Case Study Ona Age

of 22
Transcript of Case Study Ona Age
-
8/9/2019 Case Study Ona Age
1/22
-
8/9/2019 Case Study Ona Age
2/22
II. Nursing Assessment
A. PERSONAL DATA
1. Demographic data
In order to keep the life of our patient in private and to keep confidentiality let us just callhim Butad, 46 year old; male separated with his wife. He is 11th among the 12 children he
currently residing in Dolores Angeles city. He was admitted on April 15, 2010 and diagnosed as
AGE and discharge last April 20, 2010.
2. Socio-Economic and Cultural Factors
He is a jeepney driver and work 6 days a week with one day rest. His daily income
300/day most of his income is spends on food. Butad stop schooling when he was on his 1 st year
high school. He is a roman catholic. He was not able to attend mass regularly because of hiswork. Butad doesnt believe in faith healers and albularyo he directly goes to the hospital when
he feels sick.
History of Past Illness
Butad had fever and cough months before the admission.
History of Present Illness
Butad experience dizziness and vomiting at 3:00 pm on April 15, 2010. He went
straightly to ONA and got admitted on the same date.
F. Diagnostic and Laboratory Procedure
Diagnostic /
laboratory
procedure
Date
ordered
Date
results in
Indications or
Purposes
Results
(1st,2nd,3rd)
Normal
Values
(units used in
hospital)
Analysis and
Interpretations
of Results
(book-based)
Fecalysis Date
ordered
April 15,
2010
Date
To determine
the presence
of parasites
andcharacteristic
of stool.
Color: brown
Consistency:
soft
Color: brown
Consistency:
soft
Brown stools
and soft in
consistency
indicate normal
bowel
movement.
-
8/9/2019 Case Study Ona Age
3/22
results in
April 16,
2010
Others: no
ova or
parasite seen
No ova or
parasite seen
No eggs or
parasite seen
indicates that the
patient is freefrom intestinal
parasite
infestation.
1. PHYSICAL EXAMINATION (IPPA Cephalocaudal Approach)Initial Assessment upon Admission (April 15, 2010)Lifted from the chart .
a. Physical Assessment
Head / EENT: sclera pink conjunctiva
Chest: (-) retractions,
Cardiovascular: normal rate, regular rhythm
Abdomen: flabby, mass, soft, non tender
Extremities: fall and equal pulses
Nurse-Patient Interaction #1 (April 19, 2010)
Vital Signs as follows:
T: 36 C
P: 89bpm
R: 16cpm
BP:110/90 mmHg
Appearance and Mental Status
-
8/9/2019 Case Study Ona Age
4/22
Butad was received sitting on bed, conscious and coherent, afebrile, wearing short and t-
shirt. He was able to perform full ROM. He is able to understand and comprehend spoken
words.
Integumentary
Skin: (-) jaundice with good skin turgor; brown in color
Hair: black, long, straight and oily; with equal distribution;
Nails: pale nail beds; with no evidence of clubbing or unusual dryness or cracking;
convex nail curve; good capillary refill of 2 seconds; normal angle
Color: brown
Head
Skull: normocephalic, well-rounded and symmetrical in shape; no nodules or masses; no
abnormal prominence noted
Face: symmetrical facial movement; symmetrical facial feature; no lesion; no masses,
nodules and abnormal prominence
Eyes and Vision: iris are black in color; eyes are symmetrical; evenly distributed thin
eyebrows are symmetrically aligned; (-) ptosis; (+) PERRLA; pupils appears black and
equal in size, round; pink palpebral conjunctiva
Ear and Hearing: (+) whisper test; no lesions or abnormal discharges or swelling noted;
with minimal cerumen; hears normal conversation; pinna can be easily folded
Nose: symmetrical and straight; no evidence of deviated nasal septum; no tenderness;
uniform in color; presence of clear secretion; no flaring noted
Mouth: (-) halitosis; no teeth missing, teeth are white and shiny lips is pinkish in color;
tongue can move freely
Neck: no pain; no abnormal distention of jugular vein; trachea is located in the normal
position-midline; lymph nodes are not palpable and not swollen
Lymph Nodes:
anterior and posterior lymph nodes are not palpable; no generalized enlargement of lymph nodes
Thorax and Lungs: no abnormal shape and symmetry of the thorax; spine is vertically
aligned; spinal column is straight; there is full and symmetric chest expansion; no
tenderness; rales noted on both lung fields
Peripheral Pulses: there is a symmetrical pulse volume with full and regular pulsations
Abdomen: Hyperactive bowel sounds 40, mass rounded and flabby.
