn~ t10n Nwlbvr Or ~ flt)rCl is to be cOlplctcd for och cnso nnd th forlJO Ilubmi tted to thu )opllntion Prorrnnme Of fice tOGether with tho Dily Ro~iBtors lhwev~r should the clork leuTI of tho clint B FormlI Uocintra tion lUlllb r )0[(10 Cubmi ttinft the D1ily IOCI otro t hen the nUQbcr shoulo bo -ri ton in colucns 47-51 lna the special foro should lJo deotroyotl
l7 bullbullbullbullbull
r lt bull bull
ADXI ) Pap S ot S
11 UD LV~ (cc 525)
It tb( cliont io ~ivQn An IUD tor the firot tl~o then you should Sri to Codo 1 Inuort ill colurJI 52
It tho olimiddotsnt ia rvinGgtrtltld i th An I UD bullbull tben wse Coda 2 RelnDltlrt shyin (01Uil11 52
It the clLmt is ~tte~~dint chnic beruse her IUD CflClQ out by Haol (cxpll Iion i ~hcn fir te todo ~- UIlllrli1 53~
If c-ltr IU fj IIIS reov in -ne cllnic by tho doctor or nurso t~on vlritI Codec in column 5
II the eli nt otends eiLlie tld explin[l th(lt she rccovcd the IUD tlllleel nen write Coda H in Colwlm 53
It the IUD jr still within the uterus nd the WOIraquoI1 1 11rc6llJlnt thon lIrite 1gt40 4 in Column 53
lZ np h5t (ce 54) It 0 Pull 5mor ie t~ken durin thi visit tben Codo 1 ehould be ampDtere4 in ColWlln 54 Should he c110nt lltt rQ(uircd to rttturn to clin1c for a rogtol1t Pnl) t06t then CoLe 2 llhould bo middotwrittcn in column 54
It no Pllp Scou io taken tde visit Itove colUQn 54 blank
Iraferti1lli (CQ 55)
Ii the e liett io nl1 infortili tr eaoe use Cor1o Ill in colUQn 55
If tbia 1000 not tlpl lonve column 55 blonk
20 Totaltll
CO~1ploete the [)ldegO 1gty puti YI tne totals betweon the double lines nt tu b()ttctl Carrj colUlllnc 20 21 nd gt4 Must hlve tho Bnoe JllIIber and thiG Would coreslonc to the numocr ir attencbnco
Writ$ th to1ul nUlllior of Drop-Outs returned (c022)
Urito 41eo tb totnls fOJ each card column 0 to 9 under tho h(adinu Method thiB Vioit Show tho tote L fgtr OlCl type of contraceptive issued (cc 25-40)
1)0 Dot wrLte 1111 totll lUl(Ier Card Columns 15-19 29 41-51
21 COPmllh bull ~lt h~t~ Monthly ROilort
OQ thG DaLl oCator forlll thnt ccrrOspOldB to tho 1(8t 1$06610n lt 0
oth yo Olllt (vwlgtleto the items nt the botto of the [orampl This is tour ontll~1 n(olt nnd includcD tho totll lumber of sesions Ilntl tho total Iluolcr ( r crop-outs durinr the Qonth
An tiUlsilt n drir which n doctor liB in nttcndnncc is a doctor sOfll~1on and shoulc 00 re(liGtcnd in coltns 56-57 All other sessions 1116 conlliid~recl supply stllciona and thtlY 1110 rocordod in columns 58-59
the total Ilum)nl Jf drop-outo ld the drop-outs by method durinc the onth nre 10 bu oltorou in the inrlicllted boxes
72 Chad Your ~
Milke I ura th t all thE fijul4gtu rre c101r -tNever writo our nutlUQrS 50 InrjEl that they oxtend out of tho
ap~rotr1ato ~ox
Cheek to BoJa tht 1111 numuors 1110 in tho correct boxes -- CJslHloially when Writi1 the totlB
Mllxe Cirtc O thmiddott t1e infoT1I1ntion i6 clear on the corbon COllY before sep rmiddotinr the sheets
Jitn the Fomiddotl lien tly sien YOUl nr me 1t the bot tOil right hnnd corner btl forc subol ttinG it Keep tle CL rb n copy for your rocordn
i
-l ________~~---------~
I _1
Adminiatr-atlve SKVieu
P inba ~~~l1cal lrlnbin~~eltltcal -1 te~ra t~~rvicc (lnatittloaa)
--1- - shy -1------------_-L_ l-r-aJiil- shy _-L_tet1lal d
PlIinm1tJ8 atdUon DetalMid H8Il1tb ~ ________bull Care
-----~ Office of i
the FlIily _IPlill3 roarshy
1- - - -------RegiatUll urnr
ltIi 1 Drelttor Rcgicaat Director Souta Tabqo tacallortb ~ counu gt____ ~ (4 ouottet)
Off1ce of the Res10nal Diractoc L
r----- _L_ -- shy i I bull IREgional Ipitl I
District IIttaltb I bull Othn RelOl ond Hcpital CenteIntt itlt j In 1__ _shy-~- ---- -_j
J r Ii~lth
C~nlef
L
I Ihnlth lie I th Offlcu (1ft lc~
Coullty 1I0p1ta1
Henlth tentet
I

- 11 shy
The COUlcil ITIltW constitute cOlClmittees for Finance - Accounts Personnel and Sup lies nd Stores ir~whi ch )nly members may be included Other commitles sc1h as those 01 training info1nation and education and researCl ara ~valuation r1ili also include experts from outside
410 he Off1ce raquo) cc im Panning Program which at present forms part of th ~Hnis try or [i n should be placed under the Council and its staff strelgtl ilcn~ii2 i~ r181 it may cease to depend upon the services of the Mir is t y of H~alth
C Office of the Family Planning Program
4 11ollwther the Offic~ of the Family Planning Program remains a part of the Mirisry of Health or is transferred under a statutory council if one is set uP i needs to be strengthened to meet the requirements of an expAndshying pr )gn m At present the following sys terns need to be ins ti tuted in this Office
a a 3ystem of setting annual targets for the enrollment of acceptors and the projection of service fadli ties in relation to these targets
I Ci ~ystem oE V)glC loHitoring (the monthly statistics flowing from the clini~s c~iiiain unproc(~s5erl for months)
a system of program evaluation eg demographic effect of tte program cost studies
1 an overall design for media communication based on a study of the reach a~d cost effectiveness of different media and the effect of the meflBsge content and
e a m88t~r plan for training which would comprise an assessment of the training needK of the existing staff and future reshycruits and a long-term plan divided into annual programs
412 Th2 Prograll afiie s~lould have the services of a demographer and a meeia expert A training adviser is expected to be provided by the PARO
413 1be Program Office should evolve schedules of field tours to overliee field operatio1s E~1eh health cente heal th office should be visi ted peridicaLy by the Milt~dical fElce- the Nursing Officer and the Health EduCltoI who should guide and assis t the local staff in carrying out the progam Their tour notes should go into separate dossiers for each institushytion and ~ach dossier should have basic demographic data about the area coveled by each institution These dossiers would be a useful record for revilwing l)errOmance The staff of the Program Office should be augmented to Ol)erte this control procedure
- 12 shy
D Decentralization of Powers
414 ~hete is a concentration of administrative and financial powers in the 11in s try of Health I-JllJCi1 results in an accumulation of references in the Miristl) and delays n field operations Specific powers should be delegated ~o (a) the PliO concerned with MCH and family planningmiddot (b) the Directcr o the Program Office (c) the Regional Director and (d) the County Medica1 Oficecs The Ministry should invite suggestions from these officers and wOlk 01t a schedule of delegated powers
415 A tdgh priority in the matter of delegation of powers is to arm the Regiond Directors with sufficient administrative and financial authority to implement with expedition the health and family planning programs of the Ministmiddoty 1 thin the areas in their jurisdictions
E Integration of Family Planning wi th Haternal and Child Health Services
416 At present family planning services are being provided at 48 Goverrnent hospitals health centers and health offices by using the full shytime E taf cf these institutions and employing part-time (sessional) doctors nurse~ anI clerks where necessary At 29 of these institutions separate famil cl~nics are held on specified days in the weck some being doctor sessi(ms mel others supply sessions run hy nurses and clerks At the remaining 18 imtit1tions family planning services are combined with antenatal child healtL cr postnatal services The Family Planning Association runs 8 unishypurpoe f am ly planning centers which provide daily services and contribute a 11 t le less than half the total number of new acceptors per year
417 N assessment has b~en marie of the effect of integrated MOl and famil~ p~ nnning services an the recrl1i tment of acceptors nor were ~ data readily avallable for this purpose It may be observed however that in a situation of shortages of trained personnel for health services utilization of the existing health staff and facilitieR for family planning is inevitable parU cllLrl y in the interior where such shortages are more pronounced This underlines the need of evaluation of the integrated xai and family planning progtam for its impact on the number of acceptors Also a study needs to be made of che utilization of medical and pilramedical manpower so that it leads to bdter ~llocation of duties and optimUJl utilization of personnel
418 ile integration of faMily planning into Mcn services has certain advalltages as well as attendant risks The advantages are
a Lbe association of family planning with the care of mothers and children helps project a benevolent image of family planning as a program of family welfare This creates a
- 13 shy
1imate favorab~e to the acceptance of family planning aa lt p-)si tL1e il-Eare rreasure rather than a negative program cE limiting c~ildren
h t elps erlist ~r2tion tf doctars and nurses who as c -~ass enjo tft~ Y)er)et~ a~d confidf~nce of the communities i712~ Eerve
c ~ieD of contact with women
d luni-purposa clhlics for ~lCH and family planning services are onenient for motn~rs who would have to travel considerable (listances to the clinics
e hete is better utilizat1on of Acarce heAlth manpower
419 he limitatio$ of integrating family planning with MCH servicesI
are the posiOili ties of loss of focus on family planning as a high priori ty prograrr ald the diffusion of pol1sibility for its implementation These could tlow ve r he safegurded agaifls t by adopting the following measures
a 11e job descriptions of doctors and nurses should be rewritten 0 include the family planning function
b hE perf0rt1iai1ce of ctoltors and nurses should be judged as much )y tbeir inteceq t in planning ~vork as in maternal and ~hjld care and this should he lade known to them
c )octors and nurses involved in ~CH services should be given middot)rj entation and traIning in famj ly planning and their interest 3UEtained by refresher courses seminars meetings and supplies of literature
d Thl techrical (xpert~ in the Office of the Family Planninl Program should maintain liaison with and guide the field agencies in implementing the family plannin~ program For this purpose schedules shoul d be marle out for periodic field inspections
420 It is suggested that the working of half-a-dozen centers where family plbnnLng services have been integrated wi th MCH sessions should be studiei for ehe purpose of standardizing the methodology of delivery of servicl~ Such a study should include staff strength patient load recoril shykeepills 10middot of patents in the clinic timing and frequency of clinic sesaios ani convenience vf patients
F Voluntary Organizations
421 I i~ internrticri31 expedence that the birth control movement is pion aTC tt volunh[~ JilC S Qltl that hen the national governments step in wi tl cmbi ti 019 prjhns wi thin the sLate welfare system voluntary bodies ieh tteir limited ilsrluces restrict their service activities and shift the emplasi i 0 educedgt (f the community training research and contracepshytive Sf vic not 1l7gtilflblr in he official program or in areas not reached by it In nagni tude and expanse the of ficial program in Trinidad and Tobago has alrad~ orertak~n Ce 101umary program Increasingly it will become the domLnart tartner in the total national program while the voluntary agencies will cOltirlU1~ to receive financial support and encouragement to set up high standaeis If service and explore new areas thus acting as a stimulus and an additi_e tl the official program
G FrOB-ram Infomation
422 Thre is no concurrent evaluation or monitoring of the Program The daa or lq72 flowing in from the clinics month by month have r8Jllsined unprocss~d tn the Program Office The official Annual Report - 1971 Sums up th~ poition as fcllo~s
ITThe Research and Evaluation component continued to be the weakest in the Population Program Although a systen of evaluation had been built into the program the follow-up procedures for analyzing the data and for correcting inshyconsistencies are inadequate Requests were made to extend the staff to establish a more viable unit but by the end of the year no chllnges had been made
423 T1e recording and riporting jJrocedures were revised effective Januery 1972 and there has been a further change recently at the instance of t1e Evaluation Adviser Under the system now established the clinics are lequ Lreurod to maintain the following records
a Family Planning Clinic Case Card - New Cases This was introduced on January 1 1972 and has thirty-one entries giving age parity contraceptive listory pregnancies socio-economic background ource of family planning information and agency for notvat ion bull (Annex 2) The case card is made out in duplicate for each new acceptor and a copy sent to the Program Office
b Daily Regis ter This fs a ne~gt1 form recently introduced in replacement of the old regis ter and is preparen
- 15 shy
ie) ruplicate the original to be transmitted to the Program (fHce and the carbon copy to be retained in the clinic Th~ is a very 121zborute form requiring 36 entries to be aa~ for each Chse nel and old attending a session includin~ (ntries to cit L to contTaceptive supplies issued
AijCleX 3 T~13e fcnnG are required to be sent to the Program lffce in i7JO balches every month the first batch for the i IS fif~eeL days and the second for the remaining part of hE month The trtention is that the data appearing in the ~EZlic daily legis ter forms should be compiled in the Program Office and fed back to the clinics Although it is claimed that this new form has been pretested and is workable ex)erience alone will show whether the majority of clinic cL~rks are able to cope with it in a busy session
bull o now-Ho Card TIlis card is intended to keep track of ac ceptor--It has entries for name addresfI and month fcr which a visit is due for each year
bull Aphabe tical Index This is a card index of clients with aidresses
Each i)at en is given a simple clinic card on which the dates of further appo~utnli rc3 an~ indicated A special fonT[ has been devised for the reporting ot cases unler the Post-IartumPost-Abortal Education and Referral Program
424 J system of monitoring progrRm performance from month to month need to bE develQped as a high priori ty The problem is not so much reshycord ng mc transmission of data by the clinics but its aggregation and proclssi ng in the Program Office every month which at present takes a long time The Statistical Officer should have a statistical assistant to help him Ln I he taflk Monthly progress reports should be available to the Mini H t~ n H(llllth and A11 offt eerlil of the ProKrnm Office so that remedial ac tl m I lAY h(~ tuk~n n rll1u- WhOnh1f ~Hfl(AlJtlaTY
42 For the analysis of data and evaluation the Program office shouln haVE th(~ full-time services of a trained demographer
H Field Workers
42) Tie Program nemiddotis tne services of a cadre of field workers to enr)ll neii aceeptoTs follow up acceptors in their homes and revive the int 2remiddott of dropouts Such a category of workers could also be utilizerl for pr1fficting other health programs such as the VD campaign and the inmuni~ation program
47 As an experimental measure one field ~]orker may be assigned to a emi l~ of Hi 000 population This would mean 100 field workers in all
- 16 shy
Earh of the workers should preferably have harl a higher secondary education otherwLe 1gt junior secondalY education They should be married persons with middoti1ltt mot tl-an two or tlree children recruited from the locali ty in which they armiddot~ requlred to function Only persons who have the capaci ty to comnunl at~ and or6anl~e should c chosen A months ini tial orientation
slcu1d enable them to start functioning in the field though reshyfresher CO rSeS tvould be necesslt1ry in due course In Port-of-Spain married mer~ a1C women may be employed on a part-time basis
I Hanagement Study
428 A nanagement study of the Family Planning Program should include a sctu iny of the top m~nagement Atructure (Population Council - Office of the Fanil) PLanning Program - Principal Medical Officer for MCH and Family Planni Ig fetices) the field structure for the delivery of family planning servics (Re0ional Director - District Health Services) including the utilizlti(n if medical and paramedical personnel for adding the function of del ve y )f family planning services and the control and communication proCed1reF Lfnking the top management with the field structure
429 The management consultants may study the functioning of the Popul tio I Council and advise whether it adequately serves the purpose of givini po Licy direction to the Program and if not what changes in its compo itt m and operating procedures may be introduced without altering its bsic craracter as an advisory agency The consultants may suggest an alern at ve form of organizati)n and utilization of personnel which in thir p nion may be better adapted to the needs of the Program
430 Irrespective of whether the Population Council is maintained or it is replaced by an agency of a different character a formation like the Offic of be Family Planning Program would be necessary for the administrashytion i)f 1 he program a task for which i 1 appears inadequately equipped at preselt Its obvious requirements are in the areas of program monitoring and el7alnation program supervision communication and training The manag ememiddotlt consultants may study the structure and procedures of this form~ tio Gnd make suggestions with regard to the augmentation of professional and ~ upp)rt lng staffgt and modification of operating procedures
431 The linkage of the Office of the Family Planning Program with the Miniutry of Health (Central Office) and the District Health Services should be sudied In view of the policy of the Government to integrate MCH and faI11iLy rlallning services it should be examined whether the Principal Medi al Officer for Communi ty Heal th Services (MCH and Family Planning) should be agtpoj nt~d as the Chief of the Office of the Family Planning Program and an adTlilistrative officer of a suitable level inducted in that Office to assist him TIle implication of this suggestion is that the head of the Family PlanJling Program would control the District Health Services
- 17 shy
432 rf 1e management consultants should examine the delegation of adminshyistratiie Bld financial powers of the Ministry of Health to different levels of Progam aclrlirdstration viz bull PMO Program Office Regional Director and County ~djca~ Officers
l33 he system of 01 af Togram information from the clinlcs to the Pr()~ra1 O~fice and tOile processing and use of information in the latter office iholld )e studied
434 he working procedures at the integrated McP and family planning clinics shnuLl be studied This would involve a study of each stage which a clien tpcticmt has to go through from the point of entry to the point of exit after receiving advice service or supplies This study shoulci lead to star dartization of procedures and functions and evolution of -lork norms CognatE st tdies of the working procedures at uni-purpose family planning clinics and su~ply SEssions should also be undertaken An essential component of these ~ tad ~es would be to examine Nhich functions currently performed by docshytors lealh visitors nurses and midives respectively hav~ become so roushytinize ttl it they can he relegated (0 the next 10Her level
435 Reated to working procedures is the problem of job description of medcal 8nd parrunedical personnel involved in family planning from the centra i tc the field level This job description needs to be studied wi th a vie VIW8Id txaminiDg the uttlization of skills and allocation of time by the staff lcc(rd~ng to the functional prj ori ties
436 frV management consultants should study the workings of the curren slralgements fOJ family planning counselling under the Post-Partul11 Post-Abortal Education and Referral Program at the Port-of-Spain and San Fenaldo General Hospitals
437 SU1ect to the ItBrcement of the Gove1nment the management conshy8ultal ts ~hOLlld undertake a study of th requirement of field workers (home vinitcru) in tmtlUI of are nnd population cov(ra~e
ANNEX 1
Names of Persons Met
Ii Mr T C Taitt Pem1(H~nt 3~crtarY) Ministry of Health
2 Dr M n Henry Chitd Medical Officer Ministry of Health
Ellubeth Quam a Prindpal Medical Officer (1S)
4 Mr G Z Jaine ~ uJiector Population Council
5 Dr Norma Andrews Medical Officer Population Council
6 Mr Jc~n Coury~ Evaluation Adviser Population Council
7 Mr A Jriseph Principal Statistical Officer Population Council
8 Dr C 0 Colman Country Representative Pan American Health )rg ni~ation
9 Mr ranca Kippel Health Education Specialist Ministry of Iea th
10 (1 bullbullines Principal Nursing Officer Ministry of Health
11 Dr Mx won (formerlyHinistry of Health)
12 M3 late Carops Ex-Chairman of Population Council
--
4i 1_ middotIIlt F-ntCWclOotf_Y v OJ t tl
GOVIIlHMEIgt(I OF TINIOAD AND TOampAGQ - NNISTJY OF HIALftf AIJIE1 2NATIONAL FAMilY PLANNING PROGRAMME
F MIL Y PLANNING CUNIC CASE CARD - NEW CASES - NFPPl
li ~~___ 1 ________
~ ecll-U
-- --------------------- shy~) ~~middot~------------------~~~~~~---CIJ------ middot~ii--middot-middot----middot-middot---middot--------- shy
ltv Writt N_ 01(111________________
a ~4itiJtmiddotl_____ ilIIIltIoI~____~____~-__----- shybull ~4
fie l$ - JO tDql IIfIA- tr-JMimiddot _ iJ 1 Odoor o
14aorielaquol_ _~ 0 lio witIleo-La ~ 01 bull - OJ ( _01 1~ltgt1lh o bull- 0$
AacJcu 0 2 CIIriIWA 0 J Os 0
Yv~MONTH ltnollOf~nfIGHTI
Undu 1100U$ Utgtdn 5SCI Undu 11200 01 ~ 50 - 9949 amp100 - 1199 02UlOO - nn9E~ (
0)~ 10- $99 SiOO -- U9~ lOO -- U99 12400 - 1359)-------_-r----shy ~l)o SIS n600 - Hm1300 -- 019 OJ200 il~9 ~------ 99~ a 1)0 m Os1)00 -- l99 1400 -shy $4100 -- 1S999r--- shy
1500 donl S6000aad O399 - lt499I~- I 0lt
ltII
IJ -IC _~tltlioltgti lS
02 IaampJIIocI OJ 04 laM Os
w Oltwio I_-l(~u IrIaa U
h~~ ~Clubl 01 OJ
IS ~C-n 01 toSIitDI 02
Ji poundI on 01 IriIIIuy M ur 02 IV OJ
WU 10 pltIoII~ llaMtl 411 cIIiId 01 Ol it fIolto ~ do~ _14 rou IIlgtJo 1Ia1 ___~_ shy
40
It _ I 00 ~bull FPIiIJ 1
OJ 02 OJ 06
)0 III- iy wOWcf ~1
aMIIl Os
11 T 1gtlt ( h _______ 4)~
06
04 (MIbullbull middot bIrlI ~___~__~_ (-fIJI ~- -~-- (1HJ 49middot SJ
U 10k 01( 1__ raquo$-4
iU1) DOl F ToWotfOlnC DOl 001 or Do [IP 006 001 OIIgtu___Spltclty DOll Nltmo 010
U1Mo I orcpmiddot laquo55middot16
1lD 001 Foam Toblelf_ICim DOl Condom DOl CoomS~ 004 oe Oos WlttuJn 1J OIkr DSpody) 101~ ~Iu 006 Rhylhm 001 DOG OJO
no wI~lmm 4 cd
(I 0) 1110 01 Condor 03 (lorn bull l S~muoidIl 04 Faa TabioolfIIltr- Os RhyUlm 01 lnJrl tible O Advico 090 06
la slt 1)0 19 loti ~rltnlt) ([)sl or 1llOn) ____ --__ bullbully-J n SV - ~JcdS
v~ Cl NCI 0 30 OJI_O I Wr blJ1h 0 I ~ OJ 1 ~ (fOOd V 01 No 02 laquo 6) Cf4
WIiI 1 172
004 001
j D middotmiddot middot
1 ~
r
~
bull I
bullI I I
r c i
ANNEX 3 Pagemiddot 1 of 5
0 raquo rshy -lt l)J ~ 111 t G) 5 shy (J) ~ -
fT1u
i
MINISTTY OF Ho1TH
NTIONl F~ILY LNNING PR-GRbullbullM-tE
~~5tructions to C11nic ClerKa
How to co~ploto the Daily Rogister
~~ ~~v1sd Daily Rosi8ter replnc~D tho one which is now in use tb$ Monthly PC~ri rOt~ arti tho 01( Ci() Dod PollJ j f m It is a pre-coded form and 1411 cl~1p Jd tl a1I6iniul-mIHvn Oel Clinic nctivi~y
110 )rm rollt biJ coupJot)d lrl cupLtcoto using a o(roon shoot Tho top aheot or oriinai ~ust bl) 6(Ult to tho CQgt1tral O[[lCO and tho carbon copy retained in the Gliaic rilo dll the for6a that ar uD~d betwoen the 1st 4nd the 15th of the oIIollth aut bo subClittud tocho office 35 Lnc blttch Those oomp1cted betwoon tho 16th _lid tqemc of tho month must bo ~cnt in a secJnll batch
P lOvLior hns boon Illllde for 25 clients on cZlch forlll new forlll must b IIlied f r poundh 50[810n2 whothur or not ono or lIIore session are hoIdiit the clinic on he sarne day
I th ro alO more htl 25 clionta 1n attondnnco at tho session the additi shyOhAl m~bOl of clionts 10 clients nu~ber 26 27 etc sh0u1l be ontered on the next Imiddotrlll ~i ttout a1tpoundring the numbtlrs in the cvlumn hond Series
51 ppOfil th~ number of aUcnts lQr that session ws 5 this would mean thllt two rJlS ~ lst be 6ubllIitt~dl the first filled uF 1 tltgt 25 And the laquoIncond 1 to 10 Th~ cal bon ofies should bo st~plod togother at thu t0P l~rt h4nd corner of the torm ard ktpt in the Clinic filo lou IIlU6t stapl~ the originftls in the 8~~ monnshyer for lIub~ssion to the ofticl
ie h~ ll idontiflctior- (cc 1 - )
0 lot Ji 9 anythin~ hGro poundhia is int(mdClc for tha computer code
2 ~~pound~ - Print clOflrly tho name of your Clinic
C1Lic Huml or - (cc 4 - 8) Evar1 Clinic Numbor has 5 digits Virite each dig t il a t$purate box
It Pai~_thllsectgdllion (00 lt) -1 1) - Dl monll 10M
lw) bolte IlrO proY140d fetr olAoh pr 01 thQ dISh Enter tho dA) ldns a R
d16ih
emiddot5middot (0 11 I for 115t ( 0 21 for 5th etc Treat month the am pay
e ~ 10 ~ I for I-hrch 0 [2] for September Tho y~nr must be (into ad
I Z I ~ I I 71 q etc
Take as in IixulIple tho dOlte 3rd tllrch 1973 7~ie must bo written
[0131 LSLDI[7l3JDny Month Ye~r
5middot 1~J $~~ - Irom ~-------- To --------shytntol hOI II the time the Clinic 111118 in SW5sion emiddot8middot
(i) 11011 500 lm To 1200 non
(11) Frclt 100 pm To 400 pm
(iii ) IX-OG OO pllI To 6~00 pm
f
2
ADEJ ) Paae ) of S
6 Eov
_ 1hA 1gtIpoundC iIIUlt be nu~o7Ifd tler1ally 1 throurh n lU tbey Are Wled In ~1l8ellJ IInel 1301 tlU 1 Orcl 1 Wled tor a o5038ioll - -I 2 tonY tho _boul~ b I1WJbtl 1 and 2
hlrlll are 25 linos OIl the fOnl Ilnd thoae muet be UBtleS for 25 clients 9 one ior bullbull 01 I ini
ot ~h lc II ol1cM lOlivpound til e linic before soeinc DurOI or doc tor ilnc ii hox rristrltltion nUlJbet had alrearll been recorded on the Dai 1y Roiuter then n line ~hollld be drawn through that entry an1 the eliort nust not 06 includttd in tho totals tor that 0eDion
1lw Ileifitration Num)~r of cueh client must be IiIritten IS n 5-dlrlt oode ClhnC IH11IlElr 315 1IIU8 tborotore be enterod 18J010117]5]
~ Clt ZOt
Coda 1 Codo
10 ~tl c 2t j co 21)
~w elSe - Coda 1 0) d CltaEl - Code 2 Revislt Code 3
Only pound1 01 theBe coiles may be usod
11 prol-O~ ~Eil~1 (cc 22)
If ma climt was L drop-out IIho haoS returned now to the Clinio tor tho first no linmiddot bullwin lt1ro1eo o t he or she should be given CCe 1 It this do 5 II It nprlly leu this colWlln blank
u Hothod middothisllill loe 23)
NOh til t otly ~ Cod 16 tp he ontered in 2lpound of the columna oven thOUGh 10 co11lllJlB 10 provided on the torm The Codes llrol-
Oral Contraceptive Code 0 1 U D Code 1 Condom plUD Codo Z Condor (only) Code 3 Foum tAblets cream Code it DitphrClGJII Code 5 Rhythm Cde 6 Injectible Code 7 Advice Code 8 Other Code 9
It for middotDo-le 1 client rlllll ji yen cclldorls ord foam or creall Iou Qust entor Coole i (condom plulJ) in the appropri~te column This Quat be the only lIotmiddot) tarcie If an in the cnse of a tlnle clinic I the client is Bup)lieu lith COIlOrW only you rmot entEr CorlQ 3 (cpndolll) Do not use a ticII ~ tho (odo Nwber
It is CUi tomary fur 11 cliont 110 is beine put on the oral contraceptive for the first tiT1o and even on other occasionn be issued condoms and 11 crelle or foam a Ilell rI3 a pgtcket of pilla In such Cllses when the piDQ Ilre Ilctually iouou you tlust record Orll (Co~e 0) 08 tho onll metbod ilo othor ntry sll0uld ho nnrlo
Uovever n SJC~ canas vucru condoms and fOHa ~rc eiven but no pilJa (even thoJRh _t _n the intention to issue pills nt the noxt vioit) than the Mothol Th5 ifli t ohoulcl be recorded uo Condor Plus (Code 2)
13 Seen Bybullbullbullbullbull
~rot S-1 SO l
Doctor (Dr) - Code 1 j Nurse (Nul ) - Code 2
Clark (Olk-) - Code If tho Clhnt is vcen hy both tho llootor tlnd the Nurse enter Code 1 t Doctor It 6~61l by the Nurso only arite Code 2 Cod bullbull Cerk is l)llnt for FA Cllnica Clerks in tho Government Cli1t hiwo Llttoll istructed not to i56uo supplios on their own volition
14 fl221~
lhio S~tiCl of -Ie fvrtl t~ke 16 (llrci coluMna (cc 25-+0) nnd 10 tho only part at th iOIQ in llich iore thAn one cod is Zlccoptl1blo Tho purpoco of the )ecton is to 0 able to arrive nt the Cjunntity of 6tock dilltlitJutshyed YOI IIlUdt writo in the CllllOjH-iata colulna the nUllbJr of Il1ch 4rtic1o i~JSu~d ~lo e ha I Oral Contrcilpti vea are aub-di vi dod into types ae_ 3 PIllCKC 9 0 Elynnn LlUot be entered Codo in card column 25
If tor eXllrplc t l cliunt is iosued wi th packots of Zucynon nnd aJ(1 ~ivn 1 conuotll (8inoloo) you ouot enter in oard column 25 and 11 It
cnrd col~8 )2 and J (io 1 in card colucn 2 nnd 2 1n card coluun 33) Nota C)lldoIlU ale to b(t ruoordod individually not os packots of throo) Should n ne LlondoClo be isoued thil3 is to be rc-Qed as 09
If It clint 6 t~ot isoued Blly lIupplies thon you must writo Codo 1 in CQllAlilD 41
It Q eli nt isite the clinic to check on her LUD or her Diaphra~t IUId ro DI W 6 ppl ills nre ispounducd then Code 1 1s wri t ten in column 40
In the FA clinios here a variety ot orll contraceptiveo in orer~l tho elerll wilmiddot~ bJ provided with a specill code shoot The idontifyin coo will b wiittn in Column 29 nnd the nUlber of packets iosued in colwm )0
lralaer-In Code 1 lrllllsie r~ut Coda 2 leIllPQrArr Trnnsfer-In Codo gt
In the cao of n 2ratl8fcr-In I you lUot n160 cOrlpleto coluons 42-51
In the cllU J of A ~~emporary TranGfor-1n (an individual who i8 only v1citing fur clinic tor some epecial trcatcont hna who will bo rdnlnin
~middot(II~~~fO~l~SIl~I3~nn~~~h~rO~nh~1~~190~~nll 2-46 and ler rei IItrntion numbu in colullnll41-51
It the oli( nt i iNt a CrllnoforwIu - Out or loClporu1 tMn loave oolumn 1 blank
16 lr4nst(gtr-tl2~~morrry TilJnder-In (co 42-51) Forl1ltl CUn E1~ (cc 112-46)
hen you rei iatlr L irllsfcrln or Il TJlporary Trnnsfer-In you IIIUBt write I ere the five-digit clinio nucbor of the Clinic iraQ which tho ltlient Me (uIlO
2mer ]letr ~2n ~ (cc 47-51)
frlta fllao Clo r-~itrlltion Nuc~Er ot the client in the Former Clinic (i c bullbull th 1 Sis rnmiddotion ~UlIlh()r which the client carrics 1n the tormor clinio) bull
It tho Forrltl Ho( ist rntion Number iIJ not readily wnilnble you tluct oocpluto thtl epcciol [orlll Transfer-In Not Identifiod Dy Forrlcr RCGi(trn~ t10n Nwlbvr Or ~ flt)rCl is to be cOlplctcd for och cnso nnd th forlJO Ilubmi tted to thu )opllntion Prorrnnme Of fice tOGether with tho Dily Ro~iBtors lhwev~r should the clork leuTI of tho clint B FormlI Uocintra tion lUlllb r )0[(10 Cubmi ttinft the D1ily IOCI otro t hen the nUQbcr shoulo bo -ri ton in colucns 47-51 lna the special foro should lJo deotroyotl
l7 bullbullbullbullbull
r lt bull bull
ADXI ) Pap S ot S
11 UD LV~ (cc 525)
It tb( cliont io ~ivQn An IUD tor the firot tl~o then you should Sri to Codo 1 Inuort ill colurJI 52
It tho olimiddotsnt ia rvinGgtrtltld i th An I UD bullbull tben wse Coda 2 RelnDltlrt shyin (01Uil11 52
It the clLmt is ~tte~~dint chnic beruse her IUD CflClQ out by Haol (cxpll Iion i ~hcn fir te todo ~- UIlllrli1 53~
If c-ltr IU fj IIIS reov in -ne cllnic by tho doctor or nurso t~on vlritI Codec in column 5
II the eli nt otends eiLlie tld explin[l th(lt she rccovcd the IUD tlllleel nen write Coda H in Colwlm 53
It the IUD jr still within the uterus nd the WOIraquoI1 1 11rc6llJlnt thon lIrite 1gt40 4 in Column 53
lZ np h5t (ce 54) It 0 Pull 5mor ie t~ken durin thi visit tben Codo 1 ehould be ampDtere4 in ColWlln 54 Should he c110nt lltt rQ(uircd to rttturn to clin1c for a rogtol1t Pnl) t06t then CoLe 2 llhould bo middotwrittcn in column 54
It no Pllp Scou io taken tde visit Itove colUQn 54 blank
Iraferti1lli (CQ 55)
Ii the e liett io nl1 infortili tr eaoe use Cor1o Ill in colUQn 55
If tbia 1000 not tlpl lonve column 55 blonk
20 Totaltll
CO~1ploete the [)ldegO 1gty puti YI tne totals betweon the double lines nt tu b()ttctl Carrj colUlllnc 20 21 nd gt4 Must hlve tho Bnoe JllIIber and thiG Would coreslonc to the numocr ir attencbnco
Writ$ th to1ul nUlllior of Drop-Outs returned (c022)
Urito 41eo tb totnls fOJ each card column 0 to 9 under tho h(adinu Method thiB Vioit Show tho tote L fgtr OlCl type of contraceptive issued (cc 25-40)
1)0 Dot wrLte 1111 totll lUl(Ier Card Columns 15-19 29 41-51
21 COPmllh bull ~lt h~t~ Monthly ROilort
OQ thG DaLl oCator forlll thnt ccrrOspOldB to tho 1(8t 1$06610n lt 0
oth yo Olllt (vwlgtleto the items nt the botto of the [orampl This is tour ontll~1 n(olt nnd includcD tho totll lumber of sesions Ilntl tho total Iluolcr ( r crop-outs durinr the Qonth
An tiUlsilt n drir which n doctor liB in nttcndnncc is a doctor sOfll~1on and shoulc 00 re(liGtcnd in coltns 56-57 All other sessions 1116 conlliid~recl supply stllciona and thtlY 1110 rocordod in columns 58-59
the total Ilum)nl Jf drop-outo ld the drop-outs by method durinc the onth nre 10 bu oltorou in the inrlicllted boxes
72 Chad Your ~
Milke I ura th t all thE fijul4gtu rre c101r -tNever writo our nutlUQrS 50 InrjEl that they oxtend out of tho
ap~rotr1ato ~ox
Cheek to BoJa tht 1111 numuors 1110 in tho correct boxes -- CJslHloially when Writi1 the totlB
Mllxe Cirtc O thmiddott t1e infoT1I1ntion i6 clear on the corbon COllY before sep rmiddotinr the sheets
Jitn the Fomiddotl lien tly sien YOUl nr me 1t the bot tOil right hnnd corner btl forc subol ttinG it Keep tle CL rb n copy for your rocordn
i
-l ________~~---------~
I _1
Adminiatr-atlve SKVieu
P inba ~~~l1cal lrlnbin~~eltltcal -1 te~ra t~~rvicc (lnatittloaa)
--1- - shy -1------------_-L_ l-r-aJiil- shy _-L_tet1lal d
PlIinm1tJ8 atdUon DetalMid H8Il1tb ~ ________bull Care
-----~ Office of i
the FlIily _IPlill3 roarshy
1- - - -------RegiatUll urnr
ltIi 1 Drelttor Rcgicaat Director Souta Tabqo tacallortb ~ counu gt____ ~ (4 ouottet)
Off1ce of the Res10nal Diractoc L
r----- _L_ -- shy i I bull IREgional Ipitl I
District IIttaltb I bull Othn RelOl ond Hcpital CenteIntt itlt j In 1__ _shy-~- ---- -_j
J r Ii~lth
C~nlef
L
I Ihnlth lie I th Offlcu (1ft lc~
Coullty 1I0p1ta1
Henlth tentet
I

