Mania & ADHD
47
Mania and ADHD What should you know? Why should you care? Gabrielle A. Carlson, MD Professor of Psychiatry and Pediatrics Director, Child and Adolescent Psychiatry Stony Brook University School of Medicine Stony Brook, New York 631-632-8840
-
Upload
babarsaggu -
Category
Documents
-
view
226 -
download
0
Transcript of Mania & ADHD

8/13/2019 Mania & ADHD
http://slidepdf.com/reader/full/mania-adhd 1/47
Mania and ADHD What should you know?
Why should you care?
Gabrielle A. Carlson, MDProfessor of Psychiatry and Pediatrics
Director, Child and Adolescent PsychiatryStony Brook University School of Medicine
Stony Brook, New York
631-632-8840

8/13/2019 Mania & ADHD
http://slidepdf.com/reader/full/mania-adhd 2/47
What ADHD is
• ADHD is a heterogeneous, clinical condition
• If appropriately defined (with symptoms,pervasiveness and impairment) it may constitute
a difference of degree and possibly kind from“normal”
• “Deficit” does not mean “None”. It means thatattention cannot be sustained when the child or
adult is not interested.

8/13/2019 Mania & ADHD
http://slidepdf.com/reader/full/mania-adhd 3/47
H-I-D-E (ADHD)Developmentally inappropriate levels of:
Hyperactivity (6/9 sx): fidgets with hands or feet or squirms in seat;
leaves seat in classroom inappropriately; runs about or climbs
excessively; has difficulty playing quietly; is “on the go” or “driven by a
motor”; talks excessively
Impulsivity: blurts out answers before questions are completed; has
difficulty awaiting turn; interrupts or intrudes on others
Distractibility (6/9 sx): fails to give close attention to details; difficulty
sustaining attention; does not seem to listen; does not follow through on
instructions; difficulty organizing tasks or activities; avoids tasks
requiring sustained mental effort; loses things necessary for tasks;
easily distracted; forgetful in daily activities
Emotionality (associated symptom): Low frustration tolerance; sensitive
to criticism; over-reactive

8/13/2019 Mania & ADHD
http://slidepdf.com/reader/full/mania-adhd 4/47
Differentiation from ―normal‖
REMEMBER THE 3 Ps:
• Condition is PERSISTANT. It has gone on
for at least 6 months
• It is PERVASIVE. More than one personobserves it- present in different settings
• It is imPAIRING: interfering with child’s
functioning at home, with peers, with
family, and/oror with his/her self- esteem or
development.

8/13/2019 Mania & ADHD
http://slidepdf.com/reader/full/mania-adhd 5/47
“Hyperkinetic Child Syndrome”-Laufer and Denhoff, 1957
SYMPTOM DESCRIPTOR DSM IV
ADHD
Hyperactivity Involuntary and constant overactivity that greatly
surpasses normal
YES
Poor
Concentration
Frequent shifting from one activity to another YES
Variability Behavior is unpredictable. "Sometimes he is good,
sometimes bad"
NO
Irritability/
Explosiveness
Fits of anger easily provoked ; reactions almost
volcanic in intensity
NO
Impulsiveness Does things on the spur of the moment. Cannot delaygratification YES
Sleep
disturbance
Falls asleep at proper time but wakens after only a few
hours "rampaging through the house in hyperactive,
noisy, sleep-disturbing play"
NO
G. Carlson, 2009

8/13/2019 Mania & ADHD
http://slidepdf.com/reader/full/mania-adhd 6/47
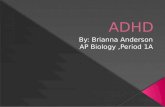
OppositionalOppositional
Defiant DisorderDefiant Disorder
ADHD aloneADHD alone
TicTic
DisDis..
ConductConduct
DisorderDisorderAnxietyAnxiety
DisorderDisorder
MoodMood
DisDis..
31%
4%14%
40%
34%
11%
Co-Occurring Disorders in MTA Children
(n=579)

