Va Respiratory System08

of 35
Transcript of Va Respiratory System08
-
8/14/2019 Va Respiratory System08
1/35
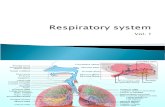
Va. Respiratory SystemThe term respiration includes three separate but related functions: 1) ventilation(breathing); 2) gas exchange , which occurs between the air and blood in the lungs and
between the blood and other tissues of the body; and 3) oxygen utilization by tissues inthe energy-liberation reaction in the mitochondria of the cells involving the Krebs cycle(citric acid cycle) and oxidative phosphyorylation. In this section we will only addressventilation and gas exchange.
A. Structure of the Respiratory System
1
-
8/14/2019 Va Respiratory System08
2/35
The air passages of the respiratory system are divided into two function zones: theconducting zone , which includes all of the anatomical structures through which air
passes before reaching the respiratory zone; and the respiratory zone, which is theregion where gas exchange occurs.
The conducting zone of the respiratorysystem, in summary, consists of themouth, nose, pharynx, trachea, primarybronchi, and all successive branchingof the bronchi up to and including theterminal bronchioles. The structures of the conducting zone serve the followingfunctions : warming and humidifying the inspired air; and filtration and cleaning of the inspired air. Regardlessof the temperature and humidity of theambient air, when inspired air reaches
the respiratory zone it is at a temperatureof 37 C (body temperature), and issaturated with water vapor as it flowsover warm, wet mucous membranes thatline the respiratory airways. Thisinsures that a constant internal bodytemperature will be maintained and thatthe delicate lung tissue will be protectedagainst desiccation. Mucus secreted bygoblet cells (see below) of theconducting zone epithelium serves totrap small particles in the inspired air and thereby performs a filtration
function. This mucus blanket is moved up the airways to the trachea at a rate of 1-2centimeters per minute by cilia projecting from the tops of the cilia cells that line theconducting zone.
2
-
8/14/2019 Va Respiratory System08
3/35
As you can see in the above diagram, the epithelium of the conduction zone also consistof two other types of cells, clara cells and basal cells. The clara cells are thought tohave two main functions: 1) to synthesize and secret proteins such as antibodies andlysosymes to detoxify harmful substances (e.g., bacteria, fungi) inhaled into the lungs;and 2) can also differentiate into ciliated cells to regenerate bronchiolar epithelium. Thebasal cells are thought to be bronchial stem cells and can differentiate into either claracells or ciliated cells. Submucosal glands of the tracheobronchial airways provide theimportant function of secreting mucins, antimicrobial substances and copious amounts of fluid that add to the liquid the composes the mucociliary blanket . The important rolethe submucosal glands play in proper maintenance of the mucociliary blanket isdemonstrated in the disease of cystic fibrosis, which we will cover in the next section.
The respiratory zone of the lungs is the location for gaseous exchange and consists of therespiratory bronchioles , alveoli sacs , and alveoli.
3
-
8/14/2019 Va Respiratory System08
4/35
B. Thoracic Cavity
There are two serous membrane layers that surround the lungs called the pleural membranes. The parietal pleura lines the inside of the thoracic wall and covers thediaphragm. The visceral pleura covers the surface of the lungs. In between the parietal
4
-
8/14/2019 Va Respiratory System08
5/35
and visceral pleura is the pleural cavity . Note how similar this is to the anatomicalassociation of the visceral and parietal pericardium and pericardial cavity for the heart.There is, under healthy conditions, a potential space called the intrapleural space that can become a real space if the visceral and parietal pleura separate when a lungcollapses, as in a pneumothorax.
1. Physical Aspects of Ventilation
The diagram above shows pressure relationships of the atmospheric pressure (760 mmHg), lungs ( intrapulmonary or intra-alveolar pressure = 760 mm Hg ), and the pleuralcavity ( intrapleural pressure = 755 mm Hg) at the end of respiration.
5
-
8/14/2019 Va Respiratory System08
6/35
The following diagrams represent a schematic of the intrapleural space (yellow), theintrapulmonary/intra-alveolar pressure in the lung and air conducting pathway (blue) and theambient air surrounding the body (also shown in blue as it is continuous with the air in the lung).Recall that atmospheric pressure is approximately 760 mmHg. The pressures shown in thesediagrams are the difference from atmospheric pressure (ie., 760-755 = -5). Thus, a value of 0mmHg in any of the diagrams indicates no difference from atmospheric pressure!
A. End expiration (diagram above): At rest, intrapleural pressure must remain slightlynegative (here it is shown as -5 mmHg) as i) the lung is elastic and has a tendency tocollapse or shrink, and ii) the fluid lining the alveolar surfaces generates surface tensionthat works to collapse the lung (stay tuned). Notice that both the lung and the air conducting pathways are labeled as 0 mmHg; this means that the pressure in the lungsand air conducting pathway are not different from atmospheric pressure! If the pressures
in the lung or air conducting pathway are different than atmospheric, there will bemovement of air into or out of the lung!
B. Inspiration (diagram above): Since air moves by bulk flow, if there is no pressuredifference between any 2 spaces, air will not move between those spaces. Withinspiration, intrapleural pressure becomes more negative (-10) as the chest expands. The
6
-
8/14/2019 Va Respiratory System08
7/35
increased negative pressure of the intrapleural space stretches the lung as the chest movesup and out and the diaphragm moves down, creating negative pressure in the lung! Thenegative pressure in the lung gradually decreases as air moves through the conducting
pathways (-6) towards their openings with the atmosphere (-3).