- 12 shy
D Decentralization of Powers
414 ~hete is a concentration of administrative and financial powers in the 11in s try of Health I-JllJCi1 results in an accumulation of references in the Miristl) and delays n field operations Specific powers should be delegated ~o (a) the PliO concerned with MCH and family planningmiddot (b) the Directcr o the Program Office (c) the Regional Director and (d) the County Medica1 Oficecs The Ministry should invite suggestions from these officers and wOlk 01t a schedule of delegated powers
415 A tdgh priority in the matter of delegation of powers is to arm the Regiond Directors with sufficient administrative and financial authority to implement with expedition the health and family planning programs of the Ministmiddoty 1 thin the areas in their jurisdictions
E Integration of Family Planning wi th Haternal and Child Health Services
416 At present family planning services are being provided at 48 Goverrnent hospitals health centers and health offices by using the full shytime E taf cf these institutions and employing part-time (sessional) doctors nurse~ anI clerks where necessary At 29 of these institutions separate famil cl~nics are held on specified days in the weck some being doctor sessi(ms mel others supply sessions run hy nurses and clerks At the remaining 18 imtit1tions family planning services are combined with antenatal child healtL cr postnatal services The Family Planning Association runs 8 unishypurpoe f am ly planning centers which provide daily services and contribute a 11 t le less than half the total number of new acceptors per year
417 N assessment has b~en marie of the effect of integrated MOl and famil~ p~ nnning services an the recrl1i tment of acceptors nor were ~ data readily avallable for this purpose It may be observed however that in a situation of shortages of trained personnel for health services utilization of the existing health staff and facilitieR for family planning is inevitable parU cllLrl y in the interior where such shortages are more pronounced This underlines the need of evaluation of the integrated xai and family planning progtam for its impact on the number of acceptors Also a study needs to be made of che utilization of medical and pilramedical manpower so that it leads to bdter ~llocation of duties and optimUJl utilization of personnel
418 ile integration of faMily planning into Mcn services has certain advalltages as well as attendant risks The advantages are
a Lbe association of family planning with the care of mothers and children helps project a benevolent image of family planning as a program of family welfare This creates a
- 13 shy
1imate favorab~e to the acceptance of family planning aa lt p-)si tL1e il-Eare rreasure rather than a negative program cE limiting c~ildren
h t elps erlist ~r2tion tf doctars and nurses who as c -~ass enjo tft~ Y)er)et~ a~d confidf~nce of the communities i712~ Eerve
c ~ieD of contact with women
d luni-purposa clhlics for ~lCH and family planning services are onenient for motn~rs who would have to travel considerable (listances to the clinics
e hete is better utilizat1on of Acarce heAlth manpower
419 he limitatio$ of integrating family planning with MCH servicesI
are the posiOili ties of loss of focus on family planning as a high priori ty prograrr ald the diffusion of pol1sibility for its implementation These could tlow ve r he safegurded agaifls t by adopting the following measures
a 11e job descriptions of doctors and nurses should be rewritten 0 include the family planning function
b hE perf0rt1iai1ce of ctoltors and nurses should be judged as much )y tbeir inteceq t in planning ~vork as in maternal and ~hjld care and this should he lade known to them
c )octors and nurses involved in ~CH services should be given middot)rj entation and traIning in famj ly planning and their interest 3UEtained by refresher courses seminars meetings and supplies of literature
d Thl techrical (xpert~ in the Office of the Family Planninl Program should maintain liaison with and guide the field agencies in implementing the family plannin~ program For this purpose schedules shoul d be marle out for periodic field inspections
420 It is suggested that the working of half-a-dozen centers where family plbnnLng services have been integrated wi th MCH sessions should be studiei for ehe purpose of standardizing the methodology of delivery of servicl~ Such a study should include staff strength patient load recoril shykeepills 10middot of patents in the clinic timing and frequency of clinic sesaios ani convenience vf patients
F Voluntary Organizations
421 I i~ internrticri31 expedence that the birth control movement is pion aTC tt volunh[~ JilC S Qltl that hen the national governments step in wi tl cmbi ti 019 prjhns wi thin the sLate welfare system voluntary bodies ieh tteir limited ilsrluces restrict their service activities and shift the emplasi i 0 educedgt (f the community training research and contracepshytive Sf vic not 1l7gtilflblr in he official program or in areas not reached by it In nagni tude and expanse the of ficial program in Trinidad and Tobago has alrad~ orertak~n Ce 101umary program Increasingly it will become the domLnart tartner in the total national program while the voluntary agencies will cOltirlU1~ to receive financial support and encouragement to set up high standaeis If service and explore new areas thus acting as a stimulus and an additi_e tl the official program
G FrOB-ram Infomation
422 Thre is no concurrent evaluation or monitoring of the Program The daa or lq72 flowing in from the clinics month by month have r8Jllsined unprocss~d tn the Program Office The official Annual Report - 1971 Sums up th~ poition as fcllo~s
ITThe Research and Evaluation component continued to be the weakest in the Population Program Although a systen of evaluation had been built into the program the follow-up procedures for analyzing the data and for correcting inshyconsistencies are inadequate Requests were made to extend the staff to establish a more viable unit but by the end of the year no chllnges had been made
423 T1e recording and riporting jJrocedures were revised effective Januery 1972 and there has been a further change recently at the instance of t1e Evaluation Adviser Under the system now established the clinics are lequ Lreurod to maintain the following records
a Family Planning Clinic Case Card - New Cases This was introduced on January 1 1972 and has thirty-one entries giving age parity contraceptive listory pregnancies socio-economic background ource of family planning information and agency for notvat ion bull (Annex 2) The case card is made out in duplicate for each new acceptor and a copy sent to the Program Office
b Daily Regis ter This fs a ne~gt1 form recently introduced in replacement of the old regis ter and is preparen
- 15 shy
ie) ruplicate the original to be transmitted to the Program (fHce and the carbon copy to be retained in the clinic Th~ is a very 121zborute form requiring 36 entries to be aa~ for each Chse nel and old attending a session includin~ (ntries to cit L to contTaceptive supplies issued
AijCleX 3 T~13e fcnnG are required to be sent to the Program lffce in i7JO balches every month the first batch for the i IS fif~eeL days and the second for the remaining part of hE month The trtention is that the data appearing in the ~EZlic daily legis ter forms should be compiled in the Program Office and fed back to the clinics Although it is claimed that this new form has been pretested and is workable ex)erience alone will show whether the majority of clinic cL~rks are able to cope with it in a busy session
bull o now-Ho Card TIlis card is intended to keep track of ac ceptor--It has entries for name addresfI and month fcr which a visit is due for each year
bull Aphabe tical Index This is a card index of clients with aidresses
Each i)at en is given a simple clinic card on which the dates of further appo~utnli rc3 an~ indicated A special fonT[ has been devised for the reporting ot cases unler the Post-IartumPost-Abortal Education and Referral Program
424 J system of monitoring progrRm performance from month to month need to bE develQped as a high priori ty The problem is not so much reshycord ng mc transmission of data by the clinics but its aggregation and proclssi ng in the Program Office every month which at present takes a long time The Statistical Officer should have a statistical assistant to help him Ln I he taflk Monthly progress reports should be available to the Mini H t~ n H(llllth and A11 offt eerlil of the ProKrnm Office so that remedial ac tl m I lAY h(~ tuk~n n rll1u- WhOnh1f ~Hfl(AlJtlaTY
42 For the analysis of data and evaluation the Program office shouln haVE th(~ full-time services of a trained demographer
H Field Workers
42) Tie Program nemiddotis tne services of a cadre of field workers to enr)ll neii aceeptoTs follow up acceptors in their homes and revive the int 2remiddott of dropouts Such a category of workers could also be utilizerl for pr1fficting other health programs such as the VD campaign and the inmuni~ation program
47 As an experimental measure one field ~]orker may be assigned to a emi l~ of Hi 000 population This would mean 100 field workers in all
- 16 shy
Earh of the workers should preferably have harl a higher secondary education otherwLe 1gt junior secondalY education They should be married persons with middoti1ltt mot tl-an two or tlree children recruited from the locali ty in which they armiddot~ requlred to function Only persons who have the capaci ty to comnunl at~ and or6anl~e should c chosen A months ini tial orientation
slcu1d enable them to start functioning in the field though reshyfresher CO rSeS tvould be necesslt1ry in due course In Port-of-Spain married mer~ a1C women may be employed on a part-time basis
I Hanagement Study
428 A nanagement study of the Family Planning Program should include a sctu iny of the top m~nagement Atructure (Population Council - Office of the Fanil) PLanning Program - Principal Medical Officer for MCH and Family Planni Ig fetices) the field structure for the delivery of family planning servics (Re0ional Director - District Health Services) including the utilizlti(n if medical and paramedical personnel for adding the function of del ve y )f family planning services and the control and communication proCed1reF Lfnking the top management with the field structure
429 The management consultants may study the functioning of the Popul tio I Council and advise whether it adequately serves the purpose of givini po Licy direction to the Program and if not what changes in its compo itt m and operating procedures may be introduced without altering its bsic craracter as an advisory agency The consultants may suggest an alern at ve form of organizati)n and utilization of personnel which in thir p nion may be better adapted to the needs of the Program
430 Irrespective of whether the Population Council is maintained or it is replaced by an agency of a different character a formation like the Offic of be Family Planning Program would be necessary for the administrashytion i)f 1 he program a task for which i 1 appears inadequately equipped at preselt Its obvious requirements are in the areas of program monitoring and el7alnation program supervision communication and training The manag ememiddotlt consultants may study the structure and procedures of this form~ tio Gnd make suggestions with regard to the augmentation of professional and ~ upp)rt lng staffgt and modification of operating procedures
431 The linkage of the Office of the Family Planning Program with the Miniutry of Health (Central Office) and the District Health Services should be sudied In view of the policy of the Government to integrate MCH and faI11iLy rlallning services it should be examined whether the Principal Medi al Officer for Communi ty Heal th Services (MCH and Family Planning) should be agtpoj nt~d as the Chief of the Office of the Family Planning Program and an adTlilistrative officer of a suitable level inducted in that Office to assist him TIle implication of this suggestion is that the head of the Family PlanJling Program would control the District Health Services
- 17 shy
432 rf 1e management consultants should examine the delegation of adminshyistratiie Bld financial powers of the Ministry of Health to different levels of Progam aclrlirdstration viz bull PMO Program Office Regional Director and County ~djca~ Officers
l33 he system of 01 af Togram information from the clinlcs to the Pr()~ra1 O~fice and tOile processing and use of information in the latter office iholld )e studied
434 he working procedures at the integrated McP and family planning clinics shnuLl be studied This would involve a study of each stage which a clien tpcticmt has to go through from the point of entry to the point of exit after receiving advice service or supplies This study shoulci lead to star dartization of procedures and functions and evolution of -lork norms CognatE st tdies of the working procedures at uni-purpose family planning clinics and su~ply SEssions should also be undertaken An essential component of these ~ tad ~es would be to examine Nhich functions currently performed by docshytors lealh visitors nurses and midives respectively hav~ become so roushytinize ttl it they can he relegated (0 the next 10Her level
435 Reated to working procedures is the problem of job description of medcal 8nd parrunedical personnel involved in family planning from the centra i tc the field level This job description needs to be studied wi th a vie VIW8Id txaminiDg the uttlization of skills and allocation of time by the staff lcc(rd~ng to the functional prj ori ties
436 frV management consultants should study the workings of the curren slralgements fOJ family planning counselling under the Post-Partul11 Post-Abortal Education and Referral Program at the Port-of-Spain and San Fenaldo General Hospitals
437 SU1ect to the ItBrcement of the Gove1nment the management conshy8ultal ts ~hOLlld undertake a study of th requirement of field workers (home vinitcru) in tmtlUI of are nnd population cov(ra~e
ANNEX 1
Names of Persons Met
Ii Mr T C Taitt Pem1(H~nt 3~crtarY) Ministry of Health
2 Dr M n Henry Chitd Medical Officer Ministry of Health
Ellubeth Quam a Prindpal Medical Officer (1S)
4 Mr G Z Jaine ~ uJiector Population Council
5 Dr Norma Andrews Medical Officer Population Council
6 Mr Jc~n Coury~ Evaluation Adviser Population Council
7 Mr A Jriseph Principal Statistical Officer Population Council
8 Dr C 0 Colman Country Representative Pan American Health )rg ni~ation
9 Mr ranca Kippel Health Education Specialist Ministry of Iea th
10 (1 bullbullines Principal Nursing Officer Ministry of Health
11 Dr Mx won (formerlyHinistry of Health)
12 M3 late Carops Ex-Chairman of Population Council
--
4i 1_ middotIIlt F-ntCWclOotf_Y v OJ t tl
GOVIIlHMEIgt(I OF TINIOAD AND TOampAGQ - NNISTJY OF HIALftf AIJIE1 2NATIONAL FAMilY PLANNING PROGRAMME
F MIL Y PLANNING CUNIC CASE CARD - NEW CASES - NFPPl
li ~~___ 1 ________
~ ecll-U
-- --------------------- shy~) ~~middot~------------------~~~~~~---CIJ------ middot~ii--middot-middot----middot-middot---middot--------- shy
ltv Writt N_ 01(111________________
a ~4itiJtmiddotl_____ ilIIIltIoI~____~____~-__----- shybull ~4
fie l$ - JO tDql IIfIA- tr-JMimiddot _ iJ 1 Odoor o
14aorielaquol_ _~ 0 lio witIleo-La ~ 01 bull - OJ ( _01 1~ltgt1lh o bull- 0$
AacJcu 0 2 CIIriIWA 0 J Os 0
Yv~MONTH ltnollOf~nfIGHTI
Undu 1100U$ Utgtdn 5SCI Undu 11200 01 ~ 50 - 9949 amp100 - 1199 02UlOO - nn9E~ (
0)~ 10- $99 SiOO -- U9~ lOO -- U99 12400 - 1359)-------_-r----shy ~l)o SIS n600 - Hm1300 -- 019 OJ200 il~9 ~------ 99~ a 1)0 m Os1)00 -- l99 1400 -shy $4100 -- 1S999r--- shy
1500 donl S6000aad O399 - lt499I~- I 0lt
ltII
IJ -IC _~tltlioltgti lS
02 IaampJIIocI OJ 04 laM Os
w Oltwio I_-l(~u IrIaa U
h~~ ~Clubl 01 OJ
IS ~C-n 01 toSIitDI 02
Ji poundI on 01 IriIIIuy M ur 02 IV OJ
WU 10 pltIoII~ llaMtl 411 cIIiId 01 Ol it fIolto ~ do~ _14 rou IIlgtJo 1Ia1 ___~_ shy
40
It _ I 00 ~bull FPIiIJ 1
OJ 02 OJ 06
)0 III- iy wOWcf ~1
aMIIl Os
11 T 1gtlt ( h _______ 4)~
06
04 (MIbullbull middot bIrlI ~___~__~_ (-fIJI ~- -~-- (1HJ 49middot SJ
U 10k 01( 1__ raquo$-4
iU1) DOl F ToWotfOlnC DOl 001 or Do [IP 006 001 OIIgtu___Spltclty DOll Nltmo 010
U1Mo I orcpmiddot laquo55middot16
1lD 001 Foam Toblelf_ICim DOl Condom DOl CoomS~ 004 oe Oos WlttuJn 1J OIkr DSpody) 101~ ~Iu 006 Rhylhm 001 DOG OJO
no wI~lmm 4 cd
(I 0) 1110 01 Condor 03 (lorn bull l S~muoidIl 04 Faa TabioolfIIltr- Os RhyUlm 01 lnJrl tible O Advico 090 06
la slt 1)0 19 loti ~rltnlt) ([)sl or 1llOn) ____ --__ bullbully-J n SV - ~JcdS
v~ Cl NCI 0 30 OJI_O I Wr blJ1h 0 I ~ OJ 1 ~ (fOOd V 01 No 02 laquo 6) Cf4
WIiI 1 172
004 001
j D middotmiddot middot
1 ~
r
~
bull I
bullI I I
r c i
ANNEX 3 Pagemiddot 1 of 5
0 raquo rshy -lt l)J ~ 111 t G) 5 shy (J) ~ -
fT1u
i
MINISTTY OF Ho1TH
NTIONl F~ILY LNNING PR-GRbullbullM-tE
~~5tructions to C11nic ClerKa
How to co~ploto the Daily Rogister
~~ ~~v1sd Daily Rosi8ter replnc~D tho one which is now in use tb$ Monthly PC~ri rOt~ arti tho 01( Ci() Dod PollJ j f m It is a pre-coded form and 1411 cl~1p Jd tl a1I6iniul-mIHvn Oel Clinic nctivi~y
110 )rm rollt biJ coupJot)d lrl cupLtcoto using a o(roon shoot Tho top aheot or oriinai ~ust bl) 6(Ult to tho CQgt1tral O[[lCO and tho carbon copy retained in the Gliaic rilo dll the for6a that ar uD~d betwoen the 1st 4nd the 15th of the oIIollth aut bo subClittud tocho office 35 Lnc blttch Those oomp1cted betwoon tho 16th _lid tqemc of tho month must bo ~cnt in a secJnll batch
P lOvLior hns boon Illllde for 25 clients on cZlch forlll new forlll must b IIlied f r poundh 50[810n2 whothur or not ono or lIIore session are hoIdiit the clinic on he sarne day
I th ro alO more htl 25 clionta 1n attondnnco at tho session the additi shyOhAl m~bOl of clionts 10 clients nu~ber 26 27 etc sh0u1l be ontered on the next Imiddotrlll ~i ttout a1tpoundring the numbtlrs in the cvlumn hond Series
51 ppOfil th~ number of aUcnts lQr that session ws 5 this would mean thllt two rJlS ~ lst be 6ubllIitt~dl the first filled uF 1 tltgt 25 And the laquoIncond 1 to 10 Th~ cal bon ofies should bo st~plod togother at thu t0P l~rt h4nd corner of the torm ard ktpt in the Clinic filo lou IIlU6t stapl~ the originftls in the 8~~ monnshyer for lIub~ssion to the ofticl
ie h~ ll idontiflctior- (cc 1 - )
0 lot Ji 9 anythin~ hGro poundhia is int(mdClc for tha computer code
2 ~~pound~ - Print clOflrly tho name of your Clinic
C1Lic Huml or - (cc 4 - 8) Evar1 Clinic Numbor has 5 digits Virite each dig t il a t$purate box
It Pai~_thllsectgdllion (00 lt) -1 1) - Dl monll 10M
lw) bolte IlrO proY140d fetr olAoh pr 01 thQ dISh Enter tho dA) ldns a R
d16ih
emiddot5middot (0 11 I for 115t ( 0 21 for 5th etc Treat month the am pay
e ~ 10 ~ I for I-hrch 0 [2] for September Tho y~nr must be (into ad
I Z I ~ I I 71 q etc
Take as in IixulIple tho dOlte 3rd tllrch 1973 7~ie must bo written
[0131 LSLDI[7l3JDny Month Ye~r
5middot 1~J $~~ - Irom ~-------- To --------shytntol hOI II the time the Clinic 111118 in SW5sion emiddot8middot
(i) 11011 500 lm To 1200 non
(11) Frclt 100 pm To 400 pm
(iii ) IX-OG OO pllI To 6~00 pm
f
2
ADEJ ) Paae ) of S
6 Eov
_ 1hA 1gtIpoundC iIIUlt be nu~o7Ifd tler1ally 1 throurh n lU tbey Are Wled In ~1l8ellJ IInel 1301 tlU 1 Orcl 1 Wled tor a o5038ioll - -I 2 tonY tho _boul~ b I1WJbtl 1 and 2
hlrlll are 25 linos OIl the fOnl Ilnd thoae muet be UBtleS for 25 clients 9 one ior bullbull 01 I ini
ot ~h lc II ol1cM lOlivpound til e linic before soeinc DurOI or doc tor ilnc ii hox rristrltltion nUlJbet had alrearll been recorded on the Dai 1y Roiuter then n line ~hollld be drawn through that entry an1 the eliort nust not 06 includttd in tho totals tor that 0eDion
1lw Ileifitration Num)~r of cueh client must be IiIritten IS n 5-dlrlt oode ClhnC IH11IlElr 315 1IIU8 tborotore be enterod 18J010117]5]
~ Clt ZOt
Coda 1 Codo
10 ~tl c 2t j co 21)
~w elSe - Coda 1 0) d CltaEl - Code 2 Revislt Code 3
Only pound1 01 theBe coiles may be usod
11 prol-O~ ~Eil~1 (cc 22)
If ma climt was L drop-out IIho haoS returned now to the Clinio tor tho first no linmiddot bullwin lt1ro1eo o t he or she should be given CCe 1 It this do 5 II It nprlly leu this colWlln blank
u Hothod middothisllill loe 23)
NOh til t otly ~ Cod 16 tp he ontered in 2lpound of the columna oven thOUGh 10 co11lllJlB 10 provided on the torm The Codes llrol-
Oral Contraceptive Code 0 1 U D Code 1 Condom plUD Codo Z Condor (only) Code 3 Foum tAblets cream Code it DitphrClGJII Code 5 Rhythm Cde 6 Injectible Code 7 Advice Code 8 Other Code 9
It for middotDo-le 1 client rlllll ji yen cclldorls ord foam or creall Iou Qust entor Coole i (condom plulJ) in the appropri~te column This Quat be the only lIotmiddot) tarcie If an in the cnse of a tlnle clinic I the client is Bup)lieu lith COIlOrW only you rmot entEr CorlQ 3 (cpndolll) Do not use a ticII ~ tho (odo Nwber
It is CUi tomary fur 11 cliont 110 is beine put on the oral contraceptive for the first tiT1o and even on other occasionn be issued condoms and 11 crelle or foam a Ilell rI3 a pgtcket of pilla In such Cllses when the piDQ Ilre Ilctually iouou you tlust record Orll (Co~e 0) 08 tho onll metbod ilo othor ntry sll0uld ho nnrlo
Uovever n SJC~ canas vucru condoms and fOHa ~rc eiven but no pilJa (even thoJRh _t _n the intention to issue pills nt the noxt vioit) than the Mothol Th5 ifli t ohoulcl be recorded uo Condor Plus (Code 2)
13 Seen Bybullbullbullbullbull
~rot S-1 SO l
Doctor (Dr) - Code 1 j Nurse (Nul ) - Code 2
Clark (Olk-) - Code If tho Clhnt is vcen hy both tho llootor tlnd the Nurse enter Code 1 t Doctor It 6~61l by the Nurso only arite Code 2 Cod bullbull Cerk is l)llnt for FA Cllnica Clerks in tho Government Cli1t hiwo Llttoll istructed not to i56uo supplios on their own volition
14 fl221~
lhio S~tiCl of -Ie fvrtl t~ke 16 (llrci coluMna (cc 25-+0) nnd 10 tho only part at th iOIQ in llich iore thAn one cod is Zlccoptl1blo Tho purpoco of the )ecton is to 0 able to arrive nt the Cjunntity of 6tock dilltlitJutshyed YOI IIlUdt writo in the CllllOjH-iata colulna the nUllbJr of Il1ch 4rtic1o i~JSu~d ~lo e ha I Oral Contrcilpti vea are aub-di vi dod into types ae_ 3 PIllCKC 9 0 Elynnn LlUot be entered Codo in card column 25
If tor eXllrplc t l cliunt is iosued wi th packots of Zucynon nnd aJ(1 ~ivn 1 conuotll (8inoloo) you ouot enter in oard column 25 and 11 It
cnrd col~8 )2 and J (io 1 in card colucn 2 nnd 2 1n card coluun 33) Nota C)lldoIlU ale to b(t ruoordod individually not os packots of throo) Should n ne LlondoClo be isoued thil3 is to be rc-Qed as 09
If It clint 6 t~ot isoued Blly lIupplies thon you must writo Codo 1 in CQllAlilD 41
It Q eli nt isite the clinic to check on her LUD or her Diaphra~t IUId ro DI W 6 ppl ills nre ispounducd then Code 1 1s wri t ten in column 40
In the FA clinios here a variety ot orll contraceptiveo in orer~l tho elerll wilmiddot~ bJ provided with a specill code shoot The idontifyin coo will b wiittn in Column 29 nnd the nUlber of packets iosued in colwm )0
lralaer-In Code 1 lrllllsie r~ut Coda 2 leIllPQrArr Trnnsfer-In Codo gt
In the cao of n 2ratl8fcr-In I you lUot n160 cOrlpleto coluons 42-51
In the cllU J of A ~~emporary TranGfor-1n (an individual who i8 only v1citing fur clinic tor some epecial trcatcont hna who will bo rdnlnin
~middot(II~~~fO~l~SIl~I3~nn~~~h~rO~nh~1~~190~~nll 2-46 and ler rei IItrntion numbu in colullnll41-51
It the oli( nt i iNt a CrllnoforwIu - Out or loClporu1 tMn loave oolumn 1 blank
16 lr4nst(gtr-tl2~~morrry TilJnder-In (co 42-51) Forl1ltl CUn E1~ (cc 112-46)
hen you rei iatlr L irllsfcrln or Il TJlporary Trnnsfer-In you IIIUBt write I ere the five-digit clinio nucbor of the Clinic iraQ which tho ltlient Me (uIlO
2mer ]letr ~2n ~ (cc 47-51)
frlta fllao Clo r-~itrlltion Nuc~Er ot the client in the Former Clinic (i c bullbull th 1 Sis rnmiddotion ~UlIlh()r which the client carrics 1n the tormor clinio) bull
It tho Forrltl Ho( ist rntion Number iIJ not readily wnilnble you tluct oocpluto thtl epcciol [orlll Transfer-In Not Identifiod Dy Forrlcr RCGi(trn~ t10n Nwlbvr Or ~ flt)rCl is to be cOlplctcd for och cnso nnd th forlJO Ilubmi tted to thu )opllntion Prorrnnme Of fice tOGether with tho Dily Ro~iBtors lhwev~r should the clork leuTI of tho clint B FormlI Uocintra tion lUlllb r )0[(10 Cubmi ttinft the D1ily IOCI otro t hen the nUQbcr shoulo bo -ri ton in colucns 47-51 lna the special foro should lJo deotroyotl
l7 bullbullbullbullbull
r lt bull bull
ADXI ) Pap S ot S
11 UD LV~ (cc 525)
It tb( cliont io ~ivQn An IUD tor the firot tl~o then you should Sri to Codo 1 Inuort ill colurJI 52
It tho olimiddotsnt ia rvinGgtrtltld i th An I UD bullbull tben wse Coda 2 RelnDltlrt shyin (01Uil11 52
It the clLmt is ~tte~~dint chnic beruse her IUD CflClQ out by Haol (cxpll Iion i ~hcn fir te todo ~- UIlllrli1 53~
If c-ltr IU fj IIIS reov in -ne cllnic by tho doctor or nurso t~on vlritI Codec in column 5
II the eli nt otends eiLlie tld explin[l th(lt she rccovcd the IUD tlllleel nen write Coda H in Colwlm 53
It the IUD jr still within the uterus nd the WOIraquoI1 1 11rc6llJlnt thon lIrite 1gt40 4 in Column 53
lZ np h5t (ce 54) It 0 Pull 5mor ie t~ken durin thi visit tben Codo 1 ehould be ampDtere4 in ColWlln 54 Should he c110nt lltt rQ(uircd to rttturn to clin1c for a rogtol1t Pnl) t06t then CoLe 2 llhould bo middotwrittcn in column 54
It no Pllp Scou io taken tde visit Itove colUQn 54 blank
Iraferti1lli (CQ 55)
Ii the e liett io nl1 infortili tr eaoe use Cor1o Ill in colUQn 55
If tbia 1000 not tlpl lonve column 55 blonk
20 Totaltll
CO~1ploete the [)ldegO 1gty puti YI tne totals betweon the double lines nt tu b()ttctl Carrj colUlllnc 20 21 nd gt4 Must hlve tho Bnoe JllIIber and thiG Would coreslonc to the numocr ir attencbnco
Writ$ th to1ul nUlllior of Drop-Outs returned (c022)
Urito 41eo tb totnls fOJ each card column 0 to 9 under tho h(adinu Method thiB Vioit Show tho tote L fgtr OlCl type of contraceptive issued (cc 25-40)
1)0 Dot wrLte 1111 totll lUl(Ier Card Columns 15-19 29 41-51
21 COPmllh bull ~lt h~t~ Monthly ROilort
OQ thG DaLl oCator forlll thnt ccrrOspOldB to tho 1(8t 1$06610n lt 0
oth yo Olllt (vwlgtleto the items nt the botto of the [orampl This is tour ontll~1 n(olt nnd includcD tho totll lumber of sesions Ilntl tho total Iluolcr ( r crop-outs durinr the Qonth
An tiUlsilt n drir which n doctor liB in nttcndnncc is a doctor sOfll~1on and shoulc 00 re(liGtcnd in coltns 56-57 All other sessions 1116 conlliid~recl supply stllciona and thtlY 1110 rocordod in columns 58-59
the total Ilum)nl Jf drop-outo ld the drop-outs by method durinc the onth nre 10 bu oltorou in the inrlicllted boxes
72 Chad Your ~
Milke I ura th t all thE fijul4gtu rre c101r -tNever writo our nutlUQrS 50 InrjEl that they oxtend out of tho
ap~rotr1ato ~ox
Cheek to BoJa tht 1111 numuors 1110 in tho correct boxes -- CJslHloially when Writi1 the totlB
Mllxe Cirtc O thmiddott t1e infoT1I1ntion i6 clear on the corbon COllY before sep rmiddotinr the sheets
Jitn the Fomiddotl lien tly sien YOUl nr me 1t the bot tOil right hnnd corner btl forc subol ttinG it Keep tle CL rb n copy for your rocordn
i
-l ________~~---------~
I _1
Adminiatr-atlve SKVieu
P inba ~~~l1cal lrlnbin~~eltltcal -1 te~ra t~~rvicc (lnatittloaa)
--1- - shy -1------------_-L_ l-r-aJiil- shy _-L_tet1lal d
PlIinm1tJ8 atdUon DetalMid H8Il1tb ~ ________bull Care
-----~ Office of i
the FlIily _IPlill3 roarshy
1- - - -------RegiatUll urnr
ltIi 1 Drelttor Rcgicaat Director Souta Tabqo tacallortb ~ counu gt____ ~ (4 ouottet)
Off1ce of the Res10nal Diractoc L
r----- _L_ -- shy i I bull IREgional Ipitl I
District IIttaltb I bull Othn RelOl ond Hcpital CenteIntt itlt j In 1__ _shy-~- ---- -_j
J r Ii~lth
C~nlef
L
I Ihnlth lie I th Offlcu (1ft lc~
Coullty 1I0p1ta1
Henlth tentet
I

