Prof Dr D’Hooghe TM, MD, PhD...(Laufer et al, 1997; Borach et al, 2009; Giudice et al, 2011) •...
62
Transcript of Prof Dr D’Hooghe TM, MD, PhD...(Laufer et al, 1997; Borach et al, 2009; Giudice et al, 2011) •...


Prof Dr D’Hooghe TM, MD, PhD
Leuven University Center for Reproductive Medicine EEL CERTIFIED CLINICAL AND RESEARCH
LEVEL III CENTER OF EXCELLENCE FOR ENDOMETRIOSIS
Society for Endometriosis and Uterine Disorders (SEUD) CONGRESS, PARIS, France, 7 May 2015
Is adolescence a crucial period for endometriosis patients?

Leuven University: founded 1425; 2000 beds

Learning objectives
1. Prevalence of endometriosis in adolescents 2. Prevalence of menstrual cycle related pain
problems in adolescents 3. Early detection: how can we improve timely referral
to endo centers of expertise for adolescents with menstrual cycle related pain problems, resistant to medical management?
4. Can early treatment of adolescent endo prevent adult endometriosis?

• Definition Gynecologic disorder Endometrial-like tissue Outside the uterus (ectopic) Chronic inflammatory reaction Women of reproductive age
• Localization
Pelvis Peritoneum Pelvic organs

• Endo Classification (rAFS, 1997)
Minimal rAFS I
Mild rAFS II peritoneal / ovarian involvement Moderate rAFS III adnexal / cul-de-sac adhesions Severe rAFS IV
• Endo Phenotypes (often co-exist) -Peritoneal -Ovarian Endometrioma -Deeply Infiltrative endometriosis with extension to colorectum, bladder and ureter

Learning objectives
1. Prevalence of endometriosis in adolescents 2. Prevalence of menstrual cycle related pain
problems in adolescents 3. Early detection: how can we improve timely referral
to endo centers of expertise for adolescents with menstrual cycle related pain problems, resistant to medical management to endometriosis.
4. Early treatment of adolescent endo: prevention of adult endometriosis?

Symptoms of adolescent endometriosis (Laufer et al, 1997; Borach et al, 2009; Giudice et al, 2011)
• Pelvic Pain: cyclic or acyclic or combined • Pelvic Pain can be unpredictable, intermittent
o continuous throughout menstrual cycle • Pelvic Pain can be dull/throbbing or sharp,
possibly worse by physical activity • Laparoscopic presentation: traditionally
believed to be mostly peritoneal and subtle lesions


Systematic Review: Prevalence of endometriosis diagnosed by laparoscopy in adolescents Systematic literature search (1980-2012) in PUBMED and EMBASE key words
“endometriosis”, “laparoscopy”, “adolescents” and “chronic pelvic pain (CPP)”
Selected studies: 1014! 89!15 Number of patients: 893 Cave: diagnostic and verification bias (Evers, 2013)

Systematic Review: Prevalence of endometriosis diagnosed by laparoscopy in adolescents
Adolescents with CPP and / or dysmenorrhea, resistant to OCPs / NSAIDs
Prevalence Overall CPP
CPP resistant to OCPs
Dys- menorrhea
P value
Endo 62% (543/880); range 25-100%)
49% (204/420)
75% (237/314)
70% (102/146)
P< 0.001 but NS after meta-regression analysis (MRA)
% Moderate-severe endo (ASRM)
32% (82/259) 57% (44/77)
16% (17/108)
29% (21/74)
P < 0.01 but NS after MRA

LAPAROSCOPIC ASPECTS OF MODERATE-SEVERE ENDO ONLY DESCRIBED IN 4 STUDIES: FULL SPECTRUM • extensive disease: peritoneum, ovaries, tubes and
surrounding structures (Goldstein et al, 1980) • rectal lesions + tubo-ovarian adhesions (Davis et al, 1993) • rectovaginal -, uterovesical -, bowel -and ureteric
endometriosis (Stavroulis et al, 2006). • N=20 (<23 yrs at time of diagnosis) with 14/20 ovarian
endometrioma (5-20 cm), 15/20 adhesions (cul-de-sac, pelvic sidewall) and 1/20 deep nodule.
Advanced vs early stage endo: more random pelvic pain, less daily pelvic pain (Smorgick et al, 2014)
:

