Grup B7 Tutor 4 Blok 16
34
Scenario D block 16 Group B7 Tutor: dr Ramli Medical Faculty Sriwijaya University
-
Upload
rezkyoktariantisyahputri -
Category
Documents
-
view
222 -
download
0
Transcript of Grup B7 Tutor 4 Blok 16
8/8/2019 Grup B7 Tutor 4 Blok 16
http://slidepdf.com/reader/full/grup-b7-tutor-4-blok-16 1/34
Scenario D block 16
Group B7
Tutor: dr Ramli
Medical FacultySriwijaya University
8/8/2019 Grup B7 Tutor 4 Blok 16
http://slidepdf.com/reader/full/grup-b7-tutor-4-blok-16 2/34
Feb 5th 2010 B7 tutorial 4 2
Group Members Erisca Ayu Utami 54071001042
Zikrina Istifarani 54071001060
Magista Febra N 54071001062
Annisa Mulyandini 54071001079 Rendi ER Pratama 54071001081
Tinton Ardiyan 54071001092
Febi Stevi A 54071001093
Mohammad Shahir 54071001104
Rashidah bt M Jalil 54071001113 Azri M F 54071001116
Nor Azlan 54071001117
8/8/2019 Grup B7 Tutor 4 Blok 16
http://slidepdf.com/reader/full/grup-b7-tutor-4-blok-16 3/34
Feb 5th 2010 B7 tutorial 4 3
ScenarioMr No 53 years old was brought by his wife to a clinic with the main complaintthat her husband always repeating certain work unawarely. Whenever someoneremind him, he always answered that he did it just once. For example, locking the house door,. In every night he always locked the same door for severaltimes. This condition had already been happened around 7 months ago and
becoming proggresively worse week by week.Mr No is a senior official of a private company for 4 years and he wasgraduated from a famous National University. Although this condition hasalready happened with him but in activity of daily living such as leading themeeting, managing family financial, he was still normal except sometimes hecould not express some words orally. This condition happened in the last 1month.
Physical examination was normal. GCS was 15. Neurological examinationshowed no deficit in hard neurological function. Mental health was normal. CTscanning of the head was normal. MMSE score was 22.
Additional information: 4 years ago he got traffic accident and hospitalized for3 days.
8/8/2019 Grup B7 Tutor 4 Blok 16
http://slidepdf.com/reader/full/grup-b7-tutor-4-blok-16 4/34
Feb 5th 2010 B7 tutorial 4 4
Term Clarification
Repeating certain work unawarely
Proggresively worse
Could not express some words orally GCS
Hard neurological function
MMSE
8/8/2019 Grup B7 Tutor 4 Blok 16
http://slidepdf.com/reader/full/grup-b7-tutor-4-blok-16 5/34
Feb 5th 2010 B7 tutorial 4 5
Problem Identification1. Mr No 53 years old was brought by his wife to a clinic with the
main complain that her husband always repeating certain work unawarely.
2.
This condition had aready been happened around 7 month agoand progressively worse.
3. His activity of daily living is normal but sometime he could notexpress some word orally in the last 1 month.
4. His GSC was 15
5. Neurological examination showed no deficit in hard
neurological function6. His MMSE score was 227. He got traffic accident 4 years ago and hospitalized for 3 days
8/8/2019 Grup B7 Tutor 4 Blok 16
http://slidepdf.com/reader/full/grup-b7-tutor-4-blok-16 6/34
Feb 5th 2010 B7 tutorial 4 6
Problem Analysis1. What are cause and mechanisme of repeating certain work unwarily?
2. What are the correlation, between age and gender with his condition?
3. How his condition become progressively worse?4. What is the correlation between his activity and his condition?
5. What is the correlation between normal activities and his condition?6. What is the cause and mechanisme of could not express word orally?