C) End inspiration (diagram above): Once the chest and diaphragm stop theremovement at the end of inspiration, air pressure in the airways and alveoli(intrapulmonary and intra-alveolar pressure) equalize to that of ambient air pressure.That is, as air flow stops at the end of inspiration, the pressure in the lungs and air conducting pathways once again equalize with ambient air pressure!
D) Expiration (diagram above): Now the intercostal muscles of the chest (between theribs), and the diaphragm relaxes and the recoiling elastic properties of the lung pull thechest down and the diaphragm up. This action increases the intrapulmonary (+4) andintra-alveolar pressure (+8) over that of ambient pressure (0), and air is pushed out of the lungs.
C. Physical Properties of the Lungs
7
-
8/14/2019 Va Respiratory System08
8/35
In order to understand the main diseases of the pulmonary system, the four physical properties of the lungs that we will study in this course in order to understand the pathophysiology of pulmonary diseases are: compliance , lung elastic ity, airwayresistance , and surface tension.
In order for inspiration to occur, the lungs must be able to expand when stretched by theaction of the chest wall and diaphragm; they must have compliance. We will define lung compliance as the ease at which the lung can be expanded during inspiration.
In order of expiration to occur, the lungs must recoil when the chest wall anddiaphragm relax; they must have elasticity. We will define lung elasticity as the ease atwhich the lung can return to its resting state .
A third physical property that is involved with pulmonary disease is resistance to air flowthrough the bronchi and bronchioles, or airway resistance. The formula we studied thatdetermined resistance to blood flow holds true for resistance to airflow. That is, the
radius of the airways controls resistance to airflow (ie., bronchodilation vs bronchoconstriction)..
The fourth physical property of the lung is surface tension, that is controlled by the thinfilm of fluid normally present in the lining of the alveolus. If the thin film of fluid liningthe alveoli is not treated, the lung will fill with fluid and collapse. The treatment isthe surfactant (stay tuned)..
a. Compliance
Lung compliance (C L) is expressed as the change in lung volume (V L) for every unitchange in intrapleural pressure (P). Let us say that the 5 mm Hg drop in intrapleural
pressure above (-5 mm Hg to -10 mm Hg) or a P of 5 mm Hg, resulted in bringing intothe lungs 500 ml of air (V L = 500). To determine lung compliance the followingformula is used:
C L = V L / P or 500/5 = 100
Now lets say that a pulmonary disease has caused infiltration of lung tissue withconnective tissue proteins, a condition called pulmonary fibrosis. Pulmonary fibrosisresults in a condition called restrictive pulmonary disease . Restrictive pulmonarydiseases lower lung compliance (ie., make it harder to expand, or the intercostal musclesand diaphragm would have to work harder to expand the lungs). An example of arestrictive pulmonary disease would be the lungs reaction to chronic inhalation of mineraldust (eg., coal dust, silica, or asbestos)
8
-
8/14/2019 Va Respiratory System08
9/35
Black Lung, or Coal Miners Lung
The scaring due to Black Lung will leave the lung tissue less compliant or stiffer.Therefore, in order to move the same amount of air (500 ml) into the lungs, theintrapleural pressure must be lowered to 7 mm Hg (ie., as opposed to 5 mm Hg). Nowthe compliance is: 500/7 = 71.4. Therefore, what does lowering lung compliance mean to
the person with Black Lung disease? They must do more work to bring air into their lungs with each breath.
b. Elasticity
The term elasticity refers to the tendency of a structure to return to its initial size after being distended. Because of their high content of elastic fibers and elastin proteins (see below), the lungs are very elastic and resists distension. Since the lung is normally stuck to the chest wall, they are always in a state of elastic tension. This tension increasesduring inspiration when the lungs are stretched and is reduced during elastic recoil duringexpiration. With cigarette smoking we lose these elastic fibers (see diagrams below) andtherefore the recoil of the lungsa condition called emphysema.
c. Airway Resistance
9
-
8/14/2019 Va Respiratory System08
10/35
Close your eyes and concentrate on your breathing, the air going into and out of your lungs. Notice the ease at which this occurs. When healthy, your airways offer little, if any, resistance to air. But any condition that causes bronchoconstriction , like asthma or
bronchitis, will reduce the radius of the airways and, therefore, increase resistance of air flow. When suffering from an asthmatic attack or chronic bronchitis, a person mustfight or expend energy to breath in an attempt to overcome the resistance to airfow.We will call this obstructive pulmonary disease .
d. Surface Tension.
What is Surface Tension?Surface tension is defined as amanifestation of attracting forces
between atoms or molecules. It ismeasured in units of force/unit lengthsuch as dynes/cm. In a beaker of water, consider how attracting forcesacting on water molecule A differ from those acting on water moleculeB (see figure to right). Theintermolecular attracting forces onmolecule A are equal in alldirections, whereas molecule B at theair-liquid interface exhibits animbalance in attracting forces
because few water molecules are present in the air phase above the beaker. This imbalance of attracting forces acting on molecule B result in it being pulled downward and sidewise more than upward. This imbalance of forces actsto shrink the liquid-air interface to the smallest possible area. Thus, the force of
10
-
8/14/2019 Va Respiratory System08
11/35
surface tension acts in the plane of theair-liquid boundary to shrink or minimize the liquid-air interface (see
bottom figure ). This surface tensioncan form skin on water on whichaquatic insects can walk. However,unlike the flat interface present in the
beaker, alveoli are nearly spherical inshape, so surface tension forces of thefluid film lining alveoli must beconsidered for a sphere.