- 13 shy
1imate favorab~e to the acceptance of family planning aa lt p-)si tL1e il-Eare rreasure rather than a negative program cE limiting c~ildren
h t elps erlist ~r2tion tf doctars and nurses who as c -~ass enjo tft~ Y)er)et~ a~d confidf~nce of the communities i712~ Eerve
c ~ieD of contact with women
d luni-purposa clhlics for ~lCH and family planning services are onenient for motn~rs who would have to travel considerable (listances to the clinics
e hete is better utilizat1on of Acarce heAlth manpower
419 he limitatio$ of integrating family planning with MCH servicesI
are the posiOili ties of loss of focus on family planning as a high priori ty prograrr ald the diffusion of pol1sibility for its implementation These could tlow ve r he safegurded agaifls t by adopting the following measures
a 11e job descriptions of doctors and nurses should be rewritten 0 include the family planning function
b hE perf0rt1iai1ce of ctoltors and nurses should be judged as much )y tbeir inteceq t in planning ~vork as in maternal and ~hjld care and this should he lade known to them
c )octors and nurses involved in ~CH services should be given middot)rj entation and traIning in famj ly planning and their interest 3UEtained by refresher courses seminars meetings and supplies of literature
d Thl techrical (xpert~ in the Office of the Family Planninl Program should maintain liaison with and guide the field agencies in implementing the family plannin~ program For this purpose schedules shoul d be marle out for periodic field inspections
420 It is suggested that the working of half-a-dozen centers where family plbnnLng services have been integrated wi th MCH sessions should be studiei for ehe purpose of standardizing the methodology of delivery of servicl~ Such a study should include staff strength patient load recoril shykeepills 10middot of patents in the clinic timing and frequency of clinic sesaios ani convenience vf patients
F Voluntary Organizations
421 I i~ internrticri31 expedence that the birth control movement is pion aTC tt volunh[~ JilC S Qltl that hen the national governments step in wi tl cmbi ti 019 prjhns wi thin the sLate welfare system voluntary bodies ieh tteir limited ilsrluces restrict their service activities and shift the emplasi i 0 educedgt (f the community training research and contracepshytive Sf vic not 1l7gtilflblr in he official program or in areas not reached by it In nagni tude and expanse the of ficial program in Trinidad and Tobago has alrad~ orertak~n Ce 101umary program Increasingly it will become the domLnart tartner in the total national program while the voluntary agencies will cOltirlU1~ to receive financial support and encouragement to set up high standaeis If service and explore new areas thus acting as a stimulus and an additi_e tl the official program
G FrOB-ram Infomation
422 Thre is no concurrent evaluation or monitoring of the Program The daa or lq72 flowing in from the clinics month by month have r8Jllsined unprocss~d tn the Program Office The official Annual Report - 1971 Sums up th~ poition as fcllo~s
ITThe Research and Evaluation component continued to be the weakest in the Population Program Although a systen of evaluation had been built into the program the follow-up procedures for analyzing the data and for correcting inshyconsistencies are inadequate Requests were made to extend the staff to establish a more viable unit but by the end of the year no chllnges had been made
423 T1e recording and riporting jJrocedures were revised effective Januery 1972 and there has been a further change recently at the instance of t1e Evaluation Adviser Under the system now established the clinics are lequ Lreurod to maintain the following records
a Family Planning Clinic Case Card - New Cases This was introduced on January 1 1972 and has thirty-one entries giving age parity contraceptive listory pregnancies socio-economic background ource of family planning information and agency for notvat ion bull (Annex 2) The case card is made out in duplicate for each new acceptor and a copy sent to the Program Office
b Daily Regis ter This fs a ne~gt1 form recently introduced in replacement of the old regis ter and is preparen
- 15 shy
ie) ruplicate the original to be transmitted to the Program (fHce and the carbon copy to be retained in the clinic Th~ is a very 121zborute form requiring 36 entries to be aa~ for each Chse nel and old attending a session includin~ (ntries to cit L to contTaceptive supplies issued
AijCleX 3 T~13e fcnnG are required to be sent to the Program lffce in i7JO balches every month the first batch for the i IS fif~eeL days and the second for the remaining part of hE month The trtention is that the data appearing in the ~EZlic daily legis ter forms should be compiled in the Program Office and fed back to the clinics Although it is claimed that this new form has been pretested and is workable ex)erience alone will show whether the majority of clinic cL~rks are able to cope with it in a busy session
bull o now-Ho Card TIlis card is intended to keep track of ac ceptor--It has entries for name addresfI and month fcr which a visit is due for each year
bull Aphabe tical Index This is a card index of clients with aidresses
Each i)at en is given a simple clinic card on which the dates of further appo~utnli rc3 an~ indicated A special fonT[ has been devised for the reporting ot cases unler the Post-IartumPost-Abortal Education and Referral Program
424 J system of monitoring progrRm performance from month to month need to bE develQped as a high priori ty The problem is not so much reshycord ng mc transmission of data by the clinics but its aggregation and proclssi ng in the Program Office every month which at present takes a long time The Statistical Officer should have a statistical assistant to help him Ln I he taflk Monthly progress reports should be available to the Mini H t~ n H(llllth and A11 offt eerlil of the ProKrnm Office so that remedial ac tl m I lAY h(~ tuk~n n rll1u- WhOnh1f ~Hfl(AlJtlaTY
42 For the analysis of data and evaluation the Program office shouln haVE th(~ full-time services of a trained demographer
H Field Workers
42) Tie Program nemiddotis tne services of a cadre of field workers to enr)ll neii aceeptoTs follow up acceptors in their homes and revive the int 2remiddott of dropouts Such a category of workers could also be utilizerl for pr1fficting other health programs such as the VD campaign and the inmuni~ation program
47 As an experimental measure one field ~]orker may be assigned to a emi l~ of Hi 000 population This would mean 100 field workers in all
- 16 shy
Earh of the workers should preferably have harl a higher secondary education otherwLe 1gt junior secondalY education They should be married persons with middoti1ltt mot tl-an two or tlree children recruited from the locali ty in which they armiddot~ requlred to function Only persons who have the capaci ty to comnunl at~ and or6anl~e should c chosen A months ini tial orientation
slcu1d enable them to start functioning in the field though reshyfresher CO rSeS tvould be necesslt1ry in due course In Port-of-Spain married mer~ a1C women may be employed on a part-time basis
I Hanagement Study
428 A nanagement study of the Family Planning Program should include a sctu iny of the top m~nagement Atructure (Population Council - Office of the Fanil) PLanning Program - Principal Medical Officer for MCH and Family Planni Ig fetices) the field structure for the delivery of family planning servics (Re0ional Director - District Health Services) including the utilizlti(n if medical and paramedical personnel for adding the function of del ve y )f family planning services and the control and communication proCed1reF Lfnking the top management with the field structure
429 The management consultants may study the functioning of the Popul tio I Council and advise whether it adequately serves the purpose of givini po Licy direction to the Program and if not what changes in its compo itt m and operating procedures may be introduced without altering its bsic craracter as an advisory agency The consultants may suggest an alern at ve form of organizati)n and utilization of personnel which in thir p nion may be better adapted to the needs of the Program
430 Irrespective of whether the Population Council is maintained or it is replaced by an agency of a different character a formation like the Offic of be Family Planning Program would be necessary for the administrashytion i)f 1 he program a task for which i 1 appears inadequately equipped at preselt Its obvious requirements are in the areas of program monitoring and el7alnation program supervision communication and training The manag ememiddotlt consultants may study the structure and procedures of this form~ tio Gnd make suggestions with regard to the augmentation of professional and ~ upp)rt lng staffgt and modification of operating procedures
431 The linkage of the Office of the Family Planning Program with the Miniutry of Health (Central Office) and the District Health Services should be sudied In view of the policy of the Government to integrate MCH and faI11iLy rlallning services it should be examined whether the Principal Medi al Officer for Communi ty Heal th Services (MCH and Family Planning) should be agtpoj nt~d as the Chief of the Office of the Family Planning Program and an adTlilistrative officer of a suitable level inducted in that Office to assist him TIle implication of this suggestion is that the head of the Family PlanJling Program would control the District Health Services
- 17 shy
432 rf 1e management consultants should examine the delegation of adminshyistratiie Bld financial powers of the Ministry of Health to different levels of Progam aclrlirdstration viz bull PMO Program Office Regional Director and County ~djca~ Officers
l33 he system of 01 af Togram information from the clinlcs to the Pr()~ra1 O~fice and tOile processing and use of information in the latter office iholld )e studied
434 he working procedures at the integrated McP and family planning clinics shnuLl be studied This would involve a study of each stage which a clien tpcticmt has to go through from the point of entry to the point of exit after receiving advice service or supplies This study shoulci lead to star dartization of procedures and functions and evolution of -lork norms CognatE st tdies of the working procedures at uni-purpose family planning clinics and su~ply SEssions should also be undertaken An essential component of these ~ tad ~es would be to examine Nhich functions currently performed by docshytors lealh visitors nurses and midives respectively hav~ become so roushytinize ttl it they can he relegated (0 the next 10Her level
435 Reated to working procedures is the problem of job description of medcal 8nd parrunedical personnel involved in family planning from the centra i tc the field level This job description needs to be studied wi th a vie VIW8Id txaminiDg the uttlization of skills and allocation of time by the staff lcc(rd~ng to the functional prj ori ties
436 frV management consultants should study the workings of the curren slralgements fOJ family planning counselling under the Post-Partul11 Post-Abortal Education and Referral Program at the Port-of-Spain and San Fenaldo General Hospitals
437 SU1ect to the ItBrcement of the Gove1nment the management conshy8ultal ts ~hOLlld undertake a study of th requirement of field workers (home vinitcru) in tmtlUI of are nnd population cov(ra~e
ANNEX 1
Names of Persons Met
Ii Mr T C Taitt Pem1(H~nt 3~crtarY) Ministry of Health
2 Dr M n Henry Chitd Medical Officer Ministry of Health
Ellubeth Quam a Prindpal Medical Officer (1S)
4 Mr G Z Jaine ~ uJiector Population Council
5 Dr Norma Andrews Medical Officer Population Council
6 Mr Jc~n Coury~ Evaluation Adviser Population Council
7 Mr A Jriseph Principal Statistical Officer Population Council
8 Dr C 0 Colman Country Representative Pan American Health )rg ni~ation
9 Mr ranca Kippel Health Education Specialist Ministry of Iea th
10 (1 bullbullines Principal Nursing Officer Ministry of Health
11 Dr Mx won (formerlyHinistry of Health)
12 M3 late Carops Ex-Chairman of Population Council
--
4i 1_ middotIIlt F-ntCWclOotf_Y v OJ t tl
GOVIIlHMEIgt(I OF TINIOAD AND TOampAGQ - NNISTJY OF HIALftf AIJIE1 2NATIONAL FAMilY PLANNING PROGRAMME
F MIL Y PLANNING CUNIC CASE CARD - NEW CASES - NFPPl
li ~~___ 1 ________
~ ecll-U
-- --------------------- shy~) ~~middot~------------------~~~~~~---CIJ------ middot~ii--middot-middot----middot-middot---middot--------- shy
ltv Writt N_ 01(111________________
a ~4itiJtmiddotl_____ ilIIIltIoI~____~____~-__----- shybull ~4
fie l$ - JO tDql IIfIA- tr-JMimiddot _ iJ 1 Odoor o
14aorielaquol_ _~ 0 lio witIleo-La ~ 01 bull - OJ ( _01 1~ltgt1lh o bull- 0$
AacJcu 0 2 CIIriIWA 0 J Os 0
Yv~MONTH ltnollOf~nfIGHTI
Undu 1100U$ Utgtdn 5SCI Undu 11200 01 ~ 50 - 9949 amp100 - 1199 02UlOO - nn9E~ (
0)~ 10- $99 SiOO -- U9~ lOO -- U99 12400 - 1359)-------_-r----shy ~l)o SIS n600 - Hm1300 -- 019 OJ200 il~9 ~------ 99~ a 1)0 m Os1)00 -- l99 1400 -shy $4100 -- 1S999r--- shy
1500 donl S6000aad O399 - lt499I~- I 0lt
ltII
IJ -IC _~tltlioltgti lS
02 IaampJIIocI OJ 04 laM Os
w Oltwio I_-l(~u IrIaa U
h~~ ~Clubl 01 OJ
IS ~C-n 01 toSIitDI 02
Ji poundI on 01 IriIIIuy M ur 02 IV OJ
WU 10 pltIoII~ llaMtl 411 cIIiId 01 Ol it fIolto ~ do~ _14 rou IIlgtJo 1Ia1 ___~_ shy
40
It _ I 00 ~bull FPIiIJ 1
OJ 02 OJ 06
)0 III- iy wOWcf ~1
aMIIl Os
11 T 1gtlt ( h _______ 4)~
06
04 (MIbullbull middot bIrlI ~___~__~_ (-fIJI ~- -~-- (1HJ 49middot SJ
U 10k 01( 1__ raquo$-4
iU1) DOl F ToWotfOlnC DOl 001 or Do [IP 006 001 OIIgtu___Spltclty DOll Nltmo 010
U1Mo I orcpmiddot laquo55middot16
1lD 001 Foam Toblelf_ICim DOl Condom DOl CoomS~ 004 oe Oos WlttuJn 1J OIkr DSpody) 101~ ~Iu 006 Rhylhm 001 DOG OJO
no wI~lmm 4 cd
(I 0) 1110 01 Condor 03 (lorn bull l S~muoidIl 04 Faa TabioolfIIltr- Os RhyUlm 01 lnJrl tible O Advico 090 06
la slt 1)0 19 loti ~rltnlt) ([)sl or 1llOn) ____ --__ bullbully-J n SV - ~JcdS
v~ Cl NCI 0 30 OJI_O I Wr blJ1h 0 I ~ OJ 1 ~ (fOOd V 01 No 02 laquo 6) Cf4
WIiI 1 172
004 001
j D middotmiddot middot
1 ~
r
~
bull I
bullI I I
r c i
ANNEX 3 Pagemiddot 1 of 5
0 raquo rshy -lt l)J ~ 111 t G) 5 shy (J) ~ -
fT1u
i
MINISTTY OF Ho1TH
NTIONl F~ILY LNNING PR-GRbullbullM-tE
~~5tructions to C11nic ClerKa
How to co~ploto the Daily Rogister
~~ ~~v1sd Daily Rosi8ter replnc~D tho one which is now in use tb$ Monthly PC~ri rOt~ arti tho 01( Ci() Dod PollJ j f m It is a pre-coded form and 1411 cl~1p Jd tl a1I6iniul-mIHvn Oel Clinic nctivi~y
110 )rm rollt biJ coupJot)d lrl cupLtcoto using a o(roon shoot Tho top aheot or oriinai ~ust bl) 6(Ult to tho CQgt1tral O[[lCO and tho carbon copy retained in the Gliaic rilo dll the for6a that ar uD~d betwoen the 1st 4nd the 15th of the oIIollth aut bo subClittud tocho office 35 Lnc blttch Those oomp1cted betwoon tho 16th _lid tqemc of tho month must bo ~cnt in a secJnll batch
P lOvLior hns boon Illllde for 25 clients on cZlch forlll new forlll must b IIlied f r poundh 50[810n2 whothur or not ono or lIIore session are hoIdiit the clinic on he sarne day
I th ro alO more htl 25 clionta 1n attondnnco at tho session the additi shyOhAl m~bOl of clionts 10 clients nu~ber 26 27 etc sh0u1l be ontered on the next Imiddotrlll ~i ttout a1tpoundring the numbtlrs in the cvlumn hond Series
51 ppOfil th~ number of aUcnts lQr that session ws 5 this would mean thllt two rJlS ~ lst be 6ubllIitt~dl the first filled uF 1 tltgt 25 And the laquoIncond 1 to 10 Th~ cal bon ofies should bo st~plod togother at thu t0P l~rt h4nd corner of the torm ard ktpt in the Clinic filo lou IIlU6t stapl~ the originftls in the 8~~ monnshyer for lIub~ssion to the ofticl
ie h~ ll idontiflctior- (cc 1 - )
0 lot Ji 9 anythin~ hGro poundhia is int(mdClc for tha computer code
2 ~~pound~ - Print clOflrly tho name of your Clinic
C1Lic Huml or - (cc 4 - 8) Evar1 Clinic Numbor has 5 digits Virite each dig t il a t$purate box
It Pai~_thllsectgdllion (00 lt) -1 1) - Dl monll 10M
lw) bolte IlrO proY140d fetr olAoh pr 01 thQ dISh Enter tho dA) ldns a R
d16ih
emiddot5middot (0 11 I for 115t ( 0 21 for 5th etc Treat month the am pay
e ~ 10 ~ I for I-hrch 0 [2] for September Tho y~nr must be (into ad
I Z I ~ I I 71 q etc
Take as in IixulIple tho dOlte 3rd tllrch 1973 7~ie must bo written
[0131 LSLDI[7l3JDny Month Ye~r
5middot 1~J $~~ - Irom ~-------- To --------shytntol hOI II the time the Clinic 111118 in SW5sion emiddot8middot
(i) 11011 500 lm To 1200 non
(11) Frclt 100 pm To 400 pm
(iii ) IX-OG OO pllI To 6~00 pm
f
2
ADEJ ) Paae ) of S
6 Eov
_ 1hA 1gtIpoundC iIIUlt be nu~o7Ifd tler1ally 1 throurh n lU tbey Are Wled In ~1l8ellJ IInel 1301 tlU 1 Orcl 1 Wled tor a o5038ioll - -I 2 tonY tho _boul~ b I1WJbtl 1 and 2
hlrlll are 25 linos OIl the fOnl Ilnd thoae muet be UBtleS for 25 clients 9 one ior bullbull 01 I ini
ot ~h lc II ol1cM lOlivpound til e linic before soeinc DurOI or doc tor ilnc ii hox rristrltltion nUlJbet had alrearll been recorded on the Dai 1y Roiuter then n line ~hollld be drawn through that entry an1 the eliort nust not 06 includttd in tho totals tor that 0eDion
1lw Ileifitration Num)~r of cueh client must be IiIritten IS n 5-dlrlt oode ClhnC IH11IlElr 315 1IIU8 tborotore be enterod 18J010117]5]
~ Clt ZOt
Coda 1 Codo
10 ~tl c 2t j co 21)
~w elSe - Coda 1 0) d CltaEl - Code 2 Revislt Code 3
Only pound1 01 theBe coiles may be usod
11 prol-O~ ~Eil~1 (cc 22)
If ma climt was L drop-out IIho haoS returned now to the Clinio tor tho first no linmiddot bullwin lt1ro1eo o t he or she should be given CCe 1 It this do 5 II It nprlly leu this colWlln blank
u Hothod middothisllill loe 23)
NOh til t otly ~ Cod 16 tp he ontered in 2lpound of the columna oven thOUGh 10 co11lllJlB 10 provided on the torm The Codes llrol-
Oral Contraceptive Code 0 1 U D Code 1 Condom plUD Codo Z Condor (only) Code 3 Foum tAblets cream Code it DitphrClGJII Code 5 Rhythm Cde 6 Injectible Code 7 Advice Code 8 Other Code 9
It for middotDo-le 1 client rlllll ji yen cclldorls ord foam or creall Iou Qust entor Coole i (condom plulJ) in the appropri~te column This Quat be the only lIotmiddot) tarcie If an in the cnse of a tlnle clinic I the client is Bup)lieu lith COIlOrW only you rmot entEr CorlQ 3 (cpndolll) Do not use a ticII ~ tho (odo Nwber
It is CUi tomary fur 11 cliont 110 is beine put on the oral contraceptive for the first tiT1o and even on other occasionn be issued condoms and 11 crelle or foam a Ilell rI3 a pgtcket of pilla In such Cllses when the piDQ Ilre Ilctually iouou you tlust record Orll (Co~e 0) 08 tho onll metbod ilo othor ntry sll0uld ho nnrlo
Uovever n SJC~ canas vucru condoms and fOHa ~rc eiven but no pilJa (even thoJRh _t _n the intention to issue pills nt the noxt vioit) than the Mothol Th5 ifli t ohoulcl be recorded uo Condor Plus (Code 2)
13 Seen Bybullbullbullbullbull
~rot S-1 SO l
Doctor (Dr) - Code 1 j Nurse (Nul ) - Code 2
Clark (Olk-) - Code If tho Clhnt is vcen hy both tho llootor tlnd the Nurse enter Code 1 t Doctor It 6~61l by the Nurso only arite Code 2 Cod bullbull Cerk is l)llnt for FA Cllnica Clerks in tho Government Cli1t hiwo Llttoll istructed not to i56uo supplios on their own volition
14 fl221~
lhio S~tiCl of -Ie fvrtl t~ke 16 (llrci coluMna (cc 25-+0) nnd 10 tho only part at th iOIQ in llich iore thAn one cod is Zlccoptl1blo Tho purpoco of the )ecton is to 0 able to arrive nt the Cjunntity of 6tock dilltlitJutshyed YOI IIlUdt writo in the CllllOjH-iata colulna the nUllbJr of Il1ch 4rtic1o i~JSu~d ~lo e ha I Oral Contrcilpti vea are aub-di vi dod into types ae_ 3 PIllCKC 9 0 Elynnn LlUot be entered Codo in card column 25
If tor eXllrplc t l cliunt is iosued wi th packots of Zucynon nnd aJ(1 ~ivn 1 conuotll (8inoloo) you ouot enter in oard column 25 and 11 It
cnrd col~8 )2 and J (io 1 in card colucn 2 nnd 2 1n card coluun 33) Nota C)lldoIlU ale to b(t ruoordod individually not os packots of throo) Should n ne LlondoClo be isoued thil3 is to be rc-Qed as 09
If It clint 6 t~ot isoued Blly lIupplies thon you must writo Codo 1 in CQllAlilD 41
It Q eli nt isite the clinic to check on her LUD or her Diaphra~t IUId ro DI W 6 ppl ills nre ispounducd then Code 1 1s wri t ten in column 40
In the FA clinios here a variety ot orll contraceptiveo in orer~l tho elerll wilmiddot~ bJ provided with a specill code shoot The idontifyin coo will b wiittn in Column 29 nnd the nUlber of packets iosued in colwm )0
lralaer-In Code 1 lrllllsie r~ut Coda 2 leIllPQrArr Trnnsfer-In Codo gt
In the cao of n 2ratl8fcr-In I you lUot n160 cOrlpleto coluons 42-51
In the cllU J of A ~~emporary TranGfor-1n (an individual who i8 only v1citing fur clinic tor some epecial trcatcont hna who will bo rdnlnin
~middot(II~~~fO~l~SIl~I3~nn~~~h~rO~nh~1~~190~~nll 2-46 and ler rei IItrntion numbu in colullnll41-51
It the oli( nt i iNt a CrllnoforwIu - Out or loClporu1 tMn loave oolumn 1 blank
16 lr4nst(gtr-tl2~~morrry TilJnder-In (co 42-51) Forl1ltl CUn E1~ (cc 112-46)
hen you rei iatlr L irllsfcrln or Il TJlporary Trnnsfer-In you IIIUBt write I ere the five-digit clinio nucbor of the Clinic iraQ which tho ltlient Me (uIlO
2mer ]letr ~2n ~ (cc 47-51)
frlta fllao Clo r-~itrlltion Nuc~Er ot the client in the Former Clinic (i c bullbull th 1 Sis rnmiddotion ~UlIlh()r which the client carrics 1n the tormor clinio) bull
It tho Forrltl Ho( ist rntion Number iIJ not readily wnilnble you tluct oocpluto thtl epcciol [orlll Transfer-In Not Identifiod Dy Forrlcr RCGi(trn~ t10n Nwlbvr Or ~ flt)rCl is to be cOlplctcd for och cnso nnd th forlJO Ilubmi tted to thu )opllntion Prorrnnme Of fice tOGether with tho Dily Ro~iBtors lhwev~r should the clork leuTI of tho clint B FormlI Uocintra tion lUlllb r )0[(10 Cubmi ttinft the D1ily IOCI otro t hen the nUQbcr shoulo bo -ri ton in colucns 47-51 lna the special foro should lJo deotroyotl
l7 bullbullbullbullbull
r lt bull bull
ADXI ) Pap S ot S
11 UD LV~ (cc 525)
It tb( cliont io ~ivQn An IUD tor the firot tl~o then you should Sri to Codo 1 Inuort ill colurJI 52
It tho olimiddotsnt ia rvinGgtrtltld i th An I UD bullbull tben wse Coda 2 RelnDltlrt shyin (01Uil11 52
It the clLmt is ~tte~~dint chnic beruse her IUD CflClQ out by Haol (cxpll Iion i ~hcn fir te todo ~- UIlllrli1 53~
If c-ltr IU fj IIIS reov in -ne cllnic by tho doctor or nurso t~on vlritI Codec in column 5
II the eli nt otends eiLlie tld explin[l th(lt she rccovcd the IUD tlllleel nen write Coda H in Colwlm 53
It the IUD jr still within the uterus nd the WOIraquoI1 1 11rc6llJlnt thon lIrite 1gt40 4 in Column 53
lZ np h5t (ce 54) It 0 Pull 5mor ie t~ken durin thi visit tben Codo 1 ehould be ampDtere4 in ColWlln 54 Should he c110nt lltt rQ(uircd to rttturn to clin1c for a rogtol1t Pnl) t06t then CoLe 2 llhould bo middotwrittcn in column 54
It no Pllp Scou io taken tde visit Itove colUQn 54 blank
Iraferti1lli (CQ 55)
Ii the e liett io nl1 infortili tr eaoe use Cor1o Ill in colUQn 55
If tbia 1000 not tlpl lonve column 55 blonk
20 Totaltll
CO~1ploete the [)ldegO 1gty puti YI tne totals betweon the double lines nt tu b()ttctl Carrj colUlllnc 20 21 nd gt4 Must hlve tho Bnoe JllIIber and thiG Would coreslonc to the numocr ir attencbnco
Writ$ th to1ul nUlllior of Drop-Outs returned (c022)
Urito 41eo tb totnls fOJ each card column 0 to 9 under tho h(adinu Method thiB Vioit Show tho tote L fgtr OlCl type of contraceptive issued (cc 25-40)
1)0 Dot wrLte 1111 totll lUl(Ier Card Columns 15-19 29 41-51
21 COPmllh bull ~lt h~t~ Monthly ROilort
OQ thG DaLl oCator forlll thnt ccrrOspOldB to tho 1(8t 1$06610n lt 0
oth yo Olllt (vwlgtleto the items nt the botto of the [orampl This is tour ontll~1 n(olt nnd includcD tho totll lumber of sesions Ilntl tho total Iluolcr ( r crop-outs durinr the Qonth
An tiUlsilt n drir which n doctor liB in nttcndnncc is a doctor sOfll~1on and shoulc 00 re(liGtcnd in coltns 56-57 All other sessions 1116 conlliid~recl supply stllciona and thtlY 1110 rocordod in columns 58-59
the total Ilum)nl Jf drop-outo ld the drop-outs by method durinc the onth nre 10 bu oltorou in the inrlicllted boxes
72 Chad Your ~
Milke I ura th t all thE fijul4gtu rre c101r -tNever writo our nutlUQrS 50 InrjEl that they oxtend out of tho
ap~rotr1ato ~ox
Cheek to BoJa tht 1111 numuors 1110 in tho correct boxes -- CJslHloially when Writi1 the totlB
Mllxe Cirtc O thmiddott t1e infoT1I1ntion i6 clear on the corbon COllY before sep rmiddotinr the sheets
Jitn the Fomiddotl lien tly sien YOUl nr me 1t the bot tOil right hnnd corner btl forc subol ttinG it Keep tle CL rb n copy for your rocordn
i
-l ________~~---------~
I _1
Adminiatr-atlve SKVieu
P inba ~~~l1cal lrlnbin~~eltltcal -1 te~ra t~~rvicc (lnatittloaa)
--1- - shy -1------------_-L_ l-r-aJiil- shy _-L_tet1lal d
PlIinm1tJ8 atdUon DetalMid H8Il1tb ~ ________bull Care
-----~ Office of i
the FlIily _IPlill3 roarshy
1- - - -------RegiatUll urnr
ltIi 1 Drelttor Rcgicaat Director Souta Tabqo tacallortb ~ counu gt____ ~ (4 ouottet)
Off1ce of the Res10nal Diractoc L
r----- _L_ -- shy i I bull IREgional Ipitl I
District IIttaltb I bull Othn RelOl ond Hcpital CenteIntt itlt j In 1__ _shy-~- ---- -_j
J r Ii~lth
C~nlef
L
I Ihnlth lie I th Offlcu (1ft lc~
Coullty 1I0p1ta1
Henlth tentet
I

