Bule Stephen Cit Masters Report

of 81
-
Upload
edwinclifford -
Category
Documents
-
view
227 -
download
0
Transcript of Bule Stephen Cit Masters Report
-
7/30/2019 Bule Stephen Cit Masters Report
1/81
EVALUATION OF THE IMPACT OF WIRELESS COMMUNICATION
TECHNOLOGIES; A CASE STUDY IN HEALTHCARE SERVICE
By
BULE STEPHEN
Reg.No:2005/HD18/637U
BSc Rad(UJ), PgDip US(USA), DMR (Mak)
[email protected]/[email protected]/+256-772-441304
A Project Report Submitted to
the School of Graduate Studies in Partial Fulfilment of
the Requirements for the Award of a Master of Information Technology ofMakerere University
Option: Information Technology Management
October, 2007
-
7/30/2019 Bule Stephen Cit Masters Report
2/81
Declaration
I, Stephen Bule do hereby declare that this Project Report is original and has not been published
and/or submitted for any other degree award to any other University before.
Signed....................................................... Date.....................................................
Bule Stephen, MSc.
Department of Information Technology
Faculty of Computing and Information Technology
Makerere University
Approval
This Project Report has been submitted for Examination with the approval of the following super-
visor(s).
Signed:....................................................... Date:....................................................
Dr.Patrick Ogao, PhD
Department of Information Systems
Faculty of Computing and Information Technology
Makerere University
Signed:........................................................ Date:....................................................
Mr.Drake Mirembe, MSc.
Department of Networks
Faculty of Computing and Information Technology
Makerere University
-
7/30/2019 Bule Stephen Cit Masters Report
3/81
Dedication
I dedicate this work to my family espcially my wife Susan ,and sons Nicholas and Philip who have
been patient and supportive during this period. Lastly, I also dedicate my work to my Dad Stephen
who has always given me call when I least expect.
ii
-
7/30/2019 Bule Stephen Cit Masters Report
4/81
Acknowledgement
I would like to acknowledge the following people without whose help and contribution to this work
would never have come this far.
These are Dr.Patrick Ogao, my committed supervisor from the faculty who has indeed been very
helpful and kept me stay on track all along and particularly so for his valuable time. Associate Pro-
fessor.Micheal Kawooya my mentor and co-supervisor who has willingly encouraged me to pursue
this course and supported me in the radiology department where I work. Not-with-standing I do
acknowlodge the tireless contribution of Mr.Drake Mirembe my Assistant superior to this work at
the Faculty who assimilated and introduced me to the health informatics group/ club at the faculty
of computing and Information Technology. In the same breadth I would wish to thank Prof.Janet
Aisbett of Newcastle University, Australia for her vital and timely contribution in critiquing this
work.
Special commendations go to my memebers of radiology department in Mulago Hospital espe-
cially the acting head of department, Dr.Rosemary Byanyima, Mr.Mpiima Patrick, Principle Imag-
ing Technologist assessment centre radiology suite and Dr.Faith Ameda, Radiology Postgraduate
student for their encouragement, contribution and moral support.
My thanks also goes to the staff of the faculty of Computing and IT that created a conducive
environment that made it possible for me to complete this study in time.
Lastly I wish to thank the staff at Mulago Hospital at various departments of Radiology, Medicine,
Surgery, Pathology, Obstretrics and Gynaecology, Physiotherpy, Nursing and medical school for
the support given to this study survey
Finally, I thank myself for my personal efforts and also to the Almight God for his superb wis-
dom.
iii
-
7/30/2019 Bule Stephen Cit Masters Report
5/81
Contents
Declaration . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . i
Dedication . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ii
Acknowledgement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . iii
Abbreviations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . xi
Abstract . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . xii
1 INTRODUCTION 1
1.1 Background . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
1.2 Statement of the Problem . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
1.3 Main objectives . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
1.3.1 Specific Objectives . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
1.4 Scope of the Study . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
1.5 Significance of the study . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
2 LITERATURE REVIEW 5
2.1 Wireless technologies and Healthcare . . . . . . . . . . . . . . . . . . . . . . . . 5
iv
-
7/30/2019 Bule Stephen Cit Masters Report
6/81
2.2 Application of wireless technology in healthcare . . . . . . . . . . . . . . . . . . . 8
2.3 Measuring attitudes to technology and quality of service . . . . . . . . . . . . . . 9
2.4 UTAUT and SERVQUAL Models. . . . . . . . . . . . . . . . . . . . . . . . . . . 9
3 METHODOLOGY 11
3.1 Overview . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
3.2 Research Design . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
3.3 Study Area . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
3.4 Study Population . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
3.5 Validity and Reliability . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
3.6 Procedure of Data Collection . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
3.7 Data Analysis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
3.8 Ethical Considerations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
4 PRESENTATION AND FINDINGS. 14
4.1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
4.2 Developing questionnaire . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
4.3 Findings and characteristics of healthcare professionals. . . . . . . . . . . . . . . . 21
4.3.1 Analysis of the questionnaire by relationship . . . . . . . . . . . . . . . . 21
4.3.2 Validity and reliability . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22
4.3.3 Characterictics of Healthcare professionals. . . . . . . . . . . . . . . . . . 23
v
-
7/30/2019 Bule Stephen Cit Masters Report
7/81
4.3.4 Available wireless communication technologies . . . . . . . . . . . . . . . 25
4.3.5 Ownership of the wireless information communication technologies . . . . 26
4.3.6 Current state of use or expected time of use . . . . . . . . . . . . . . . . . 27
4.4 Deployment environment of the wireless communication technologies . . . . . . . 29
4.4.1 Regulatory policies in healthcare centres . . . . . . . . . . . . . . . . . . 29
4.4.2 National laws covering use of wireless technologies . . . . . . . . . . . . . 29
4.4.3 Lack of funding . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29
4.4.4 Changing technologies . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30
4.4.5 Availability of support personal . . . . . . . . . . . . . . . . . . . . . . . 30
4.5 Limitations of the Study . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31
4.6 The attitudes of the respondents in determining the level of technology acceptance
by the healthcare professionals . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32
4.6.1 Usefulness to job . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33
4.6.2 Enables quick accomplishment . . . . . . . . . . . . . . . . . . . . . . . . 33
4.6.3 Productivity increase . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34
4.6.4 Skilled to perform job . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34
4.6.5 Work more interesting . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34
4.7 The perception of respondents to determine the service quality when using wireless
information communication technologies. . . . . . . . . . . . . . . . . . . . . . . 34
4.7.1 Same level of healthcare services . . . . . . . . . . . . . . . . . . . . . . 35
4.7.2 Respond faster to fix problem . . . . . . . . . . . . . . . . . . . . . . . . 35
vi
-
7/30/2019 Bule Stephen Cit Masters Report
8/81
4.7.3 More care and consideration to patients . . . . . . . . . . . . . . . . . . . 36
4.7.4 Easier communication to healthcare professionals . . . . . . . . . . . . . . 36
4.7.5 Patient information more secure . . . . . . . . . . . . . . . . . . . . . . . 36
4.8 Summary of Findings . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 37
5 CONCLUSION AND RECOMMENDATIONS. 41
5.1 Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 41
5.2 Recommendations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 43
5.3 Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 44
REFERENCES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 46
APPENDIX 1 QUESTIONNAIRE . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 50
APPENDIX 2 CHI-SQUARE VALUES . . . . . . . . . . . . . . . . . . . . . . . . . . 56
vii
-
7/30/2019 Bule Stephen Cit Masters Report
9/81
List of Tables
4.1 Shows the Technology acceptance model using UTAUT technique . . . . . . . 15
4.2 Shows the SERVQUAL 10 dimensions used in healthcare service . . . . . . . . 19
4.3 Percentage distribution of the respondents according to background charac-
teristics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23
4.4 Brief background of the respondents . . . . . . . . . . . . . . . . . . . . . . . . 25
4.5 Shows the percentage distribution of the wireless technologies whether cur-
rently in use or expected to be used . . . . . . . . . . . . . . . . . . . . . . . . 28
4.6 Shows the Percentage distribution of the respondents according to the de-
