Quality of life in heart failure patients undergoing home-based telerehabilitation versus outpatient...
9
http://cnu.sagepub.com/ European Journal of Cardiovascular Nursing http://cnu.sagepub.com/content/early/2014/05/21/1474515114537023 The online version of this article can be found at: DOI: 10.1177/1474515114537023 published online 21 May 2014 Eur J Cardiovasc Nurs Walerian Piotrowski and Ryszard Piotrowicz Ewa Piotrowicz, Monika Stepnowska, Kinga Leszczynska-Iwanicka, Dorota Piotrowska, Monika Kowalska, Jan Tylka, a randomized controlled study - rehabilitation Quality of life in heart failure patients undergoing home-based telerehabilitation versus outpatient Published by: http://www.sagepublications.com On behalf of: European Society of Cardiology can be found at: European Journal of Cardiovascular Nursing Additional services and information for http://cnu.sagepub.com/cgi/alerts Email Alerts: http://cnu.sagepub.com/subscriptions Subscriptions: http://www.sagepub.com/journalsReprints.nav Reprints: http://www.sagepub.com/journalsPermissions.nav Permissions: What is This? - May 21, 2014 OnlineFirst Version of Record >> at UQ Library on November 19, 2014 cnu.sagepub.com Downloaded from at UQ Library on November 19, 2014 cnu.sagepub.com Downloaded from
Transcript of Quality of life in heart failure patients undergoing home-based telerehabilitation versus outpatient...

http://cnu.sagepub.com/European Journal of Cardiovascular Nursing
http://cnu.sagepub.com/content/early/2014/05/21/1474515114537023The online version of this article can be found at:
DOI: 10.1177/1474515114537023
published online 21 May 2014Eur J Cardiovasc NursWalerian Piotrowski and Ryszard Piotrowicz
Ewa Piotrowicz, Monika Stepnowska, Kinga Leszczynska-Iwanicka, Dorota Piotrowska, Monika Kowalska, Jan Tylka, a randomized controlled study−rehabilitation
Quality of life in heart failure patients undergoing home-based telerehabilitation versus outpatient
Published by:
http://www.sagepublications.com
On behalf of:
European Society of Cardiology
can be found at:European Journal of Cardiovascular NursingAdditional services and information for
http://cnu.sagepub.com/cgi/alertsEmail Alerts:
http://cnu.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
What is This?
- May 21, 2014OnlineFirst Version of Record >>
at UQ Library on November 19, 2014cnu.sagepub.comDownloaded from at UQ Library on November 19, 2014cnu.sagepub.comDownloaded from

European Journal of Cardiovascular Nursing 1 –8© The European Society of Cardiology 2014Reprints and permissions: sagepub.co.uk/journalsPermissions.navDOI: 10.1177/1474515114537023cnu.sagepub.com
EUROPEANSOCIETY OFCARDIOLOGY ®
Introduction
The most common manifestation of heart failure (HF) is physical capacity impairment resulting in dyspnoea, fatigue during exercise and/or at rest, which, in turn, deteriorates the quality of life (QoL).1–4 Patients’ evaluated QoL can be an important indicator for the course and success of a thera-peutic process, enabling functioning in everyday life despite the disease. Moreover, QoL is independently related
Quality of life in heart failure patients undergoing home-based telerehabilitation versus outpatient rehabilitation – a randomized controlled study
Ewa Piotrowicz1, Monika Stepnowska2, Kinga Leszczyńska-Iwanicka2, Dorota Piotrowska2, Monika Kowalska2,3, Jan Tylka3, Walerian Piotrowski4 and Ryszard Piotrowicz2
AbstractBackground: The most common manifestation of heart failure is physical capacity impairment resulting in dyspnoea and fatigue. The disease deteriorates the quality of life (QoL). Its consequences restrict not only functioning in the physical aspect of QoL but also patients’ emotional condition.Objective: The study is aimed to assess QoL changes in HF patients after home-based telemonitored cardiac rehabilitation (HTCR Group) versus outpatient-based standard cardiac rehabilitation (SCR Group).Methods: The study comprised 131 heart failure patients (aged 56.4±10.9 years; II/III NYHA) rehabilitated for eight weeks in two random groups: HTCR Group (n=75), participating in home-based rehabilitation supervised telemedically based on walking training; SCR Group (n=56), participating in traditional outpatient-based rehabilitation (cycloergometer training). QoL parameters were assessed with a Polish version of the Medical Outcomes Study Short Form 36 Health Survey Questionnaire (SF-36).Results: After rehabilitation, both groups achieved a significant QoL improvement, both physically and mentally. HTCR Group patients improved in QoL physical categories in one subscale (physical function), and in two subscales in the mental categories (mental health, vitality). In SCR Group, three physical subscales improved (physical function, role limitation caused by physical problems, bodily pain). In the mental categories, also three subscales improved (social function, mental health, vitality).Conclusions: The study demonstrated that in heart failure patients HTCR provided a similar improvement in total QoL index as SCR. Yet it differed in QoL subscales. Patients who underwent home-based telerehabilitation observed an improvement mainly in the mental categories. Patients in SCR Group improved their general physical well-being.
