Muzykoterapia dla seniora Music therapy for seniors · W historii muzyki kompozytorzy nie dobiera-...
15
GERONTOLOGIA POLSKA 2018; 26; 226-228 ARTYKUŁ POGLĄDOWY / REVIEW PAPER Zgłoszono 13.11.2017, zaakceptowano 20.01.2018 Muzykoterapia dla seniora Music therapy for seniors Michalina Radzińska Katedra i Klinika Geriatrii, Collegium Medicum UMK w Bydgoszczy Streszczenie Muzykoterapia jako jedna z metod wspomagających terapie medycyny konwencjonalnej wciąż pozostaje dziedziną, która nie została w pełni zgłębiona. Głównym założeniem terapii muzyką jest niwelowanie napięć, lęków oraz przeciwdziałanie negatywnym skutkom stresu związanego z trudami życia codziennego. Na całym świecie podejmowane są badania nad wpływem muzyki na pacjentów cierpiących z powodów różnych jednostek chorobowych. W przypadku seniorów, znaczna część badań skupia się na przeciwdziałaniu depresji oraz łagodzeniu objawów demencji i łagodnych zaburzeń poznaw- czych. Niestety większość opisanych prób zostało przeprowadzonych na małych grupach badanych (MCI), przez co nie mogą stanowić dowodu na skuteczność proponowanych rozwiązań dla ogółu populacji. (Gerontol Pol 2018; 26; 226-228) Słowa kluczowe: muzykoterapia, senior Abstract Music Therapy is still not fully explored as one of the methods assisting in conventional medicine. still is a discipline that is not fully explored. The main assumption in Music Therapy is to eliminate tension, fears and to prevent consequences of daily stress. All over the world research is undertaken to find out the influence of Music Therapy on patients suffering from different diseases. In case of elderly patients, the main point is to try to counteract depression and to alleviate symptoms of dementia and mild cognitive impairment (MCI). Unfortunately, most studies were administered in small cohorts, and can not be considered a proof of effectiveness for the general public. (Gerontol Pol 2018; 26; 226-228) Key words: music therapy, senior
Transcript of Muzykoterapia dla seniora Music therapy for seniors · W historii muzyki kompozytorzy nie dobiera-...

GERONTOLOGIA POLSKA 2018; 26; 226-228 ARTYKUŁ POGLĄDOWY / REVIEW PAPER Zgłoszono 13.11.2017, zaakceptowano 20.01.2018
CorreAdres do korespondencji: Michalina Radzińska; Katedra i Klinika Geriatrii CM UMK, ul. Marii Skłodowskiej- Curie 9, 85-094 Bydgoszcz (+48 52) 585 49 00 [email protected]
Ó Akademia Medycyny
Muzykoterapia dla seniora
Music therapy for seniors
Michalina Radzińska
Katedra i Klinika Geriatrii, Collegium Medicum UMK w Bydgoszczy
Streszczenie
Muzykoterapia jako jedna z metod wspomagających terapie medycyny konwencjonalnej wciąż pozostaje dziedziną, która nie została w pełni zgłębiona. Głównym założeniem terapii muzyką jest niwelowanie napięć, lęków oraz przeciwdziałanie negatywnym skutkom stresu związanego z trudami życia codziennego. Na całym świecie podejmowane są badania nad wpływem muzyki na pacjentów cierpiących z powodów różnych jednostek chorobowych. W przypadku seniorów, znaczna część badań skupia się na przeciwdziałaniu depresji oraz łagodzeniu objawów demencji i łagodnych zaburzeń poznaw-czych. Niestety większość opisanych prób zostało przeprowadzonych na małych grupach badanych (MCI), przez co nie mogą stanowić dowodu na skuteczność proponowanych rozwiązań dla ogółu populacji. (Gerontol Pol 2018; 26; 226-228)
Słowa kluczowe: muzykoterapia, senior
Abstract
Music Therapy is still not fully explored as one of the methods assisting in conventional medicine. still is a discipline that is not fully explored. The main assumption in Music Therapy is to eliminate tension, fears and to prevent consequences of daily stress. All over the world research is undertaken to find out the influence of Music Therapy on patients suffering from different diseases. In case of elderly patients, the main point is to try to counteract depression and to alleviate symptoms of dementia and mild cognitive impairment (MCI). Unfortunately, most studies were administered in small cohorts, and can not be considered a proof of effectiveness for the general public. (Gerontol Pol 2018; 26; 226-228)
Key words: music therapy, senior
Wprowadzenie
Pierwsze wzmianki na temat zastosowania muzyko-terapii pochodzą z czasów biblijnych. Już wtedy stoso-wano metody komunikacji za pomocą śpiewu. Muzyko-wanie na wczesnych formach instrumentów, śpiew oraz połączenie obu aktywności z tańcem można uznać za pierwotną formę terapii poprzez dźwięk i ruch.
Rozważając genezę muzykoterapii nie można pominąć osiągnięć starożytnych Greków, którzy nie tylko cenili muzykę za jej walory estetyczne, ale wykształcili cały system filozoficzny dotyczący tego zagadnienia. Staro-żytne systemy skal, choć dziś rzadko stosowane w mu-zyce, nadal mogą być używane przez muzykoterapeu-tów. Przykładowo skala lidyjska była używana podczas lamentacji, a frygijska budziła gwałtowność i niepokój. Wszystkie stosowane systemy muzyczne miały prowa-dzić do oczyszczającego umysł katharsis [1].
Również poszczególne skale w systemie dur-moll łączą się z całym wachlarzem znaczeń emocjonal-
nych. W historii muzyki kompozytorzy nie dobiera-li tonacji swoich kompozycji w sposób przypadko-wy. Właściwy wybór tonacji miał wspływ na prze-kaz dzieła i nastrój, w który słuchacz miał zostać wprowadzony. Użyta tonacja miała również wpływ na brzmienie poszczególnych instrumentów. Tonacja D-dur jest uznawana za tę, która najpełniej oddaje głębię brzmienia skrzypiec, natomiast tonacje bemolowe mają częste zastosowanie w utworach przeznaczonych na instrumenty dęte oraz dla wokalistów.
Założenia muzykoterapii
Muzykoterapia stanowi jeden z najważniejszych fi-larów arteterapii, która stawia sobie za cel wywieranie wpływu na ludzkie emocje i samopoczucie oraz może być uznawana za formę psychoterapii. Głównym aspek-tem pracy muzykoterapeuty jest wywieranie wpływu na stan emocjonalny, umysłowy, a nawet fizyczny pacjenta.

227MUZYKOTERAPIA DLA SENIORA
GERONTOLOGIA POLSKA, 2018, 3
Choć działania związane z użyciem muzyki były znane ludzkości od zarania dziejów, dziś osoby proponują-ce zajęcia muzyczne nie działają wyłącznie intuicyjnie. Muzykoterapia stała się odrębną gałęzią nauki, która łą-czy w sobie wpływy psychologii, medycyny, psychote-rapii i pedagogiki z szeroko pojętą kulturą.
