Leri Disease – case report of uncommon...
4
Chir. Narzadow Ruchu Ortop. Pol., 2019; 84(3) 97-100 DOI: 10.31139/chnriop.2019.84.3.19 97 © Polskie Towarzystwo Ortopedyczne i Traumatologiczne Chirurgia Narządów Ruchu i Ortopedia Polska / Polish Orthopaedics and Traumatology ISSN 0009-479X Author’s address: Barbara Igielska-Bela, Specialistic Hospital in Koscierzyna, Orthopedic Department Piechowskiego 36, 83-400 Kościerzyna, Poland; phone: +48 586860553; e-mail: [email protected] Received: 10.06.2019 Accepted: 22.06.2019 Published: 30.06.2019 CASE REPORT Leri Disease – case report of uncommon disease Choroba Leri’ego – opis przypadku Barbara Igielska-Bela, Marek Krzemiński Orthopedic Department, Specialistic Hospital in Koscierzyna Abstract Introduction. Leri disease (synonyms: melorheostosis, candle bone disease, melting wax syndrome) is a rare disease which affect bones, first described in 1922 by Leri and Joanny. The disease can be asymptomatic or manifested by severe pain of the limbs. A radiological feature is the increasing density of the bone structure resembling wax flowing from a candle. Case report. A 27-year-old Caucasian female presented with pain of her upper limb, a deformation of the limb and with a limitation of the active and pas- sive range of motion of the joints. The x-rays showed irregular cortical sclerosis resembling wax that has dripped down the side of the candle. The analgetics were given to the patient. The patient has also underwent a surgical treatment. Conclusions. The Leri disease is diagnosed based on the typical candle wax x-ray changes. There is no causative treatment. The treatment with bisphospho- nates and physiotherapy can bring results. The surgical treatment does not help in relieving pain. Key words: Leri disease, melorheostosis, candle wax syndrome Streszczenie Wstęp. Choroba Leriego (synonymy: meloreostoza, choroba kapiącej świecy) jest rzadko spotykanym schorzeniem kości, opisanym po raz pierwszy w 1922 przez Leri I Joanny. Choroba może przebiegać bezobjawowo lub z bólami kończyn. Radiologicznie widoczne są pasmowate zagęszczenia struktury kostnej o nierównym falistym zarysie (objaw kapiącej świecy), rozciągające się wzdłuż osi długiej kości. Opis przypadku. 27 letnia pacjentka z silnymi dolegliwościami bólowymi kończyny górnej prawej, z deformacją i ograniczeniem ruchomości w stawach. Zdjęcia radiologiczne uwidoczniły zagęszczenie struktury kostnej oraz objaw kapiącej świecy. Pacjentka otrzymywała leczenie przeciwbólowe. Wykonano także zabieg resekcji nadmiaru kości. Wnioski. Choroba Leri’ego rozpoznawana jest na podstawie charakterystycznego obrazu radiologicznego. Nie ma leczenia przyczynowego choroby. W leczeniu pomocna może być fizjoterapia oraz bisfosfoniany. Leczenie operacyjne nie łagodzi bólu. Słowa kluczowe: choroba Leri’ego, meloreostoza, choroba kapiącej świecy
Transcript of Leri Disease – case report of uncommon...

Chir. Narzadow Ruchu Ortop. Pol., 2019; 84(3) 97-100 DOI: 10.31139/chnriop.2019.84.3.19
97© Polskie Towarzystwo Ortopedyczne i Traumatologiczne
Chirurgia Narządów Ruchu i Ortopedia Polska / Polish Orthopaedics and Traumatology
ISSN 0009-479X
Author’s address: Barbara Igielska-Bela, Specialistic Hospital in Koscierzyna, Orthopedic Department Piechowskiego 36, 83-400 Kościerzyna, Poland; phone: +48 586860553; e-mail: [email protected]
Received: 10.06.2019Accepted: 22.06.2019Published: 30.06.2019
CASE REPORT
Leri Disease – case report of uncommon disease
Choroba Leri’ego – opis przypadku
Barbara Igielska-Bela, Marek Krzemiński
Orthopedic Department, Specialistic Hospital in Koscierzyna
Abstract
Introduction. Leri disease (synonyms: melorheostosis, candle bone disease, melting wax syndrome) is a rare disease which affect bones, first described in 1922 by Leri and Joanny. The disease can be asymptomatic or manifested by severe pain of the limbs. A radiological feature is the increasing density of the bone structure resembling wax flowing from a candle.Case report. A 27-year-old Caucasian female presented with pain of her upper limb, a deformation of the limb and with a limitation of the active and pas-sive range of motion of the joints. The x-rays showed irregular cortical sclerosis resembling wax that has dripped down the side of the candle. The analgetics were given to the patient. The patient has also underwent a surgical treatment.Conclusions. The Leri disease is diagnosed based on the typical candle wax x-ray changes. There is no causative treatment. The treatment with bisphospho-nates and physiotherapy can bring results. The surgical treatment does not help in relieving pain.