-
8/9/2019 Case Study Ona Age
5/22
Muscles: (-)tremors with good muscle tone and with equal size on both sides of the body; can
perform full range of motion
Bones: there are no deformities; no tenderness or swelling; minimal joint movements
Upper Extremities: symmetrically aligned (-) edema
Lower Extremities: symmetrically aligned; (-) edema
Reflexes: Patellar reflex is present as evidence by the extension or kicking out of the leg was
elicited by Mr. Jaundice
Motor Function: Kimi can perform range of motion with full resistance applied.
Pain Sensation: Kimi is able to discriminate sharp and dull sensations.
Position and kinesthetic sensation: Kimi is able to determine the position of fingers and toes.
Cranial Nerves:
CN I: able to distinguish isopropyl alcohol and chocolate drink
CN II: able to see far objects and texts, functional peripheral vision
CN III, IV, VI: (+)PERRLA, (-)ptosis, (-)nystagmus
CN V: able to feel and distinguish pinprick, wisp of cotton, hot and cold
CN VII: able to purse lips, raise the eyebrows and forehead and tightly close the eyes,
CN VIII: could hear a whispering voice.
CN IX, X: (+) gag reflex, (+) cough reflex; able to speak clear and loud
CN XI: able to elevate shoulders; turn head side to side, push head forward with resistance
CN XII: (-) tongue deviation,
Nurse-Patient Interaction #1 (April 20, 2010)
Vital Signs as follows:
T: 35.4 o C
P: 93bpm
R: 18cpm
BP:100/70mmHg
Appearance and Mental Status
Butad was received sitting on bed, conscious and coherent, afebrile, wearing
short and t-shirt. He was able to perform full ROM. He is able to understand and
comprehend spoken words.
Integumentary
-
8/9/2019 Case Study Ona Age
6/22
Skin: (-) jaundice with good skin turgor; brown in color
Hair: black, long, straight and oily; with equal distribution;
Nails: pale nail beds; with no evidence of clubbing or unusual dryness or cracking;
convex nail curve; good capillary refill of 2 seconds; normal angle
Color: brown
Head
Skull: normocephalic, well-rounded and symmetrical in shape; no nodules or masses; no
abnormal prominence noted
Face: symmetrical facial movement; symmetrical facial feature; no lesion; no masses,
nodules and abnormal prominence
Eyes and Vision: iris are black in color; eyes are symmetrical; evenly distributed thin
eyebrows are symmetrically aligned; (-) ptosis; (+) PERRLA; pupils appears black and
equal in size, round; pink palpebral conjunctiva
Ear and Hearing: (+) whisper test; no lesions or abnormal discharges or swelling noted;
with minimal cerumen; hears normal conversation; pinna can be easily folded
Nose: symmetrical and straight; no evidence of deviated nasal septum; no tenderness;
uniform in color; presence of clear secretion; no flaring noted
Mouth: (-) halitosis; no teeth missing, teeth are white and shiny lips is pinkish in color;
tongue can move freely
Neck: no pain; no abnormal distention of jugular vein; trachea is located in the normal
position-midline; lymph nodes are not palpable and not swollen
Lymph Nodes:
anterior and posterior lymph nodes are not palpable; no generalized enlargement of lymph nodes
Thorax and Lungs: no abnormal shape and symmetry of the thorax; spine is vertically
aligned; spinal column is straight; there is full and symmetric chest expansion; no
tenderness; rales noted on both lung fields
Peripheral Pulses: there is a symmetrical pulse volume with full and regular pulsations
Abdomen: Hyperactive bowel sounds 40, mass rounded and flabby.
Muscles: (-)tremors with good muscle tone and with equal size on both sides of the body; can
perform full range of motion
Bones: there are no deformities; no tenderness or swelling; minimal joint movements
Upper Extremities: symmetrically aligned (-) edema
Lower Extremities: symmetrically aligned; (-) edema
-
8/9/2019 Case Study Ona Age
7/22
Reflexes: Patellar reflex is present as evidence by the extension or kicking out of the leg was
elicited by Mr. Butad
Motor Function: Butad can perform range of motion with full resistance applied.