Muzykoterapię możemy podzielić na receptywną (słu-chanie muzyki) oraz czynną (śpiew oraz gra na instru-mentach). W kontekście odbiorcy w wieku senioralnym, zachęta do czynnego muzykowania nie zawsze jest ła-twa, lecz włączenie do świata dźwięków poprzez udział w roli słuchacza nie powinno stanowić większej trudno-ści.
Zarówno muzykoterapię aktywną, jak i receptywną możemy łączyć z innymi formami arteterapeutycznymi, takimi jak choreoterapia, terapia zajęciowa czy relaksa-cja. Wśród metod znajdujących zastosowanie w pracy z pacjentem w wieku senioralnym szczególnym powo-dzeniem cieszą się śpiew, gra na prostych instrumentach czy komponowanie piosenek.
Zajęcia muzyczne mogą być stosowane w formie spo-tkań indywidualnych jak i grupowych. Te drugie, poza walorem terapeutycznym posiadają również wymiar so-cjologiczny, wspomagający integrację w grupie równo-latków. W kwestii doboru materiału muzycznego, moż-na wyróżnić podział na utwory relaksacyjne oraz akty-wizujące [2].
Galińska, wybitna specjalistka w dziedzinie muzyko-terapii, podzieliła działania muzykoterapeutyczne na sie-dem grup w zależności od zastosowania [3]. Wyróżniła takie interwencje jak treningowe, aktywizujące emocjo-nalnie, kontemplacyjne, komunikatywne, kreatywne, re-laksacyjne oraz aktywizujące. Wydaje się, że szczególną rolę pełnią techniki aktywizujące emocjonalnie, które prowadzą słuchacza do przeżycia katharsis dzięki za-stosowaniu muzyki jako katalizatora odczuć. Na kolej-nych pozycjach należy umieścić funkcje kontemplacyjne i aktywizujące. Proponowane wyróżnienie niektórych elementów jest podziałem subiektywnym, wynikającym z obserwacji poczynionych podczas muzycznych spo-tkań z seniorami.
Praktyczne zastosowanie muzykoterapii
Muzykoterapia jako metoda wspomagająca leczenie farmakologiczne może być stosowana m. in. w przypad-ku depresji, demencji oraz łagodnych zaburzeń poznaw-czych (MCI). W chorobie Parkinsona gra na instrumen-tach wpływa na motorykę i płynność ruchu. Słuchanie muzyki oraz czynny udział w jej tworzeniu w znacznym stopniu poprawia jakość życia, nastrój i zmniejsza nie-pokój. Spadek napięcia zaobserwowano również u pa-
cjentów, którzy podczas operacji słuchali muzyki. Już w latach 70. XX wieku dr Maciej Kierył, anestezjolog i muzykoterapeuta, zastosował muzykę podczas zabie-gów operacyjnych. Stworzył on również pojęcie MRM (Mobilna Relaksacja Muzyczna), która działa w opar-ciu o akronim OZURA (Odreagowanie, Zrytmizowanie, Uwrażliwienie, Relaksacja, Aktywizacja) [4].
W Polsce bardzo dużą popularnością cieszy się wy-korzystanie muzyki podczas rehabilitacji, ale nie jest to jedyna forma terapii muzyką, z której korzystają specja-liści różnych dziedzin. Coraz większe znaczenie mają treningi relaksacyjne z użyciem muzyki stosowane w le-czeniu pacjentów narażonych na duży stres. Szczególnie poszukiwane są zajęcia muzyczne i arteterapeutyczne dedykowane pacjentom onkologicznym. W Chinach sto-sowano muzykoterapię jako wsparcie dla pacjentek po mastektomii. U grupy, która poza leczeniem farmakolo-gicznym otrzymała dodatkowy bodziec w postaci muzy-ki obserwowano mniejszy poziom bólu niż w przypadku tej, w której ograniczono się do zastosowania środków przeciwbólowych [5].
Natanson, uznawany za ojca polskiej muzykoterapii, twierdził, iż zastosowanie muzyki wpływa „na całość psychosomatycznego ustroju człowieka”. Muzyka jest stosowana również w ginekologii, geriatrii, neurofizjolo-gii oraz innych działach medycyny [6].
Terapię muzyką wykorzystuje się do oddziaływań na różne układy ludzkiego organizmu. W sferze po-znawczej poprawia nastrój psychofizyczny, wpływa na kształtowanie kompetencji społecznych oraz poprawę procesów myślowych i pamięciowych. Oddziałuje rów-nież na poczucie własnej wartości, a poprzez terapię grupową redukuje poczucie izolacji. Nie można pomijać wymiernych skutków muzykoterapii na redukcję pozio-mu kortyzolu, aktywizację układu limbicznego czy spa-dek ciśnienia krwi przy zastosowaniu odpowiednio do-branych utworów.
Muzykoterapia pacjenta starszego
Podczas pracy z pacjentem w starszym wieku najczę-ściej stosuje się muzykę do celów aktywizacyjnych bądź uspokajających. Przy zastosowaniu aktywnych form muzykoterapii zaobserwowano utrwalanie sprawności psychofizycznej przy regularnym powtarzaniu ćwiczeń. Według popularnego w Skandynawii pojęcia geronto-transcendencji, człowiek może się rozwijać na każdym etapie życia, co idzie w parze z założeniami gerontope-dagogiki.
W przypadku seniorów trzeba wziąć pod uwagę, że stanowią grupę niehomogeniczną, od całkowicie spraw-nych, po pacjentów dotkniętych wielochorobowością.

228 MICHALINA RADZIŃSKA
GERONTOLOGIA POLSKA, 2018, 3
Najczęstszą przyczyną interwencji muzycznych w tej grupie wiekowej jest przeciwdziałanie skutkom depresji, demencji, otępieniu typu alzheimerowskiego oraz defi-cytom w życiu społecznym [2,7-10].
Najważniejszym aspektem działania muzycznego jest podniesienia jakości życia odbiorcy. Celem interwencji jest głównie poprawa samopoczucia oraz zmniejszenie poziomu odczuwanego lęku. Podczas dobierania utwo-rów proponowanych seniorom, ważne jest wzięcie pod uwagę ich preferencji muzycznych. Znaczna część pozy-tywnie reaguje na utwory muzyki klasycznej oraz szla-giery pamiętane z lat młodości. Najlepiej przyjmowane są utwory o pogodnym charakterze i łagodnie kształto-wanej melodyce [6].
Senior jako adresat badań muzykoterapeutycznych – podsumowanie
W licznych opracowaniach dotyczących badań nad wpływem muzyki na podniesienie jakości życia pacjen-tów w wieku 60+ można wyróżnić kilka głównych kie-runków zainteresowań. Badacze na całym świecie sku-piają się głównie na próbach niwelowania stresu oraz łagodzeniu objawów występujących wraz z częstą u tej grupy wiekowej depresją oraz zaburzeniami funkcji po-znawczych. Naukowcy zajmujący się analizowaniem dotychczas przeprowadzonych badań dotyczących uży-cia metod muzykoterapeutycznych w pracy ze starszym pacjentem zgodnie twierdzą, iż bardzo duża część z nich została opracowana na małych grupach, przez co nie mogą być uznawane za miarodajne dla ogółu populacji. Wpływ muzyki na poprawę jakości życia człowieka sta-nowi dziedzinę, w której wciąż pozostaje wiele do od-krycia.