ployment environment of the wireless technologies . . . . . . . . . . . . . . . . 39
4.7 Shows the percentage distribution of the respondents according to the per-
ception of the healthcare professionals to the delivery of quality healthcare
services . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 40
viii
-
7/30/2019 Bule Stephen Cit Masters Report
10/81
List of Figures
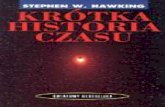
4.1 Shows the Relationships and Chi-Square value . . . . . . . . . . . . . . . . . . 22
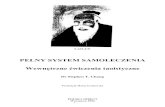
4.2 Shows the gender of respondents. . . . . . . . . . . . . . . . . . . . . . . . . . 24
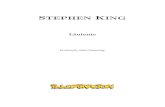
4.3 Shows Available wireless communication technologies . . . . . . . . . . . . . . 26
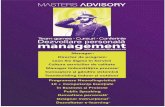
4.4 Shows Ownership of the wireless information communication technologies . . 27
4.5 Shows Percentage of usage of the wireless technologies . . . . . . . . . . . . . . 28
4.6 Shows responses on deployment environment of the wireless technologies . . . 31
4.7 Shows dimensions of technology acceptance by healthcare professionals . . . . 33
4.8 Shows Components of service Quality in healthcare service by using wireless
technologies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 35
5.1 Shows Resource necessary to use vs new technology making health centre look
modern . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 56
5.2 Shows Time to complete all tasks vs same level of healthcare . . . . . . . . . . . 57
5.3 Shows Being able complete task alone vs Faster response to fis problem . . . . . . 58
5.4 Shows Patient treated with care and consideration vs management supportive . . . 59
5.5 Shows Competence of healthcare provided vs technology acceptance . . . . . . . . 60
ix
-
7/30/2019 Bule Stephen Cit Masters Report
11/81
5.6 Shows the valuing of patients by healthcare professionals vs the technology . . . . 61
5.7 Shows skilledness to use technology vs competence in providing healthcare . . . . 62
5.8 Shows the reputation of healthcare centre vs quick accomplishment of the work . . 63
5.9 Shows the reliability of patient information source vs quick accomplishment of the
job . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 64
5.10 Shows the reliability of patient information source vs helpfulness of management . 65
5.11 Shows ease of patient communication vs technology acceptance . . . . . . . . . . 66
5.12 Shows the cost of healthcare vs quick accomplishment of the work . . . . . . . . . 67
5.13 Shows the cost of healthcare vs helpfulness of senior management . . . . . . . . . 68
x
-
7/30/2019 Bule Stephen Cit Masters Report
12/81
LIST OF SYNONYMS/ABBREVIATIONS
WICT - Wireless Information and Communication Technology
HIMSS - Healthcare Information and Management Systems society
Wi-Fi - Wireless Fidelity
ICT - Information and Communications Technology
IS - Information System
IT - Information Technology
PDA - Personal Digital Assistant
NHS - National Health Service
LAN - Local Area Network
SAN - Storage Area Network
WAN - Wide Area Network
WISP - Wireless Internet Service Provider
PAN - Personal Area Network
WLAN - Wireless Local Area Network
WWAN - Wireless Wide Area Network
SERVQUAL - Service Quality
TAM Technology Acceptance Model
UTAUT - Unified Theory in Acceptance and Use of Technilogy
xi
-
7/30/2019 Bule Stephen Cit Masters Report
13/81
Abstract
Healthcare industry is ever increasing the use of new information and communication technology.
The use of wireless information communication technology offers a successful adoption in health-
care for developing countries with relatively poor communication infrastructure.
In Uganda some healthcare centres have deliberately deployed wireless information communi-
cation technologies like PDAs, Mobile phones, and teleradiology to improve healthcare. About
50 percent of new capital investments in organisations are on IT, yet they have to be accepted and
used by employees to improve productivity. This is a concern to IT managers.
The main aim of this study is to evaluate the perceived effectiveness of wireless information com-
munication technologies on healthcare delivery by healthcare professionals.
The following are the objectives: to investigate the deployment environment of wireless informa-
tion technologies in healthcare service, to evaluate the attitudes of the health professionals to the
deployment of wireless information communication technologies, to evaluate the perception of
health professionals on the effect of the deployment of wireless communications technologies on
quality healthcare service and to develop a research instrument for use in evaluating the effect of
wireless technology in healthcare service provision.
A qualitative and quantitative survey by questionnaire was adopted,combined, modified and used
from two different research tools of a unified technology acceptance and service quality models.
We developed a research instrument called UTAUT-SERVQUAL techniques to evaluate the per-
ceived effectiveness or impact of wireless information communication technologies in healthcare
service delivery.
The results of the study have indicated that the questionnaire can generate the data required to
analyse the evaluation of the percieved effectiveness and acceptance of wireless information com-
munication technologies in healthcare service delivery. This is reflected in the respondents ac-
knowledgement of the effective use and apparent improvement of serve in using the wireless in-
formation communication technologies for healthcare service delivery.
xii
-
7/30/2019 Bule Stephen Cit Masters Report
14/81
Chapter 1
INTRODUCTION
1.1 Background
Wireless healthcare delivery is the choice to go in the developing world due to the advantages that
it offers in terms of deployment. However as the need for these technologies increase there are
equally no methods of evaluating their impact in healthcare servive delivery. The introduction of
wireless information and communications technologies (WICT) in the healthcare environment has
led to an increased accessibility to healthcare professionals, more efficient tasks and processes and
higher quality of healthcare services (Kern and Jaron, 2003) [24]. The wireless-enabled healthcare
is therefore already with us and almost every health professional even in Uganda already uses a
mobile phone, and many also have laptops, notebooks or Personal Digital Assistants (PDAs) with
at least the potential to be linked wirelessly. The potential of wireless technology in health comes
from enabling health professionals to conveniently access information and knowledge, irrespective
of their location.
In this research the terms used in the document concerning wireless communication technolo-
gies are defined and explained below:Wireless technology refers to the use of radio signals instead of physical connections to transmit
data. Wireless also implies that the system is always connected and that the data are real time
(Newbold, 2004) [31]. The range of technologies collectively termed wireless include Personal
Digital Assistants (PDAs), robots, telehealth apparatus, pagers, telephones, tablet computers, sub-
notebook computers (smaller, lighter, portable computers), smart telephones, wireless networks,
mobile hardware peripherals, and all related software (Newbold, 2004) [31].
1
-
7/30/2019 Bule Stephen Cit Masters Report
15/81
Healthcare is the prevention, treatment, and management of illness and the preservation of mental
and physical well being through the services offered by the medical and allied health professions
(Stedmans medical dictionary, 2004) [37].
E-health is a process of providing healthcare via electronic means, in particular over the Inter-
net (Broderick, 2003) [30]. The term e-health has been used to describe the variety of activitiesrelated to the electronic exchange of health-related data, voice or video. E-health is an emerging
field in the intersection of medical informatics, public health and business, according to Eysenbach
(2001) [13].
Teleradiology refers to a facilitated remote consultation, diagnosis and management of patients us-
ing telecommunication technologies. Digital images are transmitted over a distance using standard
telephone lines, satellite connections, or local area networks (LANs)(Stedmans medical dictionary,
2004) [37].
In this study, we will look at Mulago hospital which is the largest healthcare organization in
Uganda with over 2,000 bed capacity, 2,300 employees and about 300 doctors with a total of
over 6 billion US Dollar total assets (Mullan, 2005) [29]. Acording to that annual report , Mulago
hospital is defined as a nationtal referral and teaching hospital which is a not-for-profit, public-
based network of hospitals, primary healthcrae centre and practices, rehabilitation clinic , senior
health centre, and Accident and Emergency surgery centre and a medical research institute which
provides quality, safe patient care supported by medical education and scientific research
1.2 Statement of the Problem
Wireless information communications have been deployed in some hospitals in Uganda to facilitate
quick access of critical and vital patient information. It is assumed that the wireless communication
technologies installed by the hospitals are functional and in use and these are supposed to impact
positively on healthcare delivery. However to our knowledge since their deployment, no study hasbeen carried out to ascertain the impact these technologies have had on the quality of healthcare
given by health practitioners. Hence there is need to carry out this study and to develop a reliable
questionnaire for on-going evaluations in healthcare.
