Advanced Google Analytics for iOS - How to not kill your SEO

ORIGINAL ARTICLE: CLINICAL
Cladribine combined with cyclophosphamide and mitoxantrone is anactive salvage therapy in advanced non-Hodgkin’s lymphoma
TADEUSZ ROBAK, EWA LECH-MARANDA, AGNIESZKA JANUS, JERZY BLONSKI,
AGNIESZKA WIERZBOWSKA, & JOANNA GORA-TYBOR
Department of Hematology, Medical University of Lodz, Poland
(Received 22 January 2007; revised 20 March 2007; accepted 21 March 2007)
AbstractThe aim of this study was to determine the feasibility, efficacy and toxicity of the combined therapy consisting of cladribine(2-CdA), mitoxantrone and cyclophosphamide (CMC regimen) in patients with refractory or relapsed non-Hodgkin’slymphoma (NHL). Thirty six patients, 14 with mantle cell lymphoma (MCL), 10 with diffuse large B-cell lymphoma(DLBCL), 5 with follicular lymphoma (FL), 3 with small lymphocytic lymphoma (SLL), and 4 with T-cell lymphoma wereenrolled to the study. The CMC protocol consisted of 2-CdA at a dose of 0.12 mg/kg in a 2-hour infusion on days 1 through3, mitoxantrone 10 mg/m2 i.v. on day 1 and cyclophosphamide 650 mg/m2 i.v. on day 1. The CMC courses were repeated atintervals of 4 weeks. Thirty three patients were available for evaluation of response. Overall response rate (OR) was 58%(95% CI, 41 – 75%). Seven patients (21%; 95% CI, 7 – 35%) achieved a complete response (CR) and 12 patients (36%;95% CI, 20 – 52%) achieved a partial response (PR). Seven of 19 patients with CR/PR are still in remission with a medianfollow-up of 3 months (range, 2 – 17 months). The median failure-free survival (FFS) was 5 months (range, 2 – 17 months).The median overall survival (OS) for the entire group was 9 months (range, 0.1 – 77 months). There was a significantdifference in OS between responders and nonresponders after CMC therapy (log rank test, P¼ 0.015). When differentdisease status before CMC treatment was considered, a trend toward longer survival of recurrent patients was observed (logrank test, P¼ 0.08). Grade 3 – 4 neutropenia developed in 14 (39%) patients, and 16 episodes (15%) of grade 3 – 4 infectionswere observed. Grade 3 – 4 thrombocytopenia or anemia was seen in 9 patients (25%) and 10 patients (28%), respectively.The results of our study show that the CMC regimen is effective salvage therapy with acceptable toxicity in heavily pretreatedpatients with NHL including MCL and DLBCL.
Keywords: Lymphoma, 2-CdA, mitoxantrone, cyclophosphamide, DLBCL, MCL
Introduction
Cladribine (2-chlorodeoxyadenosine, 2-CdA) used
as a single agent showed remarkable activity in both
previously treated and untreated patients with low
grade non-Hodgkin’s lymphoma (LG-NHL) [1,2].
In relapsed or refractory LG-NHL patients, 2-CdA
induced durable responses with overall response
(OR) rates ranging from 32% to 76% and complete
response (CR) rates between 10% and 38% [3 – 13].
Combined use of 2-CdA with cyclophosphamide and
its derivatives showed synergistic action in both in
vitro and in vivo experiments [14 – 16]. Mitoxan-
trone and anthracyclines are also useful drugs in the
treatment of LG-NHL and can be combined with
purine nucleoside analogs. These agents potentiated
the antineoplastic activity of 2-CdA in preclinical
studies [17].