7. What is interpretation of examination
8. What is correlation of abnormal result with his condition?
9. What is correlation between he got trafict accident 4 years ago with hiscondition now?
10. Differential diagnosis in this case?11. How to diagnose?
12. Management?13. Prognosis?
14. Complication?15. GP competency.
8/8/2019 Grup B7 Tutor 4 Blok 16
http://slidepdf.com/reader/full/grup-b7-tutor-4-blok-16 7/34
Feb 5th 2010 B7 tutorial 4 7
Hypothesis
Mr No, 53 years old man, suffered from minimalcognitive impairment & proggresively became a
mild dementia
8/8/2019 Grup B7 Tutor 4 Blok 16
http://slidepdf.com/reader/full/grup-b7-tutor-4-blok-16 8/34
Feb 5th 2010 B7 tutorial 4 8
Synthesis
8/8/2019 Grup B7 Tutor 4 Blok 16
http://slidepdf.com/reader/full/grup-b7-tutor-4-blok-16 9/34
Feb 5th 2010 B7 tutorial 4 9
Anatomy & Physiology of
Neurobehaviour 4 kinds of memory:
Immediate-term memory
Few seconds
Short-term memory
Seconds to minutes; limitedstorage capacity
Intermediate-term memory
It describe the memories thatoverlap short-term and long-term memory.
Long-term memory
Days, weeks, or a lifetime;requires transfer (consolidation)from short-term; rapid recall.
2 forms of memory:
Explicit/declarative memory
correlates with knowledge of people, places, and things
involves evaluation,comparison, and interference.
Im plicit/ proceduralmemory
correlates with ´howµ to dothings
acquired slowly throughmultiple repetitions.
Both of explicit & implicit memorieshave short-term forms & long-termforms.
8/8/2019 Grup B7 Tutor 4 Blok 16
http://slidepdf.com/reader/full/grup-b7-tutor-4-blok-16 10/34
Feb 5th 2010 B7 tutorial 4 10
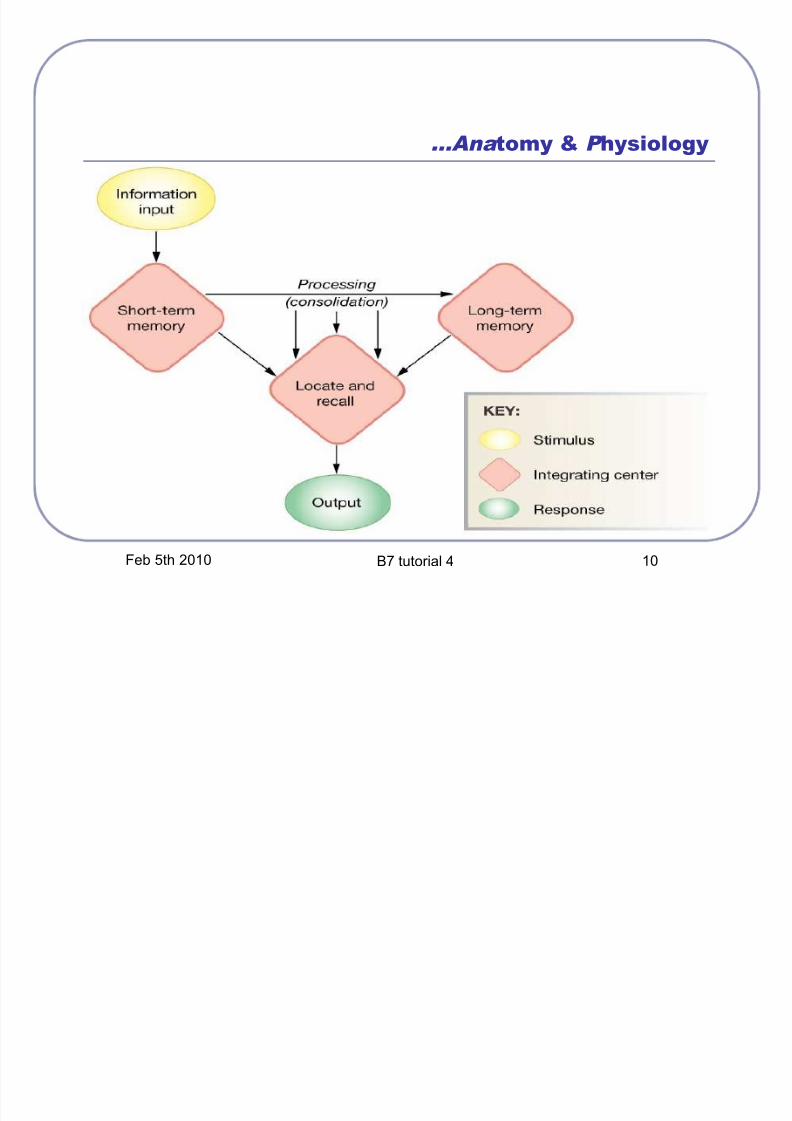
...Ana tomy & Physiology
8/8/2019 Grup B7 Tutor 4 Blok 16
http://slidepdf.com/reader/full/grup-b7-tutor-4-blok-16 11/34
Feb 5th 2010 B7 tutorial 4 11
...Ana tomy & Physiology
Anatomic areas that correlate with memory:
Explicit
Immediate: prefrontal cortex & dorsal medial thalamus or
primary & secondary sensory cortex. Short-term: hippocampus ad temporal lobe, mammilary bodies,midline diencephalic structures.