KeywordsQuality of life, heart failure, telerehabilitation
Date received: 30 November 2013; revised: 28 April 2014; accepted: 29 April 2014
1Telecardiology Centre, Institute of Cardiology, Warsaw, Poland2 Department of Cardiac Rehabilitation and Noninvasive Electrocardiology, Institute of Cardiology, Warsaw, Poland
3Cardinal Stefan Wyszynski University, Warsaw, Poland4Statistics Laboratory, Institute of Cardiology, Warsaw, Poland
Corresponding author:Ewa Piotrowicz, Telecardiology Centre, Institute of Cardiology, Alpejska 42, 04-628 Warszawa, Poland. Email: [email protected]
537023 CNU0010.1177/1474515114537023European Journal of Cardiovascular NursingPiotrowicz et al.research-article2014
Original Article
at UQ Library on November 19, 2014cnu.sagepub.comDownloaded from

2 European Journal of Cardiovascular Nursing
to survival – poor QoL scores predicted higher mortality in HF patients.3 According to the European Society of Cardiology (ESC) guidelines, cardiac rehabilitation is an acknowledged form of therapy for all stable HF patients.1 Cardiac rehabilitation improves functional capacity, auto-nomic function, peripheral haemodynamics, and in most cases exerts a beneficial effect on HF patients’ QoL, that is, an increase in the ability to function physically, mentally and socially.5
Unfortunately, due to disease related limitation, not all HF patients have the opportunity to benefit fully from the traditional, standard outpatient rehabilitation.6 Thanks to the implementation of telemedicine systems, home-based telerehabilitation can be an alternative for these patients.7 Yet little is known about the impact of this new method on QoL in HF patients.
The aim of this prospective, randomized controlled study was to assess QoL changes in HF patients during home-based telemonitored cardiac rehabilitation (telereha-bilitation) (HTCR) versus outpatient-based standard car-diac rehabilitation (SCR).
Methods
The present study formed part of a prospective randomized controlled trial which compared the effectiveness, adher-ence and safety of HTCR versus SCR in HF patients. The trial showed HTCR to be as effective as SCR. In the cur-rent paper we present the changes in QoL in detail.8
For this study, patients hospitalized between July 2005 and June 2008 were recruited by the Department of Cardiac Rehabilitation and Noninvasive Electrocardiology, Institute of Cardiology, Warsaw, Poland.
We included patients of either sex with any aetiology of left ventricular systolic HF (as defined in the ESC guide-lines) diagnosed for three months and patients with left ventricular ejection fraction <40% on echocardiography, in class II or III according to the New York Heart Association (NYHA). Additionally, the study embraced patients who were clinically stable and receiving an opti-mal and stable medication regimen for at least four weeks before enrolment and finally those who were able to exer-cise using the new model of HTCR.8
The exclusion criteria were: NYHA class I or IV; unsta-ble angina; a history of an acute coronary syndrome within the previous month, coronary artery bypass grafting within the previous two months or initiation of cardiac resynchro-nization therapy within the previous year; symptomatic and/or exercise induced cardiac arrhythmia or conduction disturbances; valvular or congenital heart disease requiring surgical treatment; hypertrophic cardiomyopathy; severe pulmonary hypertension or other severe pulmonary dis-ease; uncontrolled hypertension; anaemia (haemoglobin < 10.0g/dl); acute and/or decompensated non-cardiac dis-ease; physical disability related to severe musculoskeletal
or neurological problems; acute or chronic inflammatory disease; cancer; severe psychiatric disorder; patient refusal to participate.