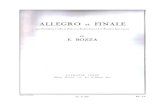
• Clinical presentations Peritoneal endometriosis

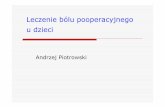
• Clinical presentations Ovarian endometriotic cyst
(endometrioma)

• Clinical presentations Deeply infiltrative endometriosis (DIE)


Systematic Review (Meuleman et al, HRU, 2011): Surgical treatment of DIE with colorectal involvement
Outcome variables
49 studies: bowel resection 32 – mixed 16 3894 patients: bowel resection 73% - full thickness disc excision 10% - superficial surgery 17%
Results
Postoperative complications (major)
94% (46/49) 0% - 43%
Pain 67% (33/49) Mean/median follow-up < 24mths: 17/33 ≠ measuring & reporting symptomatic efficacy Patient based VAS: 6/33
Improvement pain, gynaecologic & digestive symptoms
Quality of life 10% (5/49) ≠ measuring & reporting symptomatic efficacy
Improvement (significant)
Recurrence 43% (21/49) 10% (>2 years follow-up)
bowel: 2,5% / mixed: 5,7%
Fertility 37% (18/49) Number of patients wishing to conceive – time period to conception? Life table analysis: 3/18
24% - 57% Spontaneous: 45% Medically assisted: 55%

Multidisciplinary Surgical Endometriosis Team Leuven University for DIE with colorectal extension
Outcome variables
Retro 1: 9/1996-8/2004
n=56 Multidisciplinary
Response rate: 84%
(47/56) 29 months (6 – 76)
Retro 2: 9/2004-8/2006
n=45 (11%) Bowel resection
Response rate: 67%
(30/45) 27 months (16 - 40)
Prospective: 9/2006-9/2008
n=203 (47%) Moderate: n=67 Severe: n=136
[Bowel resection: n=76 (37%)]
Response rate: 83% (168/203)
19.5 months (1 – 45)
Postoperative complications (major)
5% (3/56) 0% (0/45) 2% (4/203) (bowel: 3% - no bowel: 2%)
Pain p<0,0001 p<0,0001 p<0,0001 Quality of life p<0,0001 p<0,0001 p<0,0001 Reintervent. Recurrence
9% (5/56) 7% (4/56)
11% (5/45) 4% (2/45)
5% (10/203) 4% (8/203)
Fertility 48% (16/33) Spontaneous: 44%
46% (13/28) Spontaneous: 62%
51% (75/148) Spontaneous: 41% (bowel: 58% - no bowel: 42%)

Learning objectives
1. Prevalence of endometriosis in adolescents 2. Prevalence of menstrual cycle related pain
problems in adolescents 3. Early detection: how can we improve timely referral
to endo centers of expertise for adolescents with menstrual cycle related pain problems, resistant to medical management.
4. Early treatment of adolescent endo: prevention of adult endometriosis?

Prevalence of menstrual cycle related pain in 12-year old girls in Flanders, Belgium JOnG! – Policy Research Center of Welfare, Public Health & Family
Large population-based study on characteristics of menstrual cycle and related complaints in young teenage girls at or shortly after menarche. METHODS: Part of larger multidisciplinary cohort study in Flanders,
Belgium; n=792 (age 12.8 ± 0.3 yrs); semi-structured Qaire. RESULTS: Out of 363 girls (47.2%) who had reached menarche: 42% (95%CI: 36 – 47%) reported painful menstruations!