Recent data indicate that 2-CdA in combination
with cyclophosphamide or mitoxantrone produce
higher response rates in indolent lymphoid malig-
nancies compared with 2-CdA monotherapy [18 –
24]. Thus, combination treatment with 2-CdA,
cyclophosphamide and mitoxantrone (CMC pro-
gramme) seems to be the logical conclusion of the
clinical studies in which 2-CdA was administered
with each independently. In our previous studies we
showed that the CMC regimen was an active
treatment in chronic lymphocytic leukaemia (CLL)
[25,26] and that it had significant activity and
Correspondence: Tadeusz Robak, Department of Hematology, Medical University of Lodz, Poland. E-mail: [email protected]
Leukemia & Lymphoma, June 2007; 48(6): 1092 – 1101
ISSN 1042-8194 print/ISSN 1029-2403 online � 2007 Informa UK Ltd.
DOI: 10.1080/10428190701361216
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f M
inne
sota
on
05/1
5/13
For
pers
onal
use
onl
y.

acceptable toxicity in heavily pre-treated patients
with other LG-NHL [27].
In this report, we present the up-dated results of
our study evaluating the feasibility, efficacy and
toxicity of the CMC regimen in patients with
refractory or relapsed NHL, including mantle cell
lymphoma (MCL) and diffuse large B-cell lym-
phoma (DLBCL).
Patients and methods
Patients
The study comprised 36 adult patients with relapsed
or refractory NHL treated in the Department of
Hematology, Medical University of Lodz, Poland,
between December 1999 and March 2006. The
study was approved by the local ethics committee.
Informed consent was obtained from all patients and
patients’ confidentiality was preserved in accordance
with the Polish regulations for studies of human
subjects. The diagnosis was based on the World
Health Organization (WHO) classification for NHL
[28]. Pre-treatment medical evaluation consisted of a
complete history and physical examination, blood
morphology and chemistry, including lactic dehy-
drogenase (LDH) level, bone marrow biopsy, com-
puted tomographic scan of the chest, abdomen and
pelvis, ECG and echocardiograms. The extent of the
disease was categorized according to the Ann Arbor
classification, and performance status was assessed
using criteria of the Eastern Cooperative Oncology
Group (ECOG). All patients entering the study were
at least 18 years old, had ECOG performance status
between 0 – 2 with a life expectancy greater than 3
months, and at least one area of measurable disease.
They had to be free of active infections and did not
receive radiation or chemotherapy within at least 3
weeks before entering this study. All patients had
previously received at least one chemotherapy regi-
men and had either failed to respond (refractory
disease) or developed progressive disease after the
discontinuation of previous treatment (recurrent
disease). The median number of previous regimens
was 2 (range 1 – 4). Exclusion criteria of the study
were prior malignancy, Richter’s syndrome, active
infections including HIV infection, any significant
organ dysfunction, i.e., elevated creatinine (42 mg/
dl), elevated total bilirubin (42 mg/dl), elevated
transaminases or alkaline phosphatase (426 normal
values), left ventricular ejection fraction (LVEF)
555% and symptoms of heart failure (New York
Heart Association Grade III or IV). Pregnant or
lactating women were also excluded. The pre-
treatment characteristics of the patients are shown
in Table I.
Treatment
The treatment consisted of 2-CdA (cladribine) given
at a dose of 0.12 mg/kg/day in a 2-h intravenous
infusion for 3 consecutive days, mitoxantrone
10 mg/m2 on Day 1 and cyclophosphamide
650 mg/m2 on Day 1 (CMC regimen). 2-CdA
(Biodribin) was commercially available from the
Institute of Biotechnology and Antibiotics, Bioton,
Warsaw, Poland. If a response was documented, then
patients were treated until maximal response was
achieved or prohibitive toxicity occurred. If no
response or disease progression was observed after
two cycles, the treatment was stopped. The cycles were
repeated usually at 28 days intervals. In patients who
developed an infection or a drug-induced cytopenia
(a platelet count 5506109 l71 and/or a neutrophil
count 51.06109 l71), CMC therapy was interrupted
until recovery of haematological parameters (at least
Grade 2 toxicity according to the WHO Criteria) or
recovery from infection was observed. The treatment
was re-administered at time intervals longer than 4
weeks, ranging from 5 to 8 weeks.
