
Psychiatry 2 - Practicals 4 - uniba.sk · Agitation / Agression Agitation Severe anxiety associated...
31
1 PSYCHIATRIC EMERGENCIES Psychiatry 2 – Practical # 4 Author: MUDr. Peter Janík, PhD. Supervisor: doc. MUDr. Ján Pečeňák, CSc. Psychiatrická klinika LFUK a UNB, Bratislava Podporené grantom KEGA č. 099UK-4/2012
Transcript of Psychiatry 2 - Practicals 4 - uniba.sk · Agitation / Agression Agitation Severe anxiety associated...
1
PSYCHIATRIC EMERGENCIES
Psychiatry 2 – Practical # 4
Author: MUDr. Peter Janík, PhD.Supervisor: doc. MUDr. Ján Pečeňák, CSc.
Psychiatrická klinika LFUK a UNB, Bratislava
Podporené grantom KEGA č. 099UK-4/2012
DELIRIUM
2KEGA 099UK-4/2012
3
Delirium
severe global impairment of consciousness global cognitive impairment associated with behavioral abnormalities
stereotype response of brain to a variety of insults similar clinical features whatever the primary cause
rapid onset fluctuating course clinical features can vary markedly in severity at different time of the
day (typically worsening at night)
common in patients after major surgery or trauma 10-20 %
KEGA 099UK-4/2012
4
Delirium – clinical features
impaired clarity of consciousness reduced ability to direct, sustain and shift attention global impairment of cognition with disorientation,
impaired recent memory and abstract thinking nocturnal worsening of symptoms psychomotor agitation / inhibition emotional lability illusions / hallucinations (usually visual) incoherent speech paranoid delusions
KEGA 099UK-4/2012
5
Delirium – causes
Intracranial: head injury, intracerebral bleeding, encephalitis, meningitis, brain ischemia, raised intracranial pressure, tumor, dementia
Metabolic: electrolyte disturbance, hyperamonemia, uremia, anemia, cardiac failure, hypothermia, dehydratation
Endocrine: hypoglycemia, thyroid, parathyroid, pituitary, adrenal diseases
Infective: urinary tract infection, pneumonia, HIV, pancreatitis, febrile states, septicemia
Substance intoxication or withdrawal: alcohol, psychoactive substances, BZD, anticonvulsants, steroids, anticholinergic agents
Hypoxia: secondary to any cause
Trauma: head, chest, abdomen, polytrauma, burns
KEGA 099UK-4/2012
6
Delirium – causes
I I
WWAATTCCHH
DDEEAATTHH
←←
←←←←←←←←←←
←←←←←←←←←←
IInfectionnfection
WWithdrawalithdrawalAAcute metaboliccute metabolicTTraumaraumaCCNS pathologyNS pathologyHHypoxiaypoxia
DDeficiencieseficienciesEEndocrinopathiesndocrinopathiesAAcute vascularcute vascularTToxins or drugsoxins or drugsHHeavy metals eavy metals
KEGA 099UK-4/2012
7
Delirium – management
Treatment: identification and treatment of primary cause antipsychotics – pacification benzodiazepines (alcohol, PA substances, BZD withdrawal) supplementation of electrolytes, vitamins, rehydratation explanation, reorientation, reasurance
Prognosis: usually lasts less than 1 week amnesia for the period of delirium development of dementia death – 1 year mortality 50 %
KEGA 099UK-4/2012
AGITATION & AGGRESSION
KEGA 099UK-4/2012 8
Agitation / Agression
Agitation Severe anxiety associated with motor restlessness Seen in dementia, depression, anxiety disorders, withdrawal state Treatment: Benzodiazepines
Aggression Forceful, goal-directed action that can be verbal or physical; the
motor counterpart of the affect of rage, anger, or hostility. Seen in neurological deficit, temporal lobe disorder, impulse-control
disorders, mania, schizophrenia, personality disorders, intoxications Treatment: Antipsychotics, Benzodiazepines, use of restraints
9KEGA 099UK-4/2012
SUICIDALITY
KEGA 099UK-4/2012 10
11
Suicidality
one of the most common psychiatric emergency problems with mental disorder without mental disorder
suicidal ideation: thoughts about ending one's own life suicidal plan: planning of taking one's own life suicidal behavior: act of taking one's own life
KEGA 099UK-4/2012
12
Suicidality – psychiatrist's role
evaluation of actual state risk of suicidal behavior underlying mental disorder history of suicidal attempts presence of psychoactive substances social background
hospitalization or different intervention?
KEGA 099UK-4/2012
13
Suicidality – questions
How do you feel about the future?Have you ever thought that life was not worth living?Have you ever wished you could go to bed and not to wake up in the morning?Have you had thoughts of ending your life?Have you thought about how would you do it?Have you made any preparations?Have you tried to take your own life in the past?