Surface Tension in a Sphere: the LaPlace RelationshipThe fluid film lining alveoli assumes a spherical shape because of the nearly sphericalnature of alveoli. In many regards, the fluid film lining alveoli resembles a soap bubble. In
a soap bubble, the relationship between pressure and surface tension (S.T.) is related inan equation derived by LaPlace for spherical objects. This equation states that thedistending (inflating) or collapsing (recoil) pressure for a soap bubble is directly related toS.T. of the air-fluid interface and inversely related to the radius (r) of the sphere. Thefluid film lining alveoli is an ultrafiltrate of plasma, and S.T. is nearly constant andmeasure somewhere between 50 to 70 dynes/cm, regardless of alveolar radius.
LaPlace Relations
11
-
8/14/2019 Va Respiratory System08
12/35
Alveolar Instability with Constant Surface Tension If alveolar surface tension is assumed to be constant, say 50 dynes/cm, then therecoil (collapsing pressure) could be calculated for alveoli of different radii usingthe LaPlace equation (see top figure ). Using arbitrary units for radius and
pressure, the calculations indicate that alveolus A, with a radius of 1 unit, has ahigher pressure than alveolus B, with a radius of 2 units. Since all lung alveoli areinterconnected by the airways, the higher pressure in alveolus A would cause it todischarge its air volume into alveolus B (see bottom animation ). According to theLaPlace equation, as the radius of alveolus A becomes progressively smaller asair moves to alveolus B, pressure in alveolus A steadily increases as the radiusdecreases with deflation. At the same time, pressure in alveolus B declines further
because its radius increases as it fills with air. The implications for the lung as awhole are that alveoli with smaller radii (high pressure) would empty their air volume into larger alveoli and eventually collapse. In a short time, most of the air in the lung would be contained in a few large-radius alveoli, with most remaining
alveoli collapsed. Such alveolar instability would result in a marked reduction insurface area for gas exchange.
www.lib.mcg.edu/.../section4/4ch2/s4ch2_35.htm
12
http://www.lib.mcg.edu/edu/eshuphysio/program/section4/4ch2/s4ch2_35.htmhttp://www.lib.mcg.edu/edu/eshuphysio/program/section4/4ch2/s4ch2_35.htm -
8/14/2019 Va Respiratory System08
13/35
Alveolar Opening Pressure with Constant Surface Tension Alveolar instability would not only result in smaller radii alveoli dumping their air intolarger alveoli, but collapsed alveoli, or those with extremely small radii, would requireextremely high opening pressures to inflate. Thus, freshly inspired air would be directedtowards large-radii alveoli (alveolus B) because the pressure required to expand them
would be less than that to inflate collapsed or small-radii alveoli (alveolus A). In fact, if alveoli had a constant surface tension, it is unlikely that the respiratory muscles would beable to generate sufficient pressure (force) to inflate smaller radii alveoli because of their high opening pressures. Likewise, if ventilated alveoli collapsed during expiration, itwould be difficult to inflate them on the next breath because of the high opening
pressures associated with their small radius ( figure ).
Physiochemical Properties of Surfactant The ability of surfactants to lower surface tension is related to their chemical structure.Because lung surfactants have hydrophobic (water-fearing) and hydrophilic (water-loving)groups at different ends of the molecule, they preferentially accumulate at the liquid-air interface. At the interface, the hydrophilic end of the molecule extends into the liquid andthe hydrophobic end projects into the air phase above (see top figure ). Surfactant naturallyaccumulates at the liquid-air interface to reduce the number of water molecules that wouldnormally occupy the interface. The presence of surfactant molecules disrupts attractingforces between water molecules to reduce surface tension. Moreover, as surface area isdecreased, such as when an alveolus deflates, the relative concentration of surfactantmolecules per unit area tends to increase. This higher concentration of surfactantmolecules is even more effective in reducing surface tension (see bottom figure ). Asalveoli inflate, water molecules must be brought to the interface, so surface tensionincreases as fewer surfactant molecules are present per unit area. The Laplace relationshipis still applicable, however, alveolar surface tension is not constant but decreases asalveolar radius decreases. As a result, pressures in small-radii alveoli are less than in large-radii alveoli. During inspiration, air initially moves into smaller radii alveoli or from larger to smaller alveoli to ensure uniform filling of all alveoli. Also, the presence of surfactantreduces the opening and expanding pressures of small-radii alveoli. This enhances alveolar stability and reduces the work of breathing.
13
http://www.lib.mcg.edu/edu/eshuphysio/program/section4/4ch2/s4ch2_34.htmhttp://www.lib.mcg.edu/edu/eshuphysio/program/section4/4ch2/s4ch2_34.htm -
8/14/2019 Va Respiratory System08
14/35
Chemical Composition of Lung Surfactant
The surfactant present in the fluidlining lung alveoli is a complex"cocktail" of several differentmolecules. However, the principalmolecules are dipalmityl
phosphatidylcholine (lecithin) and phosphatidylglycerol. Thesecompounds, along with severalothers, appear to be synthetized byalveolar Type II cells and releasedinto the alveolus by exocytosis. Thetwo main stimuli for surfactantsecretion appear to be stretching the
alveolus during inflation and -adrenergic activation. Some of thesurfactant appear to be recirculated.However, with each breath, some"fresh" surfactant is secreted while some is taken up for re-release by the Type II cells.