F Voluntary Organizations
421 I i~ internrticri31 expedence that the birth control movement is pion aTC tt volunh[~ JilC S Qltl that hen the national governments step in wi tl cmbi ti 019 prjhns wi thin the sLate welfare system voluntary bodies ieh tteir limited ilsrluces restrict their service activities and shift the emplasi i 0 educedgt (f the community training research and contracepshytive Sf vic not 1l7gtilflblr in he official program or in areas not reached by it In nagni tude and expanse the of ficial program in Trinidad and Tobago has alrad~ orertak~n Ce 101umary program Increasingly it will become the domLnart tartner in the total national program while the voluntary agencies will cOltirlU1~ to receive financial support and encouragement to set up high standaeis If service and explore new areas thus acting as a stimulus and an additi_e tl the official program
G FrOB-ram Infomation
422 Thre is no concurrent evaluation or monitoring of the Program The daa or lq72 flowing in from the clinics month by month have r8Jllsined unprocss~d tn the Program Office The official Annual Report - 1971 Sums up th~ poition as fcllo~s
ITThe Research and Evaluation component continued to be the weakest in the Population Program Although a systen of evaluation had been built into the program the follow-up procedures for analyzing the data and for correcting inshyconsistencies are inadequate Requests were made to extend the staff to establish a more viable unit but by the end of the year no chllnges had been made
423 T1e recording and riporting jJrocedures were revised effective Januery 1972 and there has been a further change recently at the instance of t1e Evaluation Adviser Under the system now established the clinics are lequ Lreurod to maintain the following records
a Family Planning Clinic Case Card - New Cases This was introduced on January 1 1972 and has thirty-one entries giving age parity contraceptive listory pregnancies socio-economic background ource of family planning information and agency for notvat ion bull (Annex 2) The case card is made out in duplicate for each new acceptor and a copy sent to the Program Office
b Daily Regis ter This fs a ne~gt1 form recently introduced in replacement of the old regis ter and is preparen
- 15 shy
ie) ruplicate the original to be transmitted to the Program (fHce and the carbon copy to be retained in the clinic Th~ is a very 121zborute form requiring 36 entries to be aa~ for each Chse nel and old attending a session includin~ (ntries to cit L to contTaceptive supplies issued
AijCleX 3 T~13e fcnnG are required to be sent to the Program lffce in i7JO balches every month the first batch for the i IS fif~eeL days and the second for the remaining part of hE month The trtention is that the data appearing in the ~EZlic daily legis ter forms should be compiled in the Program Office and fed back to the clinics Although it is claimed that this new form has been pretested and is workable ex)erience alone will show whether the majority of clinic cL~rks are able to cope with it in a busy session
bull o now-Ho Card TIlis card is intended to keep track of ac ceptor--It has entries for name addresfI and month fcr which a visit is due for each year
bull Aphabe tical Index This is a card index of clients with aidresses
Each i)at en is given a simple clinic card on which the dates of further appo~utnli rc3 an~ indicated A special fonT[ has been devised for the reporting ot cases unler the Post-IartumPost-Abortal Education and Referral Program
424 J system of monitoring progrRm performance from month to month need to bE develQped as a high priori ty The problem is not so much reshycord ng mc transmission of data by the clinics but its aggregation and proclssi ng in the Program Office every month which at present takes a long time The Statistical Officer should have a statistical assistant to help him Ln I he taflk Monthly progress reports should be available to the Mini H t~ n H(llllth and A11 offt eerlil of the ProKrnm Office so that remedial ac tl m I lAY h(~ tuk~n n rll1u- WhOnh1f ~Hfl(AlJtlaTY
42 For the analysis of data and evaluation the Program office shouln haVE th(~ full-time services of a trained demographer
H Field Workers
42) Tie Program nemiddotis tne services of a cadre of field workers to enr)ll neii aceeptoTs follow up acceptors in their homes and revive the int 2remiddott of dropouts Such a category of workers could also be utilizerl for pr1fficting other health programs such as the VD campaign and the inmuni~ation program
47 As an experimental measure one field ~]orker may be assigned to a emi l~ of Hi 000 population This would mean 100 field workers in all
- 16 shy
Earh of the workers should preferably have harl a higher secondary education otherwLe 1gt junior secondalY education They should be married persons with middoti1ltt mot tl-an two or tlree children recruited from the locali ty in which they armiddot~ requlred to function Only persons who have the capaci ty to comnunl at~ and or6anl~e should c chosen A months ini tial orientation
slcu1d enable them to start functioning in the field though reshyfresher CO rSeS tvould be necesslt1ry in due course In Port-of-Spain married mer~ a1C women may be employed on a part-time basis
I Hanagement Study
428 A nanagement study of the Family Planning Program should include a sctu iny of the top m~nagement Atructure (Population Council - Office of the Fanil) PLanning Program - Principal Medical Officer for MCH and Family Planni Ig fetices) the field structure for the delivery of family planning servics (Re0ional Director - District Health Services) including the utilizlti(n if medical and paramedical personnel for adding the function of del ve y )f family planning services and the control and communication proCed1reF Lfnking the top management with the field structure
429 The management consultants may study the functioning of the Popul tio I Council and advise whether it adequately serves the purpose of givini po Licy direction to the Program and if not what changes in its compo itt m and operating procedures may be introduced without altering its bsic craracter as an advisory agency The consultants may suggest an alern at ve form of organizati)n and utilization of personnel which in thir p nion may be better adapted to the needs of the Program
430 Irrespective of whether the Population Council is maintained or it is replaced by an agency of a different character a formation like the Offic of be Family Planning Program would be necessary for the administrashytion i)f 1 he program a task for which i 1 appears inadequately equipped at preselt Its obvious requirements are in the areas of program monitoring and el7alnation program supervision communication and training The manag ememiddotlt consultants may study the structure and procedures of this form~ tio Gnd make suggestions with regard to the augmentation of professional and ~ upp)rt lng staffgt and modification of operating procedures
431 The linkage of the Office of the Family Planning Program with the Miniutry of Health (Central Office) and the District Health Services should be sudied In view of the policy of the Government to integrate MCH and faI11iLy rlallning services it should be examined whether the Principal Medi al Officer for Communi ty Heal th Services (MCH and Family Planning) should be agtpoj nt~d as the Chief of the Office of the Family Planning Program and an adTlilistrative officer of a suitable level inducted in that Office to assist him TIle implication of this suggestion is that the head of the Family PlanJling Program would control the District Health Services
- 17 shy
432 rf 1e management consultants should examine the delegation of adminshyistratiie Bld financial powers of the Ministry of Health to different levels of Progam aclrlirdstration viz bull PMO Program Office Regional Director and County ~djca~ Officers
l33 he system of 01 af Togram information from the clinlcs to the Pr()~ra1 O~fice and tOile processing and use of information in the latter office iholld )e studied
434 he working procedures at the integrated McP and family planning clinics shnuLl be studied This would involve a study of each stage which a clien tpcticmt has to go through from the point of entry to the point of exit after receiving advice service or supplies This study shoulci lead to star dartization of procedures and functions and evolution of -lork norms CognatE st tdies of the working procedures at uni-purpose family planning clinics and su~ply SEssions should also be undertaken An essential component of these ~ tad ~es would be to examine Nhich functions currently performed by docshytors lealh visitors nurses and midives respectively hav~ become so roushytinize ttl it they can he relegated (0 the next 10Her level
435 Reated to working procedures is the problem of job description of medcal 8nd parrunedical personnel involved in family planning from the centra i tc the field level This job description needs to be studied wi th a vie VIW8Id txaminiDg the uttlization of skills and allocation of time by the staff lcc(rd~ng to the functional prj ori ties
436 frV management consultants should study the workings of the curren slralgements fOJ family planning counselling under the Post-Partul11 Post-Abortal Education and Referral Program at the Port-of-Spain and San Fenaldo General Hospitals
437 SU1ect to the ItBrcement of the Gove1nment the management conshy8ultal ts ~hOLlld undertake a study of th requirement of field workers (home vinitcru) in tmtlUI of are nnd population cov(ra~e
ANNEX 1
Names of Persons Met
Ii Mr T C Taitt Pem1(H~nt 3~crtarY) Ministry of Health
2 Dr M n Henry Chitd Medical Officer Ministry of Health
Ellubeth Quam a Prindpal Medical Officer (1S)
4 Mr G Z Jaine ~ uJiector Population Council
5 Dr Norma Andrews Medical Officer Population Council
6 Mr Jc~n Coury~ Evaluation Adviser Population Council
7 Mr A Jriseph Principal Statistical Officer Population Council
8 Dr C 0 Colman Country Representative Pan American Health )rg ni~ation
9 Mr ranca Kippel Health Education Specialist Ministry of Iea th
10 (1 bullbullines Principal Nursing Officer Ministry of Health
11 Dr Mx won (formerlyHinistry of Health)
12 M3 late Carops Ex-Chairman of Population Council
--
4i 1_ middotIIlt F-ntCWclOotf_Y v OJ t tl
GOVIIlHMEIgt(I OF TINIOAD AND TOampAGQ - NNISTJY OF HIALftf AIJIE1 2NATIONAL FAMilY PLANNING PROGRAMME
F MIL Y PLANNING CUNIC CASE CARD - NEW CASES - NFPPl
li ~~___ 1 ________
~ ecll-U
-- --------------------- shy~) ~~middot~------------------~~~~~~---CIJ------ middot~ii--middot-middot----middot-middot---middot--------- shy
ltv Writt N_ 01(111________________
a ~4itiJtmiddotl_____ ilIIIltIoI~____~____~-__----- shybull ~4
fie l$ - JO tDql IIfIA- tr-JMimiddot _ iJ 1 Odoor o
14aorielaquol_ _~ 0 lio witIleo-La ~ 01 bull - OJ ( _01 1~ltgt1lh o bull- 0$
AacJcu 0 2 CIIriIWA 0 J Os 0
Yv~MONTH ltnollOf~nfIGHTI
Undu 1100U$ Utgtdn 5SCI Undu 11200 01 ~ 50 - 9949 amp100 - 1199 02UlOO - nn9E~ (
0)~ 10- $99 SiOO -- U9~ lOO -- U99 12400 - 1359)-------_-r----shy ~l)o SIS n600 - Hm1300 -- 019 OJ200 il~9 ~------ 99~ a 1)0 m Os1)00 -- l99 1400 -shy $4100 -- 1S999r--- shy
1500 donl S6000aad O399 - lt499I~- I 0lt
ltII
IJ -IC _~tltlioltgti lS
02 IaampJIIocI OJ 04 laM Os
w Oltwio I_-l(~u IrIaa U
h~~ ~Clubl 01 OJ
IS ~C-n 01 toSIitDI 02
Ji poundI on 01 IriIIIuy M ur 02 IV OJ
WU 10 pltIoII~ llaMtl 411 cIIiId 01 Ol it fIolto ~ do~ _14 rou IIlgtJo 1Ia1 ___~_ shy
40
It _ I 00 ~bull FPIiIJ 1
OJ 02 OJ 06
)0 III- iy wOWcf ~1
aMIIl Os
11 T 1gtlt ( h _______ 4)~
06
04 (MIbullbull middot bIrlI ~___~__~_ (-fIJI ~- -~-- (1HJ 49middot SJ
U 10k 01( 1__ raquo$-4
iU1) DOl F ToWotfOlnC DOl 001 or Do [IP 006 001 OIIgtu___Spltclty DOll Nltmo 010
U1Mo I orcpmiddot laquo55middot16
1lD 001 Foam Toblelf_ICim DOl Condom DOl CoomS~ 004 oe Oos WlttuJn 1J OIkr DSpody) 101~ ~Iu 006 Rhylhm 001 DOG OJO
no wI~lmm 4 cd
(I 0) 1110 01 Condor 03 (lorn bull l S~muoidIl 04 Faa TabioolfIIltr- Os RhyUlm 01 lnJrl tible O Advico 090 06
la slt 1)0 19 loti ~rltnlt) ([)sl or 1llOn) ____ --__ bullbully-J n SV - ~JcdS
v~ Cl NCI 0 30 OJI_O I Wr blJ1h 0 I ~ OJ 1 ~ (fOOd V 01 No 02 laquo 6) Cf4
WIiI 1 172
004 001
j D middotmiddot middot
1 ~
r
~
bull I
bullI I I
r c i
ANNEX 3 Pagemiddot 1 of 5
0 raquo rshy -lt l)J ~ 111 t G) 5 shy (J) ~ -
fT1u
i
MINISTTY OF Ho1TH
NTIONl F~ILY LNNING PR-GRbullbullM-tE
~~5tructions to C11nic ClerKa
How to co~ploto the Daily Rogister
~~ ~~v1sd Daily Rosi8ter replnc~D tho one which is now in use tb$ Monthly PC~ri rOt~ arti tho 01( Ci() Dod PollJ j f m It is a pre-coded form and 1411 cl~1p Jd tl a1I6iniul-mIHvn Oel Clinic nctivi~y
110 )rm rollt biJ coupJot)d lrl cupLtcoto using a o(roon shoot Tho top aheot or oriinai ~ust bl) 6(Ult to tho CQgt1tral O[[lCO and tho carbon copy retained in the Gliaic rilo dll the for6a that ar uD~d betwoen the 1st 4nd the 15th of the oIIollth aut bo subClittud tocho office 35 Lnc blttch Those oomp1cted betwoon tho 16th _lid tqemc of tho month must bo ~cnt in a secJnll batch
P lOvLior hns boon Illllde for 25 clients on cZlch forlll new forlll must b IIlied f r poundh 50[810n2 whothur or not ono or lIIore session are hoIdiit the clinic on he sarne day
I th ro alO more htl 25 clionta 1n attondnnco at tho session the additi shyOhAl m~bOl of clionts 10 clients nu~ber 26 27 etc sh0u1l be ontered on the next Imiddotrlll ~i ttout a1tpoundring the numbtlrs in the cvlumn hond Series
51 ppOfil th~ number of aUcnts lQr that session ws 5 this would mean thllt two rJlS ~ lst be 6ubllIitt~dl the first filled uF 1 tltgt 25 And the laquoIncond 1 to 10 Th~ cal bon ofies should bo st~plod togother at thu t0P l~rt h4nd corner of the torm ard ktpt in the Clinic filo lou IIlU6t stapl~ the originftls in the 8~~ monnshyer for lIub~ssion to the ofticl
ie h~ ll idontiflctior- (cc 1 - )
0 lot Ji 9 anythin~ hGro poundhia is int(mdClc for tha computer code
2 ~~pound~ - Print clOflrly tho name of your Clinic
C1Lic Huml or - (cc 4 - 8) Evar1 Clinic Numbor has 5 digits Virite each dig t il a t$purate box
It Pai~_thllsectgdllion (00 lt) -1 1) - Dl monll 10M
lw) bolte IlrO proY140d fetr olAoh pr 01 thQ dISh Enter tho dA) ldns a R
d16ih
emiddot5middot (0 11 I for 115t ( 0 21 for 5th etc Treat month the am pay
e ~ 10 ~ I for I-hrch 0 [2] for September Tho y~nr must be (into ad
I Z I ~ I I 71 q etc
Take as in IixulIple tho dOlte 3rd tllrch 1973 7~ie must bo written
[0131 LSLDI[7l3JDny Month Ye~r
5middot 1~J $~~ - Irom ~-------- To --------shytntol hOI II the time the Clinic 111118 in SW5sion emiddot8middot
(i) 11011 500 lm To 1200 non
(11) Frclt 100 pm To 400 pm
(iii ) IX-OG OO pllI To 6~00 pm
f
2
ADEJ ) Paae ) of S
6 Eov
_ 1hA 1gtIpoundC iIIUlt be nu~o7Ifd tler1ally 1 throurh n lU tbey Are Wled In ~1l8ellJ IInel 1301 tlU 1 Orcl 1 Wled tor a o5038ioll - -I 2 tonY tho _boul~ b I1WJbtl 1 and 2
hlrlll are 25 linos OIl the fOnl Ilnd thoae muet be UBtleS for 25 clients 9 one ior bullbull 01 I ini
ot ~h lc II ol1cM lOlivpound til e linic before soeinc DurOI or doc tor ilnc ii hox rristrltltion nUlJbet had alrearll been recorded on the Dai 1y Roiuter then n line ~hollld be drawn through that entry an1 the eliort nust not 06 includttd in tho totals tor that 0eDion
1lw Ileifitration Num)~r of cueh client must be IiIritten IS n 5-dlrlt oode ClhnC IH11IlElr 315 1IIU8 tborotore be enterod 18J010117]5]
~ Clt ZOt
Coda 1 Codo
10 ~tl c 2t j co 21)
~w elSe - Coda 1 0) d CltaEl - Code 2 Revislt Code 3
Only pound1 01 theBe coiles may be usod
11 prol-O~ ~Eil~1 (cc 22)
If ma climt was L drop-out IIho haoS returned now to the Clinio tor tho first no linmiddot bullwin lt1ro1eo o t he or she should be given CCe 1 It this do 5 II It nprlly leu this colWlln blank
u Hothod middothisllill loe 23)
NOh til t otly ~ Cod 16 tp he ontered in 2lpound of the columna oven thOUGh 10 co11lllJlB 10 provided on the torm The Codes llrol-
Oral Contraceptive Code 0 1 U D Code 1 Condom plUD Codo Z Condor (only) Code 3 Foum tAblets cream Code it DitphrClGJII Code 5 Rhythm Cde 6 Injectible Code 7 Advice Code 8 Other Code 9
It for middotDo-le 1 client rlllll ji yen cclldorls ord foam or creall Iou Qust entor Coole i (condom plulJ) in the appropri~te column This Quat be the only lIotmiddot) tarcie If an in the cnse of a tlnle clinic I the client is Bup)lieu lith COIlOrW only you rmot entEr CorlQ 3 (cpndolll) Do not use a ticII ~ tho (odo Nwber
It is CUi tomary fur 11 cliont 110 is beine put on the oral contraceptive for the first tiT1o and even on other occasionn be issued condoms and 11 crelle or foam a Ilell rI3 a pgtcket of pilla In such Cllses when the piDQ Ilre Ilctually iouou you tlust record Orll (Co~e 0) 08 tho onll metbod ilo othor ntry sll0uld ho nnrlo
Uovever n SJC~ canas vucru condoms and fOHa ~rc eiven but no pilJa (even thoJRh _t _n the intention to issue pills nt the noxt vioit) than the Mothol Th5 ifli t ohoulcl be recorded uo Condor Plus (Code 2)
13 Seen Bybullbullbullbullbull
~rot S-1 SO l
Doctor (Dr) - Code 1 j Nurse (Nul ) - Code 2
Clark (Olk-) - Code If tho Clhnt is vcen hy both tho llootor tlnd the Nurse enter Code 1 t Doctor It 6~61l by the Nurso only arite Code 2 Cod bullbull Cerk is l)llnt for FA Cllnica Clerks in tho Government Cli1t hiwo Llttoll istructed not to i56uo supplios on their own volition
14 fl221~
lhio S~tiCl of -Ie fvrtl t~ke 16 (llrci coluMna (cc 25-+0) nnd 10 tho only part at th iOIQ in llich iore thAn one cod is Zlccoptl1blo Tho purpoco of the )ecton is to 0 able to arrive nt the Cjunntity of 6tock dilltlitJutshyed YOI IIlUdt writo in the CllllOjH-iata colulna the nUllbJr of Il1ch 4rtic1o i~JSu~d ~lo e ha I Oral Contrcilpti vea are aub-di vi dod into types ae_ 3 PIllCKC 9 0 Elynnn LlUot be entered Codo in card column 25
If tor eXllrplc t l cliunt is iosued wi th packots of Zucynon nnd aJ(1 ~ivn 1 conuotll (8inoloo) you ouot enter in oard column 25 and 11 It
cnrd col~8 )2 and J (io 1 in card colucn 2 nnd 2 1n card coluun 33) Nota C)lldoIlU ale to b(t ruoordod individually not os packots of throo) Should n ne LlondoClo be isoued thil3 is to be rc-Qed as 09
If It clint 6 t~ot isoued Blly lIupplies thon you must writo Codo 1 in CQllAlilD 41
It Q eli nt isite the clinic to check on her LUD or her Diaphra~t IUId ro DI W 6 ppl ills nre ispounducd then Code 1 1s wri t ten in column 40
In the FA clinios here a variety ot orll contraceptiveo in orer~l tho elerll wilmiddot~ bJ provided with a specill code shoot The idontifyin coo will b wiittn in Column 29 nnd the nUlber of packets iosued in colwm )0
lralaer-In Code 1 lrllllsie r~ut Coda 2 leIllPQrArr Trnnsfer-In Codo gt
In the cao of n 2ratl8fcr-In I you lUot n160 cOrlpleto coluons 42-51
In the cllU J of A ~~emporary TranGfor-1n (an individual who i8 only v1citing fur clinic tor some epecial trcatcont hna who will bo rdnlnin
~middot(II~~~fO~l~SIl~I3~nn~~~h~rO~nh~1~~190~~nll 2-46 and ler rei IItrntion numbu in colullnll41-51
It the oli( nt i iNt a CrllnoforwIu - Out or loClporu1 tMn loave oolumn 1 blank
16 lr4nst(gtr-tl2~~morrry TilJnder-In (co 42-51) Forl1ltl CUn E1~ (cc 112-46)
hen you rei iatlr L irllsfcrln or Il TJlporary Trnnsfer-In you IIIUBt write I ere the five-digit clinio nucbor of the Clinic iraQ which tho ltlient Me (uIlO
2mer ]letr ~2n ~ (cc 47-51)
frlta fllao Clo r-~itrlltion Nuc~Er ot the client in the Former Clinic (i c bullbull th 1 Sis rnmiddotion ~UlIlh()r which the client carrics 1n the tormor clinio) bull
It tho Forrltl Ho( ist rntion Number iIJ not readily wnilnble you tluct oocpluto thtl epcciol [orlll Transfer-In Not Identifiod Dy Forrlcr RCGi(trn~ t10n Nwlbvr Or ~ flt)rCl is to be cOlplctcd for och cnso nnd th forlJO Ilubmi tted to thu )opllntion Prorrnnme Of fice tOGether with tho Dily Ro~iBtors lhwev~r should the clork leuTI of tho clint B FormlI Uocintra tion lUlllb r )0[(10 Cubmi ttinft the D1ily IOCI otro t hen the nUQbcr shoulo bo -ri ton in colucns 47-51 lna the special foro should lJo deotroyotl
l7 bullbullbullbullbull
r lt bull bull
ADXI ) Pap S ot S
11 UD LV~ (cc 525)
It tb( cliont io ~ivQn An IUD tor the firot tl~o then you should Sri to Codo 1 Inuort ill colurJI 52
It tho olimiddotsnt ia rvinGgtrtltld i th An I UD bullbull tben wse Coda 2 RelnDltlrt shyin (01Uil11 52
It the clLmt is ~tte~~dint chnic beruse her IUD CflClQ out by Haol (cxpll Iion i ~hcn fir te todo ~- UIlllrli1 53~
If c-ltr IU fj IIIS reov in -ne cllnic by tho doctor or nurso t~on vlritI Codec in column 5
II the eli nt otends eiLlie tld explin[l th(lt she rccovcd the IUD tlllleel nen write Coda H in Colwlm 53
It the IUD jr still within the uterus nd the WOIraquoI1 1 11rc6llJlnt thon lIrite 1gt40 4 in Column 53
lZ np h5t (ce 54) It 0 Pull 5mor ie t~ken durin thi visit tben Codo 1 ehould be ampDtere4 in ColWlln 54 Should he c110nt lltt rQ(uircd to rttturn to clin1c for a rogtol1t Pnl) t06t then CoLe 2 llhould bo middotwrittcn in column 54
It no Pllp Scou io taken tde visit Itove colUQn 54 blank
Iraferti1lli (CQ 55)
Ii the e liett io nl1 infortili tr eaoe use Cor1o Ill in colUQn 55
If tbia 1000 not tlpl lonve column 55 blonk
20 Totaltll
CO~1ploete the [)ldegO 1gty puti YI tne totals betweon the double lines nt tu b()ttctl Carrj colUlllnc 20 21 nd gt4 Must hlve tho Bnoe JllIIber and thiG Would coreslonc to the numocr ir attencbnco
Writ$ th to1ul nUlllior of Drop-Outs returned (c022)
Urito 41eo tb totnls fOJ each card column 0 to 9 under tho h(adinu Method thiB Vioit Show tho tote L fgtr OlCl type of contraceptive issued (cc 25-40)
1)0 Dot wrLte 1111 totll lUl(Ier Card Columns 15-19 29 41-51
21 COPmllh bull ~lt h~t~ Monthly ROilort
OQ thG DaLl oCator forlll thnt ccrrOspOldB to tho 1(8t 1$06610n lt 0
oth yo Olllt (vwlgtleto the items nt the botto of the [orampl This is tour ontll~1 n(olt nnd includcD tho totll lumber of sesions Ilntl tho total Iluolcr ( r crop-outs durinr the Qonth
An tiUlsilt n drir which n doctor liB in nttcndnncc is a doctor sOfll~1on and shoulc 00 re(liGtcnd in coltns 56-57 All other sessions 1116 conlliid~recl supply stllciona and thtlY 1110 rocordod in columns 58-59
the total Ilum)nl Jf drop-outo ld the drop-outs by method durinc the onth nre 10 bu oltorou in the inrlicllted boxes
72 Chad Your ~
Milke I ura th t all thE fijul4gtu rre c101r -tNever writo our nutlUQrS 50 InrjEl that they oxtend out of tho
ap~rotr1ato ~ox
Cheek to BoJa tht 1111 numuors 1110 in tho correct boxes -- CJslHloially when Writi1 the totlB
Mllxe Cirtc O thmiddott t1e infoT1I1ntion i6 clear on the corbon COllY before sep rmiddotinr the sheets
Jitn the Fomiddotl lien tly sien YOUl nr me 1t the bot tOil right hnnd corner btl forc subol ttinG it Keep tle CL rb n copy for your rocordn
i
-l ________~~---------~
I _1
Adminiatr-atlve SKVieu
P inba ~~~l1cal lrlnbin~~eltltcal -1 te~ra t~~rvicc (lnatittloaa)
--1- - shy -1------------_-L_ l-r-aJiil- shy _-L_tet1lal d
PlIinm1tJ8 atdUon DetalMid H8Il1tb ~ ________bull Care
-----~ Office of i
the FlIily _IPlill3 roarshy
1- - - -------RegiatUll urnr
ltIi 1 Drelttor Rcgicaat Director Souta Tabqo tacallortb ~ counu gt____ ~ (4 ouottet)
Off1ce of the Res10nal Diractoc L
r----- _L_ -- shy i I bull IREgional Ipitl I
District IIttaltb I bull Othn RelOl ond Hcpital CenteIntt itlt j In 1__ _shy-~- ---- -_j
J r Ii~lth
C~nlef
L
I Ihnlth lie I th Offlcu (1ft lc~
Coullty 1I0p1ta1
Henlth tentet
I

- 15 shy
ie) ruplicate the original to be transmitted to the Program (fHce and the carbon copy to be retained in the clinic Th~ is a very 121zborute form requiring 36 entries to be aa~ for each Chse nel and old attending a session includin~ (ntries to cit L to contTaceptive supplies issued
AijCleX 3 T~13e fcnnG are required to be sent to the Program lffce in i7JO balches every month the first batch for the i IS fif~eeL days and the second for the remaining part of hE month The trtention is that the data appearing in the ~EZlic daily legis ter forms should be compiled in the Program Office and fed back to the clinics Although it is claimed that this new form has been pretested and is workable ex)erience alone will show whether the majority of clinic cL~rks are able to cope with it in a busy session
bull o now-Ho Card TIlis card is intended to keep track of ac ceptor--It has entries for name addresfI and month fcr which a visit is due for each year
bull Aphabe tical Index This is a card index of clients with aidresses
Each i)at en is given a simple clinic card on which the dates of further appo~utnli rc3 an~ indicated A special fonT[ has been devised for the reporting ot cases unler the Post-IartumPost-Abortal Education and Referral Program
424 J system of monitoring progrRm performance from month to month need to bE develQped as a high priori ty The problem is not so much reshycord ng mc transmission of data by the clinics but its aggregation and proclssi ng in the Program Office every month which at present takes a long time The Statistical Officer should have a statistical assistant to help him Ln I he taflk Monthly progress reports should be available to the Mini H t~ n H(llllth and A11 offt eerlil of the ProKrnm Office so that remedial ac tl m I lAY h(~ tuk~n n rll1u- WhOnh1f ~Hfl(AlJtlaTY
42 For the analysis of data and evaluation the Program office shouln haVE th(~ full-time services of a trained demographer
H Field Workers
42) Tie Program nemiddotis tne services of a cadre of field workers to enr)ll neii aceeptoTs follow up acceptors in their homes and revive the int 2remiddott of dropouts Such a category of workers could also be utilizerl for pr1fficting other health programs such as the VD campaign and the inmuni~ation program
47 As an experimental measure one field ~]orker may be assigned to a emi l~ of Hi 000 population This would mean 100 field workers in all
- 16 shy
Earh of the workers should preferably have harl a higher secondary education otherwLe 1gt junior secondalY education They should be married persons with middoti1ltt mot tl-an two or tlree children recruited from the locali ty in which they armiddot~ requlred to function Only persons who have the capaci ty to comnunl at~ and or6anl~e should c chosen A months ini tial orientation
slcu1d enable them to start functioning in the field though reshyfresher CO rSeS tvould be necesslt1ry in due course In Port-of-Spain married mer~ a1C women may be employed on a part-time basis
I Hanagement Study
428 A nanagement study of the Family Planning Program should include a sctu iny of the top m~nagement Atructure (Population Council - Office of the Fanil) PLanning Program - Principal Medical Officer for MCH and Family Planni Ig fetices) the field structure for the delivery of family planning servics (Re0ional Director - District Health Services) including the utilizlti(n if medical and paramedical personnel for adding the function of del ve y )f family planning services and the control and communication proCed1reF Lfnking the top management with the field structure
429 The management consultants may study the functioning of the Popul tio I Council and advise whether it adequately serves the purpose of givini po Licy direction to the Program and if not what changes in its compo itt m and operating procedures may be introduced without altering its bsic craracter as an advisory agency The consultants may suggest an alern at ve form of organizati)n and utilization of personnel which in thir p nion may be better adapted to the needs of the Program
430 Irrespective of whether the Population Council is maintained or it is replaced by an agency of a different character a formation like the Offic of be Family Planning Program would be necessary for the administrashytion i)f 1 he program a task for which i 1 appears inadequately equipped at preselt Its obvious requirements are in the areas of program monitoring and el7alnation program supervision communication and training The manag ememiddotlt consultants may study the structure and procedures of this form~ tio Gnd make suggestions with regard to the augmentation of professional and ~ upp)rt lng staffgt and modification of operating procedures
431 The linkage of the Office of the Family Planning Program with the Miniutry of Health (Central Office) and the District Health Services should be sudied In view of the policy of the Government to integrate MCH and faI11iLy rlallning services it should be examined whether the Principal Medi al Officer for Communi ty Heal th Services (MCH and Family Planning) should be agtpoj nt~d as the Chief of the Office of the Family Planning Program and an adTlilistrative officer of a suitable level inducted in that Office to assist him TIle implication of this suggestion is that the head of the Family PlanJling Program would control the District Health Services
- 17 shy
432 rf 1e management consultants should examine the delegation of adminshyistratiie Bld financial powers of the Ministry of Health to different levels of Progam aclrlirdstration viz bull PMO Program Office Regional Director and County ~djca~ Officers
l33 he system of 01 af Togram information from the clinlcs to the Pr()~ra1 O~fice and tOile processing and use of information in the latter office iholld )e studied
434 he working procedures at the integrated McP and family planning clinics shnuLl be studied This would involve a study of each stage which a clien tpcticmt has to go through from the point of entry to the point of exit after receiving advice service or supplies This study shoulci lead to star dartization of procedures and functions and evolution of -lork norms CognatE st tdies of the working procedures at uni-purpose family planning clinics and su~ply SEssions should also be undertaken An essential component of these ~ tad ~es would be to examine Nhich functions currently performed by docshytors lealh visitors nurses and midives respectively hav~ become so roushytinize ttl it they can he relegated (0 the next 10Her level
435 Reated to working procedures is the problem of job description of medcal 8nd parrunedical personnel involved in family planning from the centra i tc the field level This job description needs to be studied wi th a vie VIW8Id txaminiDg the uttlization of skills and allocation of time by the staff lcc(rd~ng to the functional prj ori ties
436 frV management consultants should study the workings of the curren slralgements fOJ family planning counselling under the Post-Partul11 Post-Abortal Education and Referral Program at the Port-of-Spain and San Fenaldo General Hospitals
437 SU1ect to the ItBrcement of the Gove1nment the management conshy8ultal ts ~hOLlld undertake a study of th requirement of field workers (home vinitcru) in tmtlUI of are nnd population cov(ra~e
ANNEX 1
Names of Persons Met
Ii Mr T C Taitt Pem1(H~nt 3~crtarY) Ministry of Health
2 Dr M n Henry Chitd Medical Officer Ministry of Health
Ellubeth Quam a Prindpal Medical Officer (1S)
4 Mr G Z Jaine ~ uJiector Population Council
5 Dr Norma Andrews Medical Officer Population Council
6 Mr Jc~n Coury~ Evaluation Adviser Population Council
7 Mr A Jriseph Principal Statistical Officer Population Council
8 Dr C 0 Colman Country Representative Pan American Health )rg ni~ation
9 Mr ranca Kippel Health Education Specialist Ministry of Iea th
10 (1 bullbullines Principal Nursing Officer Ministry of Health
11 Dr Mx won (formerlyHinistry of Health)
12 M3 late Carops Ex-Chairman of Population Council
--
4i 1_ middotIIlt F-ntCWclOotf_Y v OJ t tl
GOVIIlHMEIgt(I OF TINIOAD AND TOampAGQ - NNISTJY OF HIALftf AIJIE1 2NATIONAL FAMilY PLANNING PROGRAMME
F MIL Y PLANNING CUNIC CASE CARD - NEW CASES - NFPPl
li ~~___ 1 ________
~ ecll-U
-- --------------------- shy~) ~~middot~------------------~~~~~~---CIJ------ middot~ii--middot-middot----middot-middot---middot--------- shy
ltv Writt N_ 01(111________________
a ~4itiJtmiddotl_____ ilIIIltIoI~____~____~-__----- shybull ~4
fie l$ - JO tDql IIfIA- tr-JMimiddot _ iJ 1 Odoor o
14aorielaquol_ _~ 0 lio witIleo-La ~ 01 bull - OJ ( _01 1~ltgt1lh o bull- 0$
AacJcu 0 2 CIIriIWA 0 J Os 0
Yv~MONTH ltnollOf~nfIGHTI
Undu 1100U$ Utgtdn 5SCI Undu 11200 01 ~ 50 - 9949 amp100 - 1199 02UlOO - nn9E~ (
0)~ 10- $99 SiOO -- U9~ lOO -- U99 12400 - 1359)-------_-r----shy ~l)o SIS n600 - Hm1300 -- 019 OJ200 il~9 ~------ 99~ a 1)0 m Os1)00 -- l99 1400 -shy $4100 -- 1S999r--- shy
1500 donl S6000aad O399 - lt499I~- I 0lt
ltII
IJ -IC _~tltlioltgti lS
02 IaampJIIocI OJ 04 laM Os
w Oltwio I_-l(~u IrIaa U
h~~ ~Clubl 01 OJ
IS ~C-n 01 toSIitDI 02
Ji poundI on 01 IriIIIuy M ur 02 IV OJ
WU 10 pltIoII~ llaMtl 411 cIIiId 01 Ol it fIolto ~ do~ _14 rou IIlgtJo 1Ia1 ___~_ shy
40
It _ I 00 ~bull FPIiIJ 1
OJ 02 OJ 06
)0 III- iy wOWcf ~1
aMIIl Os
11 T 1gtlt ( h _______ 4)~
06
04 (MIbullbull middot bIrlI ~___~__~_ (-fIJI ~- -~-- (1HJ 49middot SJ
U 10k 01( 1__ raquo$-4
iU1) DOl F ToWotfOlnC DOl 001 or Do [IP 006 001 OIIgtu___Spltclty DOll Nltmo 010
U1Mo I orcpmiddot laquo55middot16
1lD 001 Foam Toblelf_ICim DOl Condom DOl CoomS~ 004 oe Oos WlttuJn 1J OIkr DSpody) 101~ ~Iu 006 Rhylhm 001 DOG OJO
no wI~lmm 4 cd
(I 0) 1110 01 Condor 03 (lorn bull l S~muoidIl 04 Faa TabioolfIIltr- Os RhyUlm 01 lnJrl tible O Advico 090 06
la slt 1)0 19 loti ~rltnlt) ([)sl or 1llOn) ____ --__ bullbully-J n SV - ~JcdS
v~ Cl NCI 0 30 OJI_O I Wr blJ1h 0 I ~ OJ 1 ~ (fOOd V 01 No 02 laquo 6) Cf4
WIiI 1 172
004 001
j D middotmiddot middot
1 ~
r
~
bull I
bullI I I
r c i
ANNEX 3 Pagemiddot 1 of 5
0 raquo rshy -lt l)J ~ 111 t G) 5 shy (J) ~ -
fT1u
i
MINISTTY OF Ho1TH
NTIONl F~ILY LNNING PR-GRbullbullM-tE
~~5tructions to C11nic ClerKa
How to co~ploto the Daily Rogister
~~ ~~v1sd Daily Rosi8ter replnc~D tho one which is now in use tb$ Monthly PC~ri rOt~ arti tho 01( Ci() Dod PollJ j f m It is a pre-coded form and 1411 cl~1p Jd tl a1I6iniul-mIHvn Oel Clinic nctivi~y
110 )rm rollt biJ coupJot)d lrl cupLtcoto using a o(roon shoot Tho top aheot or oriinai ~ust bl) 6(Ult to tho CQgt1tral O[[lCO and tho carbon copy retained in the Gliaic rilo dll the for6a that ar uD~d betwoen the 1st 4nd the 15th of the oIIollth aut bo subClittud tocho office 35 Lnc blttch Those oomp1cted betwoon tho 16th _lid tqemc of tho month must bo ~cnt in a secJnll batch
P lOvLior hns boon Illllde for 25 clients on cZlch forlll new forlll must b IIlied f r poundh 50[810n2 whothur or not ono or lIIore session are hoIdiit the clinic on he sarne day
I th ro alO more htl 25 clionta 1n attondnnco at tho session the additi shyOhAl m~bOl of clionts 10 clients nu~ber 26 27 etc sh0u1l be ontered on the next Imiddotrlll ~i ttout a1tpoundring the numbtlrs in the cvlumn hond Series
51 ppOfil th~ number of aUcnts lQr that session ws 5 this would mean thllt two rJlS ~ lst be 6ubllIitt~dl the first filled uF 1 tltgt 25 And the laquoIncond 1 to 10 Th~ cal bon ofies should bo st~plod togother at thu t0P l~rt h4nd corner of the torm ard ktpt in the Clinic filo lou IIlU6t stapl~ the originftls in the 8~~ monnshyer for lIub~ssion to the ofticl
ie h~ ll idontiflctior- (cc 1 - )
0 lot Ji 9 anythin~ hGro poundhia is int(mdClc for tha computer code
2 ~~pound~ - Print clOflrly tho name of your Clinic
C1Lic Huml or - (cc 4 - 8) Evar1 Clinic Numbor has 5 digits Virite each dig t il a t$purate box
It Pai~_thllsectgdllion (00 lt) -1 1) - Dl monll 10M
lw) bolte IlrO proY140d fetr olAoh pr 01 thQ dISh Enter tho dA) ldns a R
d16ih
emiddot5middot (0 11 I for 115t ( 0 21 for 5th etc Treat month the am pay
e ~ 10 ~ I for I-hrch 0 [2] for September Tho y~nr must be (into ad
I Z I ~ I I 71 q etc
Take as in IixulIple tho dOlte 3rd tllrch 1973 7~ie must bo written
[0131 LSLDI[7l3JDny Month Ye~r
5middot 1~J $~~ - Irom ~-------- To --------shytntol hOI II the time the Clinic 111118 in SW5sion emiddot8middot
(i) 11011 500 lm To 1200 non
(11) Frclt 100 pm To 400 pm
(iii ) IX-OG OO pllI To 6~00 pm
f
2
ADEJ ) Paae ) of S
6 Eov
_ 1hA 1gtIpoundC iIIUlt be nu~o7Ifd tler1ally 1 throurh n lU tbey Are Wled In ~1l8ellJ IInel 1301 tlU 1 Orcl 1 Wled tor a o5038ioll - -I 2 tonY tho _boul~ b I1WJbtl 1 and 2
hlrlll are 25 linos OIl the fOnl Ilnd thoae muet be UBtleS for 25 clients 9 one ior bullbull 01 I ini
ot ~h lc II ol1cM lOlivpound til e linic before soeinc DurOI or doc tor ilnc ii hox rristrltltion nUlJbet had alrearll been recorded on the Dai 1y Roiuter then n line ~hollld be drawn through that entry an1 the eliort nust not 06 includttd in tho totals tor that 0eDion
1lw Ileifitration Num)~r of cueh client must be IiIritten IS n 5-dlrlt oode ClhnC IH11IlElr 315 1IIU8 tborotore be enterod 18J010117]5]
~ Clt ZOt
Coda 1 Codo
10 ~tl c 2t j co 21)
~w elSe - Coda 1 0) d CltaEl - Code 2 Revislt Code 3
Only pound1 01 theBe coiles may be usod
11 prol-O~ ~Eil~1 (cc 22)
If ma climt was L drop-out IIho haoS returned now to the Clinio tor tho first no linmiddot bullwin lt1ro1eo o t he or she should be given CCe 1 It this do 5 II It nprlly leu this colWlln blank
u Hothod middothisllill loe 23)
NOh til t otly ~ Cod 16 tp he ontered in 2lpound of the columna oven thOUGh 10 co11lllJlB 10 provided on the torm The Codes llrol-
Oral Contraceptive Code 0 1 U D Code 1 Condom plUD Codo Z Condor (only) Code 3 Foum tAblets cream Code it DitphrClGJII Code 5 Rhythm Cde 6 Injectible Code 7 Advice Code 8 Other Code 9
It for middotDo-le 1 client rlllll ji yen cclldorls ord foam or creall Iou Qust entor Coole i (condom plulJ) in the appropri~te column This Quat be the only lIotmiddot) tarcie If an in the cnse of a tlnle clinic I the client is Bup)lieu lith COIlOrW only you rmot entEr CorlQ 3 (cpndolll) Do not use a ticII ~ tho (odo Nwber
It is CUi tomary fur 11 cliont 110 is beine put on the oral contraceptive for the first tiT1o and even on other occasionn be issued condoms and 11 crelle or foam a Ilell rI3 a pgtcket of pilla In such Cllses when the piDQ Ilre Ilctually iouou you tlust record Orll (Co~e 0) 08 tho onll metbod ilo othor ntry sll0uld ho nnrlo
Uovever n SJC~ canas vucru condoms and fOHa ~rc eiven but no pilJa (even thoJRh _t _n the intention to issue pills nt the noxt vioit) than the Mothol Th5 ifli t ohoulcl be recorded uo Condor Plus (Code 2)
13 Seen Bybullbullbullbullbull
~rot S-1 SO l
Doctor (Dr) - Code 1 j Nurse (Nul ) - Code 2
Clark (Olk-) - Code If tho Clhnt is vcen hy both tho llootor tlnd the Nurse enter Code 1 t Doctor It 6~61l by the Nurso only arite Code 2 Cod bullbull Cerk is l)llnt for FA Cllnica Clerks in tho Government Cli1t hiwo Llttoll istructed not to i56uo supplios on their own volition
14 fl221~
lhio S~tiCl of -Ie fvrtl t~ke 16 (llrci coluMna (cc 25-+0) nnd 10 tho only part at th iOIQ in llich iore thAn one cod is Zlccoptl1blo Tho purpoco of the )ecton is to 0 able to arrive nt the Cjunntity of 6tock dilltlitJutshyed YOI IIlUdt writo in the CllllOjH-iata colulna the nUllbJr of Il1ch 4rtic1o i~JSu~d ~lo e ha I Oral Contrcilpti vea are aub-di vi dod into types ae_ 3 PIllCKC 9 0 Elynnn LlUot be entered Codo in card column 25
If tor eXllrplc t l cliunt is iosued wi th packots of Zucynon nnd aJ(1 ~ivn 1 conuotll (8inoloo) you ouot enter in oard column 25 and 11 It
cnrd col~8 )2 and J (io 1 in card colucn 2 nnd 2 1n card coluun 33) Nota C)lldoIlU ale to b(t ruoordod individually not os packots of throo) Should n ne LlondoClo be isoued thil3 is to be rc-Qed as 09
If It clint 6 t~ot isoued Blly lIupplies thon you must writo Codo 1 in CQllAlilD 41
It Q eli nt isite the clinic to check on her LUD or her Diaphra~t IUId ro DI W 6 ppl ills nre ispounducd then Code 1 1s wri t ten in column 40
In the FA clinios here a variety ot orll contraceptiveo in orer~l tho elerll wilmiddot~ bJ provided with a specill code shoot The idontifyin coo will b wiittn in Column 29 nnd the nUlber of packets iosued in colwm )0
lralaer-In Code 1 lrllllsie r~ut Coda 2 leIllPQrArr Trnnsfer-In Codo gt
In the cao of n 2ratl8fcr-In I you lUot n160 cOrlpleto coluons 42-51
In the cllU J of A ~~emporary TranGfor-1n (an individual who i8 only v1citing fur clinic tor some epecial trcatcont hna who will bo rdnlnin
~middot(II~~~fO~l~SIl~I3~nn~~~h~rO~nh~1~~190~~nll 2-46 and ler rei IItrntion numbu in colullnll41-51
It the oli( nt i iNt a CrllnoforwIu - Out or loClporu1 tMn loave oolumn 1 blank
16 lr4nst(gtr-tl2~~morrry TilJnder-In (co 42-51) Forl1ltl CUn E1~ (cc 112-46)
hen you rei iatlr L irllsfcrln or Il TJlporary Trnnsfer-In you IIIUBt write I ere the five-digit clinio nucbor of the Clinic iraQ which tho ltlient Me (uIlO
2mer ]letr ~2n ~ (cc 47-51)
frlta fllao Clo r-~itrlltion Nuc~Er ot the client in the Former Clinic (i c bullbull th 1 Sis rnmiddotion ~UlIlh()r which the client carrics 1n the tormor clinio) bull
It tho Forrltl Ho( ist rntion Number iIJ not readily wnilnble you tluct oocpluto thtl epcciol [orlll Transfer-In Not Identifiod Dy Forrlcr RCGi(trn~ t10n Nwlbvr Or ~ flt)rCl is to be cOlplctcd for och cnso nnd th forlJO Ilubmi tted to thu )opllntion Prorrnnme Of fice tOGether with tho Dily Ro~iBtors lhwev~r should the clork leuTI of tho clint B FormlI Uocintra tion lUlllb r )0[(10 Cubmi ttinft the D1ily IOCI otro t hen the nUQbcr shoulo bo -ri ton in colucns 47-51 lna the special foro should lJo deotroyotl
l7 bullbullbullbullbull
r lt bull bull
ADXI ) Pap S ot S
11 UD LV~ (cc 525)
It tb( cliont io ~ivQn An IUD tor the firot tl~o then you should Sri to Codo 1 Inuort ill colurJI 52
It tho olimiddotsnt ia rvinGgtrtltld i th An I UD bullbull tben wse Coda 2 RelnDltlrt shyin (01Uil11 52
It the clLmt is ~tte~~dint chnic beruse her IUD CflClQ out by Haol (cxpll Iion i ~hcn fir te todo ~- UIlllrli1 53~
If c-ltr IU fj IIIS reov in -ne cllnic by tho doctor or nurso t~on vlritI Codec in column 5
II the eli nt otends eiLlie tld explin[l th(lt she rccovcd the IUD tlllleel nen write Coda H in Colwlm 53
It the IUD jr still within the uterus nd the WOIraquoI1 1 11rc6llJlnt thon lIrite 1gt40 4 in Column 53
lZ np h5t (ce 54) It 0 Pull 5mor ie t~ken durin thi visit tben Codo 1 ehould be ampDtere4 in ColWlln 54 Should he c110nt lltt rQ(uircd to rttturn to clin1c for a rogtol1t Pnl) t06t then CoLe 2 llhould bo middotwrittcn in column 54
It no Pllp Scou io taken tde visit Itove colUQn 54 blank
Iraferti1lli (CQ 55)
Ii the e liett io nl1 infortili tr eaoe use Cor1o Ill in colUQn 55
If tbia 1000 not tlpl lonve column 55 blonk
20 Totaltll
CO~1ploete the [)ldegO 1gty puti YI tne totals betweon the double lines nt tu b()ttctl Carrj colUlllnc 20 21 nd gt4 Must hlve tho Bnoe JllIIber and thiG Would coreslonc to the numocr ir attencbnco
Writ$ th to1ul nUlllior of Drop-Outs returned (c022)
Urito 41eo tb totnls fOJ each card column 0 to 9 under tho h(adinu Method thiB Vioit Show tho tote L fgtr OlCl type of contraceptive issued (cc 25-40)
1)0 Dot wrLte 1111 totll lUl(Ier Card Columns 15-19 29 41-51
21 COPmllh bull ~lt h~t~ Monthly ROilort
OQ thG DaLl oCator forlll thnt ccrrOspOldB to tho 1(8t 1$06610n lt 0
oth yo Olllt (vwlgtleto the items nt the botto of the [orampl This is tour ontll~1 n(olt nnd includcD tho totll lumber of sesions Ilntl tho total Iluolcr ( r crop-outs durinr the Qonth
An tiUlsilt n drir which n doctor liB in nttcndnncc is a doctor sOfll~1on and shoulc 00 re(liGtcnd in coltns 56-57 All other sessions 1116 conlliid~recl supply stllciona and thtlY 1110 rocordod in columns 58-59
the total Ilum)nl Jf drop-outo ld the drop-outs by method durinc the onth nre 10 bu oltorou in the inrlicllted boxes
72 Chad Your ~
Milke I ura th t all thE fijul4gtu rre c101r -tNever writo our nutlUQrS 50 InrjEl that they oxtend out of tho
ap~rotr1ato ~ox
Cheek to BoJa tht 1111 numuors 1110 in tho correct boxes -- CJslHloially when Writi1 the totlB
Mllxe Cirtc O thmiddott t1e infoT1I1ntion i6 clear on the corbon COllY before sep rmiddotinr the sheets
Jitn the Fomiddotl lien tly sien YOUl nr me 1t the bot tOil right hnnd corner btl forc subol ttinG it Keep tle CL rb n copy for your rocordn
i
-l ________~~---------~
I _1
Adminiatr-atlve SKVieu
P inba ~~~l1cal lrlnbin~~eltltcal -1 te~ra t~~rvicc (lnatittloaa)
--1- - shy -1------------_-L_ l-r-aJiil- shy _-L_tet1lal d
PlIinm1tJ8 atdUon DetalMid H8Il1tb ~ ________bull Care
-----~ Office of i
the FlIily _IPlill3 roarshy
1- - - -------RegiatUll urnr
ltIi 1 Drelttor Rcgicaat Director Souta Tabqo tacallortb ~ counu gt____ ~ (4 ouottet)
Off1ce of the Res10nal Diractoc L
r----- _L_ -- shy i I bull IREgional Ipitl I
District IIttaltb I bull Othn RelOl ond Hcpital CenteIntt itlt j In 1__ _shy-~- ---- -_j
J r Ii~lth
C~nlef
L
I Ihnlth lie I th Offlcu (1ft lc~
Coullty 1I0p1ta1
Henlth tentet
I