Pain Sensation: Butad is able to discriminate sharp and dull sensations.
Position and kinesthetic sensation: Butad is able to determine the position of fingers and
toes.
Cranial Nerves:
CN I: able to distinguish isopropyl alcohol and chocolate drink
CN II: able to see far objects and texts, functional peripheral vision
CN III, IV, VI: (+)PERRLA, (-)ptosis, (-)nystagmus
CN V: able to feel and distinguish pinprick, wisp of cotton, hot and cold
CN VII: able to purse lips, raise the eyebrows and forehead and tightly close the eyes,
CN VIII: could hear a whispering voice.
CN IX, X: (+) gag reflex, (+) cough reflex; able to speak clear and loud
CN XI: able to elevate shoulders; turn head side to side, push head forward with resistance
CN XII: (-) tongue deviation,
F. Diagnostic and Labolatory Procedure
Diagnostic /
laboratory
procedure
Date
ordered
Date
results in
Indications
or Purposes
Results
(1st,2nd,3rd)
Normal
Values
(units used in
hospital)
Analysis and
Interpretations
of Results
(book-based)
Fecalysis Date
ordered
July 15,
2009
Date
results in
Color: brown
Consistency:soft
Color: brown
Consistency:soft
Brown stools and
soft in
consistencyindicate normal
bowel movement.
No eggs or
-
8/9/2019 Case Study Ona Age
8/22
July 16,2009
Others: no ova
or parasite
seen
No ova or
parasite seen
parasite seenindicates that the
patient is free
from intestinal
parasite
infestation.
Nursing Responsibilities:
Prior:
a. Explain the procedure to the patient as well as to the SO.
b. Prepare the materials needed a clean leak proof container with cap, applicator sticks
and tissue or paper towel for wiping.
c. Instruct patient, or SO, on how to obtain stool sample, or assisting them to the bathroom,
providing privacy and proper draping.
d. Maintain aseptic technique, using clean gloves in obtaining the stool sample.
During:
a. Obtain stool sample using applicator stick.
b. Ensure that no urine water or soil or other material gets in the container.
After:
a. Cover the specimen cup and label.
b. Document the procedure, the time and date performed, and the patients response to the
procedure.
c. Assist the patient in returning to bed.
d. Leave the area clean and in order.
-
8/9/2019 Case Study Ona Age
9/22
-
8/9/2019 Case Study Ona Age
10/22
Document the time and procedure done. Then, obtain results and secure it in
the patients chart. Refer
-
8/9/2019 Case Study Ona Age
11/22
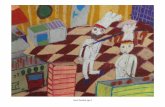
III. Anatomy and Physiology
Digestion is the break down of food to molecules that are small enough to be absorbed
into the circulation. Mechanical digestion breaks the large foods particles down into smaller ones.
Chemical digestion involves the breaking down of covalent chemical bonds in organic molecules
by digestive enzymes. Absorption begins in the stomach, where some small, lipids-soluble
molecules, such as alcohol and aspirin, can diffuse through the stomach epithelium into the
circulation. Most absorption occurs in the duodenum, and jejunum, although some occurs in the
ileum. Some molecules can diffuse through the intestinal wall. Others must be transported across
the intestinal wall. Transport requires carrier molecules and includes facilitated diffusion, co
-
8/9/2019 Case Study Ona Age
12/22
-
8/9/2019 Case Study Ona Age
13/22
-
8/9/2019 Case Study Ona Age
14/22
Duodenum
A hollow jointed tube about 25-30
cm long connecting the stomach to the jejunum. It is the first and shortest part
of the small intestine and it is where most chemical digestion takes place. The duodenum is
largely responsible for the breakdown of food in the small intestine. Brunner's glands, which
secrete mucus, are found in the duodenum. It also regulates the rate of emptying of the stomach
via hormonal pathways. Secretin and cholecystokinin are released from cells in the duodenal
epithelium in response to acidic and fatty stimuli present there when the pyloris opens and
releases gastric chyme into the duodenum for further digestion
Jejunum
the central of the three divisions of the small intestine and lies between the duodenum
and ileum. The inner surface of the jejunum, its mucous membrane, is covered in projections
called villi, which increase the surface area of tissue available to absorb nutrients from the gut
contents. The epithelial cells, which line these villi, possess even larger numbers of microvilli.