Surfactant;
14
-
8/14/2019 Va Respiratory System08
15/35
Respiratory distress syndrome (RDS) is life threatening lung disorder that commonly affects premature infants. Respiratory distress syndrome results from failure of the type II alveolar cellsto produce sufficient levels of surfactant. The incidence of RDS declines with degree of maturityat birth. It occurs in 60 percent of babies born at less than 28 weeks' gestation, 30 percent of those
born at 28 to 34 weeks, and less than 5 percent of those born after 34 weeks
D. Lung Volumes and Capacitiesa. Spirometry
15
-
8/14/2019 Va Respiratory System08
16/35
Tidal volume (TV) is the volume of air moved in and out of the respiratory tract(breathed) during each ventilatory cycle.
Inspiratory reserve volume (IRV) is the additional volume of air that can be forciblyinhaled following a normal inspiration. It can be accessed simply by inspiring maximally,
to the maximal inspiratory level.Expiratory reserve volume (ERV) is the additional volume of air that can be forciblyexhaled following a normal expiration. It can be accessed simply by expiring maximallyto the maximal expiratory level.
Vital capacity (VC) is the maximal volume of air that can be forcibly exhaled after amaximal inspiration. VC = TV + IRV + ERV.
Residual volume (RV) is that volume of air remaining in the lungs after a maximalexpiration. It cannot be expired no matter how vigorous or long the effort. RV = FRC -ERV.
b. FVC - forced expiratory vital capacity
The volume change of the lung between a full inspiration to total lung capacity and amaximal expiration to residual volume. The measurement is performed during forcefulexhalation; the preceding maximal inhalation need not be performed forcefully.Thevolume assessed is the forced expiratory vital capacity (FEVC), commonly called forced vital capacity (FVC). The maneuver is almost invariably performed in conjunction withthe assessment of the FEV1 .
16
-
8/14/2019 Va Respiratory System08
17/35
b. FEV1 - forced expiratory volume in 1 second, FEV1%VC
The FEV1 is the volume exhaled during the first second of a forced expiratory maneuver started from the level of total lung capacity.
FEV1 is by far the mostfrequently used index for
assessing airway obstruction, bronchoconstriction or bronchodilatation; FEV1 expressedas a percentage of the VC is the standard index for assessing and quantifying airflowlimitation
17
-
8/14/2019 Va Respiratory System08
18/35
E. Gas Exchange in the Lungs
According to Daltons Law, the total pressure of a gas mixture (such as air) is equal to thesum of pressures that each gas in the mixture would exert independently. The pressurethat a particular gas in a mixture exerts, independently, is the partial pressure of that gas.
18
-
8/14/2019 Va Respiratory System08
19/35
The total pressure of a gas mixture is thus equal to the sum of the partial pressures of allthe gases in the gas mixture. Since oxygen constitutes about 21% of the atmosphere, its
partial pressure (abbreviated P O2) is 21% of atmospheric pressure (760 mm Hg), or approximately 159 mm Hg(0.21 x 760 = 159 mmHg). Since nitrogen constitutes about78% of the atmosphere, its partial pressure is equal to 0.78 x 760 = 593 mm Hg. Thesetwo gases contribute approximately 99% of the total atmospheric pressure.
1. P O2 and Altitude
The atmospheric P O2 does not reflect the alveolar P O2 (P AO2 ) because we are not takinginto account the fact that as the air passes through the conducting pathways it becomes100% saturated. That is, in the alveoli we have a new gas in our mixture of air, water vapor. Water vapor has a partial pressure of 47 mm Hg.. Therefore, in order todetermine P AO2 we have to subtract 47 mm Hg from atmospheric pressure.
P AO2 = 0.21 (760-47) = 150 mm Hg (ie., not 159)
But the above formula assumes that there is no mixing of air before the tidal volumereaches the alveoli. When we breath, there is a mixing of good or fresh atmosphericair coming down with the stale air that was present in the conducting airways. When it
19
-
8/14/2019 Va Respiratory System08
20/35
is all said and done (ie., water vapor, mixing of air), at sea level (ie., atmospheric pressure= 760), P AO2 = 100 mm Hg.
Using the graph on page 19, at Denver, the atmospheric pressure is approximately 619mm Hg, thus the P O2 is 130 mm Hg. When water vapor and mixing of air is considered,this result in a P AO2 = 84 mm Hg. The take home is this, the higher the altitude, the lower the P O2 and therefore, the lower the P AO2 .2. Arterial and Alveolar O 2 and CO 2
20
-
8/14/2019 Va Respiratory System08
21/35
When the lungs are healthy, the P O2 of systemic arterial blood (PaO 2 , 97 mm Hg) is 3-5 mm Hgless than that of P AO2 (100 mm Hg). Note, that the partial pressure of carbon dioxide of arterial
blood ( PaCO 2 , 40 mm Hg ) also reflects that of the partial pressure of alveolar CO 2 ( P ACO 2 , 40mm Hg ). This is the take-home: at sea level, no matter if a person is quietly sitting or exercisingat high intensity, PaO 2 of 97 mm Hg and PaCO 2, 40 mm Hg should remain constant. Thesevalues are clinically significant because they reflect lung function.