8/13/2019 Mania & ADHD
http://slidepdf.com/reader/full/mania-adhd 7/47
—Age—
Inattentio
n
Course of the Disorder
Though less than in childhood, it is stillgreater than In non-ADHD peers; verbal
> physical
Less than in childhood;
more often verbal and
cognitive than non-AADHDsame age peers

8/13/2019 Mania & ADHD
http://slidepdf.com/reader/full/mania-adhd 8/47
Outcome of ADHD
"Developmental Delay" - about 30% outgrow the disorder by youngadulthood (symptoms minimal; Ability to compensate)* milder disorder
"Continual Display" - about 40% remain symptomatic with functional
impairment
*Worse hyperactivity/inattention---> poor academics
"Developmental Decay" - development of more serious antisocial and/or
substance use disorders
* Irritable temperament----> AGGRESSION
* Worse executive function-------> WORSE IMPULSIVITY
* Worse social adjustment----> WORSE PEERS
* More family psychopathology---> higher gene load + Less
involvement and poorer communication; high level of
fighting/domestic violence; poor supervision and monitoring.

8/13/2019 Mania & ADHD
http://slidepdf.com/reader/full/mania-adhd 9/47
Ways to compare treatment
• Statistical significance p<0.05
• Effect size
– 0.8 or higher is strong
– 0.4-.7 is modest
– 0<.4 isn’t very helpful especially if the problem
is severe
• NNT (number needed to treat) and NNH(number needed to harm
– NNT should be low; NNH should be high

8/13/2019 Mania & ADHD
http://slidepdf.com/reader/full/mania-adhd 10/47
Meta-analysis of 29 controlled studies over 25 years,encompassing 4465 children, adolescents)
with some added information
Drug Effect Size
Amphetamine 0.92
Methylphenidate 0.80
Atomoxetine 0.73
Guanfacine ER 0.73
Clonidine 0.58*
Modafinil 0.49
Bupropion 0.32
Diet without additives 0.2
Faraone SV, Spencer TJ: Presented at: American Psychiatric Association Annual Meeting, Toronto,Canada, May 2006. * Connor et al., JAACAP, 1999
(

8/13/2019 Mania & ADHD
http://slidepdf.com/reader/full/mania-adhd 11/47
Effect of severity on ADHD
Mild Moderate Severe
When obvious Elementaryschool
preschool Age <3
Where it
manifests
Unstimulating
situations;homework time
School -class and
playground;Home-except computer
Everywhere
and anywhere
Untreatedoutcome
Worsens insecondaryschool
underachievement
Disorganization anddefiance; worse insecondary school
underachievement
aggression;peer problems;drugs,
underachievement
comorbidity Oftenuncomplicated
LD, ODD,anxiety,depression
LD, ODD/CD,other disorders

8/13/2019 Mania & ADHD
http://slidepdf.com/reader/full/mania-adhd 12/47
ADHD severity and treatment
Mild Moderate Severe
Educational
interventions
Structure
PRN tutoring
accommodations
Classification; ?
Regular class
SEDclassroom;sometimeshospitalization
Home
intervention
Structure;
behavior mod PRN
Behavior modification
needed
Behavior mod
Social andmental healthrx
medication If above strategiesfail and child slips
academically andbehaviorally
During school and forhomework; +/-
elsewhere dependingon impairment
Many medicationtrials; often
combinedmedications
Therapygoals
Psychoeducation
Organizational
skills; selfesteem help
Psychoeducation
Organizationalskills; self esteem
help
Aggression,anger control
Mood
stabilization

8/13/2019 Mania & ADHD
http://slidepdf.com/reader/full/mania-adhd 13/47
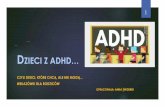
MTA: % ―Normalized‖ at 14 Months
Comb = medical management + behavioral treatment; MedMgt = medical management;
Beh = behavioral treatment; CC = community comparison group
Jensen PS, et al. J Dev Behav Pediatr. 2001;22:60-73.
88%
68%
56%
34%
25%
0%
20%
40%
60%
80%
100%
Controls Comb MedMgt Beh CC

8/13/2019 Mania & ADHD
http://slidepdf.com/reader/full/mania-adhd 14/47
=
?
Manic depression or rages?