Prevalence of menstrual cycle related pain in 12-year old girls in Flanders, Belgium JOnG! – Policy Research Center of Welfare, Public Health & Family
RESULTS: - Likelihood of dysmenorhea decreased approximately 50% for every
year that age at menarche increased (OR: 0.5; 0.3 - 0.7; p < 0,001).
- Painful menstruation: positively correlated with duration of menstrual flow and amount of blood loss.
- Negative impact of menstruation on social activities: 25%, but
higher (41%) in girls with painful menstruation than in girls without painful menstruation (14%, p < 0.001).

Adolescents N=172 3rd year high school 13-16 years
Young adults N=1028 1st year university 17-21 years
Menstrual Pelvic pain (dysmenorrhea) often/mostly/always often/mostly/always + VAS ≥ 7
40% (68/172) 17% (30/172)
52% (530/1028) 16% (165/1028)
Nonmenstrual Pelvic pain often/mostly/always often/mostly/always + VAS ≥ 7
8,7% (15/172) 2,3% (4/172)
7,6% (78/1028) 2,5% (26/1028)
Impaired QOL during menstruation often/mostly/always
12% (20/172)
11% (113/1028)
Impaired QOL outside menstruation often/mostly/always
1,7% (3/172)
14% (144/1028)
Current use of hormonal contraception 10% (18/172) 66% (681/1028)
Hormonal contraception used as analgesic 44% (8/18) 42% (286/681)
CPP Refractory to OCPs or NSAIDs 4% (7/172) 5% (47/1028)
CPP Refractory to OCPs and NSAIDs 1% (2/172) 3% (31/1028)
Prevalence of complaints suggestive for the presence of endometriosis: adolescents – young adults (Leuven)

Adolescents (n = 172) Young women (n = 1028)
Pre valence
Men strual %
Non-men
strual % Men
strual %
Non-men
strual % LBP >=often or VAS ≥ 7 44 26 25 15 393 38 183 18 LBP >=often and VAS ≥ 7 14 8.1 8 4.7 129 13 75 7.3 At least 1 uro symptom 45 26 1 0.6 234 23 116 11 At least one GI symptom 24 14 19 11 248 24 103 10

Learning objectives
1. Prevalence of endometriosis in adolescents 2. Prevalence of menstrual cycle related pain
problems in adolescents 3. Early detection: how can we improve timely referral
to endo centers of expertise for adolescents with menstrual cycle related pain problems, resistant to medical management of endometriosis.
4. Early treatment of adolescent endo: prevention of adult endometriosis?

Factors associated with development of adult endo (Treloar et al, 2010; Chapron et al, 2011)
• Reduced risk: menarche >= 14 years (Treloar et al, 2010) • Increased risk for endo vs non-endo (Treloar et al, 2010):
Frequent occurrence early dysmen. (OR 2.6, CI 1.1-6.2) • Increased risk DIE versus non DIE (Chapron et al, 2011)
-Positive Family History of endometriosis (OR 3.2; CI 1.2-8.8)
- Increased frequency (OR 4.5; CI 1.9-10.4) and duration (8 +/- 5 versus 5 +/- 4 yrs) of COC use for
severe primary dysmenorrhea - Increased frequency of school absenteism during
menstruation (OR 1.7; CI 1-3)

Development of questionnaire for detection of significant (non)menstrual pain in adolescent girls at risk for endometriosis • SR to identify questionnaires measuring QOL in women and
girls with endo and CPP !selection of 3 questionnaires with highest relevance: EHP 30 Jones et al, 2001; Nnoaham et al, 2009; Parker et al, 2010)
• Analysis of 3 other existing questionnaires previously developed within Leuven University (Hospitals)
• Comparison of the 6 selected questionnaires (3 international, 3 national)
• Development of a new questionnaire (in progress)

Development of questionnaire for detection of significant (non)menstrual pain in adolescent girls at risk for endometriosis
Next steps in development of a new screening questionnaire
as a case finding instrument for adolescents and young adults at risk of endometriosis
1/ validation 2/ integration into routine developmental surveillance practices of health-care workers who take care of adolescent girls 3/ establishment of clinical pathways for referral to endo centers of expertise (D’Hooghe and Hummelshoj, 2006)