- 16 shy
Earh of the workers should preferably have harl a higher secondary education otherwLe 1gt junior secondalY education They should be married persons with middoti1ltt mot tl-an two or tlree children recruited from the locali ty in which they armiddot~ requlred to function Only persons who have the capaci ty to comnunl at~ and or6anl~e should c chosen A months ini tial orientation
slcu1d enable them to start functioning in the field though reshyfresher CO rSeS tvould be necesslt1ry in due course In Port-of-Spain married mer~ a1C women may be employed on a part-time basis
I Hanagement Study
428 A nanagement study of the Family Planning Program should include a sctu iny of the top m~nagement Atructure (Population Council - Office of the Fanil) PLanning Program - Principal Medical Officer for MCH and Family Planni Ig fetices) the field structure for the delivery of family planning servics (Re0ional Director - District Health Services) including the utilizlti(n if medical and paramedical personnel for adding the function of del ve y )f family planning services and the control and communication proCed1reF Lfnking the top management with the field structure
429 The management consultants may study the functioning of the Popul tio I Council and advise whether it adequately serves the purpose of givini po Licy direction to the Program and if not what changes in its compo itt m and operating procedures may be introduced without altering its bsic craracter as an advisory agency The consultants may suggest an alern at ve form of organizati)n and utilization of personnel which in thir p nion may be better adapted to the needs of the Program
430 Irrespective of whether the Population Council is maintained or it is replaced by an agency of a different character a formation like the Offic of be Family Planning Program would be necessary for the administrashytion i)f 1 he program a task for which i 1 appears inadequately equipped at preselt Its obvious requirements are in the areas of program monitoring and el7alnation program supervision communication and training The manag ememiddotlt consultants may study the structure and procedures of this form~ tio Gnd make suggestions with regard to the augmentation of professional and ~ upp)rt lng staffgt and modification of operating procedures
431 The linkage of the Office of the Family Planning Program with the Miniutry of Health (Central Office) and the District Health Services should be sudied In view of the policy of the Government to integrate MCH and faI11iLy rlallning services it should be examined whether the Principal Medi al Officer for Communi ty Heal th Services (MCH and Family Planning) should be agtpoj nt~d as the Chief of the Office of the Family Planning Program and an adTlilistrative officer of a suitable level inducted in that Office to assist him TIle implication of this suggestion is that the head of the Family PlanJling Program would control the District Health Services
- 17 shy
432 rf 1e management consultants should examine the delegation of adminshyistratiie Bld financial powers of the Ministry of Health to different levels of Progam aclrlirdstration viz bull PMO Program Office Regional Director and County ~djca~ Officers
l33 he system of 01 af Togram information from the clinlcs to the Pr()~ra1 O~fice and tOile processing and use of information in the latter office iholld )e studied
434 he working procedures at the integrated McP and family planning clinics shnuLl be studied This would involve a study of each stage which a clien tpcticmt has to go through from the point of entry to the point of exit after receiving advice service or supplies This study shoulci lead to star dartization of procedures and functions and evolution of -lork norms CognatE st tdies of the working procedures at uni-purpose family planning clinics and su~ply SEssions should also be undertaken An essential component of these ~ tad ~es would be to examine Nhich functions currently performed by docshytors lealh visitors nurses and midives respectively hav~ become so roushytinize ttl it they can he relegated (0 the next 10Her level
435 Reated to working procedures is the problem of job description of medcal 8nd parrunedical personnel involved in family planning from the centra i tc the field level This job description needs to be studied wi th a vie VIW8Id txaminiDg the uttlization of skills and allocation of time by the staff lcc(rd~ng to the functional prj ori ties
436 frV management consultants should study the workings of the curren slralgements fOJ family planning counselling under the Post-Partul11 Post-Abortal Education and Referral Program at the Port-of-Spain and San Fenaldo General Hospitals
437 SU1ect to the ItBrcement of the Gove1nment the management conshy8ultal ts ~hOLlld undertake a study of th requirement of field workers (home vinitcru) in tmtlUI of are nnd population cov(ra~e
ANNEX 1
Names of Persons Met
Ii Mr T C Taitt Pem1(H~nt 3~crtarY) Ministry of Health
2 Dr M n Henry Chitd Medical Officer Ministry of Health
Ellubeth Quam a Prindpal Medical Officer (1S)
4 Mr G Z Jaine ~ uJiector Population Council
5 Dr Norma Andrews Medical Officer Population Council
6 Mr Jc~n Coury~ Evaluation Adviser Population Council
7 Mr A Jriseph Principal Statistical Officer Population Council
8 Dr C 0 Colman Country Representative Pan American Health )rg ni~ation
9 Mr ranca Kippel Health Education Specialist Ministry of Iea th
10 (1 bullbullines Principal Nursing Officer Ministry of Health
11 Dr Mx won (formerlyHinistry of Health)
12 M3 late Carops Ex-Chairman of Population Council
--
4i 1_ middotIIlt F-ntCWclOotf_Y v OJ t tl
GOVIIlHMEIgt(I OF TINIOAD AND TOampAGQ - NNISTJY OF HIALftf AIJIE1 2NATIONAL FAMilY PLANNING PROGRAMME
F MIL Y PLANNING CUNIC CASE CARD - NEW CASES - NFPPl
li ~~___ 1 ________
~ ecll-U
-- --------------------- shy~) ~~middot~------------------~~~~~~---CIJ------ middot~ii--middot-middot----middot-middot---middot--------- shy
ltv Writt N_ 01(111________________
a ~4itiJtmiddotl_____ ilIIIltIoI~____~____~-__----- shybull ~4
fie l$ - JO tDql IIfIA- tr-JMimiddot _ iJ 1 Odoor o
14aorielaquol_ _~ 0 lio witIleo-La ~ 01 bull - OJ ( _01 1~ltgt1lh o bull- 0$
AacJcu 0 2 CIIriIWA 0 J Os 0
Yv~MONTH ltnollOf~nfIGHTI
Undu 1100U$ Utgtdn 5SCI Undu 11200 01 ~ 50 - 9949 amp100 - 1199 02UlOO - nn9E~ (
0)~ 10- $99 SiOO -- U9~ lOO -- U99 12400 - 1359)-------_-r----shy ~l)o SIS n600 - Hm1300 -- 019 OJ200 il~9 ~------ 99~ a 1)0 m Os1)00 -- l99 1400 -shy $4100 -- 1S999r--- shy
1500 donl S6000aad O399 - lt499I~- I 0lt
ltII
IJ -IC _~tltlioltgti lS
02 IaampJIIocI OJ 04 laM Os
w Oltwio I_-l(~u IrIaa U
h~~ ~Clubl 01 OJ
IS ~C-n 01 toSIitDI 02
Ji poundI on 01 IriIIIuy M ur 02 IV OJ
WU 10 pltIoII~ llaMtl 411 cIIiId 01 Ol it fIolto ~ do~ _14 rou IIlgtJo 1Ia1 ___~_ shy
40
It _ I 00 ~bull FPIiIJ 1
OJ 02 OJ 06
)0 III- iy wOWcf ~1
aMIIl Os
11 T 1gtlt ( h _______ 4)~
06
04 (MIbullbull middot bIrlI ~___~__~_ (-fIJI ~- -~-- (1HJ 49middot SJ
U 10k 01( 1__ raquo$-4
iU1) DOl F ToWotfOlnC DOl 001 or Do [IP 006 001 OIIgtu___Spltclty DOll Nltmo 010
U1Mo I orcpmiddot laquo55middot16
1lD 001 Foam Toblelf_ICim DOl Condom DOl CoomS~ 004 oe Oos WlttuJn 1J OIkr DSpody) 101~ ~Iu 006 Rhylhm 001 DOG OJO
no wI~lmm 4 cd
(I 0) 1110 01 Condor 03 (lorn bull l S~muoidIl 04 Faa TabioolfIIltr- Os RhyUlm 01 lnJrl tible O Advico 090 06
la slt 1)0 19 loti ~rltnlt) ([)sl or 1llOn) ____ --__ bullbully-J n SV - ~JcdS
v~ Cl NCI 0 30 OJI_O I Wr blJ1h 0 I ~ OJ 1 ~ (fOOd V 01 No 02 laquo 6) Cf4
WIiI 1 172
004 001
j D middotmiddot middot
1 ~
r
~
bull I
bullI I I
r c i
ANNEX 3 Pagemiddot 1 of 5
0 raquo rshy -lt l)J ~ 111 t G) 5 shy (J) ~ -
fT1u
i
MINISTTY OF Ho1TH
NTIONl F~ILY LNNING PR-GRbullbullM-tE
~~5tructions to C11nic ClerKa
How to co~ploto the Daily Rogister
~~ ~~v1sd Daily Rosi8ter replnc~D tho one which is now in use tb$ Monthly PC~ri rOt~ arti tho 01( Ci() Dod PollJ j f m It is a pre-coded form and 1411 cl~1p Jd tl a1I6iniul-mIHvn Oel Clinic nctivi~y
110 )rm rollt biJ coupJot)d lrl cupLtcoto using a o(roon shoot Tho top aheot or oriinai ~ust bl) 6(Ult to tho CQgt1tral O[[lCO and tho carbon copy retained in the Gliaic rilo dll the for6a that ar uD~d betwoen the 1st 4nd the 15th of the oIIollth aut bo subClittud tocho office 35 Lnc blttch Those oomp1cted betwoon tho 16th _lid tqemc of tho month must bo ~cnt in a secJnll batch
P lOvLior hns boon Illllde for 25 clients on cZlch forlll new forlll must b IIlied f r poundh 50[810n2 whothur or not ono or lIIore session are hoIdiit the clinic on he sarne day
I th ro alO more htl 25 clionta 1n attondnnco at tho session the additi shyOhAl m~bOl of clionts 10 clients nu~ber 26 27 etc sh0u1l be ontered on the next Imiddotrlll ~i ttout a1tpoundring the numbtlrs in the cvlumn hond Series
51 ppOfil th~ number of aUcnts lQr that session ws 5 this would mean thllt two rJlS ~ lst be 6ubllIitt~dl the first filled uF 1 tltgt 25 And the laquoIncond 1 to 10 Th~ cal bon ofies should bo st~plod togother at thu t0P l~rt h4nd corner of the torm ard ktpt in the Clinic filo lou IIlU6t stapl~ the originftls in the 8~~ monnshyer for lIub~ssion to the ofticl
ie h~ ll idontiflctior- (cc 1 - )
0 lot Ji 9 anythin~ hGro poundhia is int(mdClc for tha computer code
2 ~~pound~ - Print clOflrly tho name of your Clinic
C1Lic Huml or - (cc 4 - 8) Evar1 Clinic Numbor has 5 digits Virite each dig t il a t$purate box
It Pai~_thllsectgdllion (00 lt) -1 1) - Dl monll 10M
lw) bolte IlrO proY140d fetr olAoh pr 01 thQ dISh Enter tho dA) ldns a R
d16ih
emiddot5middot (0 11 I for 115t ( 0 21 for 5th etc Treat month the am pay
e ~ 10 ~ I for I-hrch 0 [2] for September Tho y~nr must be (into ad
I Z I ~ I I 71 q etc
Take as in IixulIple tho dOlte 3rd tllrch 1973 7~ie must bo written
[0131 LSLDI[7l3JDny Month Ye~r
5middot 1~J $~~ - Irom ~-------- To --------shytntol hOI II the time the Clinic 111118 in SW5sion emiddot8middot
(i) 11011 500 lm To 1200 non
(11) Frclt 100 pm To 400 pm
(iii ) IX-OG OO pllI To 6~00 pm
f
2
ADEJ ) Paae ) of S
6 Eov
_ 1hA 1gtIpoundC iIIUlt be nu~o7Ifd tler1ally 1 throurh n lU tbey Are Wled In ~1l8ellJ IInel 1301 tlU 1 Orcl 1 Wled tor a o5038ioll - -I 2 tonY tho _boul~ b I1WJbtl 1 and 2
hlrlll are 25 linos OIl the fOnl Ilnd thoae muet be UBtleS for 25 clients 9 one ior bullbull 01 I ini
ot ~h lc II ol1cM lOlivpound til e linic before soeinc DurOI or doc tor ilnc ii hox rristrltltion nUlJbet had alrearll been recorded on the Dai 1y Roiuter then n line ~hollld be drawn through that entry an1 the eliort nust not 06 includttd in tho totals tor that 0eDion
1lw Ileifitration Num)~r of cueh client must be IiIritten IS n 5-dlrlt oode ClhnC IH11IlElr 315 1IIU8 tborotore be enterod 18J010117]5]
~ Clt ZOt
Coda 1 Codo
10 ~tl c 2t j co 21)
~w elSe - Coda 1 0) d CltaEl - Code 2 Revislt Code 3
Only pound1 01 theBe coiles may be usod
11 prol-O~ ~Eil~1 (cc 22)
If ma climt was L drop-out IIho haoS returned now to the Clinio tor tho first no linmiddot bullwin lt1ro1eo o t he or she should be given CCe 1 It this do 5 II It nprlly leu this colWlln blank
u Hothod middothisllill loe 23)
NOh til t otly ~ Cod 16 tp he ontered in 2lpound of the columna oven thOUGh 10 co11lllJlB 10 provided on the torm The Codes llrol-
Oral Contraceptive Code 0 1 U D Code 1 Condom plUD Codo Z Condor (only) Code 3 Foum tAblets cream Code it DitphrClGJII Code 5 Rhythm Cde 6 Injectible Code 7 Advice Code 8 Other Code 9
It for middotDo-le 1 client rlllll ji yen cclldorls ord foam or creall Iou Qust entor Coole i (condom plulJ) in the appropri~te column This Quat be the only lIotmiddot) tarcie If an in the cnse of a tlnle clinic I the client is Bup)lieu lith COIlOrW only you rmot entEr CorlQ 3 (cpndolll) Do not use a ticII ~ tho (odo Nwber
It is CUi tomary fur 11 cliont 110 is beine put on the oral contraceptive for the first tiT1o and even on other occasionn be issued condoms and 11 crelle or foam a Ilell rI3 a pgtcket of pilla In such Cllses when the piDQ Ilre Ilctually iouou you tlust record Orll (Co~e 0) 08 tho onll metbod ilo othor ntry sll0uld ho nnrlo
Uovever n SJC~ canas vucru condoms and fOHa ~rc eiven but no pilJa (even thoJRh _t _n the intention to issue pills nt the noxt vioit) than the Mothol Th5 ifli t ohoulcl be recorded uo Condor Plus (Code 2)
13 Seen Bybullbullbullbullbull
~rot S-1 SO l
Doctor (Dr) - Code 1 j Nurse (Nul ) - Code 2
Clark (Olk-) - Code If tho Clhnt is vcen hy both tho llootor tlnd the Nurse enter Code 1 t Doctor It 6~61l by the Nurso only arite Code 2 Cod bullbull Cerk is l)llnt for FA Cllnica Clerks in tho Government Cli1t hiwo Llttoll istructed not to i56uo supplios on their own volition
14 fl221~
lhio S~tiCl of -Ie fvrtl t~ke 16 (llrci coluMna (cc 25-+0) nnd 10 tho only part at th iOIQ in llich iore thAn one cod is Zlccoptl1blo Tho purpoco of the )ecton is to 0 able to arrive nt the Cjunntity of 6tock dilltlitJutshyed YOI IIlUdt writo in the CllllOjH-iata colulna the nUllbJr of Il1ch 4rtic1o i~JSu~d ~lo e ha I Oral Contrcilpti vea are aub-di vi dod into types ae_ 3 PIllCKC 9 0 Elynnn LlUot be entered Codo in card column 25
If tor eXllrplc t l cliunt is iosued wi th packots of Zucynon nnd aJ(1 ~ivn 1 conuotll (8inoloo) you ouot enter in oard column 25 and 11 It
cnrd col~8 )2 and J (io 1 in card colucn 2 nnd 2 1n card coluun 33) Nota C)lldoIlU ale to b(t ruoordod individually not os packots of throo) Should n ne LlondoClo be isoued thil3 is to be rc-Qed as 09
If It clint 6 t~ot isoued Blly lIupplies thon you must writo Codo 1 in CQllAlilD 41
It Q eli nt isite the clinic to check on her LUD or her Diaphra~t IUId ro DI W 6 ppl ills nre ispounducd then Code 1 1s wri t ten in column 40
In the FA clinios here a variety ot orll contraceptiveo in orer~l tho elerll wilmiddot~ bJ provided with a specill code shoot The idontifyin coo will b wiittn in Column 29 nnd the nUlber of packets iosued in colwm )0
lralaer-In Code 1 lrllllsie r~ut Coda 2 leIllPQrArr Trnnsfer-In Codo gt
In the cao of n 2ratl8fcr-In I you lUot n160 cOrlpleto coluons 42-51
In the cllU J of A ~~emporary TranGfor-1n (an individual who i8 only v1citing fur clinic tor some epecial trcatcont hna who will bo rdnlnin
~middot(II~~~fO~l~SIl~I3~nn~~~h~rO~nh~1~~190~~nll 2-46 and ler rei IItrntion numbu in colullnll41-51
It the oli( nt i iNt a CrllnoforwIu - Out or loClporu1 tMn loave oolumn 1 blank
16 lr4nst(gtr-tl2~~morrry TilJnder-In (co 42-51) Forl1ltl CUn E1~ (cc 112-46)
hen you rei iatlr L irllsfcrln or Il TJlporary Trnnsfer-In you IIIUBt write I ere the five-digit clinio nucbor of the Clinic iraQ which tho ltlient Me (uIlO
2mer ]letr ~2n ~ (cc 47-51)
frlta fllao Clo r-~itrlltion Nuc~Er ot the client in the Former Clinic (i c bullbull th 1 Sis rnmiddotion ~UlIlh()r which the client carrics 1n the tormor clinio) bull
It tho Forrltl Ho( ist rntion Number iIJ not readily wnilnble you tluct oocpluto thtl epcciol [orlll Transfer-In Not Identifiod Dy Forrlcr RCGi(trn~ t10n Nwlbvr Or ~ flt)rCl is to be cOlplctcd for och cnso nnd th forlJO Ilubmi tted to thu )opllntion Prorrnnme Of fice tOGether with tho Dily Ro~iBtors lhwev~r should the clork leuTI of tho clint B FormlI Uocintra tion lUlllb r )0[(10 Cubmi ttinft the D1ily IOCI otro t hen the nUQbcr shoulo bo -ri ton in colucns 47-51 lna the special foro should lJo deotroyotl
l7 bullbullbullbullbull
r lt bull bull
ADXI ) Pap S ot S
11 UD LV~ (cc 525)
It tb( cliont io ~ivQn An IUD tor the firot tl~o then you should Sri to Codo 1 Inuort ill colurJI 52
It tho olimiddotsnt ia rvinGgtrtltld i th An I UD bullbull tben wse Coda 2 RelnDltlrt shyin (01Uil11 52
It the clLmt is ~tte~~dint chnic beruse her IUD CflClQ out by Haol (cxpll Iion i ~hcn fir te todo ~- UIlllrli1 53~
If c-ltr IU fj IIIS reov in -ne cllnic by tho doctor or nurso t~on vlritI Codec in column 5
II the eli nt otends eiLlie tld explin[l th(lt she rccovcd the IUD tlllleel nen write Coda H in Colwlm 53
It the IUD jr still within the uterus nd the WOIraquoI1 1 11rc6llJlnt thon lIrite 1gt40 4 in Column 53
lZ np h5t (ce 54) It 0 Pull 5mor ie t~ken durin thi visit tben Codo 1 ehould be ampDtere4 in ColWlln 54 Should he c110nt lltt rQ(uircd to rttturn to clin1c for a rogtol1t Pnl) t06t then CoLe 2 llhould bo middotwrittcn in column 54
It no Pllp Scou io taken tde visit Itove colUQn 54 blank
Iraferti1lli (CQ 55)
Ii the e liett io nl1 infortili tr eaoe use Cor1o Ill in colUQn 55
If tbia 1000 not tlpl lonve column 55 blonk
20 Totaltll
CO~1ploete the [)ldegO 1gty puti YI tne totals betweon the double lines nt tu b()ttctl Carrj colUlllnc 20 21 nd gt4 Must hlve tho Bnoe JllIIber and thiG Would coreslonc to the numocr ir attencbnco
Writ$ th to1ul nUlllior of Drop-Outs returned (c022)
Urito 41eo tb totnls fOJ each card column 0 to 9 under tho h(adinu Method thiB Vioit Show tho tote L fgtr OlCl type of contraceptive issued (cc 25-40)
1)0 Dot wrLte 1111 totll lUl(Ier Card Columns 15-19 29 41-51
21 COPmllh bull ~lt h~t~ Monthly ROilort
OQ thG DaLl oCator forlll thnt ccrrOspOldB to tho 1(8t 1$06610n lt 0
oth yo Olllt (vwlgtleto the items nt the botto of the [orampl This is tour ontll~1 n(olt nnd includcD tho totll lumber of sesions Ilntl tho total Iluolcr ( r crop-outs durinr the Qonth
An tiUlsilt n drir which n doctor liB in nttcndnncc is a doctor sOfll~1on and shoulc 00 re(liGtcnd in coltns 56-57 All other sessions 1116 conlliid~recl supply stllciona and thtlY 1110 rocordod in columns 58-59
the total Ilum)nl Jf drop-outo ld the drop-outs by method durinc the onth nre 10 bu oltorou in the inrlicllted boxes
72 Chad Your ~
Milke I ura th t all thE fijul4gtu rre c101r -tNever writo our nutlUQrS 50 InrjEl that they oxtend out of tho
ap~rotr1ato ~ox
Cheek to BoJa tht 1111 numuors 1110 in tho correct boxes -- CJslHloially when Writi1 the totlB
Mllxe Cirtc O thmiddott t1e infoT1I1ntion i6 clear on the corbon COllY before sep rmiddotinr the sheets
Jitn the Fomiddotl lien tly sien YOUl nr me 1t the bot tOil right hnnd corner btl forc subol ttinG it Keep tle CL rb n copy for your rocordn
i
-l ________~~---------~
I _1
Adminiatr-atlve SKVieu
P inba ~~~l1cal lrlnbin~~eltltcal -1 te~ra t~~rvicc (lnatittloaa)
--1- - shy -1------------_-L_ l-r-aJiil- shy _-L_tet1lal d
PlIinm1tJ8 atdUon DetalMid H8Il1tb ~ ________bull Care
-----~ Office of i
the FlIily _IPlill3 roarshy
1- - - -------RegiatUll urnr
ltIi 1 Drelttor Rcgicaat Director Souta Tabqo tacallortb ~ counu gt____ ~ (4 ouottet)
Off1ce of the Res10nal Diractoc L
r----- _L_ -- shy i I bull IREgional Ipitl I
District IIttaltb I bull Othn RelOl ond Hcpital CenteIntt itlt j In 1__ _shy-~- ---- -_j
J r Ii~lth
C~nlef
L
I Ihnlth lie I th Offlcu (1ft lc~
Coullty 1I0p1ta1
Henlth tentet
I