The study was approved by the local Ethics Committee. Each patient gave a written informed consent. All patients underwent the assessment of QoL at baseline and after completing an eight-week training programme. Following the baseline measurements, eligible patients were ran-domly assigned to either HTCR based on walking training (HTCR Group) or SCR using a cycloergometer (SCR Group).
Assessment of health-related QoL
The Polish version of the Medical Outcome Survey Short Form 36 (SF-36) questionnaire was used to assess patients’ QoL related to participating in cardiac rehabilitation. Since there are social, cultural and conceptual differences between the populations of different countries, the existing tool used to assess the QoL had to be adjusted to notions and terms functioning in the Polish language, culture and conditions.9,10
The questionnaire is designed for a subjective assess-ment of a patient’s health condition. It consists of 11 items containing 36 statements that allow eight subscales to be defined.
The eight subscales are: physical function (PF), role limitation caused by physical problems (RP), bodily pain (BP), general health (GH), social function (SF), mental health (MH), role limitation caused by emotional problems (RE), vitality (VT). The eight subscales are grouped in two categories, four subscales each. The first category is the physical component summary (PCS) with a maximum score of 103, which consists of PF, RP, BP and GH. The second category is the mental component summary (MCS) with a maximum score of 68, which includes SF, MH, RE and VT. The total QoL index in SF-36 is the sum of eight subscales of QoL points and it enables the health condition to be assessed (maximum score: 171). According to the Polish version of the questionnaire a high score represents a low degree of QoL; in other words the higher the score the more restrictions in QoL.9,10
Psychological support
Apart from filling out the SF-36 questionnaire, each patient who expressed the need for psychological support was provided with individually tailored psychological care during rehabilitation. During the first five days patients from both groups participated in once-a-day individual meetings with a psychologist. The patient’s problems con-nected with the disease, its course, treatment and rehabili-tation approval were discussed. In the following seven weeks SCR Group patients could participate in meetings with a psychologist, held three times a week, on the same
at UQ Library on November 19, 2014cnu.sagepub.comDownloaded from

Piotrowicz et al. 3
day as training sessions. Patients from HTCR Group could be given psychological support individually, during tele-phone conversations with a psychologist.
In addition to being given the initial support from a psy-chologist, patients were supported mentally and motivated to a healthy lifestyle and exercise training by the whole team executing both SCR and HTCR programmes.
Having completed the rehabilitation programme, patients from both groups had two meetings with a psy-chologist, during which they presented and discussed their feelings, needs, well-being and other aspects of QoL.
Exercise training
Cardiac rehabilitation was planned in line with the pub-lished guidelines.1,6 Exercise training was tailored indi-vidually for each patient. The training heart rate (HR) was calculated in accordance with the method known as HR reserve. This method uses the percentage of the difference between the maximum HR and the resting HR and adds this value to the resting HR. The target training HR was 40–70% of the HR reserve.
The training session in both groups consisted of three parts: a warm-up lasting 5–10 minutes (breathing and light resistance exercises, calisthenics); basic aerobic endurance training for 10–30 minutes, and five minutes cooling down. Patients in both groups trained three times a week for eight weeks.
Of note, the two groups differed in the type and supervi-sion of the training. The methodology of monitoring HTCR Group has been described previously.8,11,12 Briefly – all HTCR patients received remote equipment for telem-onitoring and supervised exercise training (Pro Plus Company, Poland), which consisted of an EHO 6 device which enabled to record and transmit the ECG and a mobile phone.