The transport of nutrients across epithelial cells through the jejunum and ileum includes the
passive transport of sugar fructose and the active transport of amino acids, small peptides,
vitamins, and most glucose. The villi in the jejunum are much longer than in the duodenum or
ileum.
Ileum
Is the final section of the small
intestine. It is about 2-4 m long in humans,
follows the duodenum and jejunum. The
pH in the ileum is usually between 7 and
8 (neutral or slightly alkaline). Its function is
mainly to absorb vitamin B12 and bile salts
and whatever products of digestion that
were not absorbed by the jejunum. The
-
8/9/2019 Case Study Ona Age
15/22
wall itself is made up of folds, each of which has many tiny finger-like projections known as villi,
on its surface. In turn, the epithelial cells which line these villi possess even larger numbers of
microvilli.
Large Intestines
The large intestine is responsible for the elimination of food materials that cannot be
digested and assimilated by the body. It is also
responsible for the re-absorption of water used
during the digestive process. As food materials
pass through the large intestine, friendly
bacteria that live in the colon act upon this
waste, producing vitamin K and some of the
B-vitamins.
IV. The Patient and His Illness
Synthesis of the Disease (Book-based)
a. Definition of the Disease
Gastroenteritis (also known as gastro, gastric flu, tummy bug in some countries,
and stomach flu, although unrelated to influenza) is inflammation of the gastrointestinal tract,
involving both the stomach and the small intestine and resulting in acute diarrhea. The
inflammation is caused most often by an infection from certain viruses or less often bybacteria,
theirtoxins,parasites, or an adverse reaction to something in the diet or medication. These agents
cause diarrhea by adherence, mucosal invasion, enterotoxin production, and/or cytotoxin
production. These mechanisms result in increased fluid secretion and/or decreased absorption.
This produces an increased luminal fluid content that cannot be adequately reabsorbed, leading to
diarrhea. The epithelium of the digestive tube is protected from insult by a number of
mechanisms constituting the gastrointestinal barrier, but like many barriers, it can be breached.
Disruption of the epithelium of the intestine due to microbial pathogens is a very common cause
of diarrhea in all species. Destruction of the epithelium results not only in exudation of serum and
blood into the lumen but often is associated with widespread destruction of absorptive epithelium.
In such cases, absorption of water occurs very inefficiently and diarrhea results. Aside from that a
large volumes of water are normally secreted into the small intestinal lumen, but a large majority
of this water is efficiently absorbed before reaching the large intestine. Diarrhea occurs when
secretion of water into the intestinal lumen exceeds absorption.
http://en.wikipedia.org/wiki/Influenzahttp://en.wikipedia.org/wiki/Inflammationhttp://en.wikipedia.org/wiki/Gastrointestinal_tracthttp://en.wikipedia.org/wiki/Stomachhttp://en.wikipedia.org/wiki/Small_intestinehttp://en.wikipedia.org/wiki/Acute_(medicine)http://en.wikipedia.org/wiki/Diarrheahttp://en.wikipedia.org/wiki/Infectionhttp://en.wikipedia.org/wiki/Virushttp://en.wikipedia.org/wiki/Bacteriahttp://en.wikipedia.org/wiki/Toxinhttp://en.wikipedia.org/wiki/Parasiteshttp://en.wikipedia.org/wiki/Adverse_reactionhttp://en.wikipedia.org/wiki/Influenzahttp://en.wikipedia.org/wiki/Inflammationhttp://en.wikipedia.org/wiki/Gastrointestinal_tracthttp://en.wikipedia.org/wiki/Stomachhttp://en.wikipedia.org/wiki/Small_intestinehttp://en.wikipedia.org/wiki/Acute_(medicine)http://en.wikipedia.org/wiki/Diarrheahttp://en.wikipedia.org/wiki/Infectionhttp://en.wikipedia.org/wiki/Virushttp://en.wikipedia.org/wiki/Bacteriahttp://en.wikipedia.org/wiki/Toxinhttp://en.wikipedia.org/wiki/Parasiteshttp://en.wikipedia.org/wiki/Adverse_reaction -
8/9/2019 Case Study Ona Age
16/22
This infectious agent also triggers the body to release chemical mediator which serves as
the guard system of the body. These chemical mediator releases endogenous pyrogens that
stimulate the hypothalamus, which is the heat regulator of the brain to reset the body temperature
resulting to an increased in body temperature.