Konflikt interesówBrak / None
Piśmiennictwo
1. Kowalska M. ABC historii muzyki. Kraków: Musica lagellonica; 2001. ss. 23-32.
2. Cylkowska-Nowak M, Strzelecki W, Tobis S. Muzykoterapia pacjenta starszego jako wspomaganie oddziaływania konwencjonalnej medycyny. Gerontol Pol. 2013;4:138-42.
3. Paszkiewicz-Mes E. Muzykoterapia jako metoda wspomagająca leczenie. Hygeia Public Health. 2013;48(2):168-76.
4. http://www.zdrowamuzyka.pl/pdf/mrm.pdf
5. Zhou K, Li X, Li J, Liu M i wsp. A clinical randomized controlled trial of music therapy and progressive muscle relaxation training in female breast cancer patients after radical mastectomy: Results on depression, anxiety and length of hospital stay. Eur J Oncol Nurs. 2015;19(1):54-9.
6. Brudek P, Kierpal P, Gamrowska A. Muzykoterapia jako forma wspierania rozwoju w okresie późnej dorosłości. W: Brudek P, Steuden S, Januszewska I, Gamrowska A. (red.) Oblicza starości we współczesnym świecie. Perspektywa psychologiczno-medyczna. Lublin: Wydawnictwo KUL; 2015. ss. 241-255.
7. Tomomi U, Yoshimi S, Mai S i wsp. Effects of music therapy on behavioral and psychological symptoms of dementia: A systematic review and meta-analysis. Ageing Res Rev. 2013;12:628-41.
8. Gómez-Romero M, Jiménez-Palomares M, Rodríguez-Mansilla J. Benefits of music therapy on behaviour disorders insubjects diagnosed with dementia: A systematic review. Neurologia. 2017;32(4):253-63.
9. Yingshi Z, Jiayi C, Li A, Fuhai H i wsp. Does music therapy enhance behavioral and cognitive function inelderly dementia patients? A systematic review and meta-analysis. Ageing Res Rev. 2017;35:1-11.
10. Schall A, Haberstroh J, Pantel J. Time Series Analysis of Individual Music Therapy in Dementia. Gero Psych. 2015;28(3):113-22.

GERONTOLOGIA POLSKA 2018; 26; 229-235 CASE REPORT / OPIS PRZYPADKU Zgłoszono 6.02.2018 zaakceptowano 10.04.2018
Correspondence address: Abdalla Saad Abdalla Al-Zawi; Basildon & Thurrock University Hospital, Essex, United Kingdom [email protected]
Ó Akademia Medycyny
Coexistence of primary renal clear cell carcinoma with primary breast invasive lobular carcinoma:
a literature review and case report
Abdalla Saad Abdalla Al-Zawi, Anita Lazarevska, Mohammed Omer, Elizabeth Tan
Basildon & Thurrock University Hospital, Essex, United Kingdom
Abstract
Introduction. The concept of concomitant co-existing malignancies has been expanding since the report from Warren and Gates in 1932, and its aetiology remains controversial. Despite it being a rare occurrence, the frequency of Multiple Pri-mary Malignant Neoplasms (MPMNs) is increasing. MPMNs are considered synchronous when they present simultane-ously or within 6 months of one another. If the second cancer has been diagnosed after six months, they are known as me-tachronous. Case report. In this paper we present a case of synchronous primary breast invasive lobular carcinoma and renal clear cell carcinoma in a 75 years old patient. (Gerontol Pol 2018; 26; 229-235)
Key words: renal clear cell carcinoma, breast invasive lobular carcinoma, nephrectomy, wire-guided wide local excision, oestrogen, letrozole
Introduction
The diagnosis of two or more origin independent pri-mary cancers with unrelated histopathological features in a patient, is called Multiple Primary Malignant Neo-plasms (MPMNs). The term MPMNs was first used by Billroth in 1889, before being defined by Warren and Gates in 1932 [1].
MPMNs are considered synchronous when they present simultaneously or within 6 months of one an-other. If the second cancer has been diagnosed after six months, they are known as metachronous.
The co-existence of different primary malignancies is rare. This implies important diagnostic and therapeutic challenges, as the different cancers could be misdiag-nosed as one disease progression.
The MPMNs detection rate is rising, most likely due to an increase in the aging population, more clinician awareness of MPMNs, better reporting facilities and im-provement in diagnostic techniques. Most synchronous multiple primary tumours are seen in the genitourinary system and gastrointestinal system [2], although they may also be seen in other organs.
As breast cancer is the most common cancer in fe-males [3], it has been reported to be diagnosed with other primary cancers. The sites of reported synchronous or metachronous cancers associated with breast cancers are the contralateral breast [4], thyroid [5,6], prostate [7], colon [8,9], kidney [10-12], lung [13], skin [1,13,14],
lymphoma [1], oesophagus [15,16], stomach [17] and urinary bladder [14].
Case report
A female patient aged 75 years, presented with a re-cent history of a painful right breast lump. She had longstanding breast asymmetry, but no risk factors for breast carcinoma apart from her age. She underwent a hysterectomy and bilateral oophorectomy at age 51 for benign fibroids. She suffered from vertigo and hyperten-sion only. Clinically she had obvious breast asymme-try where the right was larger than the left. There was a clinically palpable lump measuring about 6 x 5 cm in the right breast upper outer quadrant (P3), but there was no associated lymphadenopathy.
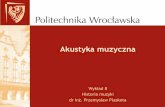
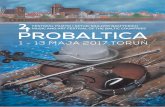
Mammogram showed right breast soft tissue density with spiculated margins, in addition to benign calcifica-tions (figures 1 & 2). This was reported as an M5 score in the BIRAD System (Breast Imaging Reporting and Data System).
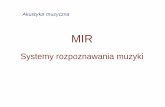
In the right breast ultrasound, there was an irregular hypoechoic lesion measuring 50 x 34 x 34 mm. It was suspicious of malignancy (Figure 3) and a BIRADS score of U5 was given.
An imaging guided biopsy revealed an invasive mam-mary carcinoma. Staining for E-Cadherin was negative, in keeping with lobular type carcinoma and Ki-67 pro-
230 ABDALLA SAAD ABDALLA AL-ZAWI, ANITA LAZAREVSKA, MOHAMMED OMER, ELIZABETH TAN
GERONTOLOGIA POLSKA, 2018, 3
liferation index was 10%. The oestrogen receptors (ER) and progesterone receptors (PR) were positive, with both scores 8/8. Her-2 receptor status was borderline (2+). After FISH (Fluorescence in situ hybridization) testing, Her-2 was not amplified, so this case was regarded as negative for Her-2 overexpression.