8/13/2019 Mania & ADHD
http://slidepdf.com/reader/full/mania-adhd 15/47
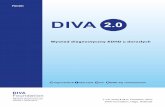
For office-based visits with a mental disorder, rates went
from .42% (n=25) in 1994 to 6.7% (n=1003)
Increase in BP
Diagnosis in youth
from nationallyrepresentative
outpatient office
visits(Moreno et al., 2007)
% of all

8/13/2019 Mania & ADHD
http://slidepdf.com/reader/full/mania-adhd 16/47
Remember these acronyms
• Mania: H*I*P*E*R*S
– Hyperactivity (goal directed), Irritability,Psychosis (grandios i ty ), E lated/expansive
mood, Rapid speech/Racing thoughts, Sleep
(doesn’t need it or want it)
• Depression: D*U*M*P*S – Definite personality change, Undeniable drop in
grades, Morbid/suidical, Pessimistic, Somatic
• Illness, drugs mania, called 2o
• Superimposed on other conditions
• Symptoms occur concurrently in episodeslasting at least a week for mania and 2 weeks
for depression.

8/13/2019 Mania & ADHD
http://slidepdf.com/reader/full/mania-adhd 17/47
ADHD and Mania: Overlapping symptoms
Carlson & Meyer, ADHD with Mood Disorders, In Brown TE, ADHD Comorbidities: Handbook for ADHD Complicationsin Children and Adults, 2009

8/13/2019 Mania & ADHD
http://slidepdf.com/reader/full/mania-adhd 18/47
GCarlson, MD
Case #1 Classic Bipolar I Disorder
• Nicola -14+ years old; shy, nice , no behavior problems or
substance abuse• Age 10, brief depressive episode after Grandma’s death; treated
with psychotherapy; increased anxiety related to school
demands in middle school.
• Several weeks before referral- parents said Nicola’s personality
had changed-
– wearing sexy clothes, talking to complete strangers, meeting boys
on internet chat rooms; up all night; vulgar language.
– Mood changes throughout the day from laughing hysterically, to
being irritable, swearing and smashing things to becoming tearful
and crying uncontrollably.
– Sleep patterns had changed; up late talking in chat rooms, sleep
for a few hours but would wake early and rearrange room, waking
the neighbours by using the vacuum cleaner at 6 am.

8/13/2019 Mania & ADHD
http://slidepdf.com/reader/full/mania-adhd 19/47
GCarlson, MD
Nicola continued
• Mental status: Nicola loud, intrusive, talked fast and
laughed loudly. Hard to follow her train of thought-she rapidly changed the subject to seeminglyunrelated topics.
• Convinced a TV actor whom she had been trying tocontact, would call her and she’d have a relationship
with him. She used her cell phone to try to call him.
• Became suspicious and hostile when asked aboutdrug use which she adamantly denied; She wouldnot allow the interviewer to see her parents alone,
likewise, didn’t want to be interviewed alone.
• She expressed a fear that her food may have beenpoisoned and that her brain had been damaged.

8/13/2019 Mania & ADHD
http://slidepdf.com/reader/full/mania-adhd 20/47
Steve
• 8 year old, 3rd grade boy in regular educationwith explosive outbursts (throws chairs,sweeps stuff off of desks, attacks staff) – Short fuse, irritable and easily annoyed
• Chronically hyperactive and impulsive athome and school
• Symptoms evident in preschool – had SEITwho did good behavioral treatment at homeand school. No episodes.
• IQ and achievement testing normal.• Steve said what makes him mad: “when my
mom tells me to do stuff I don’t want to do;too much work in school [which is too hard]; Ineed help and the teacher said “wait”.