- 17 shy
432 rf 1e management consultants should examine the delegation of adminshyistratiie Bld financial powers of the Ministry of Health to different levels of Progam aclrlirdstration viz bull PMO Program Office Regional Director and County ~djca~ Officers
l33 he system of 01 af Togram information from the clinlcs to the Pr()~ra1 O~fice and tOile processing and use of information in the latter office iholld )e studied
434 he working procedures at the integrated McP and family planning clinics shnuLl be studied This would involve a study of each stage which a clien tpcticmt has to go through from the point of entry to the point of exit after receiving advice service or supplies This study shoulci lead to star dartization of procedures and functions and evolution of -lork norms CognatE st tdies of the working procedures at uni-purpose family planning clinics and su~ply SEssions should also be undertaken An essential component of these ~ tad ~es would be to examine Nhich functions currently performed by docshytors lealh visitors nurses and midives respectively hav~ become so roushytinize ttl it they can he relegated (0 the next 10Her level
435 Reated to working procedures is the problem of job description of medcal 8nd parrunedical personnel involved in family planning from the centra i tc the field level This job description needs to be studied wi th a vie VIW8Id txaminiDg the uttlization of skills and allocation of time by the staff lcc(rd~ng to the functional prj ori ties
436 frV management consultants should study the workings of the curren slralgements fOJ family planning counselling under the Post-Partul11 Post-Abortal Education and Referral Program at the Port-of-Spain and San Fenaldo General Hospitals
437 SU1ect to the ItBrcement of the Gove1nment the management conshy8ultal ts ~hOLlld undertake a study of th requirement of field workers (home vinitcru) in tmtlUI of are nnd population cov(ra~e
ANNEX 1
Names of Persons Met
Ii Mr T C Taitt Pem1(H~nt 3~crtarY) Ministry of Health
2 Dr M n Henry Chitd Medical Officer Ministry of Health
Ellubeth Quam a Prindpal Medical Officer (1S)
4 Mr G Z Jaine ~ uJiector Population Council
5 Dr Norma Andrews Medical Officer Population Council
6 Mr Jc~n Coury~ Evaluation Adviser Population Council
7 Mr A Jriseph Principal Statistical Officer Population Council
8 Dr C 0 Colman Country Representative Pan American Health )rg ni~ation
9 Mr ranca Kippel Health Education Specialist Ministry of Iea th
10 (1 bullbullines Principal Nursing Officer Ministry of Health
11 Dr Mx won (formerlyHinistry of Health)
12 M3 late Carops Ex-Chairman of Population Council
--
4i 1_ middotIIlt F-ntCWclOotf_Y v OJ t tl
GOVIIlHMEIgt(I OF TINIOAD AND TOampAGQ - NNISTJY OF HIALftf AIJIE1 2NATIONAL FAMilY PLANNING PROGRAMME
F MIL Y PLANNING CUNIC CASE CARD - NEW CASES - NFPPl
li ~~___ 1 ________
~ ecll-U
-- --------------------- shy~) ~~middot~------------------~~~~~~---CIJ------ middot~ii--middot-middot----middot-middot---middot--------- shy
ltv Writt N_ 01(111________________
a ~4itiJtmiddotl_____ ilIIIltIoI~____~____~-__----- shybull ~4
fie l$ - JO tDql IIfIA- tr-JMimiddot _ iJ 1 Odoor o
14aorielaquol_ _~ 0 lio witIleo-La ~ 01 bull - OJ ( _01 1~ltgt1lh o bull- 0$
AacJcu 0 2 CIIriIWA 0 J Os 0
Yv~MONTH ltnollOf~nfIGHTI
Undu 1100U$ Utgtdn 5SCI Undu 11200 01 ~ 50 - 9949 amp100 - 1199 02UlOO - nn9E~ (
0)~ 10- $99 SiOO -- U9~ lOO -- U99 12400 - 1359)-------_-r----shy ~l)o SIS n600 - Hm1300 -- 019 OJ200 il~9 ~------ 99~ a 1)0 m Os1)00 -- l99 1400 -shy $4100 -- 1S999r--- shy
1500 donl S6000aad O399 - lt499I~- I 0lt
ltII
IJ -IC _~tltlioltgti lS
02 IaampJIIocI OJ 04 laM Os
w Oltwio I_-l(~u IrIaa U
h~~ ~Clubl 01 OJ
IS ~C-n 01 toSIitDI 02
Ji poundI on 01 IriIIIuy M ur 02 IV OJ
WU 10 pltIoII~ llaMtl 411 cIIiId 01 Ol it fIolto ~ do~ _14 rou IIlgtJo 1Ia1 ___~_ shy
40
It _ I 00 ~bull FPIiIJ 1
OJ 02 OJ 06
)0 III- iy wOWcf ~1
aMIIl Os
11 T 1gtlt ( h _______ 4)~
06
04 (MIbullbull middot bIrlI ~___~__~_ (-fIJI ~- -~-- (1HJ 49middot SJ
U 10k 01( 1__ raquo$-4
iU1) DOl F ToWotfOlnC DOl 001 or Do [IP 006 001 OIIgtu___Spltclty DOll Nltmo 010
U1Mo I orcpmiddot laquo55middot16
1lD 001 Foam Toblelf_ICim DOl Condom DOl CoomS~ 004 oe Oos WlttuJn 1J OIkr DSpody) 101~ ~Iu 006 Rhylhm 001 DOG OJO
no wI~lmm 4 cd
(I 0) 1110 01 Condor 03 (lorn bull l S~muoidIl 04 Faa TabioolfIIltr- Os RhyUlm 01 lnJrl tible O Advico 090 06
la slt 1)0 19 loti ~rltnlt) ([)sl or 1llOn) ____ --__ bullbully-J n SV - ~JcdS
v~ Cl NCI 0 30 OJI_O I Wr blJ1h 0 I ~ OJ 1 ~ (fOOd V 01 No 02 laquo 6) Cf4
WIiI 1 172
004 001
j D middotmiddot middot
1 ~
r
~
bull I
bullI I I
r c i
ANNEX 3 Pagemiddot 1 of 5
0 raquo rshy -lt l)J ~ 111 t G) 5 shy (J) ~ -
fT1u
i
MINISTTY OF Ho1TH
NTIONl F~ILY LNNING PR-GRbullbullM-tE
~~5tructions to C11nic ClerKa
How to co~ploto the Daily Rogister
~~ ~~v1sd Daily Rosi8ter replnc~D tho one which is now in use tb$ Monthly PC~ri rOt~ arti tho 01( Ci() Dod PollJ j f m It is a pre-coded form and 1411 cl~1p Jd tl a1I6iniul-mIHvn Oel Clinic nctivi~y
110 )rm rollt biJ coupJot)d lrl cupLtcoto using a o(roon shoot Tho top aheot or oriinai ~ust bl) 6(Ult to tho CQgt1tral O[[lCO and tho carbon copy retained in the Gliaic rilo dll the for6a that ar uD~d betwoen the 1st 4nd the 15th of the oIIollth aut bo subClittud tocho office 35 Lnc blttch Those oomp1cted betwoon tho 16th _lid tqemc of tho month must bo ~cnt in a secJnll batch
P lOvLior hns boon Illllde for 25 clients on cZlch forlll new forlll must b IIlied f r poundh 50[810n2 whothur or not ono or lIIore session are hoIdiit the clinic on he sarne day
I th ro alO more htl 25 clionta 1n attondnnco at tho session the additi shyOhAl m~bOl of clionts 10 clients nu~ber 26 27 etc sh0u1l be ontered on the next Imiddotrlll ~i ttout a1tpoundring the numbtlrs in the cvlumn hond Series
51 ppOfil th~ number of aUcnts lQr that session ws 5 this would mean thllt two rJlS ~ lst be 6ubllIitt~dl the first filled uF 1 tltgt 25 And the laquoIncond 1 to 10 Th~ cal bon ofies should bo st~plod togother at thu t0P l~rt h4nd corner of the torm ard ktpt in the Clinic filo lou IIlU6t stapl~ the originftls in the 8~~ monnshyer for lIub~ssion to the ofticl
ie h~ ll idontiflctior- (cc 1 - )
0 lot Ji 9 anythin~ hGro poundhia is int(mdClc for tha computer code
2 ~~pound~ - Print clOflrly tho name of your Clinic
C1Lic Huml or - (cc 4 - 8) Evar1 Clinic Numbor has 5 digits Virite each dig t il a t$purate box
It Pai~_thllsectgdllion (00 lt) -1 1) - Dl monll 10M
lw) bolte IlrO proY140d fetr olAoh pr 01 thQ dISh Enter tho dA) ldns a R
d16ih
emiddot5middot (0 11 I for 115t ( 0 21 for 5th etc Treat month the am pay
e ~ 10 ~ I for I-hrch 0 [2] for September Tho y~nr must be (into ad
I Z I ~ I I 71 q etc
Take as in IixulIple tho dOlte 3rd tllrch 1973 7~ie must bo written
[0131 LSLDI[7l3JDny Month Ye~r
5middot 1~J $~~ - Irom ~-------- To --------shytntol hOI II the time the Clinic 111118 in SW5sion emiddot8middot
(i) 11011 500 lm To 1200 non
(11) Frclt 100 pm To 400 pm
(iii ) IX-OG OO pllI To 6~00 pm
f
2
ADEJ ) Paae ) of S
6 Eov
_ 1hA 1gtIpoundC iIIUlt be nu~o7Ifd tler1ally 1 throurh n lU tbey Are Wled In ~1l8ellJ IInel 1301 tlU 1 Orcl 1 Wled tor a o5038ioll - -I 2 tonY tho _boul~ b I1WJbtl 1 and 2
hlrlll are 25 linos OIl the fOnl Ilnd thoae muet be UBtleS for 25 clients 9 one ior bullbull 01 I ini
ot ~h lc II ol1cM lOlivpound til e linic before soeinc DurOI or doc tor ilnc ii hox rristrltltion nUlJbet had alrearll been recorded on the Dai 1y Roiuter then n line ~hollld be drawn through that entry an1 the eliort nust not 06 includttd in tho totals tor that 0eDion
1lw Ileifitration Num)~r of cueh client must be IiIritten IS n 5-dlrlt oode ClhnC IH11IlElr 315 1IIU8 tborotore be enterod 18J010117]5]
~ Clt ZOt
Coda 1 Codo
10 ~tl c 2t j co 21)
~w elSe - Coda 1 0) d CltaEl - Code 2 Revislt Code 3
Only pound1 01 theBe coiles may be usod
11 prol-O~ ~Eil~1 (cc 22)
If ma climt was L drop-out IIho haoS returned now to the Clinio tor tho first no linmiddot bullwin lt1ro1eo o t he or she should be given CCe 1 It this do 5 II It nprlly leu this colWlln blank
u Hothod middothisllill loe 23)
NOh til t otly ~ Cod 16 tp he ontered in 2lpound of the columna oven thOUGh 10 co11lllJlB 10 provided on the torm The Codes llrol-
Oral Contraceptive Code 0 1 U D Code 1 Condom plUD Codo Z Condor (only) Code 3 Foum tAblets cream Code it DitphrClGJII Code 5 Rhythm Cde 6 Injectible Code 7 Advice Code 8 Other Code 9
It for middotDo-le 1 client rlllll ji yen cclldorls ord foam or creall Iou Qust entor Coole i (condom plulJ) in the appropri~te column This Quat be the only lIotmiddot) tarcie If an in the cnse of a tlnle clinic I the client is Bup)lieu lith COIlOrW only you rmot entEr CorlQ 3 (cpndolll) Do not use a ticII ~ tho (odo Nwber
It is CUi tomary fur 11 cliont 110 is beine put on the oral contraceptive for the first tiT1o and even on other occasionn be issued condoms and 11 crelle or foam a Ilell rI3 a pgtcket of pilla In such Cllses when the piDQ Ilre Ilctually iouou you tlust record Orll (Co~e 0) 08 tho onll metbod ilo othor ntry sll0uld ho nnrlo
Uovever n SJC~ canas vucru condoms and fOHa ~rc eiven but no pilJa (even thoJRh _t _n the intention to issue pills nt the noxt vioit) than the Mothol Th5 ifli t ohoulcl be recorded uo Condor Plus (Code 2)
13 Seen Bybullbullbullbullbull
~rot S-1 SO l
Doctor (Dr) - Code 1 j Nurse (Nul ) - Code 2
Clark (Olk-) - Code If tho Clhnt is vcen hy both tho llootor tlnd the Nurse enter Code 1 t Doctor It 6~61l by the Nurso only arite Code 2 Cod bullbull Cerk is l)llnt for FA Cllnica Clerks in tho Government Cli1t hiwo Llttoll istructed not to i56uo supplios on their own volition
14 fl221~
lhio S~tiCl of -Ie fvrtl t~ke 16 (llrci coluMna (cc 25-+0) nnd 10 tho only part at th iOIQ in llich iore thAn one cod is Zlccoptl1blo Tho purpoco of the )ecton is to 0 able to arrive nt the Cjunntity of 6tock dilltlitJutshyed YOI IIlUdt writo in the CllllOjH-iata colulna the nUllbJr of Il1ch 4rtic1o i~JSu~d ~lo e ha I Oral Contrcilpti vea are aub-di vi dod into types ae_ 3 PIllCKC 9 0 Elynnn LlUot be entered Codo in card column 25
If tor eXllrplc t l cliunt is iosued wi th packots of Zucynon nnd aJ(1 ~ivn 1 conuotll (8inoloo) you ouot enter in oard column 25 and 11 It
cnrd col~8 )2 and J (io 1 in card colucn 2 nnd 2 1n card coluun 33) Nota C)lldoIlU ale to b(t ruoordod individually not os packots of throo) Should n ne LlondoClo be isoued thil3 is to be rc-Qed as 09
If It clint 6 t~ot isoued Blly lIupplies thon you must writo Codo 1 in CQllAlilD 41
It Q eli nt isite the clinic to check on her LUD or her Diaphra~t IUId ro DI W 6 ppl ills nre ispounducd then Code 1 1s wri t ten in column 40
In the FA clinios here a variety ot orll contraceptiveo in orer~l tho elerll wilmiddot~ bJ provided with a specill code shoot The idontifyin coo will b wiittn in Column 29 nnd the nUlber of packets iosued in colwm )0
lralaer-In Code 1 lrllllsie r~ut Coda 2 leIllPQrArr Trnnsfer-In Codo gt
In the cao of n 2ratl8fcr-In I you lUot n160 cOrlpleto coluons 42-51
In the cllU J of A ~~emporary TranGfor-1n (an individual who i8 only v1citing fur clinic tor some epecial trcatcont hna who will bo rdnlnin
~middot(II~~~fO~l~SIl~I3~nn~~~h~rO~nh~1~~190~~nll 2-46 and ler rei IItrntion numbu in colullnll41-51
It the oli( nt i iNt a CrllnoforwIu - Out or loClporu1 tMn loave oolumn 1 blank
16 lr4nst(gtr-tl2~~morrry TilJnder-In (co 42-51) Forl1ltl CUn E1~ (cc 112-46)
hen you rei iatlr L irllsfcrln or Il TJlporary Trnnsfer-In you IIIUBt write I ere the five-digit clinio nucbor of the Clinic iraQ which tho ltlient Me (uIlO
2mer ]letr ~2n ~ (cc 47-51)
frlta fllao Clo r-~itrlltion Nuc~Er ot the client in the Former Clinic (i c bullbull th 1 Sis rnmiddotion ~UlIlh()r which the client carrics 1n the tormor clinio) bull
It tho Forrltl Ho( ist rntion Number iIJ not readily wnilnble you tluct oocpluto thtl epcciol [orlll Transfer-In Not Identifiod Dy Forrlcr RCGi(trn~ t10n Nwlbvr Or ~ flt)rCl is to be cOlplctcd for och cnso nnd th forlJO Ilubmi tted to thu )opllntion Prorrnnme Of fice tOGether with tho Dily Ro~iBtors lhwev~r should the clork leuTI of tho clint B FormlI Uocintra tion lUlllb r )0[(10 Cubmi ttinft the D1ily IOCI otro t hen the nUQbcr shoulo bo -ri ton in colucns 47-51 lna the special foro should lJo deotroyotl
l7 bullbullbullbullbull
r lt bull bull
ADXI ) Pap S ot S
11 UD LV~ (cc 525)
It tb( cliont io ~ivQn An IUD tor the firot tl~o then you should Sri to Codo 1 Inuort ill colurJI 52
It tho olimiddotsnt ia rvinGgtrtltld i th An I UD bullbull tben wse Coda 2 RelnDltlrt shyin (01Uil11 52
It the clLmt is ~tte~~dint chnic beruse her IUD CflClQ out by Haol (cxpll Iion i ~hcn fir te todo ~- UIlllrli1 53~
If c-ltr IU fj IIIS reov in -ne cllnic by tho doctor or nurso t~on vlritI Codec in column 5
II the eli nt otends eiLlie tld explin[l th(lt she rccovcd the IUD tlllleel nen write Coda H in Colwlm 53
It the IUD jr still within the uterus nd the WOIraquoI1 1 11rc6llJlnt thon lIrite 1gt40 4 in Column 53
lZ np h5t (ce 54) It 0 Pull 5mor ie t~ken durin thi visit tben Codo 1 ehould be ampDtere4 in ColWlln 54 Should he c110nt lltt rQ(uircd to rttturn to clin1c for a rogtol1t Pnl) t06t then CoLe 2 llhould bo middotwrittcn in column 54
It no Pllp Scou io taken tde visit Itove colUQn 54 blank
Iraferti1lli (CQ 55)
Ii the e liett io nl1 infortili tr eaoe use Cor1o Ill in colUQn 55
If tbia 1000 not tlpl lonve column 55 blonk
20 Totaltll
CO~1ploete the [)ldegO 1gty puti YI tne totals betweon the double lines nt tu b()ttctl Carrj colUlllnc 20 21 nd gt4 Must hlve tho Bnoe JllIIber and thiG Would coreslonc to the numocr ir attencbnco
Writ$ th to1ul nUlllior of Drop-Outs returned (c022)
Urito 41eo tb totnls fOJ each card column 0 to 9 under tho h(adinu Method thiB Vioit Show tho tote L fgtr OlCl type of contraceptive issued (cc 25-40)
1)0 Dot wrLte 1111 totll lUl(Ier Card Columns 15-19 29 41-51
21 COPmllh bull ~lt h~t~ Monthly ROilort
OQ thG DaLl oCator forlll thnt ccrrOspOldB to tho 1(8t 1$06610n lt 0
oth yo Olllt (vwlgtleto the items nt the botto of the [orampl This is tour ontll~1 n(olt nnd includcD tho totll lumber of sesions Ilntl tho total Iluolcr ( r crop-outs durinr the Qonth
An tiUlsilt n drir which n doctor liB in nttcndnncc is a doctor sOfll~1on and shoulc 00 re(liGtcnd in coltns 56-57 All other sessions 1116 conlliid~recl supply stllciona and thtlY 1110 rocordod in columns 58-59
the total Ilum)nl Jf drop-outo ld the drop-outs by method durinc the onth nre 10 bu oltorou in the inrlicllted boxes
72 Chad Your ~
Milke I ura th t all thE fijul4gtu rre c101r -tNever writo our nutlUQrS 50 InrjEl that they oxtend out of tho
ap~rotr1ato ~ox
Cheek to BoJa tht 1111 numuors 1110 in tho correct boxes -- CJslHloially when Writi1 the totlB
Mllxe Cirtc O thmiddott t1e infoT1I1ntion i6 clear on the corbon COllY before sep rmiddotinr the sheets
Jitn the Fomiddotl lien tly sien YOUl nr me 1t the bot tOil right hnnd corner btl forc subol ttinG it Keep tle CL rb n copy for your rocordn
i
-l ________~~---------~
I _1
Adminiatr-atlve SKVieu
P inba ~~~l1cal lrlnbin~~eltltcal -1 te~ra t~~rvicc (lnatittloaa)
--1- - shy -1------------_-L_ l-r-aJiil- shy _-L_tet1lal d
PlIinm1tJ8 atdUon DetalMid H8Il1tb ~ ________bull Care
-----~ Office of i
the FlIily _IPlill3 roarshy
1- - - -------RegiatUll urnr
ltIi 1 Drelttor Rcgicaat Director Souta Tabqo tacallortb ~ counu gt____ ~ (4 ouottet)
Off1ce of the Res10nal Diractoc L
r----- _L_ -- shy i I bull IREgional Ipitl I
District IIttaltb I bull Othn RelOl ond Hcpital CenteIntt itlt j In 1__ _shy-~- ---- -_j
J r Ii~lth
C~nlef
L
I Ihnlth lie I th Offlcu (1ft lc~
Coullty 1I0p1ta1
Henlth tentet
I

ANNEX 1
Names of Persons Met
Ii Mr T C Taitt Pem1(H~nt 3~crtarY) Ministry of Health
2 Dr M n Henry Chitd Medical Officer Ministry of Health
Ellubeth Quam a Prindpal Medical Officer (1S)
4 Mr G Z Jaine ~ uJiector Population Council
5 Dr Norma Andrews Medical Officer Population Council
6 Mr Jc~n Coury~ Evaluation Adviser Population Council
7 Mr A Jriseph Principal Statistical Officer Population Council
8 Dr C 0 Colman Country Representative Pan American Health )rg ni~ation
9 Mr ranca Kippel Health Education Specialist Ministry of Iea th
10 (1 bullbullines Principal Nursing Officer Ministry of Health
11 Dr Mx won (formerlyHinistry of Health)
12 M3 late Carops Ex-Chairman of Population Council
--
4i 1_ middotIIlt F-ntCWclOotf_Y v OJ t tl
GOVIIlHMEIgt(I OF TINIOAD AND TOampAGQ - NNISTJY OF HIALftf AIJIE1 2NATIONAL FAMilY PLANNING PROGRAMME
F MIL Y PLANNING CUNIC CASE CARD - NEW CASES - NFPPl
li ~~___ 1 ________
~ ecll-U
-- --------------------- shy~) ~~middot~------------------~~~~~~---CIJ------ middot~ii--middot-middot----middot-middot---middot--------- shy
ltv Writt N_ 01(111________________
a ~4itiJtmiddotl_____ ilIIIltIoI~____~____~-__----- shybull ~4
fie l$ - JO tDql IIfIA- tr-JMimiddot _ iJ 1 Odoor o
14aorielaquol_ _~ 0 lio witIleo-La ~ 01 bull - OJ ( _01 1~ltgt1lh o bull- 0$
AacJcu 0 2 CIIriIWA 0 J Os 0
Yv~MONTH ltnollOf~nfIGHTI
Undu 1100U$ Utgtdn 5SCI Undu 11200 01 ~ 50 - 9949 amp100 - 1199 02UlOO - nn9E~ (
0)~ 10- $99 SiOO -- U9~ lOO -- U99 12400 - 1359)-------_-r----shy ~l)o SIS n600 - Hm1300 -- 019 OJ200 il~9 ~------ 99~ a 1)0 m Os1)00 -- l99 1400 -shy $4100 -- 1S999r--- shy
1500 donl S6000aad O399 - lt499I~- I 0lt
ltII
IJ -IC _~tltlioltgti lS
02 IaampJIIocI OJ 04 laM Os
w Oltwio I_-l(~u IrIaa U
h~~ ~Clubl 01 OJ
IS ~C-n 01 toSIitDI 02
Ji poundI on 01 IriIIIuy M ur 02 IV OJ
WU 10 pltIoII~ llaMtl 411 cIIiId 01 Ol it fIolto ~ do~ _14 rou IIlgtJo 1Ia1 ___~_ shy
40
It _ I 00 ~bull FPIiIJ 1
OJ 02 OJ 06
)0 III- iy wOWcf ~1
aMIIl Os
11 T 1gtlt ( h _______ 4)~
06
04 (MIbullbull middot bIrlI ~___~__~_ (-fIJI ~- -~-- (1HJ 49middot SJ
U 10k 01( 1__ raquo$-4
iU1) DOl F ToWotfOlnC DOl 001 or Do [IP 006 001 OIIgtu___Spltclty DOll Nltmo 010
U1Mo I orcpmiddot laquo55middot16
1lD 001 Foam Toblelf_ICim DOl Condom DOl CoomS~ 004 oe Oos WlttuJn 1J OIkr DSpody) 101~ ~Iu 006 Rhylhm 001 DOG OJO
no wI~lmm 4 cd
(I 0) 1110 01 Condor 03 (lorn bull l S~muoidIl 04 Faa TabioolfIIltr- Os RhyUlm 01 lnJrl tible O Advico 090 06
la slt 1)0 19 loti ~rltnlt) ([)sl or 1llOn) ____ --__ bullbully-J n SV - ~JcdS
v~ Cl NCI 0 30 OJI_O I Wr blJ1h 0 I ~ OJ 1 ~ (fOOd V 01 No 02 laquo 6) Cf4
WIiI 1 172
004 001
j D middotmiddot middot
1 ~
r
~
bull I
bullI I I
r c i
ANNEX 3 Pagemiddot 1 of 5
0 raquo rshy -lt l)J ~ 111 t G) 5 shy (J) ~ -
fT1u
i
MINISTTY OF Ho1TH
NTIONl F~ILY LNNING PR-GRbullbullM-tE
~~5tructions to C11nic ClerKa
How to co~ploto the Daily Rogister
~~ ~~v1sd Daily Rosi8ter replnc~D tho one which is now in use tb$ Monthly PC~ri rOt~ arti tho 01( Ci() Dod PollJ j f m It is a pre-coded form and 1411 cl~1p Jd tl a1I6iniul-mIHvn Oel Clinic nctivi~y
110 )rm rollt biJ coupJot)d lrl cupLtcoto using a o(roon shoot Tho top aheot or oriinai ~ust bl) 6(Ult to tho CQgt1tral O[[lCO and tho carbon copy retained in the Gliaic rilo dll the for6a that ar uD~d betwoen the 1st 4nd the 15th of the oIIollth aut bo subClittud tocho office 35 Lnc blttch Those oomp1cted betwoon tho 16th _lid tqemc of tho month must bo ~cnt in a secJnll batch
P lOvLior hns boon Illllde for 25 clients on cZlch forlll new forlll must b IIlied f r poundh 50[810n2 whothur or not ono or lIIore session are hoIdiit the clinic on he sarne day
I th ro alO more htl 25 clionta 1n attondnnco at tho session the additi shyOhAl m~bOl of clionts 10 clients nu~ber 26 27 etc sh0u1l be ontered on the next Imiddotrlll ~i ttout a1tpoundring the numbtlrs in the cvlumn hond Series
51 ppOfil th~ number of aUcnts lQr that session ws 5 this would mean thllt two rJlS ~ lst be 6ubllIitt~dl the first filled uF 1 tltgt 25 And the laquoIncond 1 to 10 Th~ cal bon ofies should bo st~plod togother at thu t0P l~rt h4nd corner of the torm ard ktpt in the Clinic filo lou IIlU6t stapl~ the originftls in the 8~~ monnshyer for lIub~ssion to the ofticl
ie h~ ll idontiflctior- (cc 1 - )
0 lot Ji 9 anythin~ hGro poundhia is int(mdClc for tha computer code
2 ~~pound~ - Print clOflrly tho name of your Clinic
C1Lic Huml or - (cc 4 - 8) Evar1 Clinic Numbor has 5 digits Virite each dig t il a t$purate box
It Pai~_thllsectgdllion (00 lt) -1 1) - Dl monll 10M
lw) bolte IlrO proY140d fetr olAoh pr 01 thQ dISh Enter tho dA) ldns a R
d16ih
emiddot5middot (0 11 I for 115t ( 0 21 for 5th etc Treat month the am pay
e ~ 10 ~ I for I-hrch 0 [2] for September Tho y~nr must be (into ad
I Z I ~ I I 71 q etc
Take as in IixulIple tho dOlte 3rd tllrch 1973 7~ie must bo written
[0131 LSLDI[7l3JDny Month Ye~r
5middot 1~J $~~ - Irom ~-------- To --------shytntol hOI II the time the Clinic 111118 in SW5sion emiddot8middot
(i) 11011 500 lm To 1200 non
(11) Frclt 100 pm To 400 pm
(iii ) IX-OG OO pllI To 6~00 pm
f
2
ADEJ ) Paae ) of S
6 Eov
_ 1hA 1gtIpoundC iIIUlt be nu~o7Ifd tler1ally 1 throurh n lU tbey Are Wled In ~1l8ellJ IInel 1301 tlU 1 Orcl 1 Wled tor a o5038ioll - -I 2 tonY tho _boul~ b I1WJbtl 1 and 2
hlrlll are 25 linos OIl the fOnl Ilnd thoae muet be UBtleS for 25 clients 9 one ior bullbull 01 I ini
ot ~h lc II ol1cM lOlivpound til e linic before soeinc DurOI or doc tor ilnc ii hox rristrltltion nUlJbet had alrearll been recorded on the Dai 1y Roiuter then n line ~hollld be drawn through that entry an1 the eliort nust not 06 includttd in tho totals tor that 0eDion
1lw Ileifitration Num)~r of cueh client must be IiIritten IS n 5-dlrlt oode ClhnC IH11IlElr 315 1IIU8 tborotore be enterod 18J010117]5]
~ Clt ZOt
Coda 1 Codo
10 ~tl c 2t j co 21)
~w elSe - Coda 1 0) d CltaEl - Code 2 Revislt Code 3
Only pound1 01 theBe coiles may be usod
11 prol-O~ ~Eil~1 (cc 22)
If ma climt was L drop-out IIho haoS returned now to the Clinio tor tho first no linmiddot bullwin lt1ro1eo o t he or she should be given CCe 1 It this do 5 II It nprlly leu this colWlln blank
u Hothod middothisllill loe 23)
NOh til t otly ~ Cod 16 tp he ontered in 2lpound of the columna oven thOUGh 10 co11lllJlB 10 provided on the torm The Codes llrol-
Oral Contraceptive Code 0 1 U D Code 1 Condom plUD Codo Z Condor (only) Code 3 Foum tAblets cream Code it DitphrClGJII Code 5 Rhythm Cde 6 Injectible Code 7 Advice Code 8 Other Code 9
It for middotDo-le 1 client rlllll ji yen cclldorls ord foam or creall Iou Qust entor Coole i (condom plulJ) in the appropri~te column This Quat be the only lIotmiddot) tarcie If an in the cnse of a tlnle clinic I the client is Bup)lieu lith COIlOrW only you rmot entEr CorlQ 3 (cpndolll) Do not use a ticII ~ tho (odo Nwber
It is CUi tomary fur 11 cliont 110 is beine put on the oral contraceptive for the first tiT1o and even on other occasionn be issued condoms and 11 crelle or foam a Ilell rI3 a pgtcket of pilla In such Cllses when the piDQ Ilre Ilctually iouou you tlust record Orll (Co~e 0) 08 tho onll metbod ilo othor ntry sll0uld ho nnrlo
Uovever n SJC~ canas vucru condoms and fOHa ~rc eiven but no pilJa (even thoJRh _t _n the intention to issue pills nt the noxt vioit) than the Mothol Th5 ifli t ohoulcl be recorded uo Condor Plus (Code 2)
13 Seen Bybullbullbullbullbull
~rot S-1 SO l
Doctor (Dr) - Code 1 j Nurse (Nul ) - Code 2
Clark (Olk-) - Code If tho Clhnt is vcen hy both tho llootor tlnd the Nurse enter Code 1 t Doctor It 6~61l by the Nurso only arite Code 2 Cod bullbull Cerk is l)llnt for FA Cllnica Clerks in tho Government Cli1t hiwo Llttoll istructed not to i56uo supplios on their own volition
14 fl221~
lhio S~tiCl of -Ie fvrtl t~ke 16 (llrci coluMna (cc 25-+0) nnd 10 tho only part at th iOIQ in llich iore thAn one cod is Zlccoptl1blo Tho purpoco of the )ecton is to 0 able to arrive nt the Cjunntity of 6tock dilltlitJutshyed YOI IIlUdt writo in the CllllOjH-iata colulna the nUllbJr of Il1ch 4rtic1o i~JSu~d ~lo e ha I Oral Contrcilpti vea are aub-di vi dod into types ae_ 3 PIllCKC 9 0 Elynnn LlUot be entered Codo in card column 25
If tor eXllrplc t l cliunt is iosued wi th packots of Zucynon nnd aJ(1 ~ivn 1 conuotll (8inoloo) you ouot enter in oard column 25 and 11 It
cnrd col~8 )2 and J (io 1 in card colucn 2 nnd 2 1n card coluun 33) Nota C)lldoIlU ale to b(t ruoordod individually not os packots of throo) Should n ne LlondoClo be isoued thil3 is to be rc-Qed as 09
If It clint 6 t~ot isoued Blly lIupplies thon you must writo Codo 1 in CQllAlilD 41
It Q eli nt isite the clinic to check on her LUD or her Diaphra~t IUId ro DI W 6 ppl ills nre ispounducd then Code 1 1s wri t ten in column 40
In the FA clinios here a variety ot orll contraceptiveo in orer~l tho elerll wilmiddot~ bJ provided with a specill code shoot The idontifyin coo will b wiittn in Column 29 nnd the nUlber of packets iosued in colwm )0
lralaer-In Code 1 lrllllsie r~ut Coda 2 leIllPQrArr Trnnsfer-In Codo gt
In the cao of n 2ratl8fcr-In I you lUot n160 cOrlpleto coluons 42-51
In the cllU J of A ~~emporary TranGfor-1n (an individual who i8 only v1citing fur clinic tor some epecial trcatcont hna who will bo rdnlnin
~middot(II~~~fO~l~SIl~I3~nn~~~h~rO~nh~1~~190~~nll 2-46 and ler rei IItrntion numbu in colullnll41-51
It the oli( nt i iNt a CrllnoforwIu - Out or loClporu1 tMn loave oolumn 1 blank
16 lr4nst(gtr-tl2~~morrry TilJnder-In (co 42-51) Forl1ltl CUn E1~ (cc 112-46)
hen you rei iatlr L irllsfcrln or Il TJlporary Trnnsfer-In you IIIUBt write I ere the five-digit clinio nucbor of the Clinic iraQ which tho ltlient Me (uIlO
2mer ]letr ~2n ~ (cc 47-51)
frlta fllao Clo r-~itrlltion Nuc~Er ot the client in the Former Clinic (i c bullbull th 1 Sis rnmiddotion ~UlIlh()r which the client carrics 1n the tormor clinio) bull
It tho Forrltl Ho( ist rntion Number iIJ not readily wnilnble you tluct oocpluto thtl epcciol [orlll Transfer-In Not Identifiod Dy Forrlcr RCGi(trn~ t10n Nwlbvr Or ~ flt)rCl is to be cOlplctcd for och cnso nnd th forlJO Ilubmi tted to thu )opllntion Prorrnnme Of fice tOGether with tho Dily Ro~iBtors lhwev~r should the clork leuTI of tho clint B FormlI Uocintra tion lUlllb r )0[(10 Cubmi ttinft the D1ily IOCI otro t hen the nUQbcr shoulo bo -ri ton in colucns 47-51 lna the special foro should lJo deotroyotl
l7 bullbullbullbullbull
r lt bull bull
ADXI ) Pap S ot S
11 UD LV~ (cc 525)
It tb( cliont io ~ivQn An IUD tor the firot tl~o then you should Sri to Codo 1 Inuort ill colurJI 52
It tho olimiddotsnt ia rvinGgtrtltld i th An I UD bullbull tben wse Coda 2 RelnDltlrt shyin (01Uil11 52
It the clLmt is ~tte~~dint chnic beruse her IUD CflClQ out by Haol (cxpll Iion i ~hcn fir te todo ~- UIlllrli1 53~
If c-ltr IU fj IIIS reov in -ne cllnic by tho doctor or nurso t~on vlritI Codec in column 5
II the eli nt otends eiLlie tld explin[l th(lt she rccovcd the IUD tlllleel nen write Coda H in Colwlm 53
It the IUD jr still within the uterus nd the WOIraquoI1 1 11rc6llJlnt thon lIrite 1gt40 4 in Column 53
lZ np h5t (ce 54) It 0 Pull 5mor ie t~ken durin thi visit tben Codo 1 ehould be ampDtere4 in ColWlln 54 Should he c110nt lltt rQ(uircd to rttturn to clin1c for a rogtol1t Pnl) t06t then CoLe 2 llhould bo middotwrittcn in column 54
It no Pllp Scou io taken tde visit Itove colUQn 54 blank
Iraferti1lli (CQ 55)
Ii the e liett io nl1 infortili tr eaoe use Cor1o Ill in colUQn 55
If tbia 1000 not tlpl lonve column 55 blonk
20 Totaltll
CO~1ploete the [)ldegO 1gty puti YI tne totals betweon the double lines nt tu b()ttctl Carrj colUlllnc 20 21 nd gt4 Must hlve tho Bnoe JllIIber and thiG Would coreslonc to the numocr ir attencbnco
Writ$ th to1ul nUlllior of Drop-Outs returned (c022)
Urito 41eo tb totnls fOJ each card column 0 to 9 under tho h(adinu Method thiB Vioit Show tho tote L fgtr OlCl type of contraceptive issued (cc 25-40)
1)0 Dot wrLte 1111 totll lUl(Ier Card Columns 15-19 29 41-51
21 COPmllh bull ~lt h~t~ Monthly ROilort
OQ thG DaLl oCator forlll thnt ccrrOspOldB to tho 1(8t 1$06610n lt 0
oth yo Olllt (vwlgtleto the items nt the botto of the [orampl This is tour ontll~1 n(olt nnd includcD tho totll lumber of sesions Ilntl tho total Iluolcr ( r crop-outs durinr the Qonth
An tiUlsilt n drir which n doctor liB in nttcndnncc is a doctor sOfll~1on and shoulc 00 re(liGtcnd in coltns 56-57 All other sessions 1116 conlliid~recl supply stllciona and thtlY 1110 rocordod in columns 58-59
the total Ilum)nl Jf drop-outo ld the drop-outs by method durinc the onth nre 10 bu oltorou in the inrlicllted boxes
72 Chad Your ~
Milke I ura th t all thE fijul4gtu rre c101r -tNever writo our nutlUQrS 50 InrjEl that they oxtend out of tho
ap~rotr1ato ~ox
Cheek to BoJa tht 1111 numuors 1110 in tho correct boxes -- CJslHloially when Writi1 the totlB
Mllxe Cirtc O thmiddott t1e infoT1I1ntion i6 clear on the corbon COllY before sep rmiddotinr the sheets
Jitn the Fomiddotl lien tly sien YOUl nr me 1t the bot tOil right hnnd corner btl forc subol ttinG it Keep tle CL rb n copy for your rocordn
i
-l ________~~---------~
I _1
Adminiatr-atlve SKVieu
P inba ~~~l1cal lrlnbin~~eltltcal -1 te~ra t~~rvicc (lnatittloaa)
--1- - shy -1------------_-L_ l-r-aJiil- shy _-L_tet1lal d
PlIinm1tJ8 atdUon DetalMid H8Il1tb ~ ________bull Care
-----~ Office of i
the FlIily _IPlill3 roarshy
1- - - -------RegiatUll urnr
ltIi 1 Drelttor Rcgicaat Director Souta Tabqo tacallortb ~ counu gt____ ~ (4 ouottet)
Off1ce of the Res10nal Diractoc L
r----- _L_ -- shy i I bull IREgional Ipitl I
District IIttaltb I bull Othn RelOl ond Hcpital CenteIntt itlt j In 1__ _shy-~- ---- -_j
J r Ii~lth
C~nlef
L
I Ihnlth lie I th Offlcu (1ft lc~
Coullty 1I0p1ta1
Henlth tentet
I