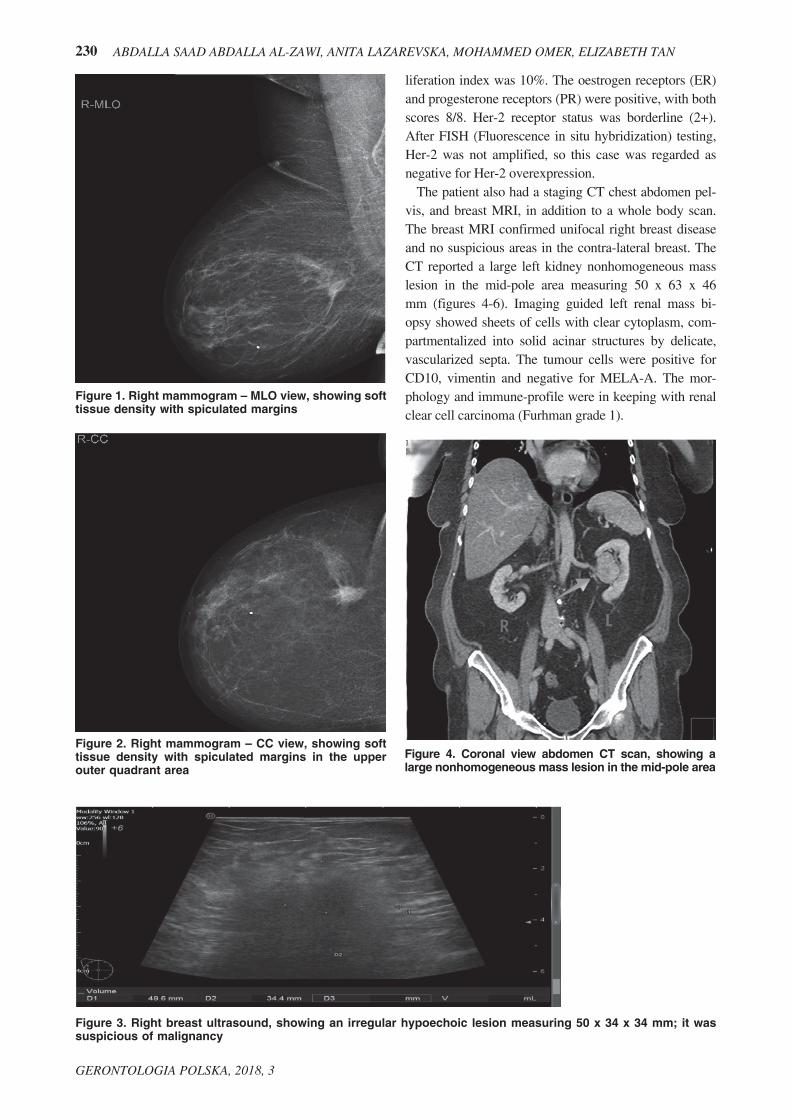
The patient also had a staging CT chest abdomen pel-vis, and breast MRI, in addition to a whole body scan. The breast MRI confirmed unifocal right breast disease and no suspicious areas in the contra-lateral breast. The CT reported a large left kidney nonhomogeneous mass lesion in the mid-pole area measuring 50 x 63 x 46 mm (figures 4-6). Imaging guided left renal mass bi-opsy showed sheets of cells with clear cytoplasm, com-partmentalized into solid acinar structures by delicate, vascularized septa. The tumour cells were positive for CD10, vimentin and negative for MELA-A. The mor-phology and immune-profile were in keeping with renal clear cell carcinoma (Furhman grade 1).
Figure 1. Right mammogram – MLO view, showing soft tissue density with spiculated margins
Figure 2. Right mammogram – CC view, showing soft tissue density with spiculated margins in the upper outer quadrant area
Figure 3. Right breast ultrasound, showing an irregular hypoechoic lesion measuring 50 x 34 x 34 mm; it was suspicious of malignancy
Figure 4. Coronal view abdomen CT scan, showing a large nonhomogeneous mass lesion in the mid-pole area

231COEXISTENCE OF PRIMARY RENAL CLEAR CELL CARCINOMA WITH PRIMARY...
GERONTOLOGIA POLSKA, 2018, 3
The multidisciplinary team recommended commencing hormonal manipulation of breast cancer with aromatase inhibitor letrozole. This was followed by laparoscopic left nephrectomy. The postoperative histopathology revealed 50 x 30 x 20 mm grade 2, clear cell carcinoma without involvement of the renal vein, renal pelvis or ureter (fig-ure 7). There was also no small vessel lympho-vascular invasion. One lymph node removed was free from cancer cells. After 6 months from the initial diagnosis and hor-monal manipulation of the right breast cancer, a repeat right breast ultrasound was consistent with a possible par-tial radiological response. The tumour measured only 19 mm in maximum diameter. The patient underwent wire guided wide local excision of the breast cancer with sen-tinel lymph node biopsy (figure 8). The postoperative his-tology results were consistent with 25 mm grade 2, inva-sive lobular carcinoma admixed with invasive lobular car-cinoma in situ (figure 9). The abnormality was completely excised and no lympho-vascular invasion was detected. Three removed lymph nodes were free from metastatic disease. The patient had an uneventful recovery and is currently under surveillance.
Figure 5. Sagittal view abdomen CT scan, showing a large nonhomogeneous mass lesion in the mid-pole area
Figure 6. Axial view abdomen CT scan, showing a large nonhomogeneous mass lesion in the mid-pole area
Figure 7. Clear cell renal carcinoma
Figure 8. Lumpogram of a wire guided wide local excision of right breast cancer, showing the removed breast cancer with good radiological resection margins

232 ABDALLA SAAD ABDALLA AL-ZAWI, ANITA LAZAREVSKA, MOHAMMED OMER, ELIZABETH TAN
GERONTOLOGIA POLSKA, 2018, 3
Discussion
The coexistence of two or more primary carcinomas simultaneously or within six months of each other are known as synchronous tumours. If the tumours develop consequently after six months, they are called metachro-nous [18]. Up to eight primary malignancies have been diagnosed in a single patient, two were synchronous and the other six were metachronous [19].
Although there are no clear answers yet behind mul-tiple malignancy aetiology, there are some theories that have been discussed. Exposure of multiple organs to car-
cinogenic factor is one of those theories [9]. This is seen in the relationship between smoking and lung, nasopha-ryngeal, oesophageal, colorectal [20], breast [21] and bladder cancer [22].
The second theory is the genetic predisposition to BRCA1 and BRCA2 mutations, which are associated with breast and ovarian cancer [10,23] (see table I). This is known as Hereditary Breast and Ovarian Cancer syndrome (HBOC). Another example is MEN2 or Sip-ple’s syndrome, which is characterised by the presence of medullary thyroid carcinoma, pheochromocytoma, and parathyroid adenoma [24]. Patients with Lynch syn-drome, also called hereditary non-polyposis colorectal cancer (HNPCC) are at high risk of developing endo-metrial ovarian, stomach, small intestine, pancreatic, re-nal, brain, and biliary tree cancer. Lynch syndrome can be caused by a mutation in any of the MMR (Mismatch Repair Genes), including MLH1, MSH6,PMS1 and PMS2 [25]. Li-Fraumeni syndrome is a rare hereditary autosomal dominant cancer disorder. It is due to a ger-mline mutation in TP53. The patients may develop sar-coma, leukaemia, brain cancers, adrenal cortex cancers and breast cancers [26].