Key words: Leri disease, melorheostosis, candle wax syndrome
Streszczenie
Wstęp. Choroba Leriego (synonymy: meloreostoza, choroba kapiącej świecy) jest rzadko spotykanym schorzeniem kości, opisanym po raz pierwszy w 1922 przez Leri I Joanny. Choroba może przebiegać bezobjawowo lub z bólami kończyn. Radiologicznie widoczne są pasmowate zagęszczenia struktury kostnej o nierównym falistym zarysie (objaw kapiącej świecy), rozciągające się wzdłuż osi długiej kości.Opis przypadku. 27 letnia pacjentka z silnymi dolegliwościami bólowymi kończyny górnej prawej, z deformacją i ograniczeniem ruchomości w stawach. Zdjęcia radiologiczne uwidoczniły zagęszczenie struktury kostnej oraz objaw kapiącej świecy. Pacjentka otrzymywała leczenie przeciwbólowe. Wykonano także zabieg resekcji nadmiaru kości.Wnioski. Choroba Leri’ego rozpoznawana jest na podstawie charakterystycznego obrazu radiologicznego. Nie ma leczenia przyczynowego choroby. W leczeniu pomocna może być fizjoterapia oraz bisfosfoniany. Leczenie operacyjne nie łagodzi bólu.
Słowa kluczowe: choroba Leri’ego, meloreostoza, choroba kapiącej świecy

Chir. Narzadow Ruchu Ortop. Pol., 2019; 84(3) 97-100
98© Polskie Towarzystwo Ortopedyczne i Traumatologiczne
Chirurgia Narządów Ruchu i Ortopedia Polska / Polish Orthopaedics and Traumatology
Barbara Igielska-Bela and Marek Krzemiński: Leri Disease – case report of uncommon disease
CASE REPORT
Introduction
Leri disease (synonyms: melorheostosis, candle bone disease, melting wax syndrome) is a rare disease which affect bones, first described in 1922 by Leri and Joanny [1]. It has sporadic characteristic. The changes concern both sexes. No heredi-tary features have been discovered. The disease can be as-ymptomatic or manifested by severe pain [1-3]. The changes are located in the bones of the limbs, usually one-sidedly. The most common part of the bone is diaphysis of the long bone of lower limb less often the axial skeleton [1-3]. A radiologi-cal feature is the increasing density of the bone structure re-sembling wax flowing from a candle [1-3].
The authors present a rare case of melorheostosis of the bones of the right upper limb.
Case report
A patient J.W., a 27-year-old Caucasian female, was admitted to the Orthopedic Department, with pain of her upper limb, a deformation of the limb and with a limitation of the active and passive range of motion of the joints, especially of the ra-diocarpal joint. The dorsal flexion of the joint was 50 degrees, and the volar flexion was about 60 degrees. The affected limb was thickened and slightly distorted.
The general history of the patient revealed melorheosto-sis. She did not give any history of an injury of her upper limb in the past. The patient has worked as a teacher.
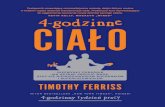
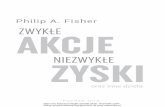
The disease started when the patient was 15 years old with severe pain of the right upper limb without changes on the x-ray. During the diagnosing process she underwent CT scans of the upper limb, scintigraphy and genetic examina-tions. The diagnose was Leri disease. Two years after the first pain symptoms there were changes on x-ray. Firstly, it was the a deformation and sclerosis of the radius and the second and the third hand ray (Fig. 1). Three years later there were typical structures resembling wax flowing from the candle (Fig. 2, 3 and 4). The skin was normal. Laboratory findings for serum calcium, phosphorus, C-reactive protein and alka-line phosphatase were within normal limits.