--
4i 1_ middotIIlt F-ntCWclOotf_Y v OJ t tl
GOVIIlHMEIgt(I OF TINIOAD AND TOampAGQ - NNISTJY OF HIALftf AIJIE1 2NATIONAL FAMilY PLANNING PROGRAMME
F MIL Y PLANNING CUNIC CASE CARD - NEW CASES - NFPPl
li ~~___ 1 ________
~ ecll-U
-- --------------------- shy~) ~~middot~------------------~~~~~~---CIJ------ middot~ii--middot-middot----middot-middot---middot--------- shy
ltv Writt N_ 01(111________________
a ~4itiJtmiddotl_____ ilIIIltIoI~____~____~-__----- shybull ~4
fie l$ - JO tDql IIfIA- tr-JMimiddot _ iJ 1 Odoor o
14aorielaquol_ _~ 0 lio witIleo-La ~ 01 bull - OJ ( _01 1~ltgt1lh o bull- 0$
AacJcu 0 2 CIIriIWA 0 J Os 0
Yv~MONTH ltnollOf~nfIGHTI
Undu 1100U$ Utgtdn 5SCI Undu 11200 01 ~ 50 - 9949 amp100 - 1199 02UlOO - nn9E~ (
0)~ 10- $99 SiOO -- U9~ lOO -- U99 12400 - 1359)-------_-r----shy ~l)o SIS n600 - Hm1300 -- 019 OJ200 il~9 ~------ 99~ a 1)0 m Os1)00 -- l99 1400 -shy $4100 -- 1S999r--- shy
1500 donl S6000aad O399 - lt499I~- I 0lt
ltII
IJ -IC _~tltlioltgti lS
02 IaampJIIocI OJ 04 laM Os
w Oltwio I_-l(~u IrIaa U
h~~ ~Clubl 01 OJ
IS ~C-n 01 toSIitDI 02
Ji poundI on 01 IriIIIuy M ur 02 IV OJ
WU 10 pltIoII~ llaMtl 411 cIIiId 01 Ol it fIolto ~ do~ _14 rou IIlgtJo 1Ia1 ___~_ shy
40
It _ I 00 ~bull FPIiIJ 1
OJ 02 OJ 06
)0 III- iy wOWcf ~1
aMIIl Os
11 T 1gtlt ( h _______ 4)~
06
04 (MIbullbull middot bIrlI ~___~__~_ (-fIJI ~- -~-- (1HJ 49middot SJ
U 10k 01( 1__ raquo$-4
iU1) DOl F ToWotfOlnC DOl 001 or Do [IP 006 001 OIIgtu___Spltclty DOll Nltmo 010
U1Mo I orcpmiddot laquo55middot16
1lD 001 Foam Toblelf_ICim DOl Condom DOl CoomS~ 004 oe Oos WlttuJn 1J OIkr DSpody) 101~ ~Iu 006 Rhylhm 001 DOG OJO
no wI~lmm 4 cd
(I 0) 1110 01 Condor 03 (lorn bull l S~muoidIl 04 Faa TabioolfIIltr- Os RhyUlm 01 lnJrl tible O Advico 090 06
la slt 1)0 19 loti ~rltnlt) ([)sl or 1llOn) ____ --__ bullbully-J n SV - ~JcdS
v~ Cl NCI 0 30 OJI_O I Wr blJ1h 0 I ~ OJ 1 ~ (fOOd V 01 No 02 laquo 6) Cf4
WIiI 1 172
004 001
j D middotmiddot middot
1 ~
r
~
bull I
bullI I I
r c i
ANNEX 3 Pagemiddot 1 of 5
0 raquo rshy -lt l)J ~ 111 t G) 5 shy (J) ~ -
fT1u
i
MINISTTY OF Ho1TH
NTIONl F~ILY LNNING PR-GRbullbullM-tE
~~5tructions to C11nic ClerKa
How to co~ploto the Daily Rogister
~~ ~~v1sd Daily Rosi8ter replnc~D tho one which is now in use tb$ Monthly PC~ri rOt~ arti tho 01( Ci() Dod PollJ j f m It is a pre-coded form and 1411 cl~1p Jd tl a1I6iniul-mIHvn Oel Clinic nctivi~y
110 )rm rollt biJ coupJot)d lrl cupLtcoto using a o(roon shoot Tho top aheot or oriinai ~ust bl) 6(Ult to tho CQgt1tral O[[lCO and tho carbon copy retained in the Gliaic rilo dll the for6a that ar uD~d betwoen the 1st 4nd the 15th of the oIIollth aut bo subClittud tocho office 35 Lnc blttch Those oomp1cted betwoon tho 16th _lid tqemc of tho month must bo ~cnt in a secJnll batch
P lOvLior hns boon Illllde for 25 clients on cZlch forlll new forlll must b IIlied f r poundh 50[810n2 whothur or not ono or lIIore session are hoIdiit the clinic on he sarne day
I th ro alO more htl 25 clionta 1n attondnnco at tho session the additi shyOhAl m~bOl of clionts 10 clients nu~ber 26 27 etc sh0u1l be ontered on the next Imiddotrlll ~i ttout a1tpoundring the numbtlrs in the cvlumn hond Series
51 ppOfil th~ number of aUcnts lQr that session ws 5 this would mean thllt two rJlS ~ lst be 6ubllIitt~dl the first filled uF 1 tltgt 25 And the laquoIncond 1 to 10 Th~ cal bon ofies should bo st~plod togother at thu t0P l~rt h4nd corner of the torm ard ktpt in the Clinic filo lou IIlU6t stapl~ the originftls in the 8~~ monnshyer for lIub~ssion to the ofticl
ie h~ ll idontiflctior- (cc 1 - )
0 lot Ji 9 anythin~ hGro poundhia is int(mdClc for tha computer code
2 ~~pound~ - Print clOflrly tho name of your Clinic
C1Lic Huml or - (cc 4 - 8) Evar1 Clinic Numbor has 5 digits Virite each dig t il a t$purate box
It Pai~_thllsectgdllion (00 lt) -1 1) - Dl monll 10M
lw) bolte IlrO proY140d fetr olAoh pr 01 thQ dISh Enter tho dA) ldns a R
d16ih
emiddot5middot (0 11 I for 115t ( 0 21 for 5th etc Treat month the am pay
e ~ 10 ~ I for I-hrch 0 [2] for September Tho y~nr must be (into ad
I Z I ~ I I 71 q etc
Take as in IixulIple tho dOlte 3rd tllrch 1973 7~ie must bo written
[0131 LSLDI[7l3JDny Month Ye~r
5middot 1~J $~~ - Irom ~-------- To --------shytntol hOI II the time the Clinic 111118 in SW5sion emiddot8middot
(i) 11011 500 lm To 1200 non
(11) Frclt 100 pm To 400 pm
(iii ) IX-OG OO pllI To 6~00 pm
f
2
ADEJ ) Paae ) of S
6 Eov
_ 1hA 1gtIpoundC iIIUlt be nu~o7Ifd tler1ally 1 throurh n lU tbey Are Wled In ~1l8ellJ IInel 1301 tlU 1 Orcl 1 Wled tor a o5038ioll - -I 2 tonY tho _boul~ b I1WJbtl 1 and 2
hlrlll are 25 linos OIl the fOnl Ilnd thoae muet be UBtleS for 25 clients 9 one ior bullbull 01 I ini
ot ~h lc II ol1cM lOlivpound til e linic before soeinc DurOI or doc tor ilnc ii hox rristrltltion nUlJbet had alrearll been recorded on the Dai 1y Roiuter then n line ~hollld be drawn through that entry an1 the eliort nust not 06 includttd in tho totals tor that 0eDion
1lw Ileifitration Num)~r of cueh client must be IiIritten IS n 5-dlrlt oode ClhnC IH11IlElr 315 1IIU8 tborotore be enterod 18J010117]5]
~ Clt ZOt
Coda 1 Codo
10 ~tl c 2t j co 21)
~w elSe - Coda 1 0) d CltaEl - Code 2 Revislt Code 3
Only pound1 01 theBe coiles may be usod
11 prol-O~ ~Eil~1 (cc 22)
If ma climt was L drop-out IIho haoS returned now to the Clinio tor tho first no linmiddot bullwin lt1ro1eo o t he or she should be given CCe 1 It this do 5 II It nprlly leu this colWlln blank
u Hothod middothisllill loe 23)
NOh til t otly ~ Cod 16 tp he ontered in 2lpound of the columna oven thOUGh 10 co11lllJlB 10 provided on the torm The Codes llrol-
Oral Contraceptive Code 0 1 U D Code 1 Condom plUD Codo Z Condor (only) Code 3 Foum tAblets cream Code it DitphrClGJII Code 5 Rhythm Cde 6 Injectible Code 7 Advice Code 8 Other Code 9
It for middotDo-le 1 client rlllll ji yen cclldorls ord foam or creall Iou Qust entor Coole i (condom plulJ) in the appropri~te column This Quat be the only lIotmiddot) tarcie If an in the cnse of a tlnle clinic I the client is Bup)lieu lith COIlOrW only you rmot entEr CorlQ 3 (cpndolll) Do not use a ticII ~ tho (odo Nwber
It is CUi tomary fur 11 cliont 110 is beine put on the oral contraceptive for the first tiT1o and even on other occasionn be issued condoms and 11 crelle or foam a Ilell rI3 a pgtcket of pilla In such Cllses when the piDQ Ilre Ilctually iouou you tlust record Orll (Co~e 0) 08 tho onll metbod ilo othor ntry sll0uld ho nnrlo
Uovever n SJC~ canas vucru condoms and fOHa ~rc eiven but no pilJa (even thoJRh _t _n the intention to issue pills nt the noxt vioit) than the Mothol Th5 ifli t ohoulcl be recorded uo Condor Plus (Code 2)
13 Seen Bybullbullbullbullbull
~rot S-1 SO l
Doctor (Dr) - Code 1 j Nurse (Nul ) - Code 2
Clark (Olk-) - Code If tho Clhnt is vcen hy both tho llootor tlnd the Nurse enter Code 1 t Doctor It 6~61l by the Nurso only arite Code 2 Cod bullbull Cerk is l)llnt for FA Cllnica Clerks in tho Government Cli1t hiwo Llttoll istructed not to i56uo supplios on their own volition
14 fl221~
lhio S~tiCl of -Ie fvrtl t~ke 16 (llrci coluMna (cc 25-+0) nnd 10 tho only part at th iOIQ in llich iore thAn one cod is Zlccoptl1blo Tho purpoco of the )ecton is to 0 able to arrive nt the Cjunntity of 6tock dilltlitJutshyed YOI IIlUdt writo in the CllllOjH-iata colulna the nUllbJr of Il1ch 4rtic1o i~JSu~d ~lo e ha I Oral Contrcilpti vea are aub-di vi dod into types ae_ 3 PIllCKC 9 0 Elynnn LlUot be entered Codo in card column 25
If tor eXllrplc t l cliunt is iosued wi th packots of Zucynon nnd aJ(1 ~ivn 1 conuotll (8inoloo) you ouot enter in oard column 25 and 11 It
cnrd col~8 )2 and J (io 1 in card colucn 2 nnd 2 1n card coluun 33) Nota C)lldoIlU ale to b(t ruoordod individually not os packots of throo) Should n ne LlondoClo be isoued thil3 is to be rc-Qed as 09
If It clint 6 t~ot isoued Blly lIupplies thon you must writo Codo 1 in CQllAlilD 41
It Q eli nt isite the clinic to check on her LUD or her Diaphra~t IUId ro DI W 6 ppl ills nre ispounducd then Code 1 1s wri t ten in column 40
In the FA clinios here a variety ot orll contraceptiveo in orer~l tho elerll wilmiddot~ bJ provided with a specill code shoot The idontifyin coo will b wiittn in Column 29 nnd the nUlber of packets iosued in colwm )0
lralaer-In Code 1 lrllllsie r~ut Coda 2 leIllPQrArr Trnnsfer-In Codo gt
In the cao of n 2ratl8fcr-In I you lUot n160 cOrlpleto coluons 42-51
In the cllU J of A ~~emporary TranGfor-1n (an individual who i8 only v1citing fur clinic tor some epecial trcatcont hna who will bo rdnlnin
~middot(II~~~fO~l~SIl~I3~nn~~~h~rO~nh~1~~190~~nll 2-46 and ler rei IItrntion numbu in colullnll41-51
It the oli( nt i iNt a CrllnoforwIu - Out or loClporu1 tMn loave oolumn 1 blank
16 lr4nst(gtr-tl2~~morrry TilJnder-In (co 42-51) Forl1ltl CUn E1~ (cc 112-46)
hen you rei iatlr L irllsfcrln or Il TJlporary Trnnsfer-In you IIIUBt write I ere the five-digit clinio nucbor of the Clinic iraQ which tho ltlient Me (uIlO
2mer ]letr ~2n ~ (cc 47-51)
frlta fllao Clo r-~itrlltion Nuc~Er ot the client in the Former Clinic (i c bullbull th 1 Sis rnmiddotion ~UlIlh()r which the client carrics 1n the tormor clinio) bull
It tho Forrltl Ho( ist rntion Number iIJ not readily wnilnble you tluct oocpluto thtl epcciol [orlll Transfer-In Not Identifiod Dy Forrlcr RCGi(trn~ t10n Nwlbvr Or ~ flt)rCl is to be cOlplctcd for och cnso nnd th forlJO Ilubmi tted to thu )opllntion Prorrnnme Of fice tOGether with tho Dily Ro~iBtors lhwev~r should the clork leuTI of tho clint B FormlI Uocintra tion lUlllb r )0[(10 Cubmi ttinft the D1ily IOCI otro t hen the nUQbcr shoulo bo -ri ton in colucns 47-51 lna the special foro should lJo deotroyotl
l7 bullbullbullbullbull
r lt bull bull
ADXI ) Pap S ot S
11 UD LV~ (cc 525)
It tb( cliont io ~ivQn An IUD tor the firot tl~o then you should Sri to Codo 1 Inuort ill colurJI 52
It tho olimiddotsnt ia rvinGgtrtltld i th An I UD bullbull tben wse Coda 2 RelnDltlrt shyin (01Uil11 52
It the clLmt is ~tte~~dint chnic beruse her IUD CflClQ out by Haol (cxpll Iion i ~hcn fir te todo ~- UIlllrli1 53~
If c-ltr IU fj IIIS reov in -ne cllnic by tho doctor or nurso t~on vlritI Codec in column 5
II the eli nt otends eiLlie tld explin[l th(lt she rccovcd the IUD tlllleel nen write Coda H in Colwlm 53
It the IUD jr still within the uterus nd the WOIraquoI1 1 11rc6llJlnt thon lIrite 1gt40 4 in Column 53
lZ np h5t (ce 54) It 0 Pull 5mor ie t~ken durin thi visit tben Codo 1 ehould be ampDtere4 in ColWlln 54 Should he c110nt lltt rQ(uircd to rttturn to clin1c for a rogtol1t Pnl) t06t then CoLe 2 llhould bo middotwrittcn in column 54
It no Pllp Scou io taken tde visit Itove colUQn 54 blank
Iraferti1lli (CQ 55)
Ii the e liett io nl1 infortili tr eaoe use Cor1o Ill in colUQn 55
If tbia 1000 not tlpl lonve column 55 blonk
20 Totaltll
CO~1ploete the [)ldegO 1gty puti YI tne totals betweon the double lines nt tu b()ttctl Carrj colUlllnc 20 21 nd gt4 Must hlve tho Bnoe JllIIber and thiG Would coreslonc to the numocr ir attencbnco
Writ$ th to1ul nUlllior of Drop-Outs returned (c022)
Urito 41eo tb totnls fOJ each card column 0 to 9 under tho h(adinu Method thiB Vioit Show tho tote L fgtr OlCl type of contraceptive issued (cc 25-40)
1)0 Dot wrLte 1111 totll lUl(Ier Card Columns 15-19 29 41-51
21 COPmllh bull ~lt h~t~ Monthly ROilort
OQ thG DaLl oCator forlll thnt ccrrOspOldB to tho 1(8t 1$06610n lt 0
oth yo Olllt (vwlgtleto the items nt the botto of the [orampl This is tour ontll~1 n(olt nnd includcD tho totll lumber of sesions Ilntl tho total Iluolcr ( r crop-outs durinr the Qonth
An tiUlsilt n drir which n doctor liB in nttcndnncc is a doctor sOfll~1on and shoulc 00 re(liGtcnd in coltns 56-57 All other sessions 1116 conlliid~recl supply stllciona and thtlY 1110 rocordod in columns 58-59
the total Ilum)nl Jf drop-outo ld the drop-outs by method durinc the onth nre 10 bu oltorou in the inrlicllted boxes
72 Chad Your ~
Milke I ura th t all thE fijul4gtu rre c101r -tNever writo our nutlUQrS 50 InrjEl that they oxtend out of tho
ap~rotr1ato ~ox
Cheek to BoJa tht 1111 numuors 1110 in tho correct boxes -- CJslHloially when Writi1 the totlB
Mllxe Cirtc O thmiddott t1e infoT1I1ntion i6 clear on the corbon COllY before sep rmiddotinr the sheets
Jitn the Fomiddotl lien tly sien YOUl nr me 1t the bot tOil right hnnd corner btl forc subol ttinG it Keep tle CL rb n copy for your rocordn
i
-l ________~~---------~
I _1
Adminiatr-atlve SKVieu
P inba ~~~l1cal lrlnbin~~eltltcal -1 te~ra t~~rvicc (lnatittloaa)
--1- - shy -1------------_-L_ l-r-aJiil- shy _-L_tet1lal d
PlIinm1tJ8 atdUon DetalMid H8Il1tb ~ ________bull Care
-----~ Office of i
the FlIily _IPlill3 roarshy
1- - - -------RegiatUll urnr
ltIi 1 Drelttor Rcgicaat Director Souta Tabqo tacallortb ~ counu gt____ ~ (4 ouottet)
Off1ce of the Res10nal Diractoc L
r----- _L_ -- shy i I bull IREgional Ipitl I
District IIttaltb I bull Othn RelOl ond Hcpital CenteIntt itlt j In 1__ _shy-~- ---- -_j
J r Ii~lth
C~nlef
L
I Ihnlth lie I th Offlcu (1ft lc~
Coullty 1I0p1ta1
Henlth tentet
I

j D middotmiddot middot
1 ~
r
~
bull I
bullI I I
r c i
ANNEX 3 Pagemiddot 1 of 5
0 raquo rshy -lt l)J ~ 111 t G) 5 shy (J) ~ -
fT1u
i
MINISTTY OF Ho1TH
NTIONl F~ILY LNNING PR-GRbullbullM-tE
~~5tructions to C11nic ClerKa
How to co~ploto the Daily Rogister
~~ ~~v1sd Daily Rosi8ter replnc~D tho one which is now in use tb$ Monthly PC~ri rOt~ arti tho 01( Ci() Dod PollJ j f m It is a pre-coded form and 1411 cl~1p Jd tl a1I6iniul-mIHvn Oel Clinic nctivi~y
110 )rm rollt biJ coupJot)d lrl cupLtcoto using a o(roon shoot Tho top aheot or oriinai ~ust bl) 6(Ult to tho CQgt1tral O[[lCO and tho carbon copy retained in the Gliaic rilo dll the for6a that ar uD~d betwoen the 1st 4nd the 15th of the oIIollth aut bo subClittud tocho office 35 Lnc blttch Those oomp1cted betwoon tho 16th _lid tqemc of tho month must bo ~cnt in a secJnll batch
P lOvLior hns boon Illllde for 25 clients on cZlch forlll new forlll must b IIlied f r poundh 50[810n2 whothur or not ono or lIIore session are hoIdiit the clinic on he sarne day
I th ro alO more htl 25 clionta 1n attondnnco at tho session the additi shyOhAl m~bOl of clionts 10 clients nu~ber 26 27 etc sh0u1l be ontered on the next Imiddotrlll ~i ttout a1tpoundring the numbtlrs in the cvlumn hond Series
51 ppOfil th~ number of aUcnts lQr that session ws 5 this would mean thllt two rJlS ~ lst be 6ubllIitt~dl the first filled uF 1 tltgt 25 And the laquoIncond 1 to 10 Th~ cal bon ofies should bo st~plod togother at thu t0P l~rt h4nd corner of the torm ard ktpt in the Clinic filo lou IIlU6t stapl~ the originftls in the 8~~ monnshyer for lIub~ssion to the ofticl
ie h~ ll idontiflctior- (cc 1 - )
0 lot Ji 9 anythin~ hGro poundhia is int(mdClc for tha computer code
2 ~~pound~ - Print clOflrly tho name of your Clinic
C1Lic Huml or - (cc 4 - 8) Evar1 Clinic Numbor has 5 digits Virite each dig t il a t$purate box
It Pai~_thllsectgdllion (00 lt) -1 1) - Dl monll 10M
lw) bolte IlrO proY140d fetr olAoh pr 01 thQ dISh Enter tho dA) ldns a R
d16ih
emiddot5middot (0 11 I for 115t ( 0 21 for 5th etc Treat month the am pay
e ~ 10 ~ I for I-hrch 0 [2] for September Tho y~nr must be (into ad
I Z I ~ I I 71 q etc
Take as in IixulIple tho dOlte 3rd tllrch 1973 7~ie must bo written
[0131 LSLDI[7l3JDny Month Ye~r
5middot 1~J $~~ - Irom ~-------- To --------shytntol hOI II the time the Clinic 111118 in SW5sion emiddot8middot
(i) 11011 500 lm To 1200 non
(11) Frclt 100 pm To 400 pm
(iii ) IX-OG OO pllI To 6~00 pm
f
2
ADEJ ) Paae ) of S
6 Eov
_ 1hA 1gtIpoundC iIIUlt be nu~o7Ifd tler1ally 1 throurh n lU tbey Are Wled In ~1l8ellJ IInel 1301 tlU 1 Orcl 1 Wled tor a o5038ioll - -I 2 tonY tho _boul~ b I1WJbtl 1 and 2
hlrlll are 25 linos OIl the fOnl Ilnd thoae muet be UBtleS for 25 clients 9 one ior bullbull 01 I ini
ot ~h lc II ol1cM lOlivpound til e linic before soeinc DurOI or doc tor ilnc ii hox rristrltltion nUlJbet had alrearll been recorded on the Dai 1y Roiuter then n line ~hollld be drawn through that entry an1 the eliort nust not 06 includttd in tho totals tor that 0eDion
1lw Ileifitration Num)~r of cueh client must be IiIritten IS n 5-dlrlt oode ClhnC IH11IlElr 315 1IIU8 tborotore be enterod 18J010117]5]
~ Clt ZOt
Coda 1 Codo
10 ~tl c 2t j co 21)
~w elSe - Coda 1 0) d CltaEl - Code 2 Revislt Code 3
Only pound1 01 theBe coiles may be usod
11 prol-O~ ~Eil~1 (cc 22)
If ma climt was L drop-out IIho haoS returned now to the Clinio tor tho first no linmiddot bullwin lt1ro1eo o t he or she should be given CCe 1 It this do 5 II It nprlly leu this colWlln blank
u Hothod middothisllill loe 23)
NOh til t otly ~ Cod 16 tp he ontered in 2lpound of the columna oven thOUGh 10 co11lllJlB 10 provided on the torm The Codes llrol-
Oral Contraceptive Code 0 1 U D Code 1 Condom plUD Codo Z Condor (only) Code 3 Foum tAblets cream Code it DitphrClGJII Code 5 Rhythm Cde 6 Injectible Code 7 Advice Code 8 Other Code 9
It for middotDo-le 1 client rlllll ji yen cclldorls ord foam or creall Iou Qust entor Coole i (condom plulJ) in the appropri~te column This Quat be the only lIotmiddot) tarcie If an in the cnse of a tlnle clinic I the client is Bup)lieu lith COIlOrW only you rmot entEr CorlQ 3 (cpndolll) Do not use a ticII ~ tho (odo Nwber
It is CUi tomary fur 11 cliont 110 is beine put on the oral contraceptive for the first tiT1o and even on other occasionn be issued condoms and 11 crelle or foam a Ilell rI3 a pgtcket of pilla In such Cllses when the piDQ Ilre Ilctually iouou you tlust record Orll (Co~e 0) 08 tho onll metbod ilo othor ntry sll0uld ho nnrlo
Uovever n SJC~ canas vucru condoms and fOHa ~rc eiven but no pilJa (even thoJRh _t _n the intention to issue pills nt the noxt vioit) than the Mothol Th5 ifli t ohoulcl be recorded uo Condor Plus (Code 2)
13 Seen Bybullbullbullbullbull
~rot S-1 SO l
Doctor (Dr) - Code 1 j Nurse (Nul ) - Code 2
Clark (Olk-) - Code If tho Clhnt is vcen hy both tho llootor tlnd the Nurse enter Code 1 t Doctor It 6~61l by the Nurso only arite Code 2 Cod bullbull Cerk is l)llnt for FA Cllnica Clerks in tho Government Cli1t hiwo Llttoll istructed not to i56uo supplios on their own volition
14 fl221~
lhio S~tiCl of -Ie fvrtl t~ke 16 (llrci coluMna (cc 25-+0) nnd 10 tho only part at th iOIQ in llich iore thAn one cod is Zlccoptl1blo Tho purpoco of the )ecton is to 0 able to arrive nt the Cjunntity of 6tock dilltlitJutshyed YOI IIlUdt writo in the CllllOjH-iata colulna the nUllbJr of Il1ch 4rtic1o i~JSu~d ~lo e ha I Oral Contrcilpti vea are aub-di vi dod into types ae_ 3 PIllCKC 9 0 Elynnn LlUot be entered Codo in card column 25
If tor eXllrplc t l cliunt is iosued wi th packots of Zucynon nnd aJ(1 ~ivn 1 conuotll (8inoloo) you ouot enter in oard column 25 and 11 It
cnrd col~8 )2 and J (io 1 in card colucn 2 nnd 2 1n card coluun 33) Nota C)lldoIlU ale to b(t ruoordod individually not os packots of throo) Should n ne LlondoClo be isoued thil3 is to be rc-Qed as 09
If It clint 6 t~ot isoued Blly lIupplies thon you must writo Codo 1 in CQllAlilD 41
It Q eli nt isite the clinic to check on her LUD or her Diaphra~t IUId ro DI W 6 ppl ills nre ispounducd then Code 1 1s wri t ten in column 40
In the FA clinios here a variety ot orll contraceptiveo in orer~l tho elerll wilmiddot~ bJ provided with a specill code shoot The idontifyin coo will b wiittn in Column 29 nnd the nUlber of packets iosued in colwm )0
lralaer-In Code 1 lrllllsie r~ut Coda 2 leIllPQrArr Trnnsfer-In Codo gt
In the cao of n 2ratl8fcr-In I you lUot n160 cOrlpleto coluons 42-51
In the cllU J of A ~~emporary TranGfor-1n (an individual who i8 only v1citing fur clinic tor some epecial trcatcont hna who will bo rdnlnin
~middot(II~~~fO~l~SIl~I3~nn~~~h~rO~nh~1~~190~~nll 2-46 and ler rei IItrntion numbu in colullnll41-51
It the oli( nt i iNt a CrllnoforwIu - Out or loClporu1 tMn loave oolumn 1 blank
16 lr4nst(gtr-tl2~~morrry TilJnder-In (co 42-51) Forl1ltl CUn E1~ (cc 112-46)
hen you rei iatlr L irllsfcrln or Il TJlporary Trnnsfer-In you IIIUBt write I ere the five-digit clinio nucbor of the Clinic iraQ which tho ltlient Me (uIlO
2mer ]letr ~2n ~ (cc 47-51)
frlta fllao Clo r-~itrlltion Nuc~Er ot the client in the Former Clinic (i c bullbull th 1 Sis rnmiddotion ~UlIlh()r which the client carrics 1n the tormor clinio) bull
It tho Forrltl Ho( ist rntion Number iIJ not readily wnilnble you tluct oocpluto thtl epcciol [orlll Transfer-In Not Identifiod Dy Forrlcr RCGi(trn~ t10n Nwlbvr Or ~ flt)rCl is to be cOlplctcd for och cnso nnd th forlJO Ilubmi tted to thu )opllntion Prorrnnme Of fice tOGether with tho Dily Ro~iBtors lhwev~r should the clork leuTI of tho clint B FormlI Uocintra tion lUlllb r )0[(10 Cubmi ttinft the D1ily IOCI otro t hen the nUQbcr shoulo bo -ri ton in colucns 47-51 lna the special foro should lJo deotroyotl
l7 bullbullbullbullbull
r lt bull bull
ADXI ) Pap S ot S
11 UD LV~ (cc 525)
It tb( cliont io ~ivQn An IUD tor the firot tl~o then you should Sri to Codo 1 Inuort ill colurJI 52
It tho olimiddotsnt ia rvinGgtrtltld i th An I UD bullbull tben wse Coda 2 RelnDltlrt shyin (01Uil11 52
It the clLmt is ~tte~~dint chnic beruse her IUD CflClQ out by Haol (cxpll Iion i ~hcn fir te todo ~- UIlllrli1 53~
If c-ltr IU fj IIIS reov in -ne cllnic by tho doctor or nurso t~on vlritI Codec in column 5
II the eli nt otends eiLlie tld explin[l th(lt she rccovcd the IUD tlllleel nen write Coda H in Colwlm 53
It the IUD jr still within the uterus nd the WOIraquoI1 1 11rc6llJlnt thon lIrite 1gt40 4 in Column 53
lZ np h5t (ce 54) It 0 Pull 5mor ie t~ken durin thi visit tben Codo 1 ehould be ampDtere4 in ColWlln 54 Should he c110nt lltt rQ(uircd to rttturn to clin1c for a rogtol1t Pnl) t06t then CoLe 2 llhould bo middotwrittcn in column 54
It no Pllp Scou io taken tde visit Itove colUQn 54 blank
Iraferti1lli (CQ 55)
Ii the e liett io nl1 infortili tr eaoe use Cor1o Ill in colUQn 55
If tbia 1000 not tlpl lonve column 55 blonk
20 Totaltll
CO~1ploete the [)ldegO 1gty puti YI tne totals betweon the double lines nt tu b()ttctl Carrj colUlllnc 20 21 nd gt4 Must hlve tho Bnoe JllIIber and thiG Would coreslonc to the numocr ir attencbnco
Writ$ th to1ul nUlllior of Drop-Outs returned (c022)
Urito 41eo tb totnls fOJ each card column 0 to 9 under tho h(adinu Method thiB Vioit Show tho tote L fgtr OlCl type of contraceptive issued (cc 25-40)
1)0 Dot wrLte 1111 totll lUl(Ier Card Columns 15-19 29 41-51
21 COPmllh bull ~lt h~t~ Monthly ROilort
OQ thG DaLl oCator forlll thnt ccrrOspOldB to tho 1(8t 1$06610n lt 0
oth yo Olllt (vwlgtleto the items nt the botto of the [orampl This is tour ontll~1 n(olt nnd includcD tho totll lumber of sesions Ilntl tho total Iluolcr ( r crop-outs durinr the Qonth
An tiUlsilt n drir which n doctor liB in nttcndnncc is a doctor sOfll~1on and shoulc 00 re(liGtcnd in coltns 56-57 All other sessions 1116 conlliid~recl supply stllciona and thtlY 1110 rocordod in columns 58-59
the total Ilum)nl Jf drop-outo ld the drop-outs by method durinc the onth nre 10 bu oltorou in the inrlicllted boxes
72 Chad Your ~
Milke I ura th t all thE fijul4gtu rre c101r -tNever writo our nutlUQrS 50 InrjEl that they oxtend out of tho
ap~rotr1ato ~ox
Cheek to BoJa tht 1111 numuors 1110 in tho correct boxes -- CJslHloially when Writi1 the totlB
Mllxe Cirtc O thmiddott t1e infoT1I1ntion i6 clear on the corbon COllY before sep rmiddotinr the sheets
Jitn the Fomiddotl lien tly sien YOUl nr me 1t the bot tOil right hnnd corner btl forc subol ttinG it Keep tle CL rb n copy for your rocordn
i
-l ________~~---------~
I _1
Adminiatr-atlve SKVieu
P inba ~~~l1cal lrlnbin~~eltltcal -1 te~ra t~~rvicc (lnatittloaa)
--1- - shy -1------------_-L_ l-r-aJiil- shy _-L_tet1lal d
PlIinm1tJ8 atdUon DetalMid H8Il1tb ~ ________bull Care
-----~ Office of i
the FlIily _IPlill3 roarshy
1- - - -------RegiatUll urnr
ltIi 1 Drelttor Rcgicaat Director Souta Tabqo tacallortb ~ counu gt____ ~ (4 ouottet)
Off1ce of the Res10nal Diractoc L
r----- _L_ -- shy i I bull IREgional Ipitl I
District IIttaltb I bull Othn RelOl ond Hcpital CenteIntt itlt j In 1__ _shy-~- ---- -_j
J r Ii~lth
C~nlef
L
I Ihnlth lie I th Offlcu (1ft lc~
Coullty 1I0p1ta1
Henlth tentet
I