Long-term: diffuse throughout the cerebrum.
Im plicit
Motor: cerebellum, basal ganglia, secondary motor cortex.
Emotion-associated: amygdala.
8/8/2019 Grup B7 Tutor 4 Blok 16
http://slidepdf.com/reader/full/grup-b7-tutor-4-blok-16 12/34
Feb 5th 2010 B7 tutorial 4 12
Chief complaint: repeating certain
work unawarely, around 7 months,
proggresively worse
Disturbance in the neuron at the first time, there was a bit damage in theneuron (not really make his conditions become worse) followed by otherneuron damage itself spread progressively worse
8/8/2019 Grup B7 Tutor 4 Blok 16
http://slidepdf.com/reader/full/grup-b7-tutor-4-blok-16 13/34
Feb 5th 2010 B7 tutorial 4 13
Normal daily living except sometimes
he could not express some words
orally, happened in the last 1 month
It is caused by the accumulation of plaque beta amyloid protein,
tangles (tau protein) the accumulation will spread communication
between cells disturb sometime forget few words
Happening in the last 1 month means the proggresivity of the disease.
8/8/2019 Grup B7 Tutor 4 Blok 16
http://slidepdf.com/reader/full/grup-b7-tutor-4-blok-16 14/34
Feb 5th 2010 B7 tutorial 4 14
Correlation between his job, educational
background & his condition
Graduated from famous national university might show probability of lack of sleep
His job as senior officer might be really busy (stressor). Lack of sleep & really busy easily forget & contribute to
progressively worsen the damaging of nerve.
8/8/2019 Grup B7 Tutor 4 Blok 16
http://slidepdf.com/reader/full/grup-b7-tutor-4-blok-16 15/34
Feb 5th 2010 B7 tutorial 4 15