The third theory is the effect of a single primary can-cer treatment. Chemotherapy and radiotherapy in breast cancer treatment results in an increased risk of develop-ing acute non-lymphocytic leukaemia [27]. Solid organs of metachronous malignancy usually take longer to de-
Figure 9. Breast tissue infiltrated by a lobular carcinoma
Table I. Hereditary MPMNs (Multiple Primary Malignant Neoplasms)
Hereditary conditions Related cancers
Neurofibromatosis type 1(NF1) Breast cancer
Pheochromocytoma
PTEN
Phosphatase and Tensin homolog Gene
/Cowden syndrome
Breast cancer
Renal cell carcinoma
Thyroid cancer
Lynch syndrome
Colonic cancer
Endometrial cancer
Gastric cancer
Renal cancer
Pancreatic cancer
Multiple Endocrine Neoplasia Type II [MEN2] [Sipple’s Syn-drome]
Pheochromocytoma
Thyroid Medullary carcinoma
Parathyroid adenoma
Li-Fraumeni syndrome
Endometrial cancer
Ovarian cancer
Gastric cancer
Pancreatic cancer
Renal cell carcinoma
Bile duct adenocarcinoma
Breast and Ovarian Cancer syndrome (HBOC).
BRCA1 & BRCA2 mutation
Breast carcinoma
Ovarian cancer

233COEXISTENCE OF PRIMARY RENAL CLEAR CELL CARCINOMA WITH PRIMARY...
GERONTOLOGIA POLSKA, 2018, 3
velop, such as a breast secondary angiosarcoma after lumpectomy and radiotherapy [28-30]. Theodor Billroth (1829-1894) is a German surgeon. In 1863 he reported for the first time, the presence of multiple primary ma-lignancies in the same patient [14]. Multiple Primary Malignant Neoplasms (MPMNs) may involve a single organ or multiple different organs [31]. The co-existence of renal cancer with other primary cancers has also been reported. The sites of such malignancies are the ova-ries [32,33], colon [9,34], lymphoma [ 35], breast [11], prostate [31], pancreas [36] and urinary bladder [31,37]. Hereditary conditions known to have MPMN are neuro-fibromatosis type 1 (NF1), which is associated with an increased risk of breast cancer [38] and pheochromocy-toma, [39,40] and Cowden syndrome (CS), associated with renal and breast cancer [41].
The sites of reported synchronous or metachronous cancers associated with breast cancers are the contralat-eral breast [4], thyroid [5,6,42], prostate [7], colon [8], kidney [10-12], lung [13,43], skin [1,13,14] , lymphoma [1], oesophagus [15,16], stomach [17], urinary bladder [14], uterus [19] and adrenal pheochromocytoma [40].
The rise in detection rate of multiple co-existing pri-mary cancers could be related to several factors, such as an increase in the overall cancer risk in the aging popu-
lation, better diagnostic modalities, increased reporting rate and more awareness of the existence of Multiple Primary Malignant Neoplasms (MPMNs).
Conclusion
The MPMNs detection rate is rising. This is most like-ly related to an increase in the aging population, more clinician awareness of MPMNs, better reporting facili-ties and improvement in diagnostic techniques.
In the case of diagnosed cancer, any suspicious addi-tional abnormality, especially if not responding to sys-temic treatment, should be biopsied. Attention should be paid to differentiate between double primary and meta-static tumours; this will require proper clinical and path-ological assessment.
AcknowledgmentWe thank Ms Julie Jobson, senior radiographer from Breast Unit Basildon & Thurrock University Hospital, for help in selection of radiological images that greatly improved the manuscript.
Conflict of interestNone
References
1. Williamson CW, Paravati A, Ghassemi M, et al. Five Simultaneous Primary Tumours in a Single Patient: A Case Report & Review of Literature. Case Rep Oncol. 2015;8:432-8.
2. McGarry RC, Papiez L, Williams M. Stereotactic body radiation therapy of early stage non-small-cell lung carcinoma: phase I study. Int J Radiat Oncol Biol Phys 2005;63:1010-5.
3. DeSantis C, Ma J, Bryan L, et al. Breast cancer statistics.CA Cancer J Clin. 2013;64:52-62, 2014.
4. Padmanabhan N, Subramanyan A, Radhakrishna S. Synchronous Bilateral Breast Cancers. J Clin Diagnos Res. 2015;9(9):5-8.
5. Ghosh S, Rao PB, Sarkar S, et al. A rare case of a synchronous anaplastic carcinoma thyroid with ductal carcinoma breast. Case Rep Oncol Med 2014;article ID 468159.
6. Zhong J, Lei J, Jiang K, et al. Synchronous papillary thyroid carcinoma and breast ductal carcinoma: A rare case report and literature review. Medicine. 2017;96(7).
7. Kantziou M, Moisidis K, Tailachidis P, et al. Coexistence of Breast and Prostate Cancers in a 79-Year-Old Man. 2017;39(8):71-2.
8. Akasbi Y, Arifi S, Najib R, et al. An Unusual Case of Multiple Primary Carcinomas: Breast Cancer and Rectal Adenocarcinoma in a Single Patient: Report of a Case and Review of the Literature. Arch Surg Oncol. 2015;1:1. DOI: 10.4172/2471-2671.1000107.
9. Ahmadnia H, Molaei M. Concomitant presence of renal cell carcinoma and adenocarcinoma of the colon. Saudi J Kidney Dis Transpl. 2009;20:1081-2.
10. Ahmed O, Tahir A. Metachronous double malignancy involving the kidney and the breast: A case report. Case Rep Clin Med. 2014;3:2:7-69.
11. Ureyen O, Dadali E, Akedeniz F, et al. Co-existent breast and renal cancer. Ulus Cerrahi Derg. 2015; 31:238-40. DOI: 10.5152/UCD.2015.2874.
234 ABDALLA SAAD ABDALLA AL-ZAWI, ANITA LAZAREVSKA, MOHAMMED OMER, ELIZABETH TAN
GERONTOLOGIA POLSKA, 2018, 3
12. Kurlekar UA, Rayate AS. Synchronous Primary Malignancies in Breast and Kidney: A Rare Case Report. Indian J Surg. 2015:77(11):6-9.
13. Kurul S, Akgun Z, Saglam EK, et al. Successful treatment of triple primary tumor. Intern J Surg Case Rep. 2013;4:1013-6.
14. Pastore AL, Palleschi G, Autieri D, et al. Synchronous primary neoplasms of the bladder, skin and breast in a male patient: a case report. World J Surg Oncol. 2013;11:282.
15. Singh A, Khare IC, Dixit AK, et al. Successfully treated synchronous double malignancy of the breast and esophagus: a case report. JMCR. 2010;4:169.
16. Akiyama Y, Iwaya T, Shioi Y, et al. Successfully treated advanced esophageal cancer with left axillary lymph node metastasis and synchronous right breast cancer: a case report. Surg Case Rep. 2015;1(1):94.
17. Kashiwagi S, Onoda N, Asano Y, et al. A rare recurrence of bilateral breast cancer in the esophagus coincidentally associated with primary gastric cancer: a case report. J Med Case Rep. 2014:8(58).
18. Tziris N, Dokmetzioglou J, Giannoulis K, et al. Synchronous and metachronous adenocarcinomas of the large intestine. Hippokratia. 2008;12(3):150-2.
