C61 Renal artery embolism
1
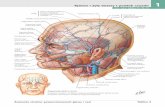
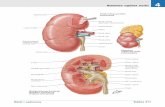
C61 Renal artery embolism Eur Urol Suppl 2013;12;e1169 Cerny J. 1 , Petrik A. 1 , Uhlirova I. 2 , Hes K. 3 1 Ceske Budejovice Hospital, Dept. of Urology, Ceské Budejovice, Czech Republic, 2 Strakonice Hospital, Dept. of General Surgery, Strakonice, Czech Republic, 3 Ceske Budejovice Hospital, Dept. of Radiology, Ceske Budejovice, Czech Republic INTRODUCTION & OBJECTIVES: The aim of the work is to present a case of renal artery embolism. MATERIAL & METHODS: Presentation of a case report of patient with renal infarction on the basis of a blood clot emboli in hypercoagulopathy. RESULTS: 49 year-old female patient without any urological or hematological history was admitted at the surgical department of the district hospital for a flank pain, mild fever and nausea. At the time of admission there was leukocytosis, erythrocyturia, CRP 19.7 in basic lab tests. Sonographic abdomen examination, KUB and VUG were without any pathological findings. Cause of sustaining complaints CT VUG was performed, showing occlusion of a left renal artery due to arterial thrombus, upper half kidney infarction with obvious persistent excretory renal function. The lower pole of the kidney is supplied by an aberrant artery without changes. Immediately after diagnosis, 38 hours after the first symptoms, the patient was transported to superior medical care centre for radiological renal artery revascularization. Minimally invasive left renal artery clot evacuation was performed without any complications. In 24 hour apart the controll angiography shew a good left renal artery patency, with a persistent residual infarction of a cranial half of the kidney. To find out the aethiology of the renal embolus pacient underwent cardiac examination, which was without pathological findings. Hematology tests discovered hypercoagulopathy. An anticoagulant and antiplatelet therapy was initiated. Patient was discharged to homecare on the 4th day of hospitalization without any difficulties. Following genetic testing revealed homozygous mutation of the gene encoding prothrombin (G20210A). In the distance of six weeks CT arteriography was performed, where two well forward arteries with ischaemic parenchymal changes in the upper half of the kidney were displayed. After 3 months the decrease level of a relative left kidney function at 35% with the cranial defect was confirmed on renal scintigraphy scan. The patient has been set on long term anticoagulant therapy. CONCLUSIONS: Kidney infarction is a rare and therefore often neglected diagnosis. Early revasularisation of the renal artery by the minimally radiological intervention reduces the likelihood of irreversible damage to the renal parenchyma. The fact that renal function was not fully altered despite the 38-hour delay of revascularisation, can give an evidence of partial closure and presence of the aberrant renal artery.
Transcript of C61 Renal artery embolism

C61 Renal artery embolism Eur Urol Suppl 2013;12;e1169
Cerny J.1, Petrik A.1, Uhlirova I.2, Hes K.3
1Ceske Budejovice Hospital, Dept. of Urology, Ceské Budejovice, Czech Republic, 2Strakonice Hospital, Dept. of General
Surgery, Strakonice, Czech Republic, 3Ceske Budejovice Hospital, Dept. of Radiology, Ceske Budejovice, Czech Republic
INTRODUCTION & OBJECTIVES: The aim of the work is to present a case of renal artery embolism.
MATERIAL & METHODS: Presentation of a case report of patient with renal infarction on the basis of a blood clot emboli in
hypercoagulopathy.
RESULTS: 49 year-old female patient without any urological or hematological history was admitted at the surgical department
of the district hospital for a flank pain, mild fever and nausea. At the time of admission there was leukocytosis, erythrocyturia,
CRP 19.7 in basic lab tests. Sonographic abdomen examination, KUB and VUG were without any pathological findings. Cause
of sustaining complaints CT VUG was performed, showing occlusion of a left renal artery due to arterial thrombus, upper half
kidney infarction with obvious persistent excretory renal function. The lower pole of the kidney is supplied by an aberrant artery
without changes. Immediately after diagnosis, 38 hours after the first symptoms, the patient was transported to superior medical
care centre for radiological renal artery revascularization. Minimally invasive left renal artery clot evacuation was
performed without any complications. In 24 hour apart the controll angiography shew a good left renal artery patency, with a
persistent residual infarction of a cranial half of the kidney. To find out the aethiology of the renal embolus pacient underwent
cardiac examination, which was without pathological findings. Hematology tests discovered hypercoagulopathy. An
anticoagulant and antiplatelet therapy was initiated. Patient was discharged to homecare on the 4th day of hospitalization without
any difficulties. Following genetic testing revealed homozygous mutation of the gene encoding prothrombin (G20210A). In the
distance of six weeks CT arteriography was performed, where two well forward arteries with ischaemic parenchymal changes in
the upper half of the kidney were displayed. After 3 months the decrease level of a relative left kidney function at 35% with the
cranial defect was confirmed on renal scintigraphy scan. The patient has been set on long term anticoagulant therapy.
CONCLUSIONS: Kidney infarction is a rare and therefore often neglected diagnosis. Early revasularisation of the renal artery
by the minimally radiological intervention reduces the likelihood of irreversible damage to the renal parenchyma. The fact that
renal function was not fully altered despite the 38-hour delay of revascularisation, can give an evidence of partial closure and
presence of the aberrant renal artery.