3. Oxygen Saturation of Arterial Blood
Each hemoglobin molecule has four Fe ++heme sites for binding oxygen. If there is nointerference (as from carbon monoxide, for example), the free O 2 molecules bind to thesesites with great avidity. The total percentage of sites actually bound with O 2 is the'saturation of blood with oxygen'. This is called SvO 2 and SaO 2 in the venous and arterialcirculations, respectively. An SaO 2 of 97% simply means that of every 100 hemoglobin
binding sites, 97 are occupied with an oxygen molecule and the other three are either bound to something else or are unbound. SaO 2 is determined mainly by PaO 2. The relationship between the two variables is the familiar oxygendissociation curve (graph on next page). Using a ruler, you candetermine from this graph that at a PaO 2 of 97 mm Hg, the SaO 2 is 98%.
21
-
8/14/2019 Va Respiratory System08
22/35
4. Oxygen Content of Arterial Blood
Given the above, one can also determine how much oxygen, in milliters per deciliter of blood (ml/dl), is being carried by blood. We will call this the oxygen content of arterial blood (CaO 2). Oxygen content is determined by the formula:
CaO 2 = Hb (gm/dl) x 1.34 ml O 2/gm Hb x SaO 2
With Hb representing blood hemoglobin levels in grams per deciliter (gm/dl), 1.34 beinga constant, and SaO 2 representing the saturation of arterial blood. Therefore, given thePaO 2 is 97 mm Hg and a Hb of 15 gms/dl, what is the oxy gen content?
PaO 2 of 97 mm Hg = SaO 2 of 98%CaO 2 = 15 gms/dl x 1.34 ml O 2/gm Hb x 98%
CaO 2 = 19.7 gms/dl
You can see from this formula that any change in hemoglobin content or oxygensaturation will have an affect on the oxygen carrying capacity of blood.
22
-
8/14/2019 Va Respiratory System08
23/35
5. Oxyhemoglobin Dissociation Curve
This curve describes the relationship between available oxygen and amount of oxygen carried by hemoglobin.
The oxyhemoglobin dissociation curve is S-shaped, or sigmoidal . The fact that it isrelatively flat at high PO 2 indicates that changes from 60 mm Hg to higher PO 2 has littleaffect on % oxygen saturation of blood. That is, at a PO 2 of 60 mm Hg, the blood would
be 90% saturated with oxygen; at a PO 2 of 70 mm Hg, 93%; at a PO 2 of 80 mm Hg,96%, and so on.
Below a PO 2 of 60 mm Hg, the curve becomes steep. This means that small changes inPO 2 will produce large differences in % oxygen saturation of blood. That is, at a PO 2 of 50 mm Hg, the blood would be 82% saturated with oxygen; at a PO 2 of 40 mm Hg, the
blood would be 73% saturated with oxygen; at a PO 2 of 30 mm Hg, the blood would be55% saturated with oxygen, and so on.
The part of the oxygenhemoglobin dissociation curve at or above a PO 2 of 60 mm Hgrepresents P AO2 . If because of either high altitude or a pulmonary disease, the P AO2 .dropsfrom 100 mm Hg (97% saturated) to 80 mm Hg (95% saturated), there is little change inthe about of oxygen that is being carried by blood as it leaves that lung. That is, a drop of 20 mm Hg of P AO2 .(100-80 mm Hg), results in only a 2% drop in oxygen saturation of the
blood.
Blood leaving the lungs will stay at the %saturation level acquired in the lungs until itreaches a capillary bed. The part of the oxygenhemoglobin dissociation curve starting at aPO 2 of 40 mm Hg represents the tissue PO 2 in the capillary bed. The % saturation thatthe blood will leave the capillary bed and enter venules to begin the journey back to theheart depends of the PO 2 of the capillary bed (see diagram below) In the diagram, thePO 2 of the capillary bed is 40 mm Hg, and therefore the PO 2 of blood leaving thecapillary blood is 40 mm Hg, and at that PO 2 , the blood is 73% saturated. That is, as
23
-
8/14/2019 Va Respiratory System08
24/35
blood flows through the capillary, its PO 2 equilibriates with the tissues PO 2 .
On the other had, if the capillary bed is situated in a skeletal muscle that is doing work (exercise) and the PO 2 of that capillary bed is 10 mm Hg, the blood will leave thatcapillary bed at the same PO 2 (10 mm Hg) and at a % saturation of 14%Lets review what we have just discussed, but instead of % oxygen saturation, letsconvert % oxygen saturation to the amount of oxygen being carried by blood. Going tothe graph on the top of page 22, blood entering the capillary blood with a PO 2 of 95-100mm Hg is carrying approximately 19.5 ml/dl of oxygen. When blood leaves the capillary
bed at a PO 2 of 40 mm Hg, it is carrying approximately 14.5 ml/dl of oxygen.Therefore, it has unloaded 5.0 ml/dl of oxygen into the capillary bed. In the exercisingmuscle, when blood leaves the capillary bed at 10 mm Hg, it is carrying approximately2.5 ml/dl, which means it has unloaded 17.0 ml/dl of oxygen.
After entering the venous system, the blood returns to the right ventricle, gets pumped tothe lungs, and the following happens.www.biotech.um.edu.mt/.../oxygen5.htm
a. Affect of pH and Temperature on Oxyhemoglobin DissociationCurve.