Examinations
Physical examination normal
No physical abnormality that play role in this case
No deficit in hard neurological function normal
No hard neurological disorder that play role in this case
8/8/2019 Grup B7 Tutor 4 Blok 16
http://slidepdf.com/reader/full/grup-b7-tutor-4-blok-16 16/34
Feb 5th 2010 B7 tutorial 4 16
...E xamina tion s
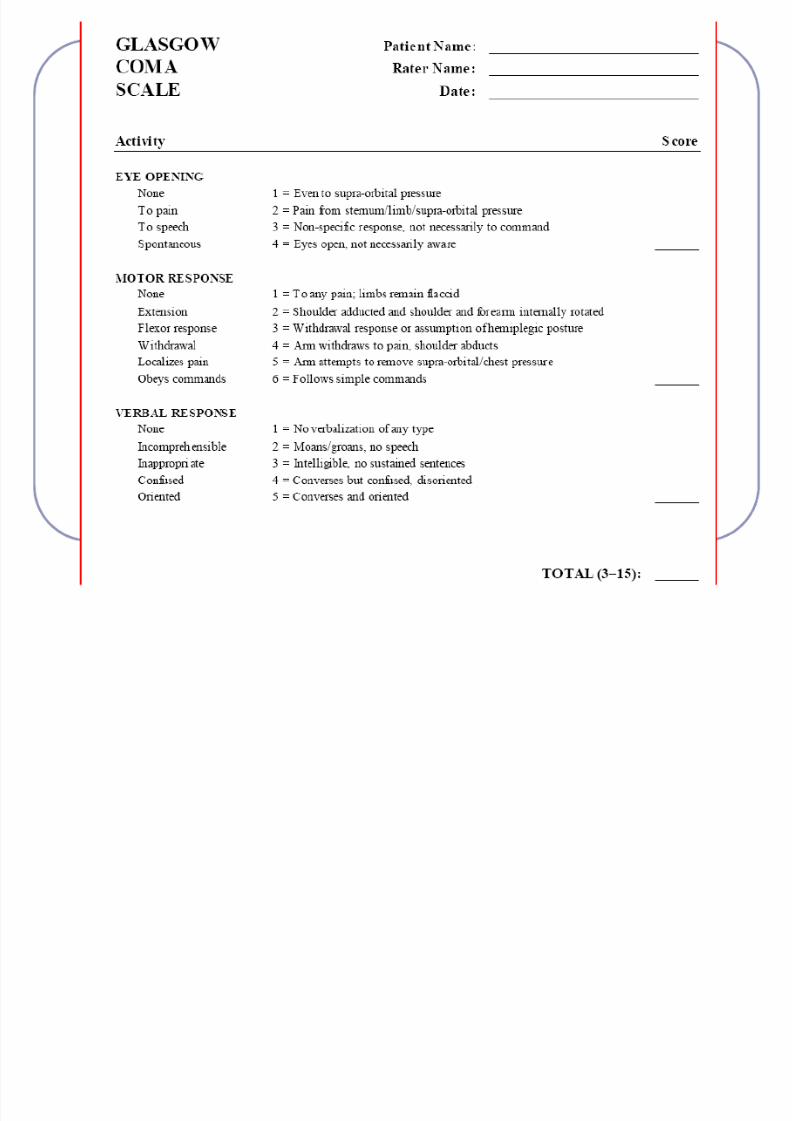
GCS was 15 normal = com pos mentis
Is a scale to assess level of consciousness 3 things to be assessed:
Eyes opening reaction
Verbal response
Motoric response
The highest value is 15 ( E4V5M6); the lowest value is 3( E1V1M1)
8/8/2019 Grup B7 Tutor 4 Blok 16
http://slidepdf.com/reader/full/grup-b7-tutor-4-blok-16 17/34
Feb 5th 2010 B7 tutorial 4 17
8/8/2019 Grup B7 Tutor 4 Blok 16
http://slidepdf.com/reader/full/grup-b7-tutor-4-blok-16 18/34
Feb 5th 2010 B7 tutorial 4 18
...E xamina tion s
Mental health normal
No psychosis is happened What things must be examined:
Common appearance Mood & affect Speech Perception Thinking
Sensorium & cognitive Impulse control Judgement & insight Realibility
8/8/2019 Grup B7 Tutor 4 Blok 16
http://slidepdf.com/reader/full/grup-b7-tutor-4-blok-16 19/34
Feb 5th 2010 B7 tutorial 4 19
...E xamina tion s
CT scanning of the head normal
No hard abnormal appearance. CT scan and MRI are used to "see" the brain and
surrounding organs. They don·t give a definitive diagnosis of
MCI.
They may show abnormalities in the brain that areconsistent with Alzheimer-like dementia. They also are usedto rule out potentially reversible causes of MCI.