2
-
7/30/2019 Bule Stephen Cit Masters Report
16/81
1.3 Main objectives
In this project we will evaluate the attitudes to wireless communication and information technolo-
gies on the service quality of healthcare service delivery and their perceived effectiveness by health
workers in selected healthcare centres in Uganda.
1.3.1 Specific Objectives
(i) To investigate the deployment environment of the wireless communication technologies
(ii) To evaluate the attitudes of healthcare professionals to the deployment of wireless commu-
nication technologies.
(iii) To evaluate the perception of healthcare professionals on the effect of the deployment of
wireless technology on the quality of healthcare service.
(iv) To develop a research instrument for use in evaluating the effect of wireless technology in
healthcare service provision.
1.4 Scope of the Study
The study will look at ICTs in healthcare focusing on wireless technologies only. The technologies
that will be targeted in this case will be PDAs, mobile phones,teleradiology sets and any wireless
technology.
The geographical coverage will be urban and or rural connectivity because of the diversity in
resource distribution like human, financial and infrastructure. In this study one urban facility (Mu-
lago hospital), which has specialists and infrastructure, will be investigated.
As noted earlier, e-health covers many stakeholders like the healthcare professionals, the patient,
government, IT vendors, marketers in health products and stokeholders. However, this study will
be concerned with the perceptions of healthcare professionals.
3
-
7/30/2019 Bule Stephen Cit Masters Report
17/81
1.5 Significance of the study
Developing countries have an overwhelming need for the provision of medical and healthcare
services especially in areas outside the cities and urban centres. The fast growing telecommuni-
cation services through MTN, Celtel, UTL and many other new ones still coming up will offer an
economical means of achieving the national policy objective Health for all with due regard to
improvement and or extension of medical and healthcare services up to rural health centre IVs.
Therefore, there is more than ever a greater need and drive by government to apply ICT in health
sector due to the cost reduction that comes alone with it.On the basis of the reasons advanced
above, it is of public and private interest to investigate the impact of wireless communication tech-
nologies in e-health.
There is need to develop a reliable research instrument for on-going evaluation of the attitudes
to, and percieved effectiveness of the use of wireless technology.
This area has always been over looked as organizations only look at acquiring new technologies but
have no idea on the concerns about the expectation and perceptions of the healthcare professionals
in service delivery.
4
-
7/30/2019 Bule Stephen Cit Masters Report
18/81
Chapter 2
LITERATURE REVIEW
2.1 Wireless technologies and Healthcare
The primary rationale for the development of e-health is to serve the population that have for geo-
graphical location, financial, or socio-economic reasons limited access to traditional, high quality
consultative, diagnostic, therapeutic and market medical services and or products such as drugs
and sundries. E-health can be delivered by using various technologies which include wireless
communication devices like pagers, blackberries, PDAs and cellular phones or use landlines like
telephone lines, local area networks, wide area networks and virtual private networks. In fact, a
new World Bank report notes 77 percent of the worlds population already lives within range of a
mobile network. (Albon, 2006) [2].
In recent years wireless technology has exploded in the southern hemisphere including the sub-
Saharan Africa where telecommunication infrastructure is less developed or lacking completely.
Uganda, like many developing countries lack the infrastructure readily available in the developed
world and is leapfrogging traditional fixed-line communication networks and adopting mobile, cel-
lular technologies to provide communication links to remote locations.
According to Gardner (1994) [16], financial, political and regulatory problems are some of the
main obstacles to communication system deployment in developing countries (Anvekar et al.,1996) [3].
However, the demand for communication and information services in developing countries is in-
creasing (Anvekar et al. (1996) [3], Meadows 1999) [28], but conventional copper wire infrastruc-
tures are too expensive to install and maintain in the rural less developed areas. Wireless communi-
5
-
7/30/2019 Bule Stephen Cit Masters Report
19/81
cation systems offer greater flexibility in network design, faster deployment, and are more suitable
in difficult terrain and climates (Javed et al.,1994) [23].
The healthcare discipline is increasing the use of new information and communication technolo-
gies. One of the technologies talked of that has transformed the activities of healthcare serviceis the wireless technology. This change is described as a revolution within the healthcare indus-
try.(Raghupathi, 2003) [35].
The introduction of wireless technology in healthcare service is a relatively new entry in the over-
all IT infrastructure. Chris Kent, the Director of the Technical Services Group of Daou Systems,
Inc.USA(Gillete, 2004) [17] maintains that The history of this kind of technology in healthcare
goes back a decade or so years. The versatility of having ethernet speed connectivity without
wires is driving the adoption of wireless data networking by healthcare industry. This functional-
ity is particularly useful in healthcare service because of the high degree of mobility involved in the
health sector. With the growing acceptance of electronic medical records (EMRs), the healthcare
providers are finding it easy to access huge amounts of patient data at the point of care, as well as
from the office or home. To better accommodate computers on carts and pocket PCs, many health-
care organizations in developing countries are deploying wireless technologies into the settings.
Installations were typically based on partnerships between an enthusiastic doctor and a special-
ist IT vendor. Until then, some projects attracted funding from central government but most were
supported, at a local level, by individual hospitals. Budget constraints meant that there was little
scope for designing custom hardware and many wireless e-health projects, especially those that
focused on heart monitoring, used equipment that was originally designed to monitor the per-
formance of athletes. The wireless version of Polar Electronics heart monitoring wristband was
particularly popular and was used in a system that remotely monitored the health of women during
pregnancy (Baker, 2003) [6].
In United Kingdom, according to Gardener (1994) [16] the successful break through to health-
care and IT became fashionable during the 1990s e.g the UKs Connecting For Health IT program
became a prime example. This saw healthcare IT funding co-ordinated at a national level and was
used to build applications that increased workflow rather than only to enhance patient monitoring.
While wireless took a share of spending programs, for example the use of Cisco WLAN and wire-
less VoIP technology, most applications differed little from those being deployed by companies in
6
-
7/30/2019 Bule Stephen Cit Masters Report
20/81
the financial services or retail sectors thus still creating a gap in wireless technologies in healthcare
(Brewin 2004) [7].
The wireless healthcare market is now moving into a new phase. According to Newbold (2004) [31],
healthcare professionals have realised that the only way to achieve the sort of cost savings seen inother sectors of the economy if technology is used, is to push care out to the edge of the health-
care network. The logic here is that, using remote healthcare, professionals can treat an increasing
number of patients while at the same time downsizing their core infrastructure. This new strategy,
to either intercept the patient before they enter the healthcare system or if that fails to care for the
patient in their own home, is highly dependent on the successful deployment of wireless based
medical devices.
Ugandas wireless health care initiative is an expansion of SATELLIFE trials with personal dig-
ital assistants (PDAs), or handheld computers, which began in 2001. In a recent AvantGo survey
(2003) [4] in Dublin, PDAs were recommended for use in our environments where computers are
impractical, because they are powerful tools that can provide critical, timely information to African
health workers. The PDAs were found to be especially useful in health administration, ordering
and tracking medical supplies, and delivering new treatment guidelines. In scaling up the project
to provide nationwide coverage for the health care initiative, a central wireless server was installed
in Ugandas capital, Kampala. It is linked to computer systems at the Ministry of Health, and at
Health Net Uganda, a local SATELLIFE affiliate housed at Makerere University, also in Kampala.
The server manages the entire network and communicates with wireless server called Jacks in
the field over commercial cellular phone networks (GSM) (Ladd 2003) [19].
Before 1996, Ugandas communication infrastructure was among the least developed, not only in
the world but also in sub-Saharan Africa (Wasukira et al, 2002) [39]. Further more, 70 percent of
the telecommunication services were concentrated in the urban areas, leaving the rural areas with
the least or totally no access to these services. As a result of liberalisation policies adopted by thegovernment of Uganda during the 1990s, the communication infrastructure situation has changed
to some extent. It is generally accepted that communication and information systems are major
factors for economical and social development, but still are underdeveloped in many developing
countries.