8/13/2019 Mania & ADHD
http://slidepdf.com/reader/full/mania-adhd 21/47
Steve’s treatment history
• Began ADHD medication in 1st
grade• takes Adderall XR 20 mg; in play therapy
• Depakote and Trileptal haven’t helped his mood
or aggression
• Behavior modification started in preschool wasn’t
continued at school or at home
• Problems at home included lack of consistency
between parents (divorced) and aunt (partial care
taker)
• Mom depressed; dad had anger managementproblems

8/13/2019 Mania & ADHD
http://slidepdf.com/reader/full/mania-adhd 22/47
SEVERE MOOD DYSREGULATION (SMD)-Leibenluft et al., 2003
• Abnormal mood (anger or sadness) : most dayssevere enough to be noticeable by parents,teachers, or peers
• Markedly increased reactivity to negative
emotional stimuli. at least three times/ week forthe past 4 weeks.
• Hyperarousal (ADHD sx): Insomnia; Physicalrestlessness; Distractibility; racing thoughts or
flight of ideas; pressured speech;intrusiveness• Onset under age 12
• Bottom Line: SMD encompasses severe ADHD+ODD

8/13/2019 Mania & ADHD
http://slidepdf.com/reader/full/mania-adhd 23/47
Temper Dysregulation Disorder with
Dysphoria
SMD TDDDVery severe outbursts with
trivial triggers; >3 Xs/week
X X
―Hyperarousal‖ (ADHD/Anx sx) X
Persistently negative mood
between outbursts
X X
Outbursts and/or negative
mood in at least 2 settings
X X
At least 12 months; onset in
childhood
age 12 age 10
Not just in current mania, MDD,
dysthymia or psychosis
X X
R l ti t f ADHD SMD d BP i th

8/13/2019 Mania & ADHD
http://slidepdf.com/reader/full/mania-adhd 24/47
Relative rates of ADHD, SMD and BP in thepopulation
0
1
2
3
4
5
6
A n x i e t y
C o n d u c t
O D D A D H D
D e p . D i s o r d e r
B P S M D C B C L a t t
C B C L J B P
%
Costello et al. AGP 1996, N=1,015 youth; 9, 11, 13 yearsSMD= Severe Mood
DysregulationBrotman et al. Bio Psych 2006, N=1,420 youth; 9, 11, 13 years
Hudziak et al., Bio Psych 2005

8/13/2019 Mania & ADHD
http://slidepdf.com/reader/full/mania-adhd 25/47
GCarlson, MD
n=614,
P < .00001
8.3%26.5%Affective disorders
n=505, n.s.20.4%20.6%Non-affective disorder
n=350, n.s.7.5%8.5%Unipolar depression
n=795,
P < .0005
0%5.4%Bipolar disorder
n=973,
P < .00001
29%52%Any mental disorder
Children of
parents without
BP
Children of
parents with
BP
Offspring diagnosis
Psychopathology in Offspring of Parents withBipolar Illness-metaanalysis
Lapalme et al., Canadian Journal of Psychiatry 42:623-31, 1997Lapalme, Hodgins, & LaRoche (1997).
Significance

8/13/2019 Mania & ADHD
http://slidepdf.com/reader/full/mania-adhd 26/47
2 types of families
• Parents with complex mood and behavior
problems have offspring who carry similar
diagnoses; that appears to be different from
classic manic depression.
• Offspring of classic manic depressives
(e.g.Amish; parents who are lithium
responsive) still have a greater chance of
developing bipolar disorder but their courseis more benign.
1. Faraone SV, et al. Am J Med Genet. 1998;81(1):108-116. 2. Meyer S, et al. In press. 3. Duffy A, et al. Am J Psychiatry. 1998;155(3):431-433. 4. Grof P. J Clin Psychiatry. 2003;64(suppl 5):53-61.