KEGA 099UK-4/2012
14
Suicidality – risk factors
male gender age > 45 years unmarried suicidal attempt in history signs of chronic automutilation bad health condition actual or risk of loss in family / job insufficient social background suicidal plan
after the attempt: persistent wishes to be dead deadliness of chosen method elimination of lifesaving chance regret of lifesaving
KEGA 099UK-4/2012
15
Suicidality – underlying diagnoses
acute stress disorder anxiety disorder affective disorder
unipolar depression bipolar depression
schizophrenia schizoaffective disorder intoxication, withdrawal (psychoactive substances) personality disorders (borderline)
KEGA 099UK-4/2012
16
Suicidality – management
treatment of basic mental disorder (if present) psychotherapy (crisis intervention) psychosocial intervention psychopharmacotherapy
benzodiazepines antipsychotics
KEGA 099UK-4/2012
CATATONIA
KEGA 099UK-4/2012 17
18
Catatonia – causes
Psychiatric: schizophrenia, mood disorders – severe mania or depression,
neuroleptic malignant syndrome
Delirium: metabolic, endocrine, infectious, autoimmune disorders, drug-
related
Neurologic: Parkinsonism, postencephalitic states, seizure disorder, lesions of
thalamus, parietal and frontal lobe
KEGA 099UK-4/2012
19
Catatonia – symptoms & signs
increased resting muscle tone which is not present on active or passive movement
motor symptom of schizophrenia
Typical signs: mutism posturing negativism staring rigidity echopraxia/echolalia vaxy flexibility
KEGA 099UK-4/2012
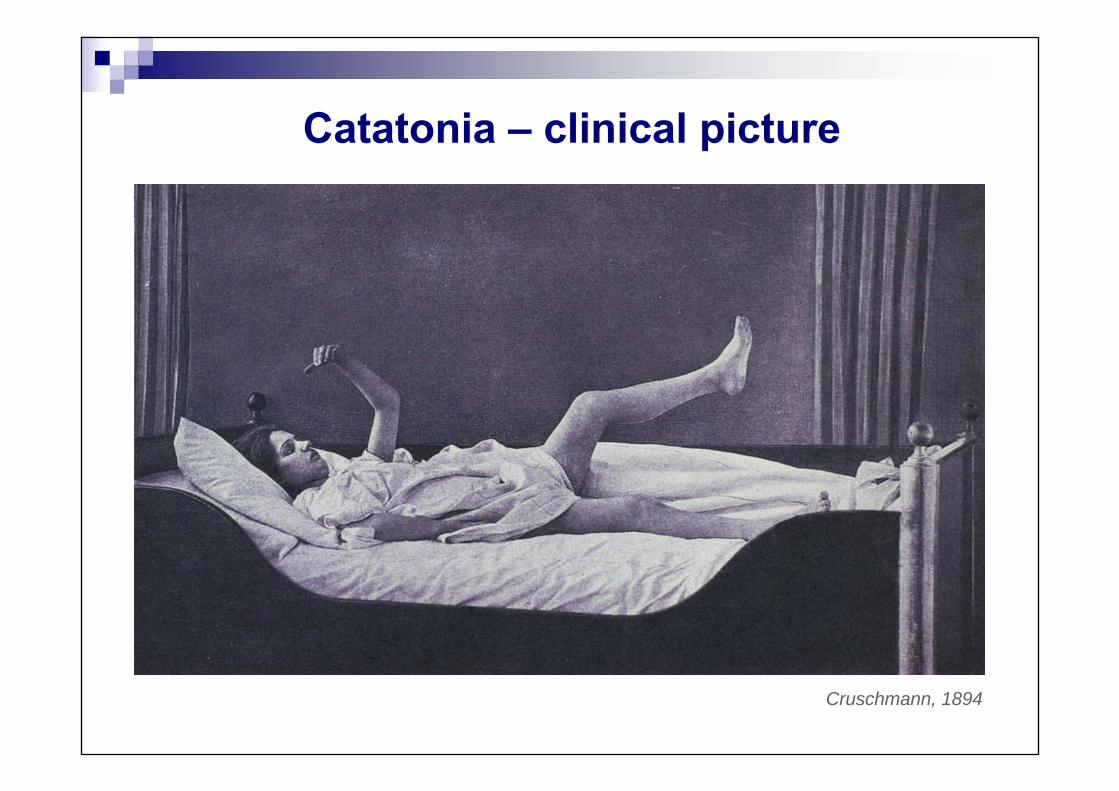
Catatonia – clinical picture
Cruschmann, 1894
21
Catatonia – management
symptomatic treatment benzodiazepines electroconvulsive therapy
KEGA 099UK-4/2012
SEROTONINE SYNDROME
KEGA 099UK-4/2012 22
23KEGA 099UK-4/2012
Serotonine syndrome (SS)
rare, but potentially fatal syndrome occurs in the context of initiation or dose increase of serotonergic