Before the beginning of a training session, patients used the mobile phone to answer a series of questions regarding their present condition and medications taken. Patients then transmitted resting ECG to the monitoring centre. If no contraindications to training were identified, patients were given permission to start the training session. The telemonitoring system had details of the training sessions pre-programmed for each patient (defined exercise dura-tion, breaks, timing of ECG recording). The times of auto-matic ECG recording were pre-set and coordinated with the exercise training. Then, the data were transmitted, stored and analysed in the monitoring centre.
Statistical analysis
Statistical analyses were performed using SAS software (version 9.2; Cary, NC, USA). To compare normally dis-tributed continuous variables, the general linear model (ANOVA) with repeated measures for changes over time
and for time–group interaction was used. The normality of distributions was verified using the Shapiro–Wilk test. The signed-rank test (for changes over time) and the Wilcoxon test (to compare groups) were used for continuous variables that were not distributed normally. The non-parametric ×2 or Fisher exact tests were used for categorical variables. p-values < 0.05 were considered significant.
According to the mean value and standard deviation of total QoL index parameter at the beginning of the experi-ment (81.6.2±27.3) and under the assumptions: signifi-cance level = 0.05, power = 0.80 and difference of this parameter over eight weeks = 20%, the sample size = 47 is satisfied. For the assumption of 25% of drop-outs the sam-ple size = 63 patients is enough for each group.
Results
Clinical characteristics and QoL
Of the 152 patients randomized, 77 were assigned to HTCR Group and 75 to SCR Group. All HTCR patients completed the eight-week rehabilitation programme. In SCR Group, 59 of 75 patients completed the rehabilitation programme. We did not observe any significant differ-ences in baseline characteristics (demographic, pharmaco-therapy, clinical parameters and NYHA functional class) and the SF-36 questionnaire score among patients who dropped out and those who completed cardiac rehabilita-tion in SCR Group. Most patients dropped out due to com-muting difficulties.
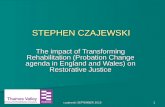
Despite the fact that two patients in HTCR Group and three patients in SCR Group completed the rehabilitation they did not undergo the final clinical examinations. One HTCR patient was waiting for heart transplantation and the other developed hyperthyroidism. Out of three SCR patients, in two cases the comorbidity (broncho- laryngeal) worsened and in one hyperthyroidism devel-oped. The remaining 75 patients in HTCR Group and 56 patients in SCR Group were included in the analysis (Figure 1). Table 1 shows the baseline clinical character-istics of the randomized patients.
At baseline, there were no significant intergroup differ-ences in terms of demographic, clinical parameters, medi-cal therapy and the total QoL index and all subscales except GH. A detailed analysis of the data obtained from the first test showed that HTCR patients assessed their GH significantly better than SCR Group patients. However, it did not affect QoL assessment in the PCS and total QoL index. A detailed outline of results in both groups before rehabilitation is presented in Table 2.
The vast majority of patients in both groups were satis-fied with the support which they received during each training session from both nurses and physiotherapists. Consequently, only two SCR patients and one HTCR patient expressed the need to contact a psychologist
at UQ Library on November 19, 2014cnu.sagepub.comDownloaded from

4 European Journal of Cardiovascular Nursing
regularly. The data were collected during meetings (SCR Group) and phone calls (HTCR Group) with the psycholo-gist and noted in the medical history.
Both groups achieved significant improvement in: total QoL index, PCS score, MCS score. In the subscales evalu-ating physical well-being, in SCR Group, improvement was observed in three (PF, RP, BP) out of four subscales. In comparison with the baseline examination findings, patients after trainings reported fewer PF restrains, found it less difficult to function socially because of better physi-cal fitness and complained less of BP.
HTCR patients improved in PCS in only one out of four subscales. They perceived their PF as better after rehabilitation. The other subscales (RP, BP, GH) did not change significantly. In the subscales assessing mental
well-being, in SCR Group, an improvement was observed in three (SF, MH, VT) out of four subscales. The results showed that SCR patients reported fewer limitations in their social functioning; moreover they had a better sense of mental health and vitality after rehabilitation completion. HTCR patients improved in MCS in two (MH, VT) out of four subscales after the rehabilitation cycle was completed. The role limitation caused by physical problems did not change signifi-cantly in both groups.