A child with gastroenteritis experiences not only decreased absorption of water but also nutrients
needed by the body, a condition resulting to weakness and pallor. Since the disease condition
mainly involves the inflammation of the gastrointestinal tract, certain gastrointestinal
disturbances are manifested by the patient, this include: nausea, vomiting, loss of appetite,
abdominal cramps and abdominal pain. The child may be lethargic, suffer lack of sleep, or run a
high fever and have signs of dehydration, which include dry mucous membranes, reduced skin
turgor, sunken fontanelles and sunken eyeballs, poor perfusion resulting to pallor.
At least 50% of cases of gastroenteritis due to foodborne illness are caused by norovirus.
Another20% of cases, and the majority of severe cases in children, are due to rotavirus. Other significant
viral agents include adenovirusand astrovirus.
Different species of bacteria can cause gastroenteritis, including Salmonella, Shigella,
Staphylococcus,Campylobacter jejuni,Clostridium,Escherichia coli,Yersinia, and others. Some
sources of the infection are improperly prepared food, reheated meat dishes, seafood, dairy, and
bakery products. Each organism causes slightly different symptoms but all result in diarrhea.
Risk factors include consumption of improperly prepared foods or contaminated water and travel
or residence in areas of poor sanitation. It is also common for river swimmers to become infected
during times of rain as a result of contaminated runoff water.
Classification
Bacterial gastroenteritis
Pseudomembranous colitis is an important cause of diarrhea in patients often recently treated with
antibiotics. If gastroenteritis in a child is severe enough to require admission to a hospital, then it
is important to distinguish between bacterial and viral infections. Bacteria, Shigella and
Campylobacter, for example, andparasites like Giardia can be treated with antibiotics. Traveler's
diarrhea is usually a type of bacterial gastroenteritis.
http://en.wikipedia.org/wiki/Foodborne_illnesshttp://en.wikipedia.org/wiki/Norovirushttp://en.wikipedia.org/wiki/Rotavirushttp://en.wikipedia.org/wiki/Adenovirushttp://en.wikipedia.org/wiki/Adenovirushttp://en.wikipedia.org/wiki/Astrovirushttp://en.wikipedia.org/wiki/Salmonellahttp://en.wikipedia.org/wiki/Shigellahttp://en.wikipedia.org/wiki/Shigellahttp://en.wikipedia.org/wiki/Staphylococcushttp://en.wikipedia.org/wiki/Staphylococcushttp://en.wikipedia.org/wiki/Campylobacter_jejunihttp://en.wikipedia.org/wiki/Campylobacter_jejunihttp://en.wikipedia.org/wiki/Campylobacter_jejunihttp://en.wikipedia.org/wiki/Clostridiumhttp://en.wikipedia.org/wiki/Escherichia_colihttp://en.wikipedia.org/wiki/Escherichia_colihttp://en.wikipedia.org/wiki/Yersiniahttp://en.wikipedia.org/wiki/Yersiniahttp://en.wikipedia.org/wiki/Yersiniahttp://en.wikipedia.org/wiki/Pseudomembranous_colitishttp://en.wikipedia.org/wiki/Shigellahttp://en.wikipedia.org/wiki/Campylobacterhttp://en.wikipedia.org/wiki/Parasitehttp://en.wikipedia.org/wiki/Giardiahttp://en.wikipedia.org/wiki/Antibiotichttp://en.wikipedia.org/wiki/Traveler's_diarrheahttp://en.wikipedia.org/wiki/Traveler's_diarrheahttp://en.wikipedia.org/wiki/Foodborne_illnesshttp://en.wikipedia.org/wiki/Norovirushttp://en.wikipedia.org/wiki/Rotavirushttp://en.wikipedia.org/wiki/Adenovirushttp://en.wikipedia.org/wiki/Astrovirushttp://en.wikipedia.org/wiki/Salmonellahttp://en.wikipedia.org/wiki/Shigellahttp://en.wikipedia.org/wiki/Staphylococcushttp://en.wikipedia.org/wiki/Campylobacter_jejunihttp://en.wikipedia.org/wiki/Clostridiumhttp://en.wikipedia.org/wiki/Escherichia_colihttp://en.wikipedia.org/wiki/Yersiniahttp://en.wikipedia.org/wiki/Pseudomembranous_colitishttp://en.wikipedia.org/wiki/Shigellahttp://en.wikipedia.org/wiki/Campylobacterhttp://en.wikipedia.org/wiki/Parasitehttp://en.wikipedia.org/wiki/Giardiahttp://en.wikipedia.org/wiki/Antibiotichttp://en.wikipedia.org/wiki/Traveler's_diarrheahttp://en.wikipedia.org/wiki/Traveler's_diarrhea -