A nationwide launch of wireless network to improve Ugandas ability to treat patients and com-
7
-
7/30/2019 Bule Stephen Cit Masters Report
21/81
bat the spread of disease was announced in September 2003. The network is built around the
countrys well-established cell phone network, inexpensive handheld computers, and innovative
wireless servers. This technology allows healthcare workers to access and share critical informa-
tion in remote facilities without fixed telephone lines or regular access to electricity (Hardy et al,
2003) [12].
2.2 Application of wireless technology in healthcare
The Healthcare network administrators in UK where already finding that wireless access to data
boosts the number of patients served, improves the quality of physician diagnosis, and speeds pay-
ments and billing cycles (Cox, 2002) [10]. According to Forrester Research (Brown, 2004) [30],
wireless and mobile technologies are top spending priorities for health care organizations. Al-
though wireless LANs (WLAN) were used in hospitals for some time in the UK, the rollouts are
getting bigger and the applications are more sophisticated. In a 2003 survey by the Healthcare
Information and Management Systems Society, the report agrees that technology can assist in
addressing patient safety issues, and a big percentage of respondents believed that reducing medi-
cation errors was the best use of technology (HIMSS, 2003) [18].
Lastly according to a study published in the British medical journal by researchers from London
School of Hygiene and Tropical Medicine (2005) [8], the process of implementation of the wireless
technologies has been suboptimal, leading to reports of low morale by the NHS staff responsible
for implementation. The overall timetable was unrealistic, and hospitals became uncertain about
their implementation schedules. The study further concludes that socio-cultural implementation
challenges were neglected but is as daunting as the technical and logistical ones.
8
-
7/30/2019 Bule Stephen Cit Masters Report
22/81
2.3 Measuring attitudes to technology and quality of service
According to Oliver,(1997) [32] Satisfaction is a judgment that a product or service provides a
pleasurable level of consumption-related fulfillment, including levels of under- or over-fulfillment.
According to Prybutok and Spink (1999) [34] Customer satisfaction is one key attribute in quality
healthcare. In an information system (IS) setting within an organization, user satisfaction (US)
is measured by a comparison of user expectations (or needs) of the IS with the perceived perfor-
mance (or capability) of the IS on a number of different facets of the IS (Landrum and Prybutok,
2003) [34]. User Satisfaction is thus measured as the gap between user expectations and the per-
ceptions of the system.
2.4 UTAUT and SERVQUAL Models.
Wireless information communication technologies are new technologies in the Ugandan setting
which were introduced in less than a decade ago. According to Lee et al.,(2003,) [26]and Lu
et al.(1999) [27],technology acceptance and use is one of the most researched areas in the field
of information systems.The models like Technology Acceptance Model (TAM)assumes perceived
usefulness, rather than ease of use, as a strong indicator of usage. The end user satisfaction
model was developed to measure the end user satisfaction in a mandatory environment, and to
test the usefulness versus ease of use assumption (Adamson and Shine, 2003) [1].The Unified
Theory of Acceptance and Use of Technology(UTAUT)model by Venkatesh et al.(2003) [38]is an
acceptancy model that was developed due to a need for a review and synthesis in order to progress
toward a unified view of user acceptance. According to Venkatesh et al.(2003), the objectives of
the UTAUT was to understand the individual acceptance of new information technologies, com-
pare these models, formulate a unified theory of acceptance and use of technology, and validate
UTAUT by testing it. The methodology looks at four major dimensions that contribute to technol-
ogy acceptance which are performance expectance, effort expectance, social influence and lastly
facilitating conditions in the environment. The variables were gender, age, experience and volun-
tariness of use. According to Rosen (2004) [36] UTAUT was used successfully in studying the
willingness of an individual in using or trying out a new information technology. In this case its
9
-
7/30/2019 Bule Stephen Cit Masters Report
23/81
possible to explain the process of adoption and use of a new technology in information system/
technology.
According to Westland and Clark (2000), the presence of computer and information technologies
in todays organizations has expanded dramatically. Yet,for technologies to improve productivity,they must be accepted and used by employees in organizations.Parasuraman et al. (1988) [33]
developed a multi-item scale for measuring customer/ user perceptions of the service quality. The
two words of service and quality were combined to form what is now known as the SERVQUAL
technique. It is an empirically derived method that may be used by service organisations to im-
prove service quality. The method involves the development of an understanding of the percieved
service needs of the target group. SERVQUAL takes into account the the perceptions of the cus-
tomer/user of the relative importance of service attributed. The methodology was originally based
around five key dimensions (tangibles, reliability, responsiveness, assurance, empathy).according
to Zeithaml et al., (1994) [41] The current one which was used in this design is made of a series of
questions based around a number of key service dimensions such as tangibles, reliability, respon-
siveness, competence, courtesy, credibility, feel secure, access, communication and understanding
the customer. Satisfaction can be measured by performance, which in itself is a measure of quality
service. It is therefore upon this background that the study to evaluate the impact or percieved
effectiveness of the wireless technologies on the enhancement of healthcare service delivery will
use the combination of UTAUT and SERVQUAL model, which has not been done before.
10
-
7/30/2019 Bule Stephen Cit Masters Report
24/81
Chapter 3
METHODOLOGY
3.1 Overview
Methods of evaluation of customer satisfaction widely used by the IS/IT industry are several and
include sample survey techniques, focus group methods, evaluation and suggestion slips, Delphi
or normal group methods,and complaints analysis (Babbar, 1992; Yang, 2003) [5], [40]. Among
these methods, the survey by questionnaire and the complaints analysis are more popular than
others. However, because the complaints analysis is a passive method which does not allow under-
standing the status of customers satisfaction completely, more and more organizations are using the
questionnaire survey method. Hence in this study we will combine the SERVQUAL and UTAUT
questionnaire to develop a research instrument/ tool for use in evaluating wireless information
communication technologies in healthcare delivery by IT managers. The questionnaires will be
tested in the health centres / hospitals to assess the quality of healthcare service wireless technol-
ogy can deliver. The data collected will be used to process valuable information on the current
impact of wireless information communication technologies in healthcare service delivery. The
questionnaire will also be validated.
3.2 Research Design
There are several evaluation methods used to measure customer satisfaction and in this research we
will employ the survey methodologies similar to suit the wireless technologies for healthcare. A
11
-
7/30/2019 Bule Stephen Cit Masters Report
25/81
combination of two questionnaires of UTAUT and SERVQUAL will be used to form a questionnare
to address the attitudes and perceptions of healthcare professionals on healthcare delivery using
wireless information communication technologies.Observations and follow-ups interviews will be
used as required.
3.3 Study Area
The study will focus on investigating the impact of wireless technologies in Mulago hospital, which
is the national teaching and referral urban healthcare facility in central Uganda. The other centre
studed will be Rakai health facility, which is a small remote rural healthcare centre, connected with
the deployed wireless technologies selected for that reason. The study aims at addressing urban
and or rural information sharing using wireless technology. But due to time and resources factors
available, rural centres will be studied later
3.4 Study Population
The Healthcare professionals will be interviewed to find out their view or perception on the impact
of these wireless technologies deployed. In this research, healthcare workers will be selected based
upon statistical sampling techniques to participate in the survey. These will be medical officers,
nurses and allied health professionals. Other stakeholders like the patients, administrators, local
authorities, network service providers and IT vendors may be involved in a later research but are
not included in this project for reasons of time and reduce costs.
3.5 Validity and Reliability
The validity of an instrument as will be used in this study is consistent with definition provided by
Miles and Huberman (1994) [21], as the extent to which the items in the instrument measures what
they are set out to measure. Therefore existing instruments mentioned earlier will be amended to
develop a draft instrument.The supervisor will then establish the validity of the questionnaire and
a pilot study will be conducted. The reliability still, according to Miles and Huberman (1994) [21],
12
-
7/30/2019 Bule Stephen Cit Masters Report
26/81
has to do with the extent to which the items in an instrument generate consistent responses over
several trials with different audiences in the same setting or circumstances. The reliability will be
established through statistical analysis of the responses in the questionnaire.
3.6 Procedure of Data Collection
Permission will be sought from relevant areas to allow the study to be carried out. A requesting
letter will be written. An introductory or covering letter from the deputy dean, graduate studies will
be obtained. The identified respondents will be informed of the purpose of the study and obtain an
oral consent from them. Confidentiality of their information and identity will be maintained.