There were no statistically significant differences between the groups regarding the improvement in total QoL index, PCS score (PF, RP, BP) or MCS score (MH, RE, VT). Groups differed in terms of sense of GH and SF. An improvement in SF was observed only in SCR Group.
Figure 1. Flow of patients through the study.OHT: orthotropic heart transplantation
at UQ Library on November 19, 2014cnu.sagepub.comDownloaded from

Piotrowicz et al. 5
Cardiac rehabilitation did not have a significant effect on the sense of GH in both groups. The difference between the groups in the analysis is due to the fact that in terms of this parameter the groups differed before the beginning of the rehabilitation. Table 2 shows the details of the QoL results.
Discussion
The main and novel finding of our prospective randomized controlled study is that in stable HF patients the proposed model of HTCR provided improvement similar to SCR in terms of total QoL index, PCS and MCS. Very few reports indicated that telemonitored cardiac rehabilitation can improve QoL in low-risk cardiac patients with no HF.13,14 There is only one paper which reports that QoL improve-ment achieved during the outpatient programme was maintained during the next 12 months only in telemoni-tored, adherent patients.15
Regular well-planned exercise training in most cases improves the QoL of HF patients. It improves their psy-chological and mental condition, they become more self-reliant and independent in the performance of daily activities, which consequently produces the sensation that the disease and disability are affecting them far less than before. Although some previous studies have shown incon-sistent or even null results regarding the improvement of QoL in HF patients after cardiac rehabilitation (hospital, outpatient and/or home-based), most research indicates a significant improvement in QoL among HF patients in their physical and mental spheres.12–20 These conflicting results may be attributed to variations in the kind of psy-chological support, age and gender of participants, differ-ent training modalities (type, intensity, duration, setting, supervision) and patients’ adherence to and acceptance of recommendations. Moreover, there are many different val-idation scales used in the literature to evaluate health-related QoL, making comparisons difficult.2
Table 1. Baseline characteristics.
SCR Group (n = 56)
HTCR Group (n = 75)
Males, n (%) 53 (95) 64 (85)Age, years, mean ± SD 60.5 ± 8.8 56.4 ± 10.9LVEF, %, mean ± SD 30.8 ± 6.7 30.2 ± 8.2Atrial fibrillation or atrial flutter, n (%) 5 (8.9) 7 (9.3)Body mass index (kg/m2), mean ± SD 26.5 ± 3.8 27.7 ± 4.3Aetiology of HF, n (%) Ischaemic 48 (85.7) 55 (73.3) Non-ischaemic 8 (14.3) 20 (26.7) Myocardial infarction 44 (78.6) 48 (64.0)Past medical history, n (%) Angioplasty 29 (51.8) 38 (50.7) Coronary artery bypass grafting 19 (33.9) 20 (26.7) Stroke 4 (7.1) 7 (9.3) Diabetes 25 (44,6) 19 (25.3) Hyperlipidaemia 43 (76.8) 49 (65.3) Current smoker/former smoker 4 (7.3)/17(30.9) 4 (5.3)/17 (22.7)Functional status NYHA II, n (%) 31 (55.4) 37 (49.3) NYHA III, n (%) 25 (44.6) 38 (50.7)Treatment, n (%) Beta-blocker 56 (100) 75 (100) Angiotensin converting enzyme inhibitors 51 (92.7) 69 (92.0) Angiotensin receptor blockers 5 (9.1) 11 (14.7) Digoxin 8 (14.5) 17 (22.7) Loop diuretics 40 (72.7) 58 (77.3) Spironolactone 51 (92.7) 72 (96.0) Aspirin 48 (85.7) 55 (73.3) Anticoagulants 16 (29.6) 28 (37.3) Statins 52 (94.5) 67 (89.3) Implantable cardioverter-defibrillator 13 (23.2) 24 (32.0)
HTCR: home-based tele-monitored cardiac rehabilitation; SCR: standard outpatient cardiac rehabilitation; SD: standard deviation; LVEF: left ven-tricular ejection fraction; HF: heart failure; NYHA: New York Heart Association class
at UQ Library on November 19, 2014cnu.sagepub.comDownloaded from

6 European Journal of Cardiovascular Nursing
The novelty of our study consisted in the introduction of different training modalities while conserving relatively homogeneous study groups. Once groups comparable in terms of demographic data, aetiology of HF and accept-ance of the proposed cardiac rehabilitation model were established, we applied the same tests to assess their QoL, but varied them in terms of some training modalities. The differentiation included variables such as type, setting, supervision and place of psychological support perfor-mance, that is: walking versus cycling, home-based versus outpatient-based, telemonitored versus direct and phone calls versus face-to-face meetings, respectively.