19. Zhao J, Tan Y, Wu Y, et al. A rare case of eight multiple primary malignant neoplasms in a female patient: A case report and review of the literature. Oncology Letters. 2015;9:587-90.
20. Ray G, Henson DE, Schwartz AM. Cigarette smoking as a cause of cancers other than lung cancer: An exploratory study using the SEER Program. Chest. 2010;138:491-9.
21. Bjerkaas E, Parajuli R, Engeland A, et al. The association between lifetime exposure and breast cancer mortality-results from a Norwegian cohort. Cancer Med. 2014;3(5);1448-57.DOI;10.1002/cam4.304.
22. Dalal S, Garg P, Nityasha Jain A. Synchronous double malignancy: Adeno-carcinoma of caecum and renal cell carcinoma. Int J Gastroenterol. 2006;6(4).
23. Petrucelli N, Daley MB, Bars Culver JO, et al. (Updated 6/ 19/2007). BRCA1 and BRCA2 hereditary breast and ovarian cancer. In: GeneReviews at GeneTests: Medical Genetics Information Resource (database online). Copyright, University of Washington, Seattle. 1997-2017. Available from: http://www.genetests.org. Accessed December 26, 2017.
24. Romei C, et al. Modifications in the papillary thyroid cancer gene profile over the last 15 years. J Clin Endocrinol Metab. 2012;97:1758-65.
25. American cancer Society. Family cancer Syndromes. www.cancer.org. Viewed on 26 December 2017.
26. Zhou R, Xu A, Gingold J, et al. Li–Fraumeni Syndrome Disease Model: A Platform to Develop Precision Cancer Therapy Targeting Oncogenic p53. Trends Pharmacol Sci. 2017;38(10):908-27.
27. Curtis RE, Boice RE, Boice JD Jr, et al. Risk of leukemia after chemotherapy and radiation for breast cancer. N Engl J Med. 1992;326:1745-51.
28. Frey JD, Levine PG, Darvishian F, et al. Angiosarcoma of the Breast Masquerading as Hemangioma: Exploring Clinical and Pathological Diagnostic Challenges. Arch Plast Surg. 2015 March;42(2):261-3.
29. Chouhou L, Moussaoui DR, Khaled H, et al. Les angiosarcomes du sein : à propos de trois observations [Breast angiosarcomas: three case reports]. Ann Chir. 200;128:43-8.
30. Al-Zawi ASA, Salih A, Idaewor P, et al. Recurrent Primary Bilateral Breast Angiosarcoma. Case Report & Literature Review. IJMRPS. 2017;4(8). DOI- 10.5281/zenodo.838937.
31. Tiwari P, Tripathi A, Bansal P, et al. Synchronous primary cancers of urinary bladder and kidney and prostate. Saudi J Kidney Dis Transpl. 2012;23:786-9.
32. Huang KH, Chueh SC, Huang SY, et al. Coexistence of ovarian cancer and renal cell carcinoma. J Formos Med Assoc. 2007;106(3):15-9.
33. Tsili AC, Charisiadi, A, Koliopoulos G, et al. Synchronous primary tumors of the kidney and the ovaries: Imaging findings. Radiol Case. 2008;2(5):2-8.
34. Papalampros AE, Petrou AS, Mantonakis EI, et al. Coexistence of a colon carcinoma with two distinct renal cell carcinomas: a case report. J Med Case Reports. 2011;5(1):134.
35. Kunthur A, Wiernik PH, Dutcher JP . Renal parenchymal tumors and lymphoma in the same patient: case series and review of the literature. Am J Hematol. 2006. 81:271-80. DOI/abs/10.2214/AJR.13.10669.
36. Ismail TO, Janane A, Hajji F, et al. Synchronous primary tumours of the kidney and pancrease: Case report. African J Urol. 2010;16(4);128-31.

235COEXISTENCE OF PRIMARY RENAL CLEAR CELL CARCINOMA WITH PRIMARY...
GERONTOLOGIA POLSKA, 2018, 3
37. Rabbani F, Grimaldi G, Russo P. Multiple Primary malignancies in renal cell carcinoma. J Urol. 1998;160(4):1255-9.
38. Howell SJ, Hockenhull K, Salih Z, et al. Increased risk of breast cancer in Neurofibromatosis type 1: Current insights. Breast Cancer. (Dove Med Press). 2017;21(9):531-6. doi: 10.2147/BCTT.S111397.
39. Kumar KVSH, Shaikh A, Sandhu Prusty ASP. Neurofibromatosis 1 with pheochromocytoma. Indian J Endocrinol Metabol. 2011;15(4).
40. Demirpence MM, Bahceci M, Dolek D, et al. A very rare association; coexistence of breast cancer, pheochromocytoma and neurofibromatosis type 1 in a female patient. Intern J Case Rep Med. 2013;6.
41. Haas NB, Nathanson KL. Hereditary kidney cancer syndromes. Adv Chronic Kidney Dis. 2014;21:81-90.
42. Wang CC, Shen WL, Lee HH, et al. Thyroid Cancer Presenting with Concomitant Metastatic Breast Cancer in the Thyroid. J Cancer Res Pract. 2014;1(3):248-53.
43. Acharya P, Ramakrishna A, Kanchan T, et al. Dual primary malignancy: A rare organ combination. Case Rep Pulmonol. 2014;2014:760631.


GERONTOLOGIA POLSKA, 2018, 3
Regulamin ogłaszania prac w kwartalniku Gerontologia Polska
Gerontologia Polska jest oficjalnym czasopismem Polskiego Towarzystwa Gerontologicznego, w którym są publi-kowane recenzowane artykuły poglądowe, oryginalne prace badawcze z zakresu biologii starzenia się, gerontologii klinicznej i społecznej, a także problemów interdyscyplinarnych, prace kazuistyczne (opisy przypadków), listy, re-cenzje książek oraz komentarze redakcyjne.
Prace należy nadsyłać drogą elektroniczną na adres: [email protected]
1. Do druku przyjmowane są prace w języku polskim lub angielskim. Zaakceptowane do druku prace w j. angiel-skim ukazują się w pierwszej kolejności.
2. Prace o charakterze doświadczalnym muszą być w zgodzie z wymogami Konferencji Helsińskiej. Autorzy muszą uzy-skać pisemną zgodę osób badanych, po wcześniejszym poinformowaniu ich o przebiegu badań i o ewentualnych szko-dliwościach z nich wynikających. Prace, których przedmiotem jest człowiek, mogą być wykonywane i publikowane tylko za zgodą Komisji Bioetycznej i nie mogą ujawniać ich danych osobowych bez załączenia ich pisemnej zgody.
3. Nadesłanie pracy do druku jest jednoznaczne ze stwierdzeniem, że praca nie została zgłoszona do innego czasopisma. 4. Manuskrypty niekompletne lub przygotowane w stylu niezgodnym z zasadami podanymi niżej redakcja odsyła
Autorom bez oceny merytorycznej. Artykuły przygotowane zgodnie z wymogami poniżej zostają zarejestrowane i przekazane do oceny niezależnym recenzentom. Akceptacja pracy do druku odbywa się na podstawie pozytyw-nych opinii recenzentów.