3.7 Data Analysis
The quantitative data that will be collected from the questionnaire will be summarised and tabu-
lated. Basic SPSS will be used to analyse responses and Microsoft Excel statistical spreadsheets
will be used to prepare graphics to aid description of key variables. The data generated from the
investigations will be analyzed, discussed and recommendations will be made where necessary.
Thereafter the results will be disseminated to the faculty.
3.8 Ethical Considerations
The ethical considerations will be pursued during the study focused on upholding social science
and applied science research namely: anonymity and confidentiality, and informed consent of the
respondents.
13
-
7/30/2019 Bule Stephen Cit Masters Report
27/81
Chapter 4
PRESENTATION AND FINDINGS.
4.1 Introduction
The results presented were obtained from a sample of 20 respondents at Mulago hospital. The
results are according to the objectives which are stated below.
The specific objectives of the study which are being addressed are as follows:
(a) To investigate the deployment environment of the wireless communication technologies
(b) To evalute the attitudes of healthcare professionals to the deployment of wireless communi-
cation technologies.
(c) To evaluate the perception of healthcare professionals on the effect of the deployment of
wireless technology on the quality of healthcare service.
(d) To develop a research instrument for use in evaluating the effect of wireless technology in
healthcare service provision.
4.2 Developing questionnaire
The research instrument was designed and used to carried out the study. The questionnaire that
was developed from the two research techniques of UTAUT and SERVQUAL had initially eighty
five questions all together. These questions were curved out from these set of questions originating
14
-
7/30/2019 Bule Stephen Cit Masters Report
28/81
from UTAUT and SERVQUAL as shown below: The sample questions to ask were generated from
Table 4.1: Shows the Technology acceptance model using UTAUT technique
Acceptance dimension Sample of questions to ask
Performance Expectancy:
Concerns percieved usefulness, job-fit, relative advantage and
Outcome expectations
Effort Expectancy:
Concerns Percieved ease of use, complexity and
ease of use
Social Influence:
Concerns subjective norm, social factors and image
Facilitating condition:
Concerns percieved behavioural control, facilitating conditions
and complexity
those dimensions in the above table and are as follows:
Performance Expectancy:
Performance expectancy is defined as the degree to which an individual believes that using the
system will help him or her to attain gains in job performance.
Percieved Usefulness:
The degree to which a person believes that using a particular system would enhance his or her job
performance.
1. Using the system in my job would enable me to accomplish tasks more quickly.
2. Using the system would improve my job performance.
3. Using the system in my job would increase my productivity.
4. Using the system would enhance my effectiveness on the job.
5. Using the system would make it easier to do my job.
6. I would find the system useful in my job.
Job-fit:
How the capabilities of a system enhance an individuals job performance.1. Use of the system will have no effect on the performance of my job.
2. Use of the system can decrease the time needed for my important job responsibilities.
3. Use of the system can significantly increase the quality of output on my job.
4. Use of the system can increase the effectiveness of performing job tasks.
5. Use can increase the quantity of output for the same amount of effort.
6. Considering all tasks, the general extent to which use of the system could assist on the job.
15
-
7/30/2019 Bule Stephen Cit Masters Report
29/81
Relative Advantage:
The degree to which using an innovation is perceived as being better than using its precursor.
1. Using the system enables me to accomplish tasks more quickly.
2. Using the system improves the quality of the work I do.
3. Using the system makes it easier to do my job.4. Using the system enhances my effectiveness on the job.
5. Using the system increases my productivity.
Outcome Expectation:
1. I will increase my effectiveness on the job.
2. I will spend less time on routine job tasks.
3. I will increase the quality of output of my job.
4. I will increase the quantity of output for the same amount of effort.
5. My coworkers will perceive me as competent.
6. I will increase my chances of obtaining a promotion.
7. I will increase my chances of getting a raise.
Effort Expectancy:
Effort expectancy is defined as the degree of ease associated with the use of the system.
Percieved Ease of Use:
The degree to which a person believes that using a system would be free of effort.
1. Learning to operate the system would be easy for me.
2. I would find it easy to get the system to do what I want it to do.
3. My interaction with the system would be clear and understandable.
4. I would find the system to be flexible to interact with.
5. It would be easy for me to become skillful at using the system
6. I would find the system easy to use.
Complexity:
The degree to which a system is perceived as relatively difficult to understand and use.1. Using the system takes too much time from my normal duties.
2. Working with the system is so complicated, it is difficult to understand what is going on.
3. Using the system involves too much time doing mechanical operations.
4. It takes too long to learn how to use the system to make it worth the effort.
Ease of Use:
The degree to which using an innovation is perceived as being difficult to use.
16
-
7/30/2019 Bule Stephen Cit Masters Report
30/81
1. My interaction with the system is clear and understandable.
2. I believe that it is easy to get the system to do what I want it to do.
3. Overall, I believe that the system is easy to use.
4. Learning to operate the system is easy for me.
Social Influence:
Social influence is defined as the degree to which an individual perceives that important others
believe he or she should use the new system.
Subjective Norm:
The persons perception that most people who are important to him think he should or should not
perform the behavior in question.
1. People who influence my behavior think that I should use the system.
2. People who are important to me think that I should use the system.
Social Factors:
The individuals internalization of the reference groups subjective culture,and specific interper-
sonal agreements that the individual has made with others,in specific social situations.
1. I use the system because of the proportion of coworkers who use the system.
2. The senior management of this business has been helpful in the use of the system.
3. My supervisor is very supportive of the use of the system for my job.
4. In general, the organization has supported the use of the system.
Image:
The degree to which use of an innovation is perceived to enhance ones image or status in ones
social system.
1. People in my organization who use the system have more prestige than those who do not.
2. People in my organization who use the system have a high profile.
3. Having the system is a status symbol in my organization.
Facilitating Conditions:Facilitating conditions are defined as the degree to which an individual believes that an organiza-
tional and technical infrastructure exists to support use of the system.
Perceived Behavioral Control:
Reflects perceptions of internal and external constraints on behavior and encompasses self efficacy,
resource facilitating conditions, and technology facilitating conditions.
1. I have control over using the system.
17
-
7/30/2019 Bule Stephen Cit Masters Report
31/81
2. I have the resources necessary to use the system.
3. I have the knowledge necessary to use the system.
4. Given the resources, opportunities and knowledge it takes to use the system, it would be easy
for me to use the system.
5. The system is not compatible with other systems I use.Facilitating Conditions:
Objective factors in the environment that observers agree make an act easy to do, including the
provision of computer support.
1. Guidance was available to me in the selection of the system.
2. Specialized instruction concerning the system was available to me.
3. A specific person (or group) is available for assistance with system difficulties.
Compatibility:
The degree to which an innovation is perceived as being consistent with existing values, needs, and
experiences of potential adopters.
1. Using the system is compatible with all aspects of my work.
2. I think that using the system fits well with the way I like to work.
3. Using the system fits into my work style.
18
-
7/30/2019 Bule Stephen Cit Masters Report
32/81
Table 4.2: Shows the SERVQUAL 10 dimensions used in healthcare service
Quality dimension Samples of questions to ask
Tangibles:
Appearences of physical facilities,
equipment, personnel and information
Reliability:Ability to perform promised service
dependably and accurately
Responsiveness:
Willingness to help user to provide
prompt healthcare service
Competence:
Possession of the required skill and
knowledge to perform service
Courtesy:
Politiness, respect and consideration
Credibility:Trustworthiness, believability,
honesty of the healthcare service provider
Security:
Free from danger, risk or doubt
Access:
Approachability and ease of contact
Communication:
Listening to patient and acknowledging
their comments/ concerns/ queries
Understanding the patient/ client:Making the effort to know patients and their needs
The 10 dimesions were used to generate samples of questions to ask which are in the following
order as shown in table 4.2
Tangibles:
1. Are the healthcare facilities attractive?
2. Are the healthcare professionals knowledgable?
3. Are the wireless technologies modern?4. Is the sent information easy to understand?
Reliability:
1. If a response is assured to a patient at a certain time, does it happen?
2. Is the information free of errors?
3. Is the healthcare service offered or performed right the first time?
4. Is the level of healthcare service the same at all times of the day
19
-
7/30/2019 Bule Stephen Cit Masters Report
33/81
Responsiveness:
1. When there is a problem, do the healthcare centre respond quickly?
2. Are healthcare professionals willing to answer patient questions?
3. Are public situations treated with care and seriousness?
Competence:1. Can the heathcare professionals provide service through wireless technology?