Despite this training differentiation, we observed a sim-ilar improvement in total QoL index, PCS and MCS in both groups. The only significant difference we found was related to the initial general health assessment. Before car-diac rehabilitation the HTCR Group assessed their general health to be better than did the SCR Group. Post-training assessment was more coherent: for both groups physical training did not result in being of significantly beneficial importance in general health. This may be due to the fact that patients were aware of the implications of chronic dis-eases, such as HF, and they learned to live with it despite disease-related limitations.
Post-training results showed that the essence and the upturn mechanism of QoL in HTCR Group were different
in detail from those observed in SCR Group. Patients in HTCR Group improved mainly in the MCS of QoL. Since they did not have to visit the hospital for check-up visits, patients might have had a feeling of psychological com-fort. Avoiding the hospital gave them an obvious and sub-jective sense of health.17,21 They possibly felt that their own influence on treatment and rehabilitation was stronger. These results, it should be stressed, could significantly improve the mental dimensions of SF-36. The positive assessment of the health condition perception by patients after completing HTCR probably helped them to function more independently and also to adapt better to restrictions in physical functioning. Their assessment of this aspect of life seemed more positive as well.
Similar results to those in the present study were reported by Jolly et al. and Oka et al. Patients in home-based rehabilitation improved in the mental component; however, in the physical aspect no improvement was noted. The authors highlighted the importance of the sup-port from the medical personnel supervising the progress in home-based rehabilitation. They also pointed to the role the feedback information played in home-based rehabilita-tion.17,21 Our study confirmed the fact that HTCR patients accepted this new model of telerehabilitation. They also found interactive collaboration with the monitoring centre of great importance.
Table 2. Comparison of outcomes before and after cardiac rehabilitation.
Subscales SCR group p1a value HTCR group p2
b value p3c value p4
d value
Before After Before After
M ± SD M ± SD
Physical function 25.39±10.89 23.20±10.71 0.0436 23.2±11.32 21.60±9.65 0.0490 NS NSRole limitation caused by physical problems
13.80±7.46 11.39±8.43 0.0342 13.07±7.96 12.74±7.17 NS NS NS
Bodily pain 2.74±2.54 2.00±2.07 0.0110 3.00±2.43 2.66±2.22 NS NS NSGeneral health 15.46±4.67 14.59±4.03 NS 13.79±3.88 13.14±3.80 NS 0.0281 <0.05Physical component summary
57.39±18.06 51.37±19.60 0.0356 52.95±17.51 50.27±17.06 0.0390 NS NS
Social function 2.22±1.98 1.63±1.54 0.0056 2.53±2.07 2.64±2.84 NS NS <0.05Mental health 7.52±4.51 5.89±3.58 0.0095 8.05±3.81 7.15±4.03 0.0123 NS NSRole limitation caused by emotional problems
5.09±6.48 4.35±6.07 NS 6.05±6.36 4.93±6.15 NS NS NS
Vitality 7.94±4.17 6.76±3.17 0.0197 8.44±3.36 7.25±3.78 0.0008 NS NSMental component summary
22.78±13.22 18.56±9.18 0.0099 25.11±12.01 21.68±12.46 0.0052 NS NS
Total quality of life index
81.6±27.3 69.2±26.4 0.0045 79.3±25.6 70.5±25.4 0.0074 NS NS
SCR: standard cardiac rehabilitation; HTCR: home-based telemonitored cardiac rehabilitation; M: mean; SD: standard deviation; NS: statistically not significant; QoL: quality of lifea p1: level of significance (comparison of QoL in outpatient-based rehabilitation group (SCR Group) before rehabilitation and after its completion, within SCR Group analysis).