To prevent hyperuricemia, allopurinol (300 mg
daily) was given. No prophylactic antibiotics, anti-
viral agents, or haematopoietic growth factors were
Table I. Clinical characteristics of NHL patients before CMC
treatment.
Number of patients 36
Age, median (range) 59 (19 – 83)
Sex (male/female) 23/13
Histology
Mantle cell lymphoma 14
Diffuse large B-cell lymphoma 10
Follicular lymphoma 5
Small lymphocytic lymphoma 3
T-cell lymphomas* 4
Ann Arbor stage III, IV (%) 32 (89)
B-symptoms (%) 23 (64)
Extranodal involved sites 41 (%) 15 (42)
Elevated LDH (%) 27 (75)
Bone marrow involvement (%) 21 (58)
Bulky disease (410 cm) (%) 6 (17)
Elevated b2-microglobulin (%) 33 (92)
Disease status before CMC treatment
Refractory 21
Recurrent 15
Prior courses of chemotherapy
1 regimen 17
2 regimes 9
3 or more regimens 10
Prior radiotherapy 3
Median white cell count 6109 l71 (range) 9.5 (1.5 – 152.0)
Median neutrophil count 6109 l71 (range) 3.72 (0.5 – 26.2)
Median haemoglobin g/dl (range) 11.6 (7.3 – 15.3)
Median platelets count 6109 l71 (range) 161 (27 – 434)
*T-cell lymphomas included anaplastic large T-cell lymphoma,
Sezary syndrome, angioimmunoblastic lymphoma, T-cell lympho-
blastic lymphoma.
Cladribine, cyclophosphamide, and mitoxantrone in NHL 1093
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f M
inne
sota
on
05/1
5/13
For
pers
onal
use
onl
y.

given. However, patients received granulocyte-col-
ony stimulating factor (G-CSF) if the absolute
granulocyte count was 51.06 109 l71 and an active
infection was present.
Response criteria
Response criteria were defined according to NCI
sponsored International Working Group [28].
Complete response (CR) was defined as disappear-
ance of all disease manifestations by physical
examination, bone marrow biopsy, imaging studies
and normalisation of all laboratory values, lasting at
least 2 months with no development of any new
lesions. Partial response (PR) was defined as a
reduction of at least 50% in all the involved areas of
disease, lasting for at least 2 months. The duration
of response was computed from the time of onset of
CR or PR to the time of relapse, last follow-up, or
death. Patients who had not achieved CR or PR
were classified as non-responders. If CR was
achieved, no further therapy was administered; in
the case of PR, CMC treatment was continued up
to 6 cycles. Non-responders were put on another
treatment.
Toxicity monitoring
Toxicity was monitored and assessed according to
the WHO Criteria [29]. Blood counts, creatinine,
bilirubin, GOT, GPT, ECG, urinalysis and general
physical examination were serially evaluated and
recorded. Treatment induced anaemia, thrombocy-
topenia and neutropenia were diagnosed if after any
treatment course a further decrease of haemoglobin
level and/or platelets and neutrophil counts were
observed.
Only major and moderate infections that required
oral or parenteral antibiotics, antiviral or antifungal
therapy and/or hospitalisation were recorded. Fever
of unknown origin (FUO) requiring parenteral
antibiotics therapy was also recorded as an infectious
event. Infections were reported as CMC treatment
related if they developed on therapy or within 4
weeks of the completion of the CMC therapy.
Statistical analysis
Statistical analysis of the differences in the percentages
of NHL patients’ response was evaluated using the
chi-square test. Ninety-five percent confidence inter-
vals for response probability were calculated using the
method described by Duffy and Santner [30]. Failure
free survival (FFS) and overall survival (OS) curves
were calculated using the method of Kaplan and
Meier [31] and compared between groups using the
log-rank test. FFS was measured from the onset of CR
or PR achievement to the time of disease recurrence.