i
MINISTTY OF Ho1TH
NTIONl F~ILY LNNING PR-GRbullbullM-tE
~~5tructions to C11nic ClerKa
How to co~ploto the Daily Rogister
~~ ~~v1sd Daily Rosi8ter replnc~D tho one which is now in use tb$ Monthly PC~ri rOt~ arti tho 01( Ci() Dod PollJ j f m It is a pre-coded form and 1411 cl~1p Jd tl a1I6iniul-mIHvn Oel Clinic nctivi~y
110 )rm rollt biJ coupJot)d lrl cupLtcoto using a o(roon shoot Tho top aheot or oriinai ~ust bl) 6(Ult to tho CQgt1tral O[[lCO and tho carbon copy retained in the Gliaic rilo dll the for6a that ar uD~d betwoen the 1st 4nd the 15th of the oIIollth aut bo subClittud tocho office 35 Lnc blttch Those oomp1cted betwoon tho 16th _lid tqemc of tho month must bo ~cnt in a secJnll batch
P lOvLior hns boon Illllde for 25 clients on cZlch forlll new forlll must b IIlied f r poundh 50[810n2 whothur or not ono or lIIore session are hoIdiit the clinic on he sarne day
I th ro alO more htl 25 clionta 1n attondnnco at tho session the additi shyOhAl m~bOl of clionts 10 clients nu~ber 26 27 etc sh0u1l be ontered on the next Imiddotrlll ~i ttout a1tpoundring the numbtlrs in the cvlumn hond Series
51 ppOfil th~ number of aUcnts lQr that session ws 5 this would mean thllt two rJlS ~ lst be 6ubllIitt~dl the first filled uF 1 tltgt 25 And the laquoIncond 1 to 10 Th~ cal bon ofies should bo st~plod togother at thu t0P l~rt h4nd corner of the torm ard ktpt in the Clinic filo lou IIlU6t stapl~ the originftls in the 8~~ monnshyer for lIub~ssion to the ofticl
ie h~ ll idontiflctior- (cc 1 - )
0 lot Ji 9 anythin~ hGro poundhia is int(mdClc for tha computer code
2 ~~pound~ - Print clOflrly tho name of your Clinic
C1Lic Huml or - (cc 4 - 8) Evar1 Clinic Numbor has 5 digits Virite each dig t il a t$purate box
It Pai~_thllsectgdllion (00 lt) -1 1) - Dl monll 10M
lw) bolte IlrO proY140d fetr olAoh pr 01 thQ dISh Enter tho dA) ldns a R
d16ih
emiddot5middot (0 11 I for 115t ( 0 21 for 5th etc Treat month the am pay
e ~ 10 ~ I for I-hrch 0 [2] for September Tho y~nr must be (into ad
I Z I ~ I I 71 q etc
Take as in IixulIple tho dOlte 3rd tllrch 1973 7~ie must bo written
[0131 LSLDI[7l3JDny Month Ye~r
5middot 1~J $~~ - Irom ~-------- To --------shytntol hOI II the time the Clinic 111118 in SW5sion emiddot8middot
(i) 11011 500 lm To 1200 non
(11) Frclt 100 pm To 400 pm
(iii ) IX-OG OO pllI To 6~00 pm
f
2
ADEJ ) Paae ) of S
6 Eov
_ 1hA 1gtIpoundC iIIUlt be nu~o7Ifd tler1ally 1 throurh n lU tbey Are Wled In ~1l8ellJ IInel 1301 tlU 1 Orcl 1 Wled tor a o5038ioll - -I 2 tonY tho _boul~ b I1WJbtl 1 and 2
hlrlll are 25 linos OIl the fOnl Ilnd thoae muet be UBtleS for 25 clients 9 one ior bullbull 01 I ini
ot ~h lc II ol1cM lOlivpound til e linic before soeinc DurOI or doc tor ilnc ii hox rristrltltion nUlJbet had alrearll been recorded on the Dai 1y Roiuter then n line ~hollld be drawn through that entry an1 the eliort nust not 06 includttd in tho totals tor that 0eDion
1lw Ileifitration Num)~r of cueh client must be IiIritten IS n 5-dlrlt oode ClhnC IH11IlElr 315 1IIU8 tborotore be enterod 18J010117]5]
~ Clt ZOt
Coda 1 Codo
10 ~tl c 2t j co 21)
~w elSe - Coda 1 0) d CltaEl - Code 2 Revislt Code 3
Only pound1 01 theBe coiles may be usod
11 prol-O~ ~Eil~1 (cc 22)
If ma climt was L drop-out IIho haoS returned now to the Clinio tor tho first no linmiddot bullwin lt1ro1eo o t he or she should be given CCe 1 It this do 5 II It nprlly leu this colWlln blank
u Hothod middothisllill loe 23)
NOh til t otly ~ Cod 16 tp he ontered in 2lpound of the columna oven thOUGh 10 co11lllJlB 10 provided on the torm The Codes llrol-
Oral Contraceptive Code 0 1 U D Code 1 Condom plUD Codo Z Condor (only) Code 3 Foum tAblets cream Code it DitphrClGJII Code 5 Rhythm Cde 6 Injectible Code 7 Advice Code 8 Other Code 9
It for middotDo-le 1 client rlllll ji yen cclldorls ord foam or creall Iou Qust entor Coole i (condom plulJ) in the appropri~te column This Quat be the only lIotmiddot) tarcie If an in the cnse of a tlnle clinic I the client is Bup)lieu lith COIlOrW only you rmot entEr CorlQ 3 (cpndolll) Do not use a ticII ~ tho (odo Nwber
It is CUi tomary fur 11 cliont 110 is beine put on the oral contraceptive for the first tiT1o and even on other occasionn be issued condoms and 11 crelle or foam a Ilell rI3 a pgtcket of pilla In such Cllses when the piDQ Ilre Ilctually iouou you tlust record Orll (Co~e 0) 08 tho onll metbod ilo othor ntry sll0uld ho nnrlo
Uovever n SJC~ canas vucru condoms and fOHa ~rc eiven but no pilJa (even thoJRh _t _n the intention to issue pills nt the noxt vioit) than the Mothol Th5 ifli t ohoulcl be recorded uo Condor Plus (Code 2)
13 Seen Bybullbullbullbullbull
~rot S-1 SO l
Doctor (Dr) - Code 1 j Nurse (Nul ) - Code 2
Clark (Olk-) - Code If tho Clhnt is vcen hy both tho llootor tlnd the Nurse enter Code 1 t Doctor It 6~61l by the Nurso only arite Code 2 Cod bullbull Cerk is l)llnt for FA Cllnica Clerks in tho Government Cli1t hiwo Llttoll istructed not to i56uo supplios on their own volition
14 fl221~
lhio S~tiCl of -Ie fvrtl t~ke 16 (llrci coluMna (cc 25-+0) nnd 10 tho only part at th iOIQ in llich iore thAn one cod is Zlccoptl1blo Tho purpoco of the )ecton is to 0 able to arrive nt the Cjunntity of 6tock dilltlitJutshyed YOI IIlUdt writo in the CllllOjH-iata colulna the nUllbJr of Il1ch 4rtic1o i~JSu~d ~lo e ha I Oral Contrcilpti vea are aub-di vi dod into types ae_ 3 PIllCKC 9 0 Elynnn LlUot be entered Codo in card column 25
If tor eXllrplc t l cliunt is iosued wi th packots of Zucynon nnd aJ(1 ~ivn 1 conuotll (8inoloo) you ouot enter in oard column 25 and 11 It
cnrd col~8 )2 and J (io 1 in card colucn 2 nnd 2 1n card coluun 33) Nota C)lldoIlU ale to b(t ruoordod individually not os packots of throo) Should n ne LlondoClo be isoued thil3 is to be rc-Qed as 09
If It clint 6 t~ot isoued Blly lIupplies thon you must writo Codo 1 in CQllAlilD 41
It Q eli nt isite the clinic to check on her LUD or her Diaphra~t IUId ro DI W 6 ppl ills nre ispounducd then Code 1 1s wri t ten in column 40
In the FA clinios here a variety ot orll contraceptiveo in orer~l tho elerll wilmiddot~ bJ provided with a specill code shoot The idontifyin coo will b wiittn in Column 29 nnd the nUlber of packets iosued in colwm )0
lralaer-In Code 1 lrllllsie r~ut Coda 2 leIllPQrArr Trnnsfer-In Codo gt
In the cao of n 2ratl8fcr-In I you lUot n160 cOrlpleto coluons 42-51
In the cllU J of A ~~emporary TranGfor-1n (an individual who i8 only v1citing fur clinic tor some epecial trcatcont hna who will bo rdnlnin
~middot(II~~~fO~l~SIl~I3~nn~~~h~rO~nh~1~~190~~nll 2-46 and ler rei IItrntion numbu in colullnll41-51
It the oli( nt i iNt a CrllnoforwIu - Out or loClporu1 tMn loave oolumn 1 blank
16 lr4nst(gtr-tl2~~morrry TilJnder-In (co 42-51) Forl1ltl CUn E1~ (cc 112-46)
hen you rei iatlr L irllsfcrln or Il TJlporary Trnnsfer-In you IIIUBt write I ere the five-digit clinio nucbor of the Clinic iraQ which tho ltlient Me (uIlO
2mer ]letr ~2n ~ (cc 47-51)
frlta fllao Clo r-~itrlltion Nuc~Er ot the client in the Former Clinic (i c bullbull th 1 Sis rnmiddotion ~UlIlh()r which the client carrics 1n the tormor clinio) bull
It tho Forrltl Ho( ist rntion Number iIJ not readily wnilnble you tluct oocpluto thtl epcciol [orlll Transfer-In Not Identifiod Dy Forrlcr RCGi(trn~ t10n Nwlbvr Or ~ flt)rCl is to be cOlplctcd for och cnso nnd th forlJO Ilubmi tted to thu )opllntion Prorrnnme Of fice tOGether with tho Dily Ro~iBtors lhwev~r should the clork leuTI of tho clint B FormlI Uocintra tion lUlllb r )0[(10 Cubmi ttinft the D1ily IOCI otro t hen the nUQbcr shoulo bo -ri ton in colucns 47-51 lna the special foro should lJo deotroyotl
l7 bullbullbullbullbull
r lt bull bull
ADXI ) Pap S ot S
11 UD LV~ (cc 525)
It tb( cliont io ~ivQn An IUD tor the firot tl~o then you should Sri to Codo 1 Inuort ill colurJI 52
It tho olimiddotsnt ia rvinGgtrtltld i th An I UD bullbull tben wse Coda 2 RelnDltlrt shyin (01Uil11 52
It the clLmt is ~tte~~dint chnic beruse her IUD CflClQ out by Haol (cxpll Iion i ~hcn fir te todo ~- UIlllrli1 53~
If c-ltr IU fj IIIS reov in -ne cllnic by tho doctor or nurso t~on vlritI Codec in column 5
II the eli nt otends eiLlie tld explin[l th(lt she rccovcd the IUD tlllleel nen write Coda H in Colwlm 53
It the IUD jr still within the uterus nd the WOIraquoI1 1 11rc6llJlnt thon lIrite 1gt40 4 in Column 53
lZ np h5t (ce 54) It 0 Pull 5mor ie t~ken durin thi visit tben Codo 1 ehould be ampDtere4 in ColWlln 54 Should he c110nt lltt rQ(uircd to rttturn to clin1c for a rogtol1t Pnl) t06t then CoLe 2 llhould bo middotwrittcn in column 54
It no Pllp Scou io taken tde visit Itove colUQn 54 blank
Iraferti1lli (CQ 55)
Ii the e liett io nl1 infortili tr eaoe use Cor1o Ill in colUQn 55
If tbia 1000 not tlpl lonve column 55 blonk
20 Totaltll
CO~1ploete the [)ldegO 1gty puti YI tne totals betweon the double lines nt tu b()ttctl Carrj colUlllnc 20 21 nd gt4 Must hlve tho Bnoe JllIIber and thiG Would coreslonc to the numocr ir attencbnco
Writ$ th to1ul nUlllior of Drop-Outs returned (c022)
Urito 41eo tb totnls fOJ each card column 0 to 9 under tho h(adinu Method thiB Vioit Show tho tote L fgtr OlCl type of contraceptive issued (cc 25-40)
1)0 Dot wrLte 1111 totll lUl(Ier Card Columns 15-19 29 41-51
21 COPmllh bull ~lt h~t~ Monthly ROilort
OQ thG DaLl oCator forlll thnt ccrrOspOldB to tho 1(8t 1$06610n lt 0
oth yo Olllt (vwlgtleto the items nt the botto of the [orampl This is tour ontll~1 n(olt nnd includcD tho totll lumber of sesions Ilntl tho total Iluolcr ( r crop-outs durinr the Qonth
An tiUlsilt n drir which n doctor liB in nttcndnncc is a doctor sOfll~1on and shoulc 00 re(liGtcnd in coltns 56-57 All other sessions 1116 conlliid~recl supply stllciona and thtlY 1110 rocordod in columns 58-59
the total Ilum)nl Jf drop-outo ld the drop-outs by method durinc the onth nre 10 bu oltorou in the inrlicllted boxes
72 Chad Your ~
Milke I ura th t all thE fijul4gtu rre c101r -tNever writo our nutlUQrS 50 InrjEl that they oxtend out of tho
ap~rotr1ato ~ox
Cheek to BoJa tht 1111 numuors 1110 in tho correct boxes -- CJslHloially when Writi1 the totlB
Mllxe Cirtc O thmiddott t1e infoT1I1ntion i6 clear on the corbon COllY before sep rmiddotinr the sheets
Jitn the Fomiddotl lien tly sien YOUl nr me 1t the bot tOil right hnnd corner btl forc subol ttinG it Keep tle CL rb n copy for your rocordn
i
-l ________~~---------~
I _1
Adminiatr-atlve SKVieu
P inba ~~~l1cal lrlnbin~~eltltcal -1 te~ra t~~rvicc (lnatittloaa)
--1- - shy -1------------_-L_ l-r-aJiil- shy _-L_tet1lal d
PlIinm1tJ8 atdUon DetalMid H8Il1tb ~ ________bull Care
-----~ Office of i
the FlIily _IPlill3 roarshy
1- - - -------RegiatUll urnr
ltIi 1 Drelttor Rcgicaat Director Souta Tabqo tacallortb ~ counu gt____ ~ (4 ouottet)
Off1ce of the Res10nal Diractoc L
r----- _L_ -- shy i I bull IREgional Ipitl I
District IIttaltb I bull Othn RelOl ond Hcpital CenteIntt itlt j In 1__ _shy-~- ---- -_j
J r Ii~lth
C~nlef
L
I Ihnlth lie I th Offlcu (1ft lc~
Coullty 1I0p1ta1
Henlth tentet
I

f
2
ADEJ ) Paae ) of S
6 Eov
_ 1hA 1gtIpoundC iIIUlt be nu~o7Ifd tler1ally 1 throurh n lU tbey Are Wled In ~1l8ellJ IInel 1301 tlU 1 Orcl 1 Wled tor a o5038ioll - -I 2 tonY tho _boul~ b I1WJbtl 1 and 2
hlrlll are 25 linos OIl the fOnl Ilnd thoae muet be UBtleS for 25 clients 9 one ior bullbull 01 I ini
ot ~h lc II ol1cM lOlivpound til e linic before soeinc DurOI or doc tor ilnc ii hox rristrltltion nUlJbet had alrearll been recorded on the Dai 1y Roiuter then n line ~hollld be drawn through that entry an1 the eliort nust not 06 includttd in tho totals tor that 0eDion
1lw Ileifitration Num)~r of cueh client must be IiIritten IS n 5-dlrlt oode ClhnC IH11IlElr 315 1IIU8 tborotore be enterod 18J010117]5]
~ Clt ZOt
Coda 1 Codo
10 ~tl c 2t j co 21)
~w elSe - Coda 1 0) d CltaEl - Code 2 Revislt Code 3
Only pound1 01 theBe coiles may be usod
11 prol-O~ ~Eil~1 (cc 22)
If ma climt was L drop-out IIho haoS returned now to the Clinio tor tho first no linmiddot bullwin lt1ro1eo o t he or she should be given CCe 1 It this do 5 II It nprlly leu this colWlln blank
u Hothod middothisllill loe 23)
NOh til t otly ~ Cod 16 tp he ontered in 2lpound of the columna oven thOUGh 10 co11lllJlB 10 provided on the torm The Codes llrol-
Oral Contraceptive Code 0 1 U D Code 1 Condom plUD Codo Z Condor (only) Code 3 Foum tAblets cream Code it DitphrClGJII Code 5 Rhythm Cde 6 Injectible Code 7 Advice Code 8 Other Code 9
It for middotDo-le 1 client rlllll ji yen cclldorls ord foam or creall Iou Qust entor Coole i (condom plulJ) in the appropri~te column This Quat be the only lIotmiddot) tarcie If an in the cnse of a tlnle clinic I the client is Bup)lieu lith COIlOrW only you rmot entEr CorlQ 3 (cpndolll) Do not use a ticII ~ tho (odo Nwber
It is CUi tomary fur 11 cliont 110 is beine put on the oral contraceptive for the first tiT1o and even on other occasionn be issued condoms and 11 crelle or foam a Ilell rI3 a pgtcket of pilla In such Cllses when the piDQ Ilre Ilctually iouou you tlust record Orll (Co~e 0) 08 tho onll metbod ilo othor ntry sll0uld ho nnrlo
Uovever n SJC~ canas vucru condoms and fOHa ~rc eiven but no pilJa (even thoJRh _t _n the intention to issue pills nt the noxt vioit) than the Mothol Th5 ifli t ohoulcl be recorded uo Condor Plus (Code 2)
13 Seen Bybullbullbullbullbull
~rot S-1 SO l
Doctor (Dr) - Code 1 j Nurse (Nul ) - Code 2
Clark (Olk-) - Code If tho Clhnt is vcen hy both tho llootor tlnd the Nurse enter Code 1 t Doctor It 6~61l by the Nurso only arite Code 2 Cod bullbull Cerk is l)llnt for FA Cllnica Clerks in tho Government Cli1t hiwo Llttoll istructed not to i56uo supplios on their own volition
14 fl221~
lhio S~tiCl of -Ie fvrtl t~ke 16 (llrci coluMna (cc 25-+0) nnd 10 tho only part at th iOIQ in llich iore thAn one cod is Zlccoptl1blo Tho purpoco of the )ecton is to 0 able to arrive nt the Cjunntity of 6tock dilltlitJutshyed YOI IIlUdt writo in the CllllOjH-iata colulna the nUllbJr of Il1ch 4rtic1o i~JSu~d ~lo e ha I Oral Contrcilpti vea are aub-di vi dod into types ae_ 3 PIllCKC 9 0 Elynnn LlUot be entered Codo in card column 25
If tor eXllrplc t l cliunt is iosued wi th packots of Zucynon nnd aJ(1 ~ivn 1 conuotll (8inoloo) you ouot enter in oard column 25 and 11 It
cnrd col~8 )2 and J (io 1 in card colucn 2 nnd 2 1n card coluun 33) Nota C)lldoIlU ale to b(t ruoordod individually not os packots of throo) Should n ne LlondoClo be isoued thil3 is to be rc-Qed as 09
If It clint 6 t~ot isoued Blly lIupplies thon you must writo Codo 1 in CQllAlilD 41
It Q eli nt isite the clinic to check on her LUD or her Diaphra~t IUId ro DI W 6 ppl ills nre ispounducd then Code 1 1s wri t ten in column 40
In the FA clinios here a variety ot orll contraceptiveo in orer~l tho elerll wilmiddot~ bJ provided with a specill code shoot The idontifyin coo will b wiittn in Column 29 nnd the nUlber of packets iosued in colwm )0
lralaer-In Code 1 lrllllsie r~ut Coda 2 leIllPQrArr Trnnsfer-In Codo gt
In the cao of n 2ratl8fcr-In I you lUot n160 cOrlpleto coluons 42-51
In the cllU J of A ~~emporary TranGfor-1n (an individual who i8 only v1citing fur clinic tor some epecial trcatcont hna who will bo rdnlnin
~middot(II~~~fO~l~SIl~I3~nn~~~h~rO~nh~1~~190~~nll 2-46 and ler rei IItrntion numbu in colullnll41-51
It the oli( nt i iNt a CrllnoforwIu - Out or loClporu1 tMn loave oolumn 1 blank
16 lr4nst(gtr-tl2~~morrry TilJnder-In (co 42-51) Forl1ltl CUn E1~ (cc 112-46)
hen you rei iatlr L irllsfcrln or Il TJlporary Trnnsfer-In you IIIUBt write I ere the five-digit clinio nucbor of the Clinic iraQ which tho ltlient Me (uIlO
2mer ]letr ~2n ~ (cc 47-51)
frlta fllao Clo r-~itrlltion Nuc~Er ot the client in the Former Clinic (i c bullbull th 1 Sis rnmiddotion ~UlIlh()r which the client carrics 1n the tormor clinio) bull
It tho Forrltl Ho( ist rntion Number iIJ not readily wnilnble you tluct oocpluto thtl epcciol [orlll Transfer-In Not Identifiod Dy Forrlcr RCGi(trn~ t10n Nwlbvr Or ~ flt)rCl is to be cOlplctcd for och cnso nnd th forlJO Ilubmi tted to thu )opllntion Prorrnnme Of fice tOGether with tho Dily Ro~iBtors lhwev~r should the clork leuTI of tho clint B FormlI Uocintra tion lUlllb r )0[(10 Cubmi ttinft the D1ily IOCI otro t hen the nUQbcr shoulo bo -ri ton in colucns 47-51 lna the special foro should lJo deotroyotl
l7 bullbullbullbullbull
r lt bull bull
ADXI ) Pap S ot S
11 UD LV~ (cc 525)
It tb( cliont io ~ivQn An IUD tor the firot tl~o then you should Sri to Codo 1 Inuort ill colurJI 52
It tho olimiddotsnt ia rvinGgtrtltld i th An I UD bullbull tben wse Coda 2 RelnDltlrt shyin (01Uil11 52
It the clLmt is ~tte~~dint chnic beruse her IUD CflClQ out by Haol (cxpll Iion i ~hcn fir te todo ~- UIlllrli1 53~
If c-ltr IU fj IIIS reov in -ne cllnic by tho doctor or nurso t~on vlritI Codec in column 5
II the eli nt otends eiLlie tld explin[l th(lt she rccovcd the IUD tlllleel nen write Coda H in Colwlm 53
It the IUD jr still within the uterus nd the WOIraquoI1 1 11rc6llJlnt thon lIrite 1gt40 4 in Column 53
lZ np h5t (ce 54) It 0 Pull 5mor ie t~ken durin thi visit tben Codo 1 ehould be ampDtere4 in ColWlln 54 Should he c110nt lltt rQ(uircd to rttturn to clin1c for a rogtol1t Pnl) t06t then CoLe 2 llhould bo middotwrittcn in column 54
It no Pllp Scou io taken tde visit Itove colUQn 54 blank
Iraferti1lli (CQ 55)
Ii the e liett io nl1 infortili tr eaoe use Cor1o Ill in colUQn 55
If tbia 1000 not tlpl lonve column 55 blonk
20 Totaltll
CO~1ploete the [)ldegO 1gty puti YI tne totals betweon the double lines nt tu b()ttctl Carrj colUlllnc 20 21 nd gt4 Must hlve tho Bnoe JllIIber and thiG Would coreslonc to the numocr ir attencbnco
Writ$ th to1ul nUlllior of Drop-Outs returned (c022)
Urito 41eo tb totnls fOJ each card column 0 to 9 under tho h(adinu Method thiB Vioit Show tho tote L fgtr OlCl type of contraceptive issued (cc 25-40)
1)0 Dot wrLte 1111 totll lUl(Ier Card Columns 15-19 29 41-51
21 COPmllh bull ~lt h~t~ Monthly ROilort
OQ thG DaLl oCator forlll thnt ccrrOspOldB to tho 1(8t 1$06610n lt 0
oth yo Olllt (vwlgtleto the items nt the botto of the [orampl This is tour ontll~1 n(olt nnd includcD tho totll lumber of sesions Ilntl tho total Iluolcr ( r crop-outs durinr the Qonth
An tiUlsilt n drir which n doctor liB in nttcndnncc is a doctor sOfll~1on and shoulc 00 re(liGtcnd in coltns 56-57 All other sessions 1116 conlliid~recl supply stllciona and thtlY 1110 rocordod in columns 58-59
the total Ilum)nl Jf drop-outo ld the drop-outs by method durinc the onth nre 10 bu oltorou in the inrlicllted boxes
72 Chad Your ~
Milke I ura th t all thE fijul4gtu rre c101r -tNever writo our nutlUQrS 50 InrjEl that they oxtend out of tho
ap~rotr1ato ~ox
Cheek to BoJa tht 1111 numuors 1110 in tho correct boxes -- CJslHloially when Writi1 the totlB
Mllxe Cirtc O thmiddott t1e infoT1I1ntion i6 clear on the corbon COllY before sep rmiddotinr the sheets
Jitn the Fomiddotl lien tly sien YOUl nr me 1t the bot tOil right hnnd corner btl forc subol ttinG it Keep tle CL rb n copy for your rocordn
i
-l ________~~---------~
I _1
Adminiatr-atlve SKVieu
P inba ~~~l1cal lrlnbin~~eltltcal -1 te~ra t~~rvicc (lnatittloaa)
--1- - shy -1------------_-L_ l-r-aJiil- shy _-L_tet1lal d
PlIinm1tJ8 atdUon DetalMid H8Il1tb ~ ________bull Care
-----~ Office of i
the FlIily _IPlill3 roarshy
1- - - -------RegiatUll urnr
ltIi 1 Drelttor Rcgicaat Director Souta Tabqo tacallortb ~ counu gt____ ~ (4 ouottet)
Off1ce of the Res10nal Diractoc L
r----- _L_ -- shy i I bull IREgional Ipitl I
District IIttaltb I bull Othn RelOl ond Hcpital CenteIntt itlt j In 1__ _shy-~- ---- -_j
J r Ii~lth
C~nlef
L
I Ihnlth lie I th Offlcu (1ft lc~
Coullty 1I0p1ta1
Henlth tentet
I

~rot S-1 SO l
Doctor (Dr) - Code 1 j Nurse (Nul ) - Code 2
Clark (Olk-) - Code If tho Clhnt is vcen hy both tho llootor tlnd the Nurse enter Code 1 t Doctor It 6~61l by the Nurso only arite Code 2 Cod bullbull Cerk is l)llnt for FA Cllnica Clerks in tho Government Cli1t hiwo Llttoll istructed not to i56uo supplios on their own volition
14 fl221~
lhio S~tiCl of -Ie fvrtl t~ke 16 (llrci coluMna (cc 25-+0) nnd 10 tho only part at th iOIQ in llich iore thAn one cod is Zlccoptl1blo Tho purpoco of the )ecton is to 0 able to arrive nt the Cjunntity of 6tock dilltlitJutshyed YOI IIlUdt writo in the CllllOjH-iata colulna the nUllbJr of Il1ch 4rtic1o i~JSu~d ~lo e ha I Oral Contrcilpti vea are aub-di vi dod into types ae_ 3 PIllCKC 9 0 Elynnn LlUot be entered Codo in card column 25
If tor eXllrplc t l cliunt is iosued wi th packots of Zucynon nnd aJ(1 ~ivn 1 conuotll (8inoloo) you ouot enter in oard column 25 and 11 It
cnrd col~8 )2 and J (io 1 in card colucn 2 nnd 2 1n card coluun 33) Nota C)lldoIlU ale to b(t ruoordod individually not os packots of throo) Should n ne LlondoClo be isoued thil3 is to be rc-Qed as 09
If It clint 6 t~ot isoued Blly lIupplies thon you must writo Codo 1 in CQllAlilD 41
It Q eli nt isite the clinic to check on her LUD or her Diaphra~t IUId ro DI W 6 ppl ills nre ispounducd then Code 1 1s wri t ten in column 40
In the FA clinios here a variety ot orll contraceptiveo in orer~l tho elerll wilmiddot~ bJ provided with a specill code shoot The idontifyin coo will b wiittn in Column 29 nnd the nUlber of packets iosued in colwm )0
lralaer-In Code 1 lrllllsie r~ut Coda 2 leIllPQrArr Trnnsfer-In Codo gt
In the cao of n 2ratl8fcr-In I you lUot n160 cOrlpleto coluons 42-51
In the cllU J of A ~~emporary TranGfor-1n (an individual who i8 only v1citing fur clinic tor some epecial trcatcont hna who will bo rdnlnin
~middot(II~~~fO~l~SIl~I3~nn~~~h~rO~nh~1~~190~~nll 2-46 and ler rei IItrntion numbu in colullnll41-51
It the oli( nt i iNt a CrllnoforwIu - Out or loClporu1 tMn loave oolumn 1 blank
16 lr4nst(gtr-tl2~~morrry TilJnder-In (co 42-51) Forl1ltl CUn E1~ (cc 112-46)
hen you rei iatlr L irllsfcrln or Il TJlporary Trnnsfer-In you IIIUBt write I ere the five-digit clinio nucbor of the Clinic iraQ which tho ltlient Me (uIlO
2mer ]letr ~2n ~ (cc 47-51)
frlta fllao Clo r-~itrlltion Nuc~Er ot the client in the Former Clinic (i c bullbull th 1 Sis rnmiddotion ~UlIlh()r which the client carrics 1n the tormor clinio) bull
It tho Forrltl Ho( ist rntion Number iIJ not readily wnilnble you tluct oocpluto thtl epcciol [orlll Transfer-In Not Identifiod Dy Forrlcr RCGi(trn~ t10n Nwlbvr Or ~ flt)rCl is to be cOlplctcd for och cnso nnd th forlJO Ilubmi tted to thu )opllntion Prorrnnme Of fice tOGether with tho Dily Ro~iBtors lhwev~r should the clork leuTI of tho clint B FormlI Uocintra tion lUlllb r )0[(10 Cubmi ttinft the D1ily IOCI otro t hen the nUQbcr shoulo bo -ri ton in colucns 47-51 lna the special foro should lJo deotroyotl
l7 bullbullbullbullbull
r lt bull bull
ADXI ) Pap S ot S
11 UD LV~ (cc 525)
It tb( cliont io ~ivQn An IUD tor the firot tl~o then you should Sri to Codo 1 Inuort ill colurJI 52
It tho olimiddotsnt ia rvinGgtrtltld i th An I UD bullbull tben wse Coda 2 RelnDltlrt shyin (01Uil11 52
It the clLmt is ~tte~~dint chnic beruse her IUD CflClQ out by Haol (cxpll Iion i ~hcn fir te todo ~- UIlllrli1 53~
If c-ltr IU fj IIIS reov in -ne cllnic by tho doctor or nurso t~on vlritI Codec in column 5
II the eli nt otends eiLlie tld explin[l th(lt she rccovcd the IUD tlllleel nen write Coda H in Colwlm 53
It the IUD jr still within the uterus nd the WOIraquoI1 1 11rc6llJlnt thon lIrite 1gt40 4 in Column 53
lZ np h5t (ce 54) It 0 Pull 5mor ie t~ken durin thi visit tben Codo 1 ehould be ampDtere4 in ColWlln 54 Should he c110nt lltt rQ(uircd to rttturn to clin1c for a rogtol1t Pnl) t06t then CoLe 2 llhould bo middotwrittcn in column 54
It no Pllp Scou io taken tde visit Itove colUQn 54 blank
Iraferti1lli (CQ 55)
Ii the e liett io nl1 infortili tr eaoe use Cor1o Ill in colUQn 55
If tbia 1000 not tlpl lonve column 55 blonk
20 Totaltll
CO~1ploete the [)ldegO 1gty puti YI tne totals betweon the double lines nt tu b()ttctl Carrj colUlllnc 20 21 nd gt4 Must hlve tho Bnoe JllIIber and thiG Would coreslonc to the numocr ir attencbnco
Writ$ th to1ul nUlllior of Drop-Outs returned (c022)
Urito 41eo tb totnls fOJ each card column 0 to 9 under tho h(adinu Method thiB Vioit Show tho tote L fgtr OlCl type of contraceptive issued (cc 25-40)
1)0 Dot wrLte 1111 totll lUl(Ier Card Columns 15-19 29 41-51
21 COPmllh bull ~lt h~t~ Monthly ROilort
OQ thG DaLl oCator forlll thnt ccrrOspOldB to tho 1(8t 1$06610n lt 0
oth yo Olllt (vwlgtleto the items nt the botto of the [orampl This is tour ontll~1 n(olt nnd includcD tho totll lumber of sesions Ilntl tho total Iluolcr ( r crop-outs durinr the Qonth
An tiUlsilt n drir which n doctor liB in nttcndnncc is a doctor sOfll~1on and shoulc 00 re(liGtcnd in coltns 56-57 All other sessions 1116 conlliid~recl supply stllciona and thtlY 1110 rocordod in columns 58-59
the total Ilum)nl Jf drop-outo ld the drop-outs by method durinc the onth nre 10 bu oltorou in the inrlicllted boxes
72 Chad Your ~
Milke I ura th t all thE fijul4gtu rre c101r -tNever writo our nutlUQrS 50 InrjEl that they oxtend out of tho
ap~rotr1ato ~ox
Cheek to BoJa tht 1111 numuors 1110 in tho correct boxes -- CJslHloially when Writi1 the totlB
Mllxe Cirtc O thmiddott t1e infoT1I1ntion i6 clear on the corbon COllY before sep rmiddotinr the sheets
Jitn the Fomiddotl lien tly sien YOUl nr me 1t the bot tOil right hnnd corner btl forc subol ttinG it Keep tle CL rb n copy for your rocordn
i
-l ________~~---------~
I _1
Adminiatr-atlve SKVieu
P inba ~~~l1cal lrlnbin~~eltltcal -1 te~ra t~~rvicc (lnatittloaa)
--1- - shy -1------------_-L_ l-r-aJiil- shy _-L_tet1lal d
PlIinm1tJ8 atdUon DetalMid H8Il1tb ~ ________bull Care
-----~ Office of i
the FlIily _IPlill3 roarshy
1- - - -------RegiatUll urnr
ltIi 1 Drelttor Rcgicaat Director Souta Tabqo tacallortb ~ counu gt____ ~ (4 ouottet)
Off1ce of the Res10nal Diractoc L
r----- _L_ -- shy i I bull IREgional Ipitl I
District IIttaltb I bull Othn RelOl ond Hcpital CenteIntt itlt j In 1__ _shy-~- ---- -_j
J r Ii~lth
C~nlef
L
I Ihnlth lie I th Offlcu (1ft lc~
Coullty 1I0p1ta1
Henlth tentet
I

r lt bull bull
ADXI ) Pap S ot S
11 UD LV~ (cc 525)
It tb( cliont io ~ivQn An IUD tor the firot tl~o then you should Sri to Codo 1 Inuort ill colurJI 52
It tho olimiddotsnt ia rvinGgtrtltld i th An I UD bullbull tben wse Coda 2 RelnDltlrt shyin (01Uil11 52
It the clLmt is ~tte~~dint chnic beruse her IUD CflClQ out by Haol (cxpll Iion i ~hcn fir te todo ~- UIlllrli1 53~
If c-ltr IU fj IIIS reov in -ne cllnic by tho doctor or nurso t~on vlritI Codec in column 5
II the eli nt otends eiLlie tld explin[l th(lt she rccovcd the IUD tlllleel nen write Coda H in Colwlm 53
It the IUD jr still within the uterus nd the WOIraquoI1 1 11rc6llJlnt thon lIrite 1gt40 4 in Column 53
lZ np h5t (ce 54) It 0 Pull 5mor ie t~ken durin thi visit tben Codo 1 ehould be ampDtere4 in ColWlln 54 Should he c110nt lltt rQ(uircd to rttturn to clin1c for a rogtol1t Pnl) t06t then CoLe 2 llhould bo middotwrittcn in column 54
It no Pllp Scou io taken tde visit Itove colUQn 54 blank
Iraferti1lli (CQ 55)
Ii the e liett io nl1 infortili tr eaoe use Cor1o Ill in colUQn 55
If tbia 1000 not tlpl lonve column 55 blonk
20 Totaltll
CO~1ploete the [)ldegO 1gty puti YI tne totals betweon the double lines nt tu b()ttctl Carrj colUlllnc 20 21 nd gt4 Must hlve tho Bnoe JllIIber and thiG Would coreslonc to the numocr ir attencbnco
Writ$ th to1ul nUlllior of Drop-Outs returned (c022)
Urito 41eo tb totnls fOJ each card column 0 to 9 under tho h(adinu Method thiB Vioit Show tho tote L fgtr OlCl type of contraceptive issued (cc 25-40)
1)0 Dot wrLte 1111 totll lUl(Ier Card Columns 15-19 29 41-51
21 COPmllh bull ~lt h~t~ Monthly ROilort
OQ thG DaLl oCator forlll thnt ccrrOspOldB to tho 1(8t 1$06610n lt 0
oth yo Olllt (vwlgtleto the items nt the botto of the [orampl This is tour ontll~1 n(olt nnd includcD tho totll lumber of sesions Ilntl tho total Iluolcr ( r crop-outs durinr the Qonth
An tiUlsilt n drir which n doctor liB in nttcndnncc is a doctor sOfll~1on and shoulc 00 re(liGtcnd in coltns 56-57 All other sessions 1116 conlliid~recl supply stllciona and thtlY 1110 rocordod in columns 58-59
the total Ilum)nl Jf drop-outo ld the drop-outs by method durinc the onth nre 10 bu oltorou in the inrlicllted boxes
72 Chad Your ~
Milke I ura th t all thE fijul4gtu rre c101r -tNever writo our nutlUQrS 50 InrjEl that they oxtend out of tho
ap~rotr1ato ~ox
Cheek to BoJa tht 1111 numuors 1110 in tho correct boxes -- CJslHloially when Writi1 the totlB
Mllxe Cirtc O thmiddott t1e infoT1I1ntion i6 clear on the corbon COllY before sep rmiddotinr the sheets
Jitn the Fomiddotl lien tly sien YOUl nr me 1t the bot tOil right hnnd corner btl forc subol ttinG it Keep tle CL rb n copy for your rocordn
i
-l ________~~---------~
I _1
Adminiatr-atlve SKVieu
P inba ~~~l1cal lrlnbin~~eltltcal -1 te~ra t~~rvicc (lnatittloaa)
--1- - shy -1------------_-L_ l-r-aJiil- shy _-L_tet1lal d
PlIinm1tJ8 atdUon DetalMid H8Il1tb ~ ________bull Care
-----~ Office of i
the FlIily _IPlill3 roarshy
1- - - -------RegiatUll urnr
ltIi 1 Drelttor Rcgicaat Director Souta Tabqo tacallortb ~ counu gt____ ~ (4 ouottet)
Off1ce of the Res10nal Diractoc L
r----- _L_ -- shy i I bull IREgional Ipitl I
District IIttaltb I bull Othn RelOl ond Hcpital CenteIntt itlt j In 1__ _shy-~- ---- -_j
J r Ii~lth
C~nlef
L
I Ihnlth lie I th Offlcu (1ft lc~
Coullty 1I0p1ta1
Henlth tentet
I

i
-l ________~~---------~
I _1
Adminiatr-atlve SKVieu
P inba ~~~l1cal lrlnbin~~eltltcal -1 te~ra t~~rvicc (lnatittloaa)
--1- - shy -1------------_-L_ l-r-aJiil- shy _-L_tet1lal d
PlIinm1tJ8 atdUon DetalMid H8Il1tb ~ ________bull Care
-----~ Office of i
the FlIily _IPlill3 roarshy
1- - - -------RegiatUll urnr
ltIi 1 Drelttor Rcgicaat Director Souta Tabqo tacallortb ~ counu gt____ ~ (4 ouottet)
Off1ce of the Res10nal Diractoc L
r----- _L_ -- shy i I bull IREgional Ipitl I
District IIttaltb I bull Othn RelOl ond Hcpital CenteIntt itlt j In 1__ _shy-~- ---- -_j
J r Ii~lth
C~nlef
L
I Ihnlth lie I th Offlcu (1ft lc~
Coullty 1I0p1ta1
Henlth tentet
I