24
http://www.biotech.um.edu.mt/home_pages/chris/Respiration/oxygen5.htmhttp://www.biotech.um.edu.mt/home_pages/chris/Respiration/oxygen5.htm -
8/14/2019 Va Respiratory System08
25/35
In addition to changes in PO 2 , the percent of oxygen saturation at a given PO 2 is alsoinfluence by changes in the affinity of hemoglobin for oxygen. Such changes ensure thatactive skeletal muscle will receive more oxygen from the blood than they do at rest..Thisoccurs as a result of lowered ph and increased temperature in exercising muscle.
The affinity of oxygen for hemoglobin is decreased when pH is lowered and increasedwhen pH is raised: this is called the Bohr effect .
As you might imagine, the Bohr effect was first discovered by a guy named Bohr! Hediscovered that there were other factors that affected the loading/unloading of oxygen byHb. One of the factors that he discovered was pH. He found that if the pH was lower thannormal (normal physiological pH is 7.4), then Hb does not bind oxygen as well. This isshown in the following % Saturation graph.
This plot includes the % Saturation of Hb at normal pH ( 7.4 ) and at a lower pH value
(7.2 ). You should notice that the curves are not identical suggesting that pH affects the binding of oxygen to Hb. Let us examine the % saturation at the lungs and at the tissueswhen only the pH is changed. In the lungs (pO 2 = 100 mm Hg), Hb is 98% saturated at
both pH 7.4 and 7.2. Thus the binding of oxygen to Hb in the lungs is not affected bychanging the pH and oxygen will load normally. The situation is different at the tissues.The change in the pH results in a lower % saturation of Hb even though the pO 2 in thetissues has remained at 40 mm Hg for this example. Reading from the graph, the %saturation at pH 7.4 with a pO 2 of 40 mm Hg is about 70% (meaning 30% of the oxygencoming to the tissue is released). At a pH of 7.2, the value is close to 60% (meaning 40%
25
-
8/14/2019 Va Respiratory System08
26/35
of the oxygen coming to the tissue is released). Thus more oxygen is delivered to tissuesat a lower pH even when the pO 2 remains unchanged. Lowering the pH appears to shiftthe entire red curve to the right.
Now, is this just a boring piece of information or does it have physiological significance.Remember, if we were to design an oxygen delivery system, we would like to deliver
more oxygen to the more active tissues, the ones that need the oxygen. How would weknow if a tissue is more active and requires more oxygen? One way is by the amount of oxygen present in a tissue. If the tissue is using more oxygen, then one would expect theamount of oxygen (pO 2) would be lower. Another indicator that a tissue has a highmetabolic rate (and thus a need for increased oxygen delivery) is the production of carbondioxide. When a tissue is more active, the amount of carbon dioxide produced will beincreased (PCO 2 is higher). Carbon dioxide reacts with water as shown in the followingequation:
CO 2+ H 2O H + + HCO -3What this means is that as the amount of carbon dioxide increases, more H + are formedand the pH will decrease. Thus, a lower pH in the blood is suggestive of an increasedcarbon dioxide concentration which in turn is suggestive of a more active tissue thatrequires more oxygen. According to Bohr, the lower pH will cause Hb to deliver moreoxygen! Just what we want to occur.
Note that if pO 2 and pH should drop together, even more oxygen will be delivered than if only one of the parameters were changed (for example, pH = 7.2, pO 2 = 30 mm Hgcompared to pH = 7.4, pO 2 = 30 mm Hg).
A few more items to add to your knowledge base: If the pH of the tissues should rise (dueto a drop in the carbon dioxide concentration), then the % Saturation curve shifts to theleft (see graph below) and results in less oxygen being delivered. Does that make sense?Also, there are several other factors that will also affect the binding of oxygen to Hb. Oneof these is temperature. A more active tissue will be producing more heat and will bewarmer. This increased temperature shifts the curve to the right (see below) just asdecreased pH does. Is this beneficial to the tissue? Why
26
-
8/14/2019 Va Respiratory System08
27/35
b. Affect of 2,3-DPG on Oxyhemoglobin Dissociation Curve
2,3-diphosphoglyceric acid (2,3-DPG) is an anaerobic metabolite produced in red bloodcells during glycolysis. 2,3-DPG facilitates the release of oxygen into the tissues bycombining with subunits of hemoglobin to reduce its affinity for oxygen. Therefore, itaffects the oxyhemoglobin dissociation curve in the same manner as increasedtemperature and decreased pH. When oxyhemoglobin concentration is decreased due tohigh altitude or pulmonary lung disease, the concentration of 2,3-DPG within the RBCsis increased.
6. Ventilation Perfusion
a.a. DefinitionsDefinitionsi.i.
VA= alveolar ventilation= alveolar ventilation
ii.ii.
Q
= pulmonary capillary blood flow.= pulmonary capillary blood flow. Often referred to asOften referred to as
"perfusion"."perfusion".