8/13/2019 Mania & ADHD
http://slidepdf.com/reader/full/mania-adhd 27/47
How does treatment of kids with rages stack up
0
10
20
30
40
50
60
70
ADHD Anx/Dep SMD Bipolar LD
% dx'ed% Rxed
therapy
Bottom line: Many kids referred for treatment; many fewer get the
right treatment

8/13/2019 Mania & ADHD
http://slidepdf.com/reader/full/mania-adhd 28/47
GCarlson, MD
Do kids with rages/SMD develop manicdepression as adults
• Classic manic depression is not a significant
outcome in long term follow up studies of childrenwith ―hyperactivity‖/ADHD (Klein, 1999)
• Manic depression is not an outcome of children withsevere aggression – though these children docontinue to have higher rates of aggression thanother peopel;
• 3 y.o.s who are identified as impulsive, negativisticand distractible become unreliable, antagonistic and
over-reactive adults (Caspi et al., 2003)
• Boys (age 8) with severe temper tantrumsimpulsive, moody, irritable, overly dramatic adults
with poor job and marital histories (Caspi et al., 1990)

8/13/2019 Mania & ADHD
http://slidepdf.com/reader/full/mania-adhd 29/47
Bottom line with Steve
• Lots of things going on• Although he was prescribed Adderall XR 20 mg, it
wasn’t working very well; needed much closermonitoring
• Lots of stress and inconsistency at home-neededbehavioral program not play therapy
• Though he was smart enough, he needed moreattention in school and a smaller class with a BIP
• If that isn’t enough, it is worth adding an atypicalantipsychotic
• He has ADHD and ODD; one could say he has “severemood dysregulation” or TDDD; some might call him“bipolar” but it is unlikely he will develop adult manicdepression; he is at high risk for drug abuse, drop out,and depression

8/13/2019 Mania & ADHD
http://slidepdf.com/reader/full/mania-adhd 30/47
How ADHD and BP are similar
• They are both chronic disorders
• They are both highly heritable
• Both require medication and psychosocial
treatment• Both often have academic impairments
• Comorbidities may be similar (e.g. anxiety
disorders, oppositional defiant disorder
and substance abuse)
• Substance abuse is a complication of both

8/13/2019 Mania & ADHD
http://slidepdf.com/reader/full/mania-adhd 31/47
How are they different?
• ADHD is not episodic (though it does fluctuatedepending on child’s interest or level of structure) andis developmental
• Key mood symptoms are absent (elation andgrandiosity, though these can be misidentified easily if
you really want the child to have bipolar disorder)• Rates of BP in offspring are higher in families with BP;
ADHD rates may be high in both if parents havecomorbid BP + externalizing disorder
• Some outcomes may be similar (e.g. substance abuse)but long term studies of children with ADHD do not findrates of BP I, at least classically defined.
• Primary medication treatment is different

8/13/2019 Mania & ADHD
http://slidepdf.com/reader/full/mania-adhd 32/47
Why does it matter if there is a
diagnostic mistake?
• Parents feel they have a solution prematurely
• Clinicians don’t look for other conditions thatneed to be identified; and the differential
diagnosis is much broader than ADHD butthat is the easiest to discuss
• Everyone assumes there will be a connectionto bipolar disorder in adulthood
• Or that medications for bipolar disorder willclean things up nice.

8/13/2019 Mania & ADHD
http://slidepdf.com/reader/full/mania-adhd 33/47
Why does it matter if there is a diagnostic
mistake
• ADHD-do you use ADHD meds instead of? In additionto? Not at all?
• PDDspectrum - What kind of educational interventionwill be necessary because of language and social
issues?• Psychosis NOS-Will this be stable quirkiness,
schizophrenia prodrome, or mood disorder prodrome
• “Organic brain syndrome” - are there neurological
“tests” that will be needed • Traumatized child-is there past or current abuse that
needs dealing with?
For all conditions, how does the prognosis change?