The centre/network of expertise (excellence) in endometriosis a framework for long term multi-disciplinary patient management
Surgeons Reproductive endocrinologists
Immunologists Nutritionists
Psychologists/counsellors Pain management
Patient support groups
Nurses
Complementary therapies
WOMAN and
GYNAECOLOGIST
the decision making team
TCM Homeopathy Reflexology Herbalists
Telephone Online Meetings Literature Onsite support
Gynaecological General Bowel Bladder Lung
IVF ICSI IUI
Physiotherapy Massage Acupuncture Stress mgmt Exercise

Communicating endometriosis with young women to decrease diagnosis time (Shadbolt et al, Health Promot J Austr 2013)
Research Question: What do women know/want to know about endometriosis and how is this best communicated? • Online survey for women aged 16-25 yrs (n=131) -52% had heard about endometriosis (but often vague/wrong) -89% thought female teenagers should be educated about it -78% thought young men should be educated about it • Sources of information: - schools (40%), internet (13%), magazines (13%) - talking to doctor (75%), parent (59%) or friend (51%)

Learning objectives
1. Prevalence of endometriosis in adolescents 2. Prevalence of menstrual cycle related pain
problems in adolescents 3. Early detection: how can we improve timely referral
to endo centers of expertise for adolescents with menstrual cycle related pain problems, resistant to medical management to endometriosis.
4. Early treatment of adolescent endo: prevention of adult endometriosis?

TREATMENT OF ENDOMETRIOSIS-ASSOCIATED PAIN
Recommendations

Empirical treatment
Applied to adolescents with presumed endometriosis: INDIVIDUALIZE - Pain killers: paracetamol, NSAIDs - Cyclical combined hormonal contraceptives ! semicontinuous
during 2, 3 consecutive months ! continuous use - Progestins: little data in adolescents

Are hormonal therapies effective for painful symptoms associated with endometriosis?

Are hormonal therapies effective for painful symptoms associated with endometriosis? Hormonal contraceptives

Are hormonal therapies effective for painful symptoms associated with endometriosis? Progestagens and anti-progestagens

LNG IUD use in adolescents (Yoost et al, 2013)
• Retrospect., n=18, 14-22 yrs • IUD placed at time of
diagnostic laparoscopy (n=8) or after surgery + hormonal therapy (mostly GnRHa, n=10)
• Result: pain improvement within 4-5/12 after placement of LNG-IUD, BUT 67% required additional hormonal therapy for suppression of pain and pelvic bleeding

Are hormonal therapies effective for painful symptoms associated with endometriosis? GnRH agonists

Are hormonal therapies effective for painful symptoms associated with endometriosis? Aromatase inhibitors

Are analgesics effective for symptomatic relief of pain associated with endometriosis?

Is surgery effective for painful symptoms associated with endometriosis?

Is surgery effective for painful symptoms associated with endometriosis? Ablation versus excision of endometriosis

Is surgery effective for painful symptoms associated with endometriosis?
Surgical interruption of pelvic nerve pathways

Is surgery effective for painful symptoms associated with endometriosis?
Pain associated with ovarian endometrioma

Is surgery effective for painful symptoms associated with endometriosis?
Pain associated with deep endometriosis


Is untreated endometriosis progressive in adolescents?
• 6/12 (Thomas and Cooke, 1987): 47% deterioration (adults)
• 12/12 (Mahmood and Templeton, 1990): 73% progression/status quo (adults)
(64% progression, 9% status quo) • Beyond 12/12: limited data

AJOG, 1993: progression at 0.3 AFS points per month

BABOON MODEL FOR ENDOMETRIOSIS • Spontaneous endometriosis is a progressive
disease when followed by laparoscopies every 6 months during 2 years (D’Hooghe et al, 1996b)
• Baboons with an initially normal pelvis develop in 64% histologically proven minimal endometriosis after 32 months as assessed by laparoscopies every 6 months
(D’Hooghe et al, 1996c) • Increased duration of captivity --> increased
prevalence of endometriosis (D’Hooghe et al, 1996a)