8/8/2019 Grup B7 Tutor 4 Blok 16
http://slidepdf.com/reader/full/grup-b7-tutor-4-blok-16 20/34
Feb 5th 2010 B7 tutorial 4 20
...E xamina tion s
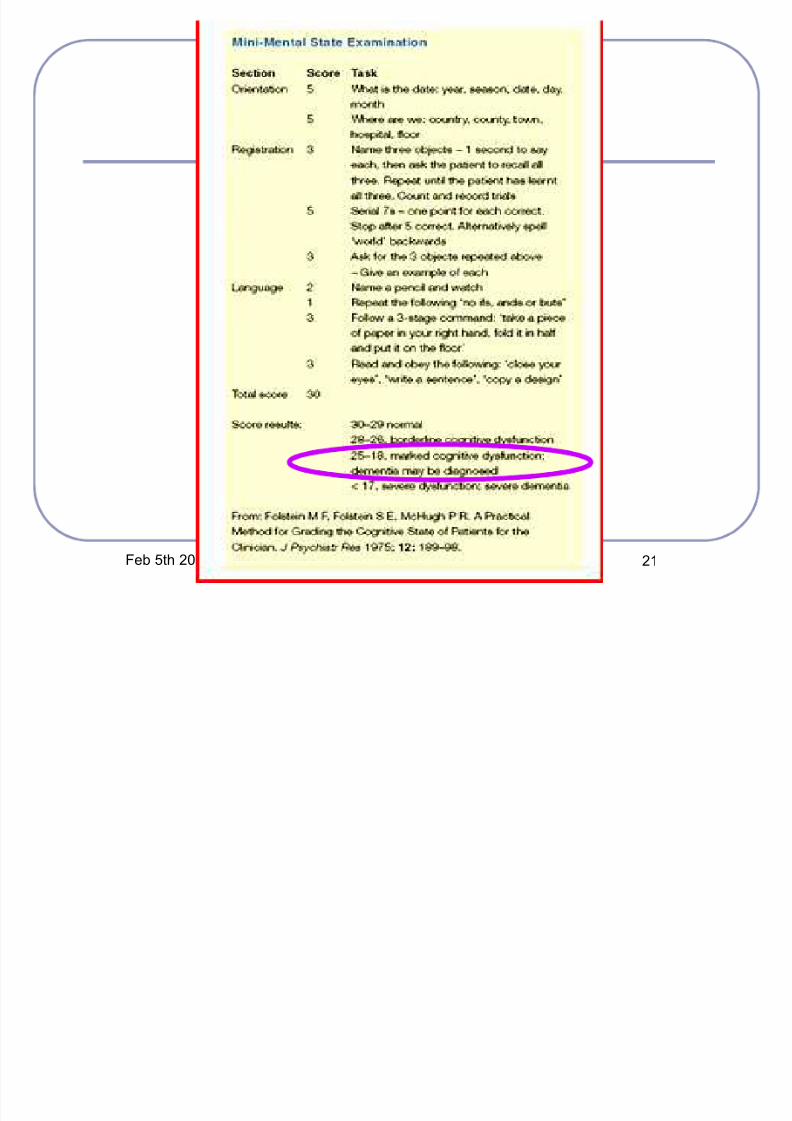
MMSE score was 22 ABNOR MAL
It is to indicate the presence of cognitive impairment
It is an 11-question measure that tests 5 areas of cognitive function:
Orientation (sekarang?, di mana?)
Registration (sebut 3 buah benda)
Attention & calculation (Kurangi 100 dengan 7 sebanyak 5x)
Recall (sebut 3 buah benda tadi) Language (sebut nama benda, ulang kata, lakukan perintah, baca &lakukan perintah, menulis spontan, menggambar bentuk)
8/8/2019 Grup B7 Tutor 4 Blok 16
http://slidepdf.com/reader/full/grup-b7-tutor-4-blok-16 21/34
Feb 5th 2010 B7 tutorial 4 21
8/8/2019 Grup B7 Tutor 4 Blok 16
http://slidepdf.com/reader/full/grup-b7-tutor-4-blok-16 22/34
Feb 5th 2010 B7 tutorial 4 22
Additional Information: traffic
accident 4 years ago & hospitalized
for 3 days
Concussion (Latin: to shake violently ) is the most common type
of traumatic brain injury
Concussion may be caused by:
blow to the head, or
acceleration forces without a direct impact.
It causes a variety of physical, cognitive, and emotional symptoms
8/8/2019 Grup B7 Tutor 4 Blok 16
http://slidepdf.com/reader/full/grup-b7-tutor-4-blok-16 23/34
Feb 5th 2010 B7 tutorial 4 23
Differential Diagnosis Normal aging
mild degree of forgetfulness it doesn·t disturb daily activities
MCI
turunnya penampilan kognitif (hendaya daya ingat, daya belajar, sulitberkonsentrasi)
tidak sampai memenuhi kriteria diagnosis demensia, sindromamnestik organik, atau delirium
dapat mendahului/menyertai/mengikuti berbagai macam gangguaninfeksi, fisik baik serebral maupun sistemik.