2. Can the professionals use the technology quickly and skillfully?
3. Do the healthcare professionals appear to know what they are doing?
Courtesy:
1. Are the responses on wireless technologies considerate and polite?
2. Do the healthcare professionals observe consideration of the property and value ptients?
3. Do the healthcare professionals refrain from acting busy?
Credibility:
1. Do healthcare centres have a good reputation?
2. Are the consultations/ responses in healthcare given accurately and consistently with other reli-
able sources?
3. Does the healthcare centre gurantee its services?
Security:
1. Is it safe to use the wireless technologies?
2. Are the information relayed on wireless technology secure?
3. Can patients be confident that e-health provided was done correclty?
Access:
1. How easy isit to communicate to a consultant/ that knowledgable healthcare professional?
2. Is it easy to access the healthcare professional on wireless technology?
3. Are the healthcare service access points conviniently located?
Communication:
1. Do healthcare professionals avoid using medical jargons when communicating?
2. Do healthcare professionals call if scheduled appointment will be missed/ changed?Understanding the patient:
1. Is the level of service and cost of service consistent with the requirements and affordability?
2. Are healthcare professionals flexible enough to accomomdate patients schedule?
We looked at all of them and related their relevancy to the this reaseach and came out with 66
questions. We subjected these questions to a number of healthcare professionals from around
20
-
7/30/2019 Bule Stephen Cit Masters Report
34/81
Kampala and Mulago hospital in the pilot study. Over ten questionnaires were given out for this
purpose, 6 were returned with comments and suggestions. There were some questions which the
respondents said meant almost the same in that they stressed on the same point. The questions
that we felt were emphasizing the same point were dropped. We ended up with 45 questions that
addressed issues concerning technology acceptance, service quality and deployment environmentin healthcare services. See questionnaire Appendix 1
4.3 Findings and characteristics of healthcare professionals.
The new questionnaire were then distributed in Mulago hospital and some sent to Rakai health-
care a rural setting. After a period of four weeks, 20 questionnaires were recieved from Mulago
Hospital and non from the rural health centre. The health professionals in Rakai health centre did
recieve the questionnaires but have not had time to respond to the them due to their busy schedules
of duty.
Therefore results presented here were exclusively obtained from a sample of 20 respondents out
of 25 at Mulago hospital showing response rate of 80 percent. This chapter covers the testing of
the questionnaire, selected background characteristics of the respondents such as sex, profession
and years of experience. It further covers the deployment environment of the wireless technology,
attitude of the respondents towards the use of the technology and the perception. The results are
according to the objectives which are stated in chapter 4.1 above.
4.3.1 Analysis of the questionnaire by relationship
From the data collected analysis was done using SPSS to study the relevancy of the questionnaire
since it is a combination of two model questionnaires. The chi-square obtained by looking at the
relationship of the variables in UTAUT and SERVQUAL were significant in that they have level
of significancy of below 0.05.
The figure 4.1 below clearly indicates that the questionnaire is valid and can provide the neces-
sary information it is intended to generate for the study of the evaluation of wireless information
communication technologies.
21
-
7/30/2019 Bule Stephen Cit Masters Report
35/81
For more relationships relating to the questions in the questionnare please check the Appendix
2 on Chi-Square comparing some items.
Figure 4.1: Shows the Relationships and Chi-Square value
.
4.3.2 Validity and reliability
The questionnaire was subjected to the respondents in the initial stage, then a pilot survey was car-
ried out. Following these stages basing on the new questionnaires all the respondents responded
well and understood what the questions meant. An interview with four respondents who had ear-
lier participated in the survey showed that questions were in keeping with what they were intended
for. The responses were consistent with the earlier responses proving its reliability.
Secondly these were questions adopted from UTAUT and SERVQUAL techniques which have
been tested and proved to be valid and reliable. Most errors can be avoided by use of good tech-
niques, this therefore has tested validity.
22
-
7/30/2019 Bule Stephen Cit Masters Report
36/81
4.3.3 Characterictics of Healthcare professionals.
Table 4.3: Percentage distribution of the respondents according to background characteris-
tics
Charateristics Frequency Percentage
SexMale 12 60
Female 8 40
Total 20 100
Profession
Medical doctor 8 40
Nurse 1 5
Pathologist 1 5
Physiotherapist 3 15
Radiographer 3 15
Radiologist 4 20Total 20 100
Years of Experience
-5 1 5
5-9 10 50
10-14 4 20
15+ 5 25
Total 20 100
Gender
Sex is one of the background characteristics included in this study and it was categorized as male
and female. The results presented in Figure 4.2 and Table 4.3 Show that the majority of the
respondents are males as represented by 60 percent whereas the females constituted 40 percent
of the respondents.The questionnaires were given out at random focusing mainly the different
departments of speciality. Note that gender did not play a key role as a variable since the use of
these technologies are not sex dependant.
23
-
7/30/2019 Bule Stephen Cit Masters Report
37/81
Figure 4.2: Shows the gender of respondents.
Profession
Several healthcare disciplines were involved in this survey and majority of them were the medical
doctors (40 percent), followed by radiologists (20 percent). On the other hand, the proportion of re-
spondents who were physiotherapists by profession was the same as the proportion of respondents
who were radiographers (15 percent) respectively. The least score was registered by those whose
profession was nursing and pathologists that constituted 5percent respectively. 5 questionnaires
were given out in the various departments although the responses did not portray that since some
respondents did not complete the questionnaire at the time of collecting the data. It was noted that
profession determined the exposure and frequency of use of some of the wireless technologies.
Medical doctors were more exposed to using PDAs and mobile phones while the radiologists used
teleradiology and mobile phones.
Years of Experience
Over 50 percent of the respondents had an experience of 5 years with majority at 5-9 years of
experience. The difference in size of the sub samples in terms of experience was by coincidence.
24
-
7/30/2019 Bule Stephen Cit Masters Report
38/81
The respondents had years of experince ranging from one to twenty one years. See table 4.3 and 4.4
The respondents among others were a senior consultant with vast years of experience and also
Table 4.4: Brief background of the respondents
No Post Holding Department Sex Years of Experience ICT Awareness
1 Senior Consultant Radiology Male 25 Over 2 yrs
2 Consultants Radiology Female 16 Over 2 yrs
1 Consultant Pathology Male 12 Over 2 yrs
2 Medical officers S.G Surgery Male 10-15 Over 2 yrs
1 Medical officers S.G Medicine Female 14 Over 2yrs
1 Medical officers S.G Radiology Female 16 Over 2 yrs
5 Medical Officers Mixed Mixed 6-16 Over 2 yrs
2 Senior Physiotherapists Physiotherapy Male 9-14 Over 2yrs
1 Physiotherapist Physiotherapy Female 6 Over 2 yrs
2 Radiographers Radio1ogy Male 1-2 Over 2yrs1 Teaching Assistant Medical School Male 1 1 yr
1 Senior Nurse Officer Private Wing Female 20 Over 2 yrs
20
involved with issues concerning ICTs in health sector. A good number of doctors were involved
ranging from consultants down to the general medical practitioners with at least six years of ex-
perience and over two years of ICT awareness in hospital setting. Other healthcare cadres were
also involved from the nurse to the allied health profesionals who are always in contact with the
patient. See table 4.4 below
4.3.4 Available wireless communication technologies
The existing wireless communication technologies in this study included PDA, Mobile phones and
teleradiology. The results presented in the Figure 4. shows that amongst the healthcare profes-
sional the mobile phone has been available for over 2 years represented by over 90 percent of the
respondents whereas wireless teleradiology was the least used with over 60 percent of the respon-
dents having not used it before. A number of the respondents indicated that they have never used
PDAs and teleradiology.
25
-
7/30/2019 Bule Stephen Cit Masters Report
39/81
Figure 4.3: Shows Available wireless communication technologies
.