bp2: level of significance (comparison of QoL in HTCR Group before rehabilitation and after its completion, within HTCR Group analysis).cp3: level of significance (comparison of QoL in groups studied before rehabilitation cycle – between groups analysis).dp4: level of significance (comparison of QoL in groups studied after rehabilitation cycle completion – between groups analysis).
at UQ Library on November 19, 2014cnu.sagepub.comDownloaded from

Piotrowicz et al. 7
Patients in SCR Group observed fewer restrictions in PF. The fact that they reported feeling less pain had various implications. First, it might have allowed them to function better within the family and professionally. Seemingly, they also found it less difficult to function socially since their physical state improved, which might have allowed them to continue working or performing other activities. Better physical efficiency is associated with positive self-assessment – especially in terms of vigour and vitality. A positive change in PF for these patients probably improved their mental welfare. Improvement in the MCS might have resulted from positive changes in terms of their physical state. Positive changes in PF, on the other hand, might have improved their general well-being. A beneficial upturn in PF of SCR Group could be associated with the constant access and contact with a physician immediately after the training and, what was even more important, with the availability of a prompt intervention in the case of a patient’s physical and/or mental state deteriorating. It is necessary to underline the fact that in this form of cardiac rehabilitation, the medical staff were focused mainly on the training parameters and improving patients’ physical capacity, which, it turn, could have led to better physical results than among HTCR patients.
Quittan et al. reported similar results. The improvement indicator concerned mainly the general feeling of health as well as physical and social functioning. The authors pointed to the importance of dyspnoea and fatigue reduc-tion, which was reflected in better QoL results.22
Similarly, Koukouvou et al. indicated a positive effect of cardiac rehabilitation in the form of physical fitness increase and improvement in general sense of condition in HF patients.23
Finally, both groups, apart from benefiting from exer-cise training and the possibility to take advantage of psy-chological assistance, received parallel support from the rehabilitation team (physician, physiotherapist, nurse). Therefore it is difficult to determine whether the improve-ment in QoL reported in both groups was exercise related or caused in part by the overall psychosocial support com-ponent of each programme. Probably, each of them some-how contributed to the QoL improvement.
Limitations
The duration of training in this study was eight weeks only. Most of the target group were male (85%), and thus the results obtained cannot be fully extrapolated to the female population. The final limitation is the lack of long-term follow-up to determine the number of patients whose QoL remained improved after each of the interventions.
Conclusion
The study demonstrated that in HF patients HTCR pro-vided an improvement in total QoL index similar to SCR.
Yet it differed in QoL subscales. Patients who underwent HTCR observed an improvement mainly in the mental cat-egories. Patients in SCR Group improved their general physical well-being. Due to limitations associated with HF, HTCR may be a viable alternative to SCR.
Implications for practice
•• New technologies can be applied in everyday medical and clinical practice.
•• We can implement (1) telerehabilitation, (2) tel-ecare and (3) psychological support in telephone conversations.
•• All of these procedures will result in an improve-ment of quality of life.
Conflict of interest
None declared.
Funding
This work was supported by the Institute of Cardiology, Warsaw, Poland (study number 2.9/I/06).
References
1. McMurray JJ, Adamopoulos S, Anker SD, et al. ESC guide-lines for the diagnosis and treatment of acute and chronic heart failure 2012: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology. Developed in collabora-tion with the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail 2012; 14: 803–869.
2. Hoekstra T, Lesman-Leegte I, van Veldhuisen DJ, et al. Quality of life is impaired similarly in heart failure patients with preserved and reduced ejection fraction. Eur J Heart Fail 2011; 13: 1013–1018.
3. Hoekstra T, Jaarsma T, van Veldhuisen DJ, et al. Quality of life and survival in patients with heart failure. Eur J Heart Fail 2013; 15: 94–102.
4. Heo S, Moser DK, Pressler SJ, et al. Dose-dependent rela-tionship of physical and depressive symptoms with health-related quality of life in patients with heart failure. Eur J Cardiovasc Nurs 2013; 12: 454–460.