Dementia penurunan kemampuan daya ingat & daya pikir, mengganggu
kegiatan harian clear consciousness gejala sudah nyata 6 bulan
8/8/2019 Grup B7 Tutor 4 Blok 16
http://slidepdf.com/reader/full/grup-b7-tutor-4-blok-16 24/34
Feb 5th 2010 B7 tutorial 4 24
...Differen tial Diagno si s
Organic A mnestic Syndrome
penurunan daya ingat jangka pendek amnesia retrograde anterograde riwayat cedera otak atau penyakit otak lainnya (terutama di
diensefalon & temporal medial) tidak kurang daya ingat segera atau immediate recall tidak ada gangguan kesadaran dan gangguan perhatian
Delirium
ganguan kesadaran dan perhatian gangguan kognitif secara umum, gangguan psikomotor, gangguan
siklus tidur bangun, gangguan emosional Onset cepat perjalanan penyakit hilang timbul setiap hari, keadaan 6 bulan
8/8/2019 Grup B7 Tutor 4 Blok 16
http://slidepdf.com/reader/full/grup-b7-tutor-4-blok-16 25/34
Feb 5th 2010 B7 tutorial 4 25
How to diagnose Multiaxial diagnosis
Axis I : F06.7 gangguan kognitif ringan
Axis II : Z03.2 tidak ada diagnosis axis II Axis III : -
Axis IV : -
Axis V : 70 ² 61
8/8/2019 Grup B7 Tutor 4 Blok 16
http://slidepdf.com/reader/full/grup-b7-tutor-4-blok-16 26/34
Feb 5th 2010 B7 tutorial 4 26
Working diagnosis Diagnosis: Minimal Cognitive Impairment Definition: Gangguan memori (ingatan) nyata, bahasa, tetapi tidak
mempengaruhi aktifitas atau kegiatan sehari-hari penderitanya. MCImerupakan fase degenerasi otak ( otak mengalami kemunduran).
Etiology: Process of brain degeneration Abnormality of metabolism Vitamin deficiency Plaque
Hippocampus atrophy
Parkinson disease Epidemiology
Average age of patient is more than 75 years old
8/8/2019 Grup B7 Tutor 4 Blok 16
http://slidepdf.com/reader/full/grup-b7-tutor-4-blok-16 27/34
Feb 5th 2010 B7 tutorial 4 27
...Working diagno si s
Stage of brain deterioration:1. SENESCENCE (physiological)
Ditandai dengan mudah lupa (forgetfulness) Merupakan proses fisiologis (normal) pada usia lanjut
Prevalensi: 35% di usia > 65 tahun 39% kelompok usia 59-60 tahun 85% usia > 80 tahun
2. SENELITY (in between group)
Ditandai dengan memori dan language nyata tanpa demensia Pada Mild cognitive impairment (MCI) merupakan fasetransisi ke demensia