4.3.5 Ownership of the wireless information communication technologies
Among the deployed wireless technologies mobile phones were owned by individual shown by100 percent, followed by the PDAs (90 percent). While for the teleradiology set, respondents felt
it either belongs to the health centre or a private organization. In this case, through interviewing the
responsible persons we discovered that it was owned by a private organisation that deployed it at
the health facility as a project to pilot connectivity between hospitals for specialised consultation.
This was to link Mulago, Mengo and Butabika hospitals. In the survey, the findings were that the
PDAa were either belonging to individuals or provided for by the institution such as the Mulago
medical school to medical students and practising doctors at postgraduate level.
26
-
7/30/2019 Bule Stephen Cit Masters Report
40/81
Figure 4.4: Shows Ownership of the wireless information communication technologies
.
4.3.6 Current state of use or expected time of use
The respondents in table 4.4 indicate that 95 percent of them use mobile phones which was fol-lowed in use by a few who use PDAs. See table 4.4 more more details in figures. The least
used is teleradiology more precisely because it is a specialised wireless technology for tranmit-
ting images,video, data/ text and audio using ISDN and the linked to a remote site using wireless
connectivity provided by service providers like MTN. Data on the current state of use and the ex-
pected time of use was also captured in this study.From the figures in table 4.4, the respondents
were optimistic that they would use the unavailable wireless technologies in about five years time.
This an indicator that they are embrassing use of wireless technology which in itself implies that
technology is being accepted in healthcare service delivery.
Hopefully as the cost of technology goes down the assumption is that a quarter of the healthcare
professionals would be using some of the wiereless technologies in two years time.
The Figure 4.4 shows a pie chart with the cummulative percentages of use from all the respondents
27
-
7/30/2019 Bule Stephen Cit Masters Report
41/81
Table 4.5: Shows the percentage distribution of the wireless technologies whether currently
in use or expected to be used
I currently use Expect in 12 Months Expect in 2 years Expect in 5 y
PDA 35 20 25
Mobile phone 95
Wireless Teleradiology 15 10 25
a total with mobile phones most used followed by PDAs.The results presented in the figure 4.4
indicate that all the wireless information communication technologies are currently in use with
teleradiology being the least used and mobile phones being the most used.
Figure 4.5: Shows Percentage of usage of the wireless technologies
.
28
-
7/30/2019 Bule Stephen Cit Masters Report
42/81
4.4 Deployment environment of the wireless communication tech-
nologies
Here we look at the various factors in environment affecting the deployment of the wireless infor-
mation communication technologies and the attitudes of the healthcare professionals towards the
regulatory policies in hospitals, national laws covering use of electronics, lack of fund, the chang-
ing technologies and availability of support personal. The attitudes were categorised as strongly
agree, agree, no difference, disagree and strongly disagree. See Figure 4.6 and Table 4.5 below
4.4.1 Regulatory policies in healthcare centres
As shown in the Table 4.5, 45 percent of the respondents disagree that regulatory policies in health-
care centres hinders deployment of wireless communication technology in the healthcare centres.
One-fifth of the respondents agree that it is this regulatory policies that hinders deployment of
wireless communication technologies. The proportion of respondents who said that they strongly
agree that this policies affects deployment of wireless communication technologies is the same as
those who said that there is no difference represented by 10 percent respectively.
4.4.2 National laws covering use of wireless technologies
As shown in the Table 4.5, most of the respondents believe that there is no difference in the national
laws concerning deployment of wireless communication technology in the healthcare centres. The
proportion that agree and disagree that this laws affect deployment of wireless communication is
same (21.1percent) respectively.
4.4.3 Lack of funding
Lack of funding is one of the factors that affect the deployment of wireless information communi-
cation technology in healthcare service delivery. The findings in Table 4.5 shows that 75 percent
of the respondents both strongly agree and agree that lack of funding affects deployment of this
technologies. On the other hand, there was a significant number of respondents who felt no differ-
29
-
7/30/2019 Bule Stephen Cit Masters Report
43/81
ence(10 percent) and those who disagree.
4.4.4 Changing technologies
The respondents response on the change of technology disagreed that it could affect deployment.
The Table 4.5 shows that 55 percent of the respondent disagreed on the statement that chang-
ing technology affects the deployment of wireless information communication technologies. The
number of respondents who agreed and those who show no difference to the statement were the
same at 15 percent. While 10 percent and 5 percent strongly disagreed and strongly agreed on the
issues concerning changing technologies.
4.4.5 Availability of support personal
The presence of support personal featured strongly for purpose of deploying the wireless technol-
ogy in a healthcare centre. 35 percent of the respondents fill they required a support personal while
10 percent felt it was not necessary.
30
-
7/30/2019 Bule Stephen Cit Masters Report
44/81
Figure 4.6: Shows responses on deployment environment of the wireless technologies
.
4.5 Limitations of the Study
There are three important limitations to the study.
First, the survey on perceptions and attitudes is of questionable validity but this one used UTAUT
and SERVQUAL model of questions. During the pilot survey some staffs felt that a few items
needed to be reworded. Since many of the items refer to the concepts of wireless technology and
healthcare service delivery, the reliability and validity of the items depends on the strength of ref-
erence held by these terms. The designer of the questionnaire attempted to clarify these concepts
by providing definitions of them throughout the course of the survey.
31
-
7/30/2019 Bule Stephen Cit Masters Report
45/81
Second, all sample surveys are liable to have biased findings when response rates are low. This
only represents a problem on the Mulago hospital based follow-up survey, since the attitude pilot
and tests were administered before and during the Survey. For the test survey, while the evaluator
is pleased with the 80 response rate, there is no assurance that these respondents are an unbiasedrepresentation of the whole group.
Thirdly, the healthcare professionals are very busy people thus unable to respond to large sets
of question easily. This questionnaire had 45 questions in all and therefore more time is required
to have a good and reasonable response number.
4.6 The attitudes of the respondents in determining the level oftechnology acceptance by the healthcare professionals
The attitudes of the healthcare professionals towards technology acceptance was assessed in this
study. Several dimensions are considered in addressing the attitudes of the professionals towards
technology and this include usefulness of technology, quick accomplishment, productivity increase
among others.
32
-
7/30/2019 Bule Stephen Cit Masters Report
46/81
Figure 4.7: Shows dimensions of technology acceptance by healthcare professionals
.
4.6.1 Usefulness to job
As shown in the Figure 4.7, majority of the respondents agree that the technologies was useful to
their jobs. On the other hand, only 5 percent strongly disagree that the technologies are useful
to their jobs. These resluts signify that the healthcare professionals accept the use of the wireless
technology and find it useful to their work. Even though some did not have the other wireless
technologies available to their disposal but still felt it necessary and useful to their respective jobs.
4.6.2 Enables quick accomplishment
The attitudes of the respondents was also assessed by asking the respondents if the technologies
enabled them quickly accomplish their job. This was grouped as strongly agree, agree, no differ-
ence, disagree and strongly disagree. The results presented in the Figure 4.7 shows that 85 percent
of the respondents agree whereas the rest of the responses had the same score 5 percent.
33
-
7/30/2019 Bule Stephen Cit Masters Report
47/81
4.6.3 Productivity increase
Over 70 percent of the respondents showed that the deployment of wireless information com-
munications has helped to increase productivity at workplace.The wireless communication has
increased productivity in that healthcare professional do not need to walk some distance away to
consult but make a call and business continues as usual. This greatly increases productivity.
4.6.4 Skilled to perform job
The features show that the healthcare professionals are skilled enough to use wireless information
communication technologies. The respondent indicated that they were skilled to use the availble
wireless information communication technologies. This was common with those using mobilephone and partly the PDAs. However the teleradiology was much more complex system which
some of the respondents felt they are not skilled enough to use it.
4.6.5 Work more interesting
Majority of the respondents indicate that the technologies have made healthcare service more in-
teresting as shown in figure 4.7. This has been so because they seem to embrass the use of new ITtechnologies and therefore do accept them for the delivery of healthcare service.
4.7 The perception of respondents to determine the service qual-
ity when using wireless information communication tech-
nologies.