According to the fact that it is a disease entity of an un-known etiology, there is no causative treatment. For this rea-son, the only treatment for the patient was analgesia. Ordi-nary painkillers did not help, so she was administered opioid medicines. She began to develop addiction to them, therefore the decision was made to remove the excess bones surgically.
The excess bone was surgically removed from the dor-sal surface of the distal phalanx of the III finger, the second metacarpal bone and the radius bone. During the operation, an atypical location of the anatomical structures was found,
Fig. 2. An AP x-ray of the patient’s right hand, the deformation and sclero-sis of the bones of II and III rays.
Fig. 1. The first radiological symptoms – deformation and sclerosis of the second and the third hand ray.
Fig. 3. A lateral x-ray of the patient’s right forearm, the deformation of the radius.

Chir. Narzadow Ruchu Ortop. Pol., 2019; 84(3) 97-100
99© Polskie Towarzystwo Ortopedyczne i Traumatologiczne
Chirurgia Narządów Ruchu i Ortopedia Polska / Polish Orthopaedics and Traumatology
Barbara Igielska-Bela and Marek Krzemiński: Leri Disease – case report of uncommon disease
CASE REPORT
sub periosteal bone formation. Other symptoms are the limi-tation of movement and deformity of the joints, and hyperpig-mentation of the overlying skin or/and scleroderma. The signs and symptoms usually appear in childhood or adolescence [1-3]. Leri disease can be an independent disorder or can be a part of Buschke-Ollendorff syndrome, which is characterized by osteopoikilosis, connective tissue nevi and also can include melorheostosis [3,4].
Melorheostosis may be associated with tumors such as os-teosarcoma or malignant fibrous histocytoma [5,7]. Melorheos-tosis can affect one or multiple bones, or, which is the most com-mon form, can be monomelic. The aetiology of this disease is still unknown. There are several hypotheses explaining the cause of the disease [8]. In 1979 Murray and McCredie suggested that an embryonic nerve root infection leads to neural scarring and segmental bone sclerosis [9]. Kim J-E et al. (2000) showed that in melorheostosis in the regulation of osteoblasts, there is a low-er involvement of adhesion proteins, especially transforming growth factor β induced gene product [10]. In 2004 Hellemans et al. [11] and in 2007 Mumm et al. [12] described a possible aetiology in mutation of the LEMD3 gene (12q12-12q14.3), a protein that interacts with BMP and TGF β signalling. Such hypotheses may confirm the genetic basis of this rare disease. However, further research on this matter should take place to solve the mystery of aetiology and help to determine the pos-sible role of genetic therapy in treating this disorder.
Melorheostosis does not cause changes in standard labora-tory tests or specific changes in a histopathological examination.
The treatment can be nonopertaive and operative. Majority of the patients receive symptomatic treatment. The operative treatment includes the excision of hyperostotic bone, osteoto-mies, sympathectomy or even amputation.
There are reports of effective treatment with bisphospho-nates. In Leri disease the bone pain is probably connected with osteoclastic bone resorption and the activation of pain recep-tors, increased intraosseous pressure and vascularity as a re-sult of hyperostosis. Bisphosphonates inhibit osteoclastic bone resorption by a number of mechanisms on bone vascularity or cells such as osteoblasts and macrophages. Their effects on re-ducing bone pain and deceleration of bone lesions have been shown [6,13,14].
The Leri disease has a chronic, slow nature. However, there may be periodic exacerbations. After operative excisions of hy-perostotic bone, recurrence can be expected [15].
Conclusion
The Leri disease is diagnosed based on the typical candle wax x-ray changes. There is no causative treatment. The treatment with bisphosphonates and physiotherapy can bring results.
Fig. 4. An x-ray of the humerus – the typical structures resembling wax flowing from the candle.
Fig. 5. An intraoperative photo – arrow: the II metacarpal bone, star: the intrinsic muscles.
especially in the intrinsic muscles and the vaso-nerve bunch-es (Fig. 5). Physiotherapy was administered the day after op-eration. A three-month-follow-up showed a little reduction of the hand deformity, but unfortunately the pain remained.