5. Data złożenia pracy w Redakcji, jak również data jej przyjęcia do druku, są umieszczone na początku drukowanej pracy.
6. Prace są recenzowane poufnie i anonimowo (podwójna ślepa recenzja) przez niezależnych Recenzentów z grona ekspertów w danej dziedzinie.
7. Redakcja zapoznaje Autorów z tekstem recenzji, bez ujawnienia nazwisk recenzentów.8. Recenzent może uznać pracę za:
– nadającą się do druku bez dokonania poprawek,– nadającą się do druku po dokonaniu poprawek według wskazówek Recenzenta, bez konieczności ponownej
recenzji,– nadającą się do druku po dokonaniu poprawek według wskazówek Recenzenta i po ponownej recenzji pracy,– nie nadającą się do druku.
9. Prace wymagające korekty zostaną niezwłocznie przesłane Autorom wraz z uwagami Recenzenta i Redakcji.10. W przypadku zakwalifikowania pracy do druku Autorzy zostaną o tym fakcie poinformowani e-mailowo lub tele-
fonicznie.11. Korekty, w formie elektronicznej należy zwrócić w terminie do 7 od daty wysłania z Redakcji. W wyjątkowych
wypadkach Redakcja może przedłużyć termin zwrotu korekty po wcześniejszym uzgodnieniu tego faktu z jej przedstawicielem.
12. Prace niezakwalifikowane do druku zostaną przez Redakcję zniszczone.13. Redakcja Naukowa zastrzega sobie prawo do dokonywania koniecznych poprawek i skrótów bez porozumienia
z Autorami. 14. Prace zgłaszane do druku należy przesłać w formie elektronicznej (e-mail).15. Objętość prac oryginalnych nie może przekraczać 10 stron, 12 stron dla poglądowych i 8 stron dla prac kazu-
istycznych. Na jednej stronie nie można umieścić więcej niż 1800 znaków wraz ze spacjami. 16. Wersja elektroniczna pracy powinna być dostarczona e-mailem. Materiał ilustracyjny należy przygotować w for-
macie TIFF dla materiałów zdjęciowych i skanowanych, a dla grafiki wektorowej w programach Corel Draw do wersji X7 lub Adobe Ilustrator do wersji CC(2014), dla wykresów i diagramów MS Excel lub Word.
17. Tekst oraz materiał ilustracyjny powinny być zapisane w oddzielnych plikach np. nazwa-tekst.doc, nazwa-tabela.doc.18. Obowiązkowy układ pracy: Strona tytułowa:
o tytuł artykułu w języku polskim i angielskim,o imiona i nazwiska Autorów,o pełna nazwa instytucji,o słowa kluczowe w języku polskim/angielskim (do 6 słów),o pełny adres korespondencyjny jednego z Autorów,

GERONTOLOGIA POLSKA, 2018, 3
o streszczenie pracy w języku polskim (200-250 słów w przypadku prac oryginalnych oraz 100-150 w przypad-ku prac poglądowych i opisów przypadków klinicznych; struktura jak w tekście głównym),
o streszczenie pracy w języku angielskim (200-250 słów w przypadku prac oryginalnych oraz 100-150 w przy-padku prac poglądowych oraz opisów przypadków klinicznych; struktura jak w tekście głównym),
o należy wyszczególnić wszystkie źródła finansowania wykonanej pracy naukowej.Układ tekstu głównego (w przyjętym układzie dla prac oryginalnych):
o wstęp,o cel pracy,o materiał i metody,o wyniki,o omówienie,o wnioski,o podziękowania,o spis piśmiennictwa.
19. Ryciny, tabele, wykresy i fotografie do włączenia w tekst należy nadsyłać oddzielnie, poza tekstem, w którym muszą być zacytowane. Wszystkie powinny być ponumerowane zgodnie z kolejnością występowania w pracy i opisane w języku polskim i angielskim (tabele - numeracja cyframi rzymskimi; ryciny, wykresy i fotografie – numeracja cyframi arabskimi).
20. Spis piśmiennictwa powinien ograniczyć się do niezbędnych pozycji cytowanych w pracy, w przypadku prac ory-ginalnych do 20, a poglądowych do 40 pozycji. Piśmiennictwo należy przytoczyć w kolejności cytowań w tek-ście.
21. Każdą publikację podaje się w tekście za pomocą cyfry arabskiej w nawiasie kwadratowym.22. Cytowanie w spisie piśmiennictwa powinno mieć następujący układ: dla czasopisma: nazwiska autorów z inicjałami imion, oddzielone przecinkami, zakończone kropką (jeśli licz-
ba autorów cytowanej pracy przekracza trzy osoby, to pozostałych należy zaznaczyć skrótem: „i wsp.” lub „et al.”), tytuł artykułu, kropka, nazwa czasopisma przytoczona w skrócie wg Index Medicum, kropka, spacja, rok, średnik, tom, dwukropek, pierwsza i ostatnia strona – (np.: 1. Jakobsson U, Hallberg IR. Loneliness, fear and quality of life among elderly in Sweden: a tender perspective. Aging Clin Exp Res. 2005;17(6):494-501.
dla tytułu rozdziału z książki: nazwiska autorów z inicjałami imion, oddzielone przecinkami, zakończone kropką, tytuł rozdziału, kropka, W: nazwiska redaktorów (red.), kropka, tytuł książki, kropka, miejscowość, dwukropek, spacja, wydawca, średnik, spacja, rok wydania, kropka – w przypadku wybranych stron – spacja, ss., spacja, pierwsza i ostatnia strona, kropka – np.: Wojszel ZB, Bień B. Wielkie problemy geriatryczne – rola zespołu terapeutycznego w opiece nad pacjentem. W: Kędziora-Kornatowska K, Muszalik M (red.). Kompen-dium pielęgnowania pacjentów w starszym wieku. Podręcznik dla studentów i absolwentów kierunku pielę-gniarstwo. Lublin: Wydawnictwo Czelej; 2007. ss. 97-114.
Dopuszcza się również cytowania ze źródeł elektronicznych.23. Praca powinna być zredagowana możliwie krótko, bez zarzutu pod względem stylistycznym, zgodnie z obowią-
zującą pisownią.24. Należy używać międzynarodowych (zgodnie z zasadami polszczyzny) nazw leków. Dopuszcza się podawanie
nazw handlowych w nawiasach.25. Skróty powinny być wyjaśnione w tekście w miejscu, w którym się pojawiają po raz pierwszy.26. Wraz z pracą należy złożyć Deklarację Konfliktu Interesów oraz List Przewodni z oświadczeniem Autorów,
że praca nie została i nie zostanie złożona do druku w innym czasopiśmie oraz że nie zachodzą zjawiska: „guest authorship” i „ghostwriting”.
27. Pierwszy autor/autor do korespondencji otrzymują bezpłatnie 1 egzemplarz czasopisma z wydrukowanym artykułem.28. Nie przewiduje się honorariów autorskich29. Prawa autorskie: Maszynopis zakwalifikowany do druku w kwartalniku staje się własnością czasopisma Geronto-
logia Polska. Wydawca nabywa na zasadzie wyłączności ogół praw autorskich do wydrukowanych prac (w tym prawo do wydawania drukiem, na nośnikach elektronicznych-CD i innych oraz w Internecie). Bez zgody wydaw-cy dopuszcza się jedynie drukowanie streszczeń.