agents result of overdose or drug combinations (MAOI, lithium) rapid onset, if treated usually resolved in 24-36 hours
Pathophysiology: ↑ production of serotonin due to ↑ availability of precursors ↓ metabolism of serotonin ↑ release of stored serotonin reuptake inhibition direct stimulation of serotonin receptors
24KEGA 099UK-4/2012
SS – symptoms & signs
confusion agitation hypersalivation, sweating myoclonus, rigidity, tremor, hyperreflexia, ataxia hyperthermia nausea, diarrhea mydriasis tachycardia hyper/hypotension
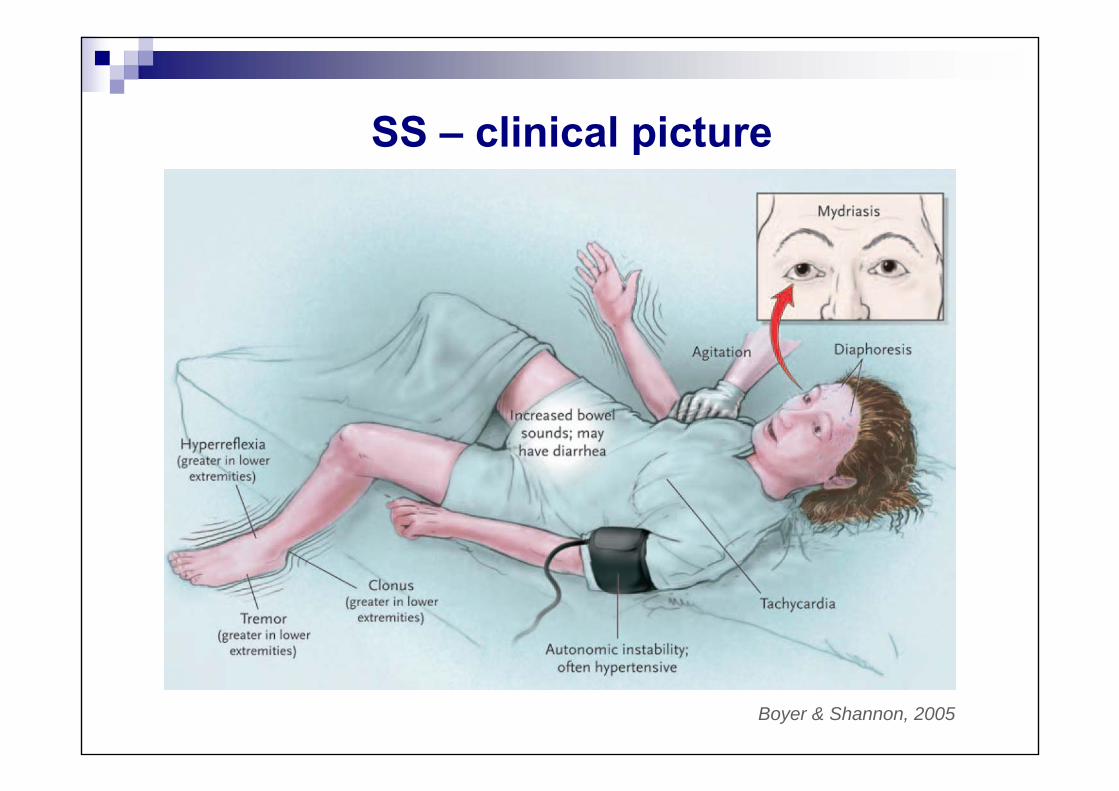
SS – clinical picture
Boyer & Shannon, 2005
26KEGA 099UK-4/2012
SS – management
if overdose – gastric lavage, activated charcoal rehydratation, cooled i.v. infusions antipyretics sodium bicarbonate – to prevent renal failure benzodiazepines – agitation, seizures, rigidity beta-blockers – to prevent dysrhytmia
NEUROLEPTIC MALIGNANTSYNDROME
KEGA 099UK-4/2012 27
28KEGA 099UK-4/2012
Neuroleptic malignant syndrome (NMS)
rare life-threatening idiosyncratic reaction to antipsychotic medication (usually typical AP) – incidence 0,07-0,2 %
mostly in first 4 weeks of treatment
D2 receptors blockade or ↓Dopamine availability in striatum (rigidity), hypothalamus (thermoregulation) → impaired Ca2+ →mobilization in muscle cells → rigidity
mortality: 5-20% respiratory failure renal failure cardiovascular collapse arrhythmias DIC
29KEGA 099UK-4/2012
NMS – symptoms & signs
hyperthermia > 38°C muscular rigidity agitation altered level of consciousness tachycardia, tachypnoe tremor hypo/hypertension ↑CK / urinary myoglobin, leukocytosis, metabolic acidosis incontinence/retention/obstruction
30KEGA 099UK-4/2012
NMS – management
ECT Dantrolen 1-2 mg/kg Amantadin, Bromocryptin
stop of taking antipsychotics benzodiazepines
rehydratation antipyretics sodium bicarbonate
31
Any questions?