Discussion
Leri disease is a chronic bone disease, which is very rare. It was first described by Leri in 1922 [1-3]. The frequency is 0,9/1 000 000. There are no hereditary features and both sexes can be af-fected. The first symptom is a pain which is connected with a
Fig. 4. An x-ray of the humerus – the typical structures resembling wax flowing from the candle.
Fig. 5. An intraoperative photo – arrow: the II metacarpal bone, star: the intrinsic muscles

Chir. Narzadow Ruchu Ortop. Pol., 2019; 84(3) 97-100
100© Polskie Towarzystwo Ortopedyczne i Traumatologiczne
Chirurgia Narządów Ruchu i Ortopedia Polska / Polish Orthopaedics and Traumatology
Barbara Igielska-Bela and Marek Krzemiński: Leri Disease – case report of uncommon disease
CASE REPORT
References
1. Leri A, Joanny J: Une affection non décrite des os hyperostose “en coulée” sur toute la longeur d’un member ou “melorhéostose”. Bull Mem Soc Med Hosp Paris. 1922;46:1141-1145.
2. Greenspan A, Azouz EM: Bone dysplasia series: melorheostosis: review and update. Can Assoc Radiol J. 1999;50:324-330.
3. Kumar R, Sankhala S, Bijarnia I: Melorheostosis – case report of rare disease. JOCR. 2004;4(2): 25-27.
4. Akinci A, Dundar I, Sigirci A: The treatment of severe pain in melorhe-ostosis with daily walking program only: a case report. Bone Abstracts. 2017;6:P183, doi:10.1530/boneabs.6.P183.
5. Baer SC, Ayala AG, Ro JY et al.: Case report 843. Malignant fibrous histiocytoma of the femur arising in melorheostosis. Skeletal Radiol. 1994;23:310.
6. Hollic RJ, Black A, Reid D: Melorheostosis and its treatment with intravenous zoledronic acid. BMJ Case Reports. 2010. doi:10.1136/bcr.04.2009.1757.
7. Murphy M, Cavanagh M, Hurson B, et al.: Occurrence of osteosarcoma in melorheostostic femur. Ir Med J. 2003;96:55-56.
8. Morris JM, Samilson RL, Corley CL: Melorheostosis. Review of the lit-erature and report of an interesting case with nineteen year follow up. J Bone Joint Surg. 1963;45A:1191-2000.
9. Murray RO, McCredie J: Melorheostosis and the sclerotomes: a radio-logical correlation. Skeletal Radiol. 1979;4:57-71.
10. Kim J-E, Kim E-H, Han E-H, et al.: A TGF-β-inducible cell adhesion molecule, βig-h3, is downregulatedin meloreosthosis and involved in osteogenesis. J Cell Biochem. 2000;77:169-78.
11. Hellemans J, Preobrazhenska O, Willaert A, et al.: Loss-of-function mutations in LEMD3 result in osteopoilikosis, Buschke-Ollendorff syndrome and melorheostosis. Nat Genet. 2004;36:1213-1218.
12. Mumm S, Wenkert D, Zhang X, et al.: Deactivating germline mutations in LEMD3 cause osteopoikilosis and Buschke-Ollendorf syndrome, but not sporadic melorheostosis. J Bone Miner Res. 2007;22:243-250.
13. Donath J, Poor G, Kiss C, et al.: Atypical form of active melorheostosis and its treatment with bisphosphonate. Skeletal Radiol 2002;31:709-13.
14. Wood J, Bonjean K, Ruetz S, et al.: Novel antiangiogenic effects of the bisphosphonate compound zaledronic acid. J Pharm Experimental Therapeutics. 2002;302:1055-61.
15. Goldman AB, Schneider R, Huvos AS, et al.: Case report 778. Melorhe-ostosis presenting as two soft-tissue masses with osseous changes lim-ited to the axial skeleton. Skeletal Radiol. 1993; 22:206-210.














![CandidateUrinePeptideBiomarkersforIgANephropathy:Where Are ...downloads.hindawi.com/journals/dm/2018/5205831.pdf · IgA nephropathy [23]. In most cases, the disease progresses over](https://static.fdocuments.pl/doc/165x107/6001a071e3df3036ef36cc5d/candidateurinepeptidebiomarkersforiganephropathywhere-are-iga-nephropathy-23.jpg)