Surgery useful in adolescents? We do not know!
• Only retro- (n=3) or prospective (n=1) case series • NO case control/contr.cohort/randomized studies • Effect surgery: some improvement, but often
recurrence/persistence of pain and about 50% require repeat surgery(Yeung et al, 2011)
• Postoperative hormonal suppression: – If not: progression reported (3 cases; Unger, 2011) – If treated: persistence/recurrence of pain (Doyle, 2009) and
significant side effects (Kaser et al, 2012) leading to compliance problems (Unger, 2011)

Endo progression in non-medically managed adolescents (Unger and Laufer, JPAG, 2011)
• Retrospective case series (n=3, 13-16 yrs) • Presenting symptom: pelvic pain resistant to continuous (n=2)
or cyclic (n=1) COC and painkillers • Diagnostic/operative laparoscopy: minimal endo (ASRM,
1997) • Postoperative hormonal suppression therapy:
noncompliance due to side effects (depression, irregular bleeding, fatigue)
• Repeat laparoscopy for recurrence AND worsening of pelvic pain: progression to severe (n=2) or mild (n=1) endo, with DIE (n=1), endometrioma (n=1), diaphragmatic endo (n=1)

Combined Surgical-Medical Intervention retards disease progression in adolescents receiving hormonal suppression (Doyle et al, JPAG, 2009) BUT MAY NOT IMPROVE PAIN
• Retrospective case series (n=90, median 7 (12-24) yrs at initial lap)
• Inclusion criterium: pain exacerbation after Lap 1 during hormonal suppression requiring Lap 2
• Operative Laparoscopy 1 (for pelvic pain resistant to hormonal suppression and NSAIDs):
Median Minimal Endo (Range Minimal-Moderate Endo)

Combined Surgical-Medical Intervention retards disease progression in adolescents receiving hormonal suppression (Doyle et al, JPAG, 2009) BUT MAY NOT IMPROVE PAIN
• Postoperative hormonal suppression in all patients (91% continuous COC, 78% GnRHa + add-back, 12% POP)
• Lap 2 (n=90, median 29/12 after Lap 1): Endo stage: no change (70%), improvement (19%),worsening (10%)
• Lap 3 (n=33, median 27/12 after Lap 2): Endo stage: no change (70%), improvement (3%) or worsening (9%)

Postop Norethindrone Acetate (5-15 mg) may be useful for young women resistant to other medical treatment (Kaser et al, JPAG, 2012) BUT SEs • Retrospective case series (n=194, median 19 years,
minimal-mild endo, only pts treated with NA alone postoperatively)
• Indication for postop NA: persistent pain or bleeding on COC (57%), or GnRHa +NA (9%), or CI for E2 use (27%)
• Significant improvement in pain scores for all patients except those previously prescribed GnRHa + addback
• Significant improvement in bleeding scores for all patients
• ! 45% significant side effects: weight gain (46%), acne (10%), mood lability (9%), vasomotor instability (8%)

Effect of complete laparoscopic excision of endo in teenagers (Yeung et al, FS, 2011): ABOUT HALF REPEAT SURGERY WITHIN 23 MONTHS • Prospective case series of teenagers (n=17, 12-19 yrs) with
laparoscopically and histologically confirmed endometriosis • Operative Laparoscopy (pain suspicious for endo):
minimal (29%), mild (65%) or moderate (6%) endo • Outcome measure: Rate of recurrent/persistent endometriosis after
complete laparoscopic excision • Follow-up (median 23/12): only 1/3 (7/17) postop temporary hormonal
suppression at own initiative (no subanalysis) • Pre-post comparison: improvement for dysmenorrhea, dyschezia,
painful bladder, QOL, … but not for CPP or dyspareunia • 47% repeat surgery for persistent or recurrent pain: NO ENDO, half
pelvic adhesions, half resection abnl peritoneum (Endo neg.)