27
-
8/14/2019 Va Respiratory System08
28/35
b. b. Normally the overall Normally the overall
/V QA
of the lung is (4 L/min)of the lung is (4 L/min) /(/(5 L/min) = 0.85 L/min) = 0.8
c.c. Since there is normally no diffusion impairment theSince there is normally no diffusion impairment thePO 2
andandPCO 2
in anin an
alveolus and its end capillary blood arealveolus and its end capillary blood are usually the same as each other usually the same as each other (PA02 = 100, PaO2 = 97, PACO2 = 40 mmHg, PaCO2 = 40 mm Hg(PA02 = 100, PaO2 = 97, PACO2 = 40 mmHg, PaCO2 = 40 mm Hg
d.d. The extreme conditions of The extreme conditions of
/V QA
Figure 1 Figure 1
A.A. If ventilation of the alveolusIf ventilation of the alveolus is stopped (e.g.,is stopped (e.g., , blockage of alveolar duct or , blockage of alveolar duct or respiratory bronchiole due to a mucus plug caused by chronic bronchitis),respiratory bronchiole due to a mucus plug caused by chronic bronchitis), thenthen alveolar air would approach that of venous blood gases andalveolar air would approach that of venous blood gases and
/V QA
< 0.8< 0.8 ((egeg ., 3/5., 3/5
= 0.6)= 0.6)
A.A. Normal Normal
A.A. If perfusIf perfus ion of the lungs are affectedion of the lungs are affected ((egeg .,., right heart failure) andright heart failure) and ventjilationventjilation to theto the lung continued while blood flow was reduced, alveolar lung continued while blood flow was reduced, alveolar aireaire would approach that of would approach that of inspired air and theinspired air and the
/V QA
> 0.8 (e.g., 4/4 = 1).> 0.8 (e.g., 4/4 = 1).
Bottom line: respiratory diseases will causeBottom line: respiratory diseases will cause
/V QA
to be below 0.8.to be below 0.8.
28
-
8/14/2019 Va Respiratory System08
29/35
F.F. Regulation of BreathingRegulation of Breathing
Inspiration and Expiration movements are produced by the contraction of theinspiratory and expiratory muscles. These muscles are striated muscles and thusrequire nervous stimulation for contraction. These stimuli are transportedthrough two descending tracts from the respiratory control centers (involuntarybreathing )and from the cerebral cortex ( voluntary breathing ). Involuntary
29
-
8/14/2019 Va Respiratory System08
30/35
breathing is automatic and involves the central and peripheral chemoreceptorstalking to the brain stem respiratory centers. We will address the brain stemrespiratory centers and chemorecptors below. Voluntary breathing is
performed when we consciously control our breathing when we talk or sing, or purposely take a deep breath. With voluntary breathing, our cerebral cortextalks to the brain stem respiratory centers.
1. Brain Stem Respiratory CentersThere are three areas in the brain stem that control respiration: two areas in the
pons (apneustic and pneumotaxic centers) and one area in the medulla(rhythmicity center)(see diagram above).
Rhythmicity Centre 1 Situated in the Medulla oblongata
2 I neurons stimulate spinal motor neurons that innervate therespiratory muscles producing Inspiration
3 E neurons inhibit the I neurons and thus produce expiration byrelaxation of the respiratory muscles
4 I and E neuronal activity varies in a reciprocal way so that arhythmic pattern is obtained
30
-
8/14/2019 Va Respiratory System08
31/35
Apneustic Centre 1 Situated in the Pons
2 Stimulate the I neurons in the Medulla Oblongata
3 Result in Inspiration
4 Provides a constant stimulus for inspiration
Pneumotaxic Centre 1 Situated in the Pons
2 Seems to antagonize the apneustic centre
3 Inhibits inspiration
1.1. Automatic Control of BreathingAutomatic Control of BreathingAutonomic control also influenced by input from receptors sensitive to chemical changes
in the blood particularly the PCO 2, PO 2 and pH. Two groups of receptors:
a. Central ChemoreceptorsFound in the ventral portion of the medulla oblongata and are most sensitive to changesin the arterial PCO 2. Neurons from this centre communicate with the respiratory centersin the medulla oblongata. An increase in the PCO 2, causes an increase in thecerebrospinal PCO 2 level with a resultant decrease in the cerebrospinal pH. The fall in pHstimulates the medullar chemoreceptors resulting in an increase in ventilatory rate.
31
-
8/14/2019 Va Respiratory System08
32/35
Stimulation of Central ChemoreceptorsThe central chemoreceptors have been located
physiologically but not anatomically.Chemosensitive areas (CSA) are located alongthe ventrolateral surface of the medulla near thecerebral spinal fluid (CSF) of the 4th ventricleof the brain. At least three areas of the brainstem appear capable of chemodetection. Likethe arterial chemoreceptors, the centralchemoreceptors are stimulated by an increase inthe PCO 2 or H + concentration, but not O2. Thesecentral chemosensitive areas appear to be moresensitive to changes in the H + or PCO 2 of CSFthan of cerebral blood. The blood brain barrier (BBB), that separates blood from the CSF,limits access of certain blood constituents, suchas HCO 3- and H + to the CSF. In contrast to the
peripheral receptors, the central chemoreceptorsare not sensitive to changes in the PO 2 of cerebral blood or CSF.
b. Peripheral Chemoreceptors
32
-
8/14/2019 Va Respiratory System08
33/35
The peripheral chemoreceptors are mainly situated in the carotid and aortic bodies. Theyreceive blood directly from small arterial branches from these large arteries. These
receptors are not stimulated directly by the PCO 2 but by a rise in the H+
concentration (adecrease in the pH). On stimulation a resultant increase in ventilation rate occurs. A verylow PO 2, around 50mmHg (only achieved through experimental means), can stimulatethe peripheral chemoreceptors directly but as this degree of hypoxaemia does notnormally occur at sea level, PO 2 does not normally exert a direct effect on breathing.
Guide Questions1. What are the two main functions of the conducting zone?2. What functions do the following cells play in the formation and/or movement as
well as function of the mucus blanket within the conducting system: ciliatedcells, clara cells, goblet cells, submucosal glands.