5. Piepoli MF, Davos C, Francis D, et al.; ExTraMATCH Collaborative. Exercise training meta-analysis of trials in patients with chronic heart failure (ExTraMATCH). BMJ 2004; 328: 189–192.
6. Conraads VM, Deaton C, Piotrowicz E, et al. Adherence of heart failure patients to exercise: Barriers and possible solu-tions: A position statement of the Study Group on Exercise Training in Heart Failure of the HFA of the ESC. Eur J Heart Fail 2012; 14: 451–458.
7. Piepoli MF, Conraads V, Corra U, et al. Exercise training in heart failure: From theory to practice. A consensus document of the HFA and the EACPR. Eur J Heart Fail 2011; 13: 347–357.
8. Piotrowicz E, Baranowski R, Bilińska M, et al. A new model of home-based telemonitored cardiac rehabilitation
at UQ Library on November 19, 2014cnu.sagepub.comDownloaded from

8 European Journal of Cardiovascular Nursing
in patients with heart failure: Effectiveness, quality of life and adherence. Eur J Heart Fail 2010; 12: 164–171.
9. Tylka J and Piotrowicz R. SF-36 Polish version. Kardiol Pol 2009; 67: 1166–1169.
10. Tylka J. SF-36 questionnaire – final part of discussion. Kardiol Pol 2010; 68: 985.
11. Piotrowicz E. How to do: Telerehabilitation in heart failure patients. Cardiol J 2012; 19: 243–248.
12. Piotrowicz E, Jasionowska A, Banaszak-Bednarczyk M, et al. ECG telemonitoring during home-based cardiac reha-bilitation in heart failure patients. J Telemed Telecare 2012; 18: 193–197.
13. Ades PA, Pashkow FJ, Fletcher G, et al. A controlled trial of cardiac rehabilitation in the home setting using electrocar-diographic and voice transtelephonic monitoring. Am Heart J 2000; 139: 543–548.
14. Giallauria F, Lucci R, Pilerci F, et al. Efficacy of telecardi-ology in improving the results of cardiac rehabilitation after acute myocardial infarction. Monaldi Arch Chest Dis 2006; 66: 8–12.
15. Smart N, Haluska B, Jeffriess L, et al. Predictors of sus-tained response to exercise training in patients with chronic heart failure: A telemonitoring study. Am Heart J 2005; 150: 1240–1247.
16. Coats AJ, Adamopoulos S, Meyer TE, et al. Effects of physical training in chronic heart failure. Lancet 1990; 335: 63–66.
17. Oka RK, De Marco T, Haskell WL, et al. Impact of a home-based walking and resistance training program on quality of life in patients with heart failure. Am J Cardiol 2000; 85: 365–369.
18. Witham MD, Gray JM, Argo IS, et al. Effect of a seated exercise program to improve physical function and health status in frail patients ≥ 70 years of age with heart failure. Am J Cardiol 2005; 95: 1120–1124.
19. Dracup K, Evangelista LS, Hamilton MA, et al. Effects of a home-based exercise program on clinical outcomes in heart failure. Am Heart J 2007; 154: 877–883.
20. Corvera-Tindel K, Doering LV, Woo MA, et al. Effects of a home walking exercise program on functional status and symptoms in heart failure. Am Heart J 2004; 147: 339–346.
21. Jolly K, Taylor RS, Lip GYH, et al. A randomized trial of the addition of home-based exercise to specialist heart fail-ure nurse care: The Birmingham Rehabilitation Uptake Maximisation study for patients with Congestive Heart Failure (BRUM-CHF) study. Eur J Heart Fail 2009; 11: 205–213.
22. Quittan M, Strum B, Wiesinger GF, et al. Quality of life in patients with chronic heart failure: A randomized controlled trial of changes induced by a regular exercise program. Scand J Rehabil Med 1999; 31: 223–228.
23. Koukouvou G, Kouidi E, Iacovides A, et al. Quality of life, psychological and physiological changes following exercise training in patients with chronic heart failure. J Rehabil Med 2004; 36: 36–41.
at UQ Library on November 19, 2014cnu.sagepub.comDownloaded from