In this study the perception of the healthcare professionals towards the wireless information com-
munication technologies was assessed on quality of healthcare services. subsection Information
on wireless technologies are delivered free of errors In Figure 4.8, majority of the respondents
disagree that information over wireless communication technologies is free of errors.
34
-
7/30/2019 Bule Stephen Cit Masters Report
48/81
Figure 4.8: Shows Components of service Quality in healthcare service by using wireless
technologies
.
4.7.1 Same level of healthcare services
In the Table 4.6, majority of the respondents represented by 65 disagree that the level of healthcare
services is the same compared to those who agree represented by 35 percent. However, small
percentage of the respondents said that there is no difference in the level of healthcare services
when using wireless technologies.
4.7.2 Respond faster to fix problem
The results in the Table 4.6 shows that over 80 percent of the respondents disagree that the respond
to fix problems fasters with the healthcare communication technologies. On the other hand, 15
percent of them agree that they respond to fix problems faster.
35
-
7/30/2019 Bule Stephen Cit Masters Report
49/81
4.7.3 More care and consideration to patients
The results in the Table 4.4 shows that 45 percent of the respondents disagree that patient are treated
with more care and consideration whereas those who strongly disagree with that were represented
by 5 percent. Furthermore, 30 percent said that there is no difference as far as patient care and
consideration is concerned.
4.7.4 Easier communication to healthcare professionals
The results in the Table 4.6 further indicates that shows that 80 of the respondents agree that
wireless information communication technologies have made patient to healthcare professional
communication much easier. Furthermore, 15 percent said that there is no difference whereas 5percent strongly disagree that patient to healthcare professional communication is much easier.
4.7.5 Patient information more secure
The results in the Table 4.6 shows that 30 percent of the respondents strongly disagree that patient
information is secure whereas 30 percent of them agree so. On the other hand, 40 percent of them
said that there is no difference in patient information security on the wireless technology.
Table 4.6 Shows the percentage distribution of the respondents according to the perception
of the healthcare professionals to the delivery of quality healthcare services
Basing on patient information confidentiality, most healthcare professionals feel uncomfortable
in sharing that information online using especially wireless technologies. It is common knowledge
that information online wireless can be tapped for several reasons, defense and security being one.
Therefore one can not ruleout malice. See next page Table 4.6
36
-
7/30/2019 Bule Stephen Cit Masters Report
50/81
4.8 Summary of Findings
1. There was virtually no change between pilot and test items reflecting baseline opinions about
healthcare and wireless in the hospital.
2. There was no change reported on pilot and test questionnaires in perception or attitude re-
garding the use of wireless information communication technologies over the course of the
Survey.
3. The six participants in the pilot survey showed some minor changes on the two questionnaire
items on the pilot survey that reflected misconceptions about an healthcare service delivery.
4. Fewer respondents believed that wireless technology were only promoting Technology-
based practices; and more respondents understood that wireless information technologies
serve the needs of both individuals and public alike especially the PDAs and mobile phones.
5. The Respondents became aware of what they were asked in the questionnaire and some how
acted as a comprehensive brief education programs on the following:
(a). Expanding knowledge and broadening perspective in use of wireless technology in
healthcare service
(b). Possible future plans to integrate health informatics into curriculum/classroom
(c). Learned to share information with others and give individual opinions, thus increase
tolerance
(d). The researcher is able to make a presentation or short presentations out of the survey
(e). The information will be eventually disseminated and shared with staff
6. The researcher has reported the following positive impacts in their work as a result of apply-
ing wireless technologies:
(a). Helped break down barriers between healthcare professionals, patients, Medical stu-
dents, and others.
37
-
7/30/2019 Bule Stephen Cit Masters Report
51/81
(b). Learned that wireless information technologies increase productivity, work is more in-
teresting and ease of use.
(c). More knowledge since remote locations with wireless technologies will have access.
(d). Network with others through information sharing using wireless technologies such as
teleradiology/ telemedicine(e). PDAs are useful and essential in collecting or gathering research data from the out-
reaches
7. There has been communications between participants since the Survey was conducted through
departmental or unit group discussions and through service and outreach.
8. A majority of respondents enjoyed the survey.
9. Several respondents urged a continuation of the Survey and expanding their exposure in
health related information systems.
38
-
7/30/2019 Bule Stephen Cit Masters Report
52/81
Table 4.6: Shows the Percentage distribution of the respondents according to the deployment
environment of the wireless technologies
Deployment environment Frequency Percentage
Hospital regulatory policies hinders deployment
Strongly agree 2 10
Agree 4 20
No difference 2 10
Disagree 9 45
Strongly disagree 3 15
Total 20 100
There are no national laws that cover use
Strongly agree 3 15
Agree 4 20
No difference 6 30
Disagree 4 20
Strongly disagree 2 10
Total 20 100
Lack of funding affects deployment
Strongly agree 8 40
Agree 7 35
No difference1 2 10
Disagree
Strongly disagree 3 15Total 20 100
The changing technology hinder deployment
Strongly agree 1 5
Agree 3 15
No difference 3 15
Disagree 11 55
Strongly disagree 2 10
Total 20 100
Availability of support Human resource
Strongly agree 6 30Agree 2 10
No difference 7 35
Disagree
Strongly disagree 5 25
Total 20 100
39
-
7/30/2019 Bule Stephen Cit Masters Report
53/81
Table 4.7: Shows the percentage distribution of the respondents according to the perception
of the healthcare professionals to the delivery of quality healthcare services
Service Quality Frequency Percentage
Information free of errors
Strongly agree
Agree 3 15No difference 3 15
Disagree 9 45
Strongly disagree 5 25
Total 20 100
Same level of healthcare service
Strongly agree 1 5
Agree 4 20
No difference 1 5
Disagree 12 60
Strongly disagree 2 10
Total 20 100
Centre responses faster to fix problems
Strongly agree
Agree 3 15
No difference
Disagree 13 65
Strongly disagree 4 20
Total 20 100
Patient treated with more care and consideration
Strongly agree
Agree 3 15No difference 6 30
Disagree 10 50
Strongly disagree 1 5
Total 20 100
Easier to communicate to healthcare professionals
Strongly agree 3 15
Agree 13 65
No difference 3 15
Disagree 1 5
Strongly disagree 5 25Total 20 100
Patient information more secure
Strongly agree
Agree 7 35
No difference 6 30
Disagree 5 25
Strongly disagree 2 10
Total 20 100
40
-
7/30/2019 Bule Stephen Cit Masters Report
54/81
Chapter 5
CONCLUSION AND
RECOMMENDATIONS.
5.1 Conclusions
The case study at Mulago hospital revealed that there are PDAs, Mobile phones and teleradiology
set in use at the hospital. However these wireless technologies were used by different profession-
als with the exeption of the mobile phone which is used all over. The PDAs is mainly used in
department of medicine, pathology and surgery, while the teleradiolgy is majorly used in the ra-
diology department. There is 100 percent usage of the mobile phones by all the respondents who
are practicing healthcare professionals. The wireless technologies that were deployed deliberatey
are to some extend the PDAs and Teleradiology which are owned by a private organisation but
not the healthcare centre as was earlier thought to be by some respondents. Mobile phones was
exclusively owned by individual.
The major finding in the deployment environment is that healthcare professionals fill that lack
of funding in these technologies to purchase, maintain, repair and technical support were hinder-
ing deployment and effective utilisation. Also important to note is that the respondents were not
sure about the current laws concering use of information communication technologies in the coun-
try. This alone has a negative impact since the administrators and managers tend not be sure of
how to proceed once faced with the intent to deploy the technologies.
The healthcare professional have to some extend individually embraced the use of wireless in-
41
-
7/30/2019 Bule Stephen Cit Masters Report
55/81
formation communication technologies especially mobile phone and PDAs amongst those who
have pursued post graduate studies. Most started using the PDAs for gathering information on pa-
tients from rural areas. A private organization in collabration with makerere medical school have
deployed PDAs and teleradiology in Mulago hospital and some upcountry health centres, notably
Mbale hospital and Rakai health centre.
The study indicates that the attitudes of the healthcare professionals on wireless technologies is
postive thus ascent to technology ac