30. Redakcja Gerontologii Polskiej posiada własną stronę internetową, na której są zamieszczane pełne wersje druko-wanych prac, jak również istotne wiadomości.
GERONTOLOGIA POLSKA, 2018, 3
Submission Manuscript Guidelines
The Polish Gerontology is the official journal for the Polish Society of Gerontology. The quarterly publishes peer--reviewed reports, original research papers on the biology of ageing, clinical and social gerontology, as well as artic-les on interdisciplinary issues relating to various aspects of the ageing process.
Please submit your papers electronically at: [email protected]
Instructions for authors
1. Only papers written in Polish or English are accepted , however, papers in English that have been approved for publication shall be published first.
2. In scientific investigations involving human subjects, experiments should be performed in accordance with the ethical standards formulated in the Helsinki Declaration. Informed consent for the research must be obtained from all participants and all clinical investigations. For papers involving human subjects, adequate documen-tation should be provided to certify that appropriate ethical safeguards and protocols have been followed ac-cording to the responsible Bioethical Committee on human experimentation (institutional or regional). Names should not be published in written descriptions, photographs, sonograms, CT scans, etc., nor should pedigrees, unless information is essential for scientific purposes and a patient (or a parent, or a guardian) has given their written informed consent for publication.
3. Manuscripts are received with the explicit understanding that they are not under simultaneous consideration by any other publication. Submission of an article implies that the work described has not been published previo-usly.
4. Manuscripts that are incomplete or whose style does not follow the below guidelines shall be returned to the Au-thors without being evaluated. Articles following the below guidelines shall be registered and sent to indepen-dent reviewers to be evaluated. A paper shall be accepted for publication based on reviewers’ positive opinions.
5. The dates of submitting and acceptance for publication are labeled at the end of each manuscript.6. Submitted manuscripts are anonymously reviewed by two impartial experts to determine their originality (“do-
uble-blind review”), scientific merit, and significance to the field.7. Reviewers shall remain anonymous, but their comments will be available to authors.8. There are several types of decision possible: accept the manuscript as submitted; accept it with revision; accept it
and invite the authors to revise the manuscript before a final decision is reached; accept it with encouragement to resubmit it after extensive revision; outright rejection.
9. Page proofs with reviewer’s remarks will be sent to corresponding author for examination and corrections.10. Information about accepting the manuscript for publication will be sent to the corresponding author.11. Corrected proofs should be returned to the Editor within seven days of posting by the Editor. Authors are re-
sponsible for obtaining the Editor’s permission for any changes in the time for returning proofs.12. When submitted manuscripts are not accepted for publication, they will be destroyed according to the Editorial
office’s schedule.13. The Editors reserve the right to make corrections in style and nomenclature without Authors’ permission.14. Authors should return the final, revised manuscript by e-mail: [email protected]. Manuscripts of original papers should not exceed 10 pages, review articles – 12 pages, case reports – 8 pages.
One page is generally limited to 1800 characters including spacing.16. The electronic version of the text should be submitted as an MS Word 98 or above. All illustration and scan files
should be in the TIFF format. For vector graphics, the digital formats of Adobe Illustrator for version CC(2014) and Corel Draw for version X7 are accepted; for graphs and diagrams - MS Excel or MS Word.
17. The text and figures must be uploaded as separate files. Files should be named with the corresponding Author’s surname and “text.doc”, “fig l.doc” ,”fig2.doc” name and extension formats, etc.
18. The paper should be laid out as follows: Provide the following data on the title page (in the order given): The article’s title (English and Polish), Authors’
names and institutional affiliations, the name of department(s) and institution(s) to which the work should be attri-buted, keywords (English/Polish, maximum of 6 keywords), full postal address of the corresponding Author, an abstract in Polish (maximum length of 200 – 250 words in case of original works and 100 – 150 in case of review articles or clinical cases. An abstract should state briefly the purpose of the research, principal results and major

GERONTOLOGIA POLSKA, 2018, 3
conclusions. An abstract in English (maximum length of 200 – 250 words in case of original works and 100 – 150 in case of review articles or clinical cases, an abstract should state briefly the purpose of the research, principal results and major conclusions, source(s) of support in the form of grants, equipment, drugs, or all of these.
Arrangement of the article (for original papers): Introduction, Abstract/Purpose of the work Experimental/Mate-rial and methods, Results, Discussion, Conclusions, Acknowledgements, References.
19. Tables, illustrations, vector graphics and photographs should be prepared and submitted on separate pages. All figures should be numbered in the order of their citation in the text and legends should be in Polish and English (tables - Roman numerals; illustrations, vector graphics and photographs - Arabic numerals).
20. References should exceed in number, and should in general be limited according the paper type: for original pa-pers – up to 20, for review articles – up to 40 items. They must be numbered in their order of appearance in the text.
21. References should be identified in the text, tables, and legends by Arabic numerals in square brackets. 22. It is allowed to use the following style for the references list: surname and initials of all authors separated by a
comma, followed by a full stop, then the article title (or the book title), a full stop, the name of the journal should be abbreviated according to the style used in the Index Medicus, the year, a semicolon, the volume number, a co-lon, the first and the last page (for books: the city, a colon, the publisher, a semicolon, the year, a colon, pages). When there are more than three authors, only the first six authors are listed, followed by „et al.”, i.e.: 1. Jakobsson U, Hallberg IR. Loneliness, fear and quality of life among the elderly in Sweden: a tender perspective. Aging Clin Exp Res. 2005;17(6):494-501. 2. Wojszel ZB, Bień B. Wielkie problemy geriatryczne – rola zespołu terapeutycz-nego w opiece nad pacjentem. In: Kędziora-Kornatowska K, Muszalik M, editors. Kompendium pielęgnowania pacjentów w starszym wieku. Podręcznik dla studentów i absolwentów kierunku pielęgniarstwo. Lublin: Wydaw-nictwo Czelej; 2007. p. 97-114.
Quoting from electronic sources is accepted. 23. A paper ought to be brief and observe general style and spelling rules. 24. International generic rather than trade names of drugs should be used. Trade or manufacturers’ names should only
be used in brackets.25. All abbreviations should be spelt out in full the first time they are used.26. A paper submitted for publication should be accompanied by a Declaration of ‘Conflict of Interest’ and a ‘Cover
Letter’ with a statement by the Author(s) confirming that the paper has not been and will not be published else-where and that there is no instance of misconduct (“ghostwriting” and “guest authorship”).
27. First Author/corresponding Author shall receive 1 copy of the issue in which the article shall be published. They shall be sent to the author(s) free of charge.
28. No remuneration shall be paid for publication. 29. Copyrights. Submission of an article for publication implies a transfer of the copyright from the Author to the
publisher upon acceptance. Accepted papers shall become permanent property of the Polish Gerontology and may not be reproduced without the written consent from the publisher. The publisher reserves the copyright (including printing, electronic version such as CDs, the Internet and others).
Only abstracts can be published elsewhere without written permission from the publisher.30. The Polish Gerontology has its website featuring full versions of printed papers as well as news published by the
Editorial Team.