8/9/2019 Case Study Ona Age
17/22
Viral gastroenteritis
Viruses causing gastroenteritis include rotavirus,norovirus, adenovirus and astrovirus. Viruses do
not respond to antibiotics and infected children usually make a full recovery after a few
days.Children admitted to hospital with gastroenteritis routinely are tested for rotavirus A togather surveillance data relevant to the epidemiological effects of rotavirus vaccination
programs.These children are routinely tested also for norovirus, which is extraordinarily
infectious and requires special isolation procedures to avoid transmission to other patients. Other
methods, electron microscopy and polyacrylamide gel electrophoresis, are used in research
laboratories.
B. Modifiable and Non-Modifiable factors
NON-MODIFIABLE FACTORS
o Age- Infants are more likely to acquire Gastroenteritis because their intestinal flora has
not yet fully developed. Lactose intolerance also aggravates the problem.
MODIFIABLE FACTORS
o Poor Environmental Sanitation-The environment plays a vital role in our health. An
unhygienic or poor environmental condition may lead to acquiring such disease.
o Poor Hygienic Practices one does not performed proper hand washing technique
after defecation and before handling food.
o Intake of Drugs
o Intake of food allergens
o Nutrient Deficiencies poor immune system
o Contaminated Food-A person who frequently eats street foods and junk foods is at risk
of having Gastroenteritis.
o Low socio-economic status-Due to low income, the tendency is that the foods that being
bought is less nutritious, hence, not being cautious with the food being consumed.
C. Signs and Symptoms
The condition is usually ofacute onset, normally lasting 16 days, and is self-limiting.
o Nausea and vomiting- stimulation of CTZ
http://en.wikipedia.org/wiki/Rotavirushttp://en.wikipedia.org/wiki/Norovirushttp://en.wikipedia.org/wiki/Adenovirushttp://en.wikipedia.org/wiki/Astrovirushttp://en.wikipedia.org/wiki/Norovirushttp://en.wikipedia.org/wiki/Electron_microscopyhttp://en.wikipedia.org/wiki/Polyacrylamide_gel_electrophoresishttp://en.wikipedia.org/wiki/Acute_(medical)http://en.wikipedia.org/wiki/Self-limiting_(biology)http://en.wikipedia.org/wiki/Nauseahttp://en.wikipedia.org/wiki/Vomitinghttp://en.wikipedia.org/wiki/Rotavirushttp://en.wikipedia.org/wiki/Norovirushttp://en.wikipedia.org/wiki/Adenovirushttp://en.wikipedia.org/wiki/Astrovirushttp://en.wikipedia.org/wiki/Norovirushttp://en.wikipedia.org/wiki/Electron_microscopyhttp://en.wikipedia.org/wiki/Polyacrylamide_gel_electrophoresishttp://en.wikipedia.org/wiki/Acute_(medical)http://en.wikipedia.org/wiki/Self-limiting_(biology)http://en.wikipedia.org/wiki/Nauseahttp://en.wikipedia.org/wiki/Vomiting -
8/9/2019 Case Study Ona Age
18/22
o Diarrhea- this is due to increased luminal fluid content that cannot be adequately
reabsorbed, leading to diarrhea. Destruction of the epithelium results not only in
exudation of serum and blood into the lumen but often is associated with widespread
destruction of absorptive epithelium thus leading to decreased absorption of water. This
manifestation can also be linked to secretion of water into the intestinal lumen which
exceeds the absorption.