8/8/2019 Grup B7 Tutor 4 Blok 16
http://slidepdf.com/reader/full/grup-b7-tutor-4-blok-16 28/34
Feb 5th 2010 B7 tutorial 4 28
...Working diagno si s
3. DEMENSIA (pathological)
Minimal adanya 3 gangguan fungsi luhur
Gangguan memori yang paling menonjol: pikun
Merupakan medical illness
8/8/2019 Grup B7 Tutor 4 Blok 16
http://slidepdf.com/reader/full/grup-b7-tutor-4-blok-16 29/34
Feb 5th 2010 B7 tutorial 4 29
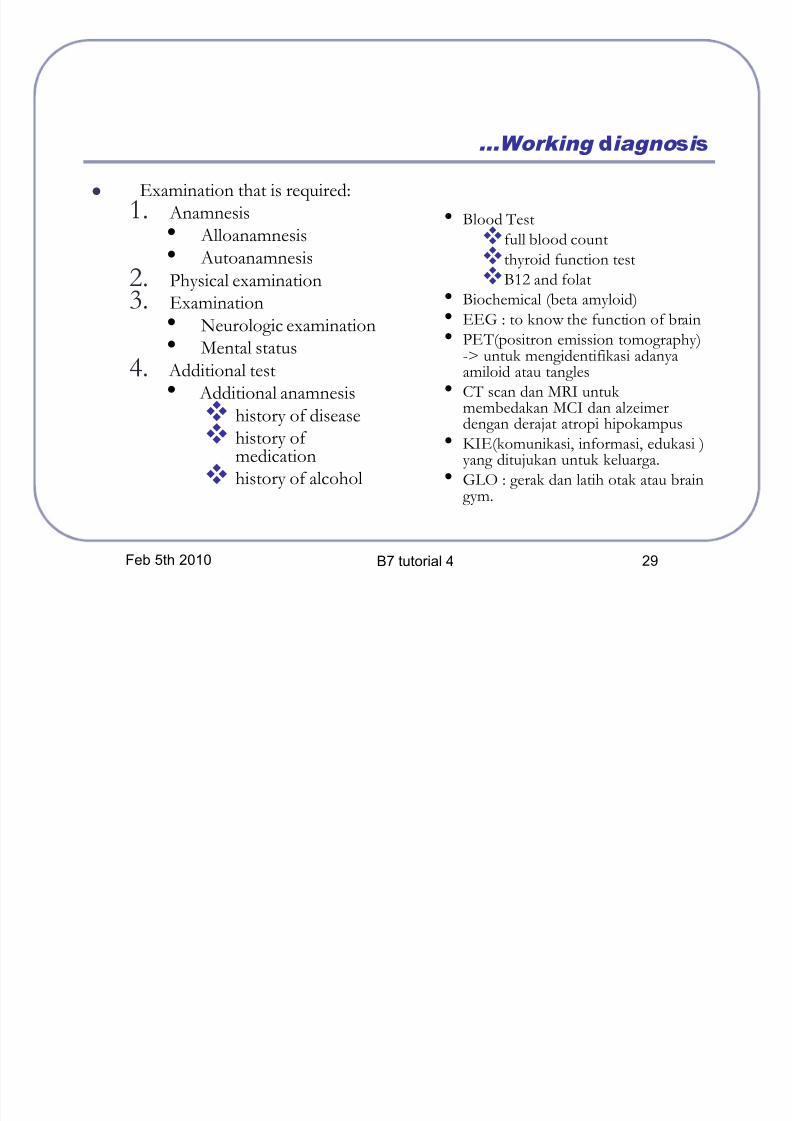
...Working diagno si s
Examination that is required:1. Anamnesis
Alloanamnesis Autoanamnesis
2. Physical examination3. Examination
Neurologic examination Mental status
4. Additional test Additional anamnesis
history of disease history of
medication history of alcohol
Blood Test
full blood count
thyroid function test
B12 and folat Biochemical (beta amyloid)
EEG : to know the function of brain
PE T(positron emission tomography)-> untuk mengidentifikasi adanyaamiloid atau tangles
CT scan dan MRI untuk membedakan MCI dan alzeimerdengan derajat atropi hipokampus
KIE(komunikasi, informasi, edukasi )yang ditujukan untuk keluarga.
GLO : gerak dan latih otak atau braingym.
8/8/2019 Grup B7 Tutor 4 Blok 16
http://slidepdf.com/reader/full/grup-b7-tutor-4-blok-16 30/34
8/8/2019 Grup B7 Tutor 4 Blok 16
http://slidepdf.com/reader/full/grup-b7-tutor-4-blok-16 31/34
Feb 5th 2010 B7 tutorial 4 31
Complication The next level of brain deterioration: Alzheimer·s dementia
8/8/2019 Grup B7 Tutor 4 Blok 16
http://slidepdf.com/reader/full/grup-b7-tutor-4-blok-16 32/34
Feb 5th 2010 B7 tutorial 4 32
Prognosis Quo ad vitam bonam
Tidak mengancam jiwa
Quo ad functionam
malamProgresif menjadi demensia
8/8/2019 Grup B7 Tutor 4 Blok 16
http://slidepdf.com/reader/full/grup-b7-tutor-4-blok-16 33/34
Feb 5th 2010 B7 tutorial 4 33
GP Competence
Neurobehaviour Disorders
MCI (Mild Cognitive Impairment) 1 2 3A 3B 4
Level 2Be able to established diagnosis based on physical examination &additional examinations
Refer to relevant specialistBe able to follow up this patient
8/8/2019 Grup B7 Tutor 4 Blok 16
http://slidepdf.com/reader/full/grup-b7-tutor-4-blok-16 34/34
Thank You
For Your Kind
Attention