3. The respiratory zone consists of what three components?4. What are the two serous membrane layers that surround the lungs? What is thespace between these membranes?
5. Using the difference from atmospheric pressure, at the end of expiration what isthe difference between intrapleural pressure and the pressure in the air conducting
pathways/alveoli (we will call the pressure in the air conducting pathways/alveoli,intrapulmonary pressure) ? B) During inspiration what are the pressuredifferences? What is the bulk movement of air during inspiration? C)At the endof inspiration what are the intrapleural and intrapulmonary pressures? At the endof inspiration, what is the bulk movement of air? D) During expiration what arethe intrapleural and intrapulmonary pressures? During expiration, what is the bulk movement of air?
6. Define lung compliance and lung elasticity.7. What controls the resistance to air flow through the conducting system8. What controls surface tension?9. What is the compliance of the lungs if a drop of 6 mm Hg in intrapleural pressure
results in the movement of 400 ml of air into the lungs? Compare the ease atwhich lung A and lung B will expand if lung A has a compliance of 100 and lungB has a compliance of 80.
33
-
8/14/2019 Va Respiratory System08
34/35
10. What components within the lungs provide the ability for the lungs to return totheir initial size after being distended during inspiration.?
11. Both alveolus A and alveolus B have a surface tension of 50, but A has a radius of 1 and B a radius of 1.5. Using the Laplace formula, what is the pressure in eachalveoli? If both were connected, which one would expand and which one wouldcollapse? Taken by themselves, which one would be easier to expand (ie. needthe least pressure to expand)?
12. How does surfactant reduce surface tension?13. Alveolus C and alveolus D are situated in a healthy lung and therefore, have the
normal presence of surfactant. If C has a radius of 1 and D a radius of 2, whichone has the greatest concentration of surfactant molecules per unit of surface areain order to prevent one collapsing into the other?
14. How would exercise and the increase in respiration rate and depth increasesurfactant secretion? What cells in the lungs are involved in this secretion?
15. Why do premature babies have a high risk for respiratory distress syndrome?16. Define tidal volume; Vital capacity?17. Person A has a FVC of 5 liters and a FEV1 of 3 liters whereas person B has a
FVC of 4 liters and a FEV1 of 3 liters. What are their FEV1/FVC ratios? Whichone most likely smokes cigarettes?
18. Given their barometric pressure, determine the partial pressure of oxygen at thefollowing locations: Houston (760 mm Hg); Denver (630 mm Hg); Wichita (730mm Hg).
19. Given the following locations in the lungs, which would have the highest P02 andwhich would have the lowest: trachea, bronchi, alveoli? Why?
For questions 20 23, use the following answers:a. 46 mm Hg
b. 40 mm Hgc. 100 mm Hgd. 97 mm Hg
20. PaO2 at rest; at peak exercise.21. PaCO2 at rest; at peak exercise.22. P AO2; P ACO223. PvO2 at rest; PvCO2 at rest.
24. Oxygen saturation of arterial blood is mainly determined by what?25. What two components of blood determine the oxygen carrying capacity of blood?26. A person has a hemoglobin content of 14 gms/dl and a SaO2 of 80. What is the
oxygen carrying capacity of this persons blood?
27. What relationship is represented by the oxyhemoglobin dissociation curve?28. What range of the oxyhemoglobin dissociation curve (ie.,PO2) represents P AO2?
When considering %oxyhemoglobin oxygen saturation, what is unique about thisrange?
29. What range of the oxygemoglobin dissociation curve (PO2) represents the tissuePO2 that surrounds systemic capillary beds? What is unique about this range?
30. Blood, with a Hb content of 14 gms/dl, enters a capillary bed with a PO2 of 93mm Hg and leaves the capillary bed at a PO2 of 40. mm Hg First, using the graph
34
-
8/14/2019 Va Respiratory System08
35/35
on page 22, estimate %oxygen saturation of blood entering and leaving thecapillary bed at the given PO2 (ie., 93 vs 46). Then, from the formula of page 23,determine CaO2 of blood entering and then again leaving the capillary. Howmuch O2, in gms/dl, was unloaded in the capillary bed?
31. This is the same question as #39, but now we will use the graph on page 25.Perform the same calculations but this time use the green saturation curve in thatthe same capillary bed that now has a pH of 7.2. How much oxygen is unloadedat a pH of 7.2? What is the difference in answers between questions 30 and 31and why?
32. In what direction (right or left) does increasing temperature in the capillary bedshift the oxyhemoglobin dissociation curve? Decreasing temperature? What affectdoes this have on the unloading of oxygen into that capillary.
33. In what direction (right or left) does increasing 2,3-DPG in the RBC shift theoxyhemoglobin dissociation curve? What two developments would cause a
persons RBCs to increase its concentration of 2,3-DPG?34. What are the components of the Ventilation/Perfusion ratio? How would
blockage of respiratory bronchi and bronchioles with mucus due to chronic
bronchitits affect this ratio (i.e., increase or decrease it) and why?35. Name and give the locations of the three areas in the brain that control respiration.
How do the I and E neurons in the rhythmicity center work to produce a rhythmic pattern?
36. What controls voluntary breathing? Involuntary breathing?37. Where are the central chemoreceptors located? How are they stimulated? Is it
CO2 or H+ that directly stimulate these receptors?38. Where are the peripheral chemoreceptors located? What directly stimulates these
receptors? What effect does PO2 have on peripheral chemoreceptors?
35