o Loss of appetite- Gastrointestinal disturbances are due to the alteration on the function of
the intestinal epithelium that occurred because of the inflammation of the gastrointestinal
tract.
o Fever- inflammatory process
o Abdominal pain- changes in the intestinal lumen or intestinal epithelium led to intestinal
spasm leading to a painful stimulation felt by the patient.
o Bloody stools (dysentery - suggesting infection by amoeba, Campylobacter, Salmonella,
Shigella or some pathogenic strains ofEscherichia coli)
o Fainting and Weakness- another manifestation that occurred due to prolonged
decreased absorption of nutrients needed by the body for energy reserve.
o Signs ofdehydration(which include dry mucous membranes), tachycardia, reduced skin
turgor, skin color discoloration, sunken fontanels, sunken eyeballs, darkened eye circles,
glassy eyes, poorperfusion and ultimately shock.
o Poor feeding- occurs because of the disturbance of gastrointestinal function.
Viral diarrhea usually causes frequent watery stools, whereas blood stained diarrhea may be
indicative of bacterial colitis. In some cases, even when the stomach is empty, bile can be
vomited up.
http://en.wikipedia.org/wiki/Diarrheahttp://en.wikipedia.org/wiki/Dysenteryhttp://en.wikipedia.org/wiki/Dehydrationhttp://en.wikipedia.org/wiki/Dehydrationhttp://en.wikipedia.org/wiki/Tachycardiahttp://en.wikipedia.org/wiki/Turgorhttp://en.wikipedia.org/wiki/Fontanelleshttp://en.wikipedia.org/wiki/Perfusionhttp://en.wikipedia.org/wiki/Shock_(medical)http://en.wikipedia.org/wiki/Colitishttp://en.wikipedia.org/wiki/Bilehttp://en.wikipedia.org/wiki/Diarrheahttp://en.wikipedia.org/wiki/Dysenteryhttp://en.wikipedia.org/wiki/Dehydrationhttp://en.wikipedia.org/wiki/Tachycardiahttp://en.wikipedia.org/wiki/Turgorhttp://en.wikipedia.org/wiki/Fontanelleshttp://en.wikipedia.org/wiki/Perfusionhttp://en.wikipedia.org/wiki/Shock_(medical)http://en.wikipedia.org/wiki/Colitishttp://en.wikipedia.org/wiki/Bile -
8/9/2019 Case Study Ona Age
19/22
-
8/9/2019 Case Study Ona Age
20/22
-
8/9/2019 Case Study Ona Age
21/22
Dizziness- defined as disorientation in space; a sense of unsteadiness;
a feeling of movement within the head such as giddiness or a
swimming sensation; lightheadedness; or a whirling sensation.
Hyper active bowels sounds- the patient had 40 bowels sounds
compared to the normal which is 20.
4. Health Promotion and Preventive Aspects
Health promotion actions for avoiding such GI infections involve instructing clients
about (1) good handwashing technique after defacation and before handling food and (2)
obtaining available vaccinations against bacterial and viral gastroenteritis. Encourage cleanliness
and sanitation as well as proper food handling, preparation and storage techniques, such as
cooking meats to 150F, cooking chicken to 170F, and not allowing food to sit at room
temperature for long periods. In developing countries, safe food practices must be done such as
avoiding tap water, ice cubes, milk products, raw meat or seafood, salads and foods that cannot
be cooked or peeled
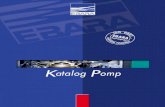
CLIENT BASED PATHOPHYSIOLOGY
Non-ModifiableFactors
Age
Modifiable Factors
Poor EnvironmentalSanitation
Poor hygienic Practices Low socio-economic
status
Entrance of Microorganisms in the digestive tract via oral route
Mucosal InvasionEndotoxin ProductionAttachment to the villi
Toxins/Viruses/bacteria/
parasites enter theintestinal epithelium
Triggers the immune
response of the bodyInflammator Process
Release of Chemical
Mediators
Destruction of the
absorptive epithelium
Destroyed intestinal
epithelium are replacedwith immature cells
-
8/9/2019 Case Study Ona Age
22/22
Release of EndogenousPyrogens
Body increase heatproduction and decrease
heat loss
Fever & dizziness 04-15& 16-10
Gastrointestinaldisturbances
Vomiting04-15-10
Hyperactivebowel sounds
04-15-10