8/13/2019 Mania & ADHD
http://slidepdf.com/reader/full/mania-adhd 34/47
When a parent describes mania in the child
The teacher sees
• moderate to severe
executive function
problems-66%
• ADHD -56%
• manic sx-36%
• PDD spectrum-26%
• ODD-25%
What the child has:
• ADHD-56%
• ODD 35%
• PDD spectrum 33%• severe anxiety 20%
including PTSD
• bipolar disorder 18%

8/13/2019 Mania & ADHD
http://slidepdf.com/reader/full/mania-adhd 35/47
Status of Double Blind, Placebo Controlled trialsand FDA approval of drugs for acute mania
Drug Age >18 Age <18lithium + Approved in teens
divalproex + FDA required study (-);another study (+)
olanzapine + Approved down to age 13
carbamazepine ER + Being studiedrisperidone + Approved to age 10
quetiapine + Approved to age 10
ziprasidone + positive
aripiprazole + Approved to age 10topiramate negative negative
oxcarbazepine Not studied negative
lamotrigine For deprecurrence
Being studied

8/13/2019 Mania & ADHD
http://slidepdf.com/reader/full/mania-adhd 36/47
Lamotrigine for Bipolar Students(LAMBS)
• Lamotrigine is a medication approved for adults
and is being tested in youth for stabilizing
symptoms of bipolar mania and depression
• We are doing a free treatment trial. If you have achild between the ages of 10-17 who is being
treated but isn’t completely better and still has
symptoms of mania (HIPERS)
• call Greg Carlson at 632-8828

8/13/2019 Mania & ADHD
http://slidepdf.com/reader/full/mania-adhd 37/47
Effect size of drugs in acute mania andaggression
Children and teens adults
mania aggression mania
Lithium .31 .5
Divalproex .28 .23 to .62 Atypicals Zip .48 to
Ris .81Ris .9 Ari .36 to
Ris .71
Haloperidol .8 but many AEs
Thioridizine .35Stimulants .78
atomoxetine .18
a
agonists .5

8/13/2019 Mania & ADHD
http://slidepdf.com/reader/full/mania-adhd 38/47
NNH
child adult
sleepy Wt
gain
akath
eps
sleepy Wt
gain
akath
eps
SGAs 4.6 7.0 30.39.8
7.1 84 11.98.0
Lithium n/a n/a n/a 90.1
ns
33.3
ns
A-Cs 19.1 ns n/a n/a 8.7 16.7 n/a

8/13/2019 Mania & ADHD
http://slidepdf.com/reader/full/mania-adhd 39/47
Treatment implications
Mania/BP MDD PDD abuse aggression ADHD
Lithium X X
Depakote X X X
Antipsychotics X X X
antidepressants X X X
ADHD meds X X X
Specific I.E.P. ? X
Language rx X If comorbid
psychotherapy FFTpsychoed
CBT Soc
skills
CBTtherapy
Beh mod Beh
mod
CPS X

8/13/2019 Mania & ADHD
http://slidepdf.com/reader/full/mania-adhd 40/47
Treatment approach for most children with―temper dysregulation‖
• Good diagnostic assessment – It matters if ADHD or anxiety or PDD or
learning disability or something else is
underlying the rages• Maximize the treatment of the base
condition – If symptoms remain, add another
medication – AAP, CAP or mood stabilizer
• Keep careful records of frequency,
intensity, number and duration of outbursts

8/13/2019 Mania & ADHD
http://slidepdf.com/reader/full/mania-adhd 41/47
TREATMENT IMPLICATIONS OF SEVEREMOOD DYSREGULATION/TDDD
Executive function Mood regulation Language Social
Medication management
ADHD treatment
Anti-aggressive/anti
Psychotic medications“mood stabilizers”
Understand “triggers”
Keep situation CALM
• Educate family members
• Figure out child’s deficits
•
Get evaluation-psych testingand language testing often useful
• if parent has a psychiatric
disorder, get it treated!
Psychological and
Psychoeducational