FIRST: WELL DESIGNED PROSPECT. CASE SERIES Clinical outcome assessment of adolescent endometriosis
Electronic file + Questionnaire (before/after design)
prospective: 1 month preoperative 6 / 12 / 18 / 24 months postoperative
• Postoperative complications:
• Pain: patient centered VAS: dysmenorrhea, deep dyspareunia, Nonmenstrual pain
• Quality of life: patient centered EHP30 (Jones, 2001)
• Reintervention Recurrence: Histological confirmation!
• Future Fertility outcome: Life table analysis

Conclusions
1. Prevalence of endometriosis in adolescents with pelvic pain resistant to COCs/painkillers: 62% (1/3 with moderate-severe endo!)
2. Prevalence of dysmenorrhea in adolescents:
- 42% (13 yrs), 40% (15-17 yrs), 52% (18-19yrs) - associated with reduced QOL (40% 13yr olds) - resistant to COCs or NSAIDs: 4-5%

Conclusions
3. Early detection: validated questionnaire needed for primary health care professionals/ school doctors to improve timely referral of adolescents with menstrual cycle related pain problems, resistant to medical management to endometriosis, to endo centers of expertise.

Conclusions
4. Can early treatment of adolescent endo prevent adult endometriosis? Unknown, No valid research. Complex: pt compliance (SE medication)? pain recurrence = not always endo recurrence? Start with well designed prospective case series with predefined PRO !controlled cohort studies !RCTs

Leuven University Center for Reproductive Medicine EEL CTFIED CLINICAL/ RESEARCH CENTER OF EXCELLENCE FOR ENDOMETRIOSIS
Gynaecology
T D’Hooghe
C Meuleman
D. De Neubourg
K Peeraer
C Tomassetti S Pelckmans P De Loecker L Segal L. Meeuwis
A Spaepen
I Thijs
Paramedical staff
E Bakelants
H De Bie
K Dhondt J Gevaerts M. Vandersanden
S Kurstjens
K Lerut
L Magis
L Rijkers
S Schildermans
H Verbiest
S Verschueren S. Dewil
F Clinckemalie
W Leus G Roels
M Toetenel
Andrology
D Vanderschueren
Ph Marcq Urology
D Deridder G Bogaert F Vanderaa
Psychology and Counselling
K Demyttenaere P. Enzlin
U. Vandenbroeck L. Van Moppes
M Vervaeke
Fertility Lab
C Spiessens
S Debrock
G Bertin
D Willemen H Devroe
H Afschrift
O De Maeght
L Hollanders
A Velaers
F Vynckier
P Bols
E Vergison
K Bullens
B Quintens
Center for Medical Genetics
JP Fryns
E Legius T de Ravel de L’Argentière
Research coördinator
M Welckenhuysen
Gastro enterological surgery
A. D’Hoore P. Wolthuis

Leuven Endometriosis Research Group/Network: 8 PhD students
Clinical Leuven
GYN T D’Hooghe
C Meuleman
C. Tomassettii
K Peeraer
L. Meeuwis S Pelckmans P De Loecker L. Segal URO B. VCleynenbreugel GE surgery A D’Hoore A.Wolthuis
Research Nairobi J Mwenda D Chai
N Kulia E Omolo Veterinary staff Animal attendants
Postdocs Leuven A Fassbender, C. Meuleman
International collaborators D. Lebovic (Ann Arbor, USA) H. Taylor (Yale, USA) H. Falconer (Karolinska, Stockholm, SE) G. Dunselman (Maastricht, NL) A. Sharkey (Cambridge, UK) P Saunders (Edinburgh, UK) A. Bokor (Budapest, HUN) K. Coleman (Oregon Primate Center, USA) World Endometriosis Research Foundation EU Network for Endometriosis (ENE)
PhD Students Leuven-Nairobi C. Kyama
PhD Students Leuven A Vodolazkaia
D. Peterse C Tomassetti E. Dancet PhD Students Leuven – int’ntl P Simsa (Budapest) A Bokor (Budapest) H Falconer (Karolinska)
Leuven Research coördinator M Welckenhuysen
Clinical Nairobi
D Chai