8/13/2019 Mania & ADHD
http://slidepdf.com/reader/full/mania-adhd 42/47
Incidence of Acute PsychiatricHospitalization Increased Markedly
Overall Change,1996-2003
1996-1997 1998-1999 2000-2001 2002-2003 Discharges LOS
Children
Discharges per 10,000 persons ...
Length of Stay (Mean)...............
16.03
12.15
20.86
12.67
20.24
12.71
26.06
11.11
62.62% -8.56%
Adolescents
Discharges per 10,000 persons...
Length of Stay (Mean)...............
58.97
8.18
67.65
7.52
85.97
7.25
83.33
7.14
41.31% -12.66%
Adults
Discharges per 10,000 persons ...
Length of Stay (Mean)...............
112.90
8.11
109.62
7.34
118.94
7.17
129.63
7.11
14.82% -12.28%

8/13/2019 Mania & ADHD
http://slidepdf.com/reader/full/mania-adhd 43/47
Children
0
5
10
15
20
25
1996-7 1998-9 2000-1 2002-3
P
e r 1 0 , 0
0 0
p e r s o n s
Conduct Bipolar Depression Psychosis Anxiety Developmental
1996-7 2002-3 % Change
Bipolar: 4.26 per 10,000 11.70 per 10,000 +174%
Conduct Problems: 4.50 per 10,000 4.51 per 10,000 +2%
Developmental: 0.49 per 10,000 1.19 per 10,000 +146%
HOSPITAL DISCHARGES 1996-2003
BIPOLAR
DX

8/13/2019 Mania & ADHD
http://slidepdf.com/reader/full/mania-adhd 44/47
• N = 29• Mean age; was 9.2 (2.1) years, 87% were male, 68%
white. Mean LOS 36.8 +22 days.
• 72% special education• 97% of parents described major explosive
outbursts occurring several times a week• 61% of parents said daily for at least a year.• Outbursts lasted up to 30 minutes, and over an
hour in 35% of cases. • Outbursts consisted of threats, insults, throwing
things, property destruction, and physicalaggression.
DO CHILDREN WITH RAGESHAVE BIPOLAR DISORDER
OR ―TEMPER DYSREGULATION‖

8/13/2019 Mania & ADHD
http://slidepdf.com/reader/full/mania-adhd 45/47
BE observation % of TDDD
sample
Irritability 51.7% n/a
Explosiveness 51.7% n/a
Temper Dysregulation
Disorder (TDDD)
31% n/a
% manic symptoms from
CMRS-P (Score >20)
51.7% 55.6%
emotional lability 52.4% 100%
TEMPER DYSREGULATION WITH
DYSPHORIA ON A CHILDREN’S
INPATIENT UNIT
TEMPER DYSREGULATION WITH DYSPHORIA

8/13/2019 Mania & ADHD
http://slidepdf.com/reader/full/mania-adhd 46/47
BE diagnosis
N=29
% of TDDD
sample ODD 61.9% 88.9%
ADHD 76.2% 88.9%
Comorbid ADHD and ODD:
Neither ADHD nor ODD 6.9% 0 ADHD without ODD 31.0% 11.1%
ODD without ADHD 6.9% 11.1
Both ADHD and ODD 55.2% 77.8%
PDD 20.7% 33.3% Anxiety disorder 41.4% 22.2%
Major depressive episode 13.8% 0
Manic episode 6.9% 0
% language disorder 62.1% 77.8%
TEMPER DYSREGULATION WITH DYSPHORIA
ON A CHILDREN’S INPATIENT UNIT

8/13/2019 Mania & ADHD
http://slidepdf.com/reader/full/mania-adhd 47/47
CONCLUSION SO FAR
• If you attribute the rages that promptadmission to acute mania, you should seesymptoms of mania during hospitalization
• Such symptoms were rarely seen
• However, of the 97% of children whoseparents described what may be called“temper dysregulation disorder withdysphoria” – Only 1/3 continued to have those
symptoms while hospitalized• What is YOUR experience?