OS was determined from the onset of treatment until
the last follow-up evaluation or death from any cause.
The duration of response was calculated from the
onset of CR or PR achievement to the time of
recurrence, last follow-up or death.
Results
Thirty-six patients with refractory or relapsed NHL
were enrolled into the study and 33 of them were
available for evaluation of response. There were 14
patients with mantle cell lymphoma (MCL), 10 with
diffuse large B-cell lymphoma (DLBCL), 5 with
follicular lymphoma (FL), 3 with small lymphocytic
lymphoma (SLL) and 4 with T-cell lymphomas.
Their characteristics are presented in Table I. All
patients received at least one standard chemotherapy
regimen and had failed to respond or progressed after
an initial response. The median number of previous
regimens administered was 2 (range 1 – 4 regimens
per patient) and the median disease duration before
the CMC therapy was 13.5 months (range 3.6 – 163
months). Twenty-one (58%) patients had refractory
disease after prior therapy, and 15 (42%) were
recurrent. Most of the patients experienced advanced
disease before entering the study, 32 (89%) patients
had disease stage III/IV, 27 (75%) elevated serum
LDH, 33 (92%) elevated b2-microglobulin levels,
and 21 (58%) bone marrow involvement. In total,
104 courses of the CMC regimen were given to the
entire group. All 33 patients, who were available for
response assessment, received at least two CMC
courses. The median number of CMC courses was 3
(range 2 – 6 courses).
Response and survival
Response and survival analysis was based on disease
status in September 2006. Nineteen patients re-
sponded (58%; 95% CI, 41 – 75%) to the CMC
treatment. Seven patients (21%; 95% CI, 7 – 35%)
achieved a CR and 12 patients (36%; 95% CI, 20 –
52%) achieved a PR. The remaining 14 patients
(42%; 95% CI, 25 – 59%) had either stable or
progressive disease.
The response to CMC treatment according to
different histological diagnosis is presented in
Table II. Overall response (OR) was obtained in
7 patients (54%; 95% CI 27 – 81%) with MCL,
in 5 patients (62.5%; 95% CI 29 – 96%) with
DLBCL. The OR was also obtained in 2 patients
(40%) with FL, in 3 patients (100%) with SLL, and 2
patients (50%) with T-cell lymphoma. There were no
statistically significant differences in response to
1094 T. Robak et al.
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f M
inne
sota
on
05/1
5/13
For
pers
onal
use
onl
y.

CMC within different NHL histological subtypes.
When different disease status (refractory or recurrent)
before the CMC therapy was considered, no sig-
nificant differences was found in terms of OR rates.
Detailed characteristics of the patients who re-
sponded to the CMC therapy are shown in Table III.
Seven of 19 patients who achieved a CR or a PR are
still in remission at the time of this report with a
median follow-up of 3 months (range 2 – 17 months).
The median failure-free survival (FFS) of responders
was 5 months (range 2 – 17 months).
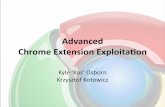
The median overall survival (OS) for the entire
group of 36 patients was 9 months (range 0.1 – 77
months), and the median OS for responders was 12.5
months (range 3 – 77 months). There was a signifi-
cant difference in overall survival between responders
and non-responders after the CMC therapy (log rank
test, P¼ 0.015) (Figure 1). When different disease
status before CMC was considered, no significant
differences were found between refractory and
recurrent patients in FFS (log rank test, P¼ 0.1);
however, in terms of OS, a trend toward longer
survival of recurrent patients was observed (log rank
test, P¼ 0.08) (Figure 2).
During the whole period of follow-up, 25 patients
died, including 17 deaths from the disease progres-
sion, three treatment related deaths (one septic shock
after the 1st cycle, and two septic shocks after the 3rd
cycle), and five deaths from other causes. Of five
deaths that were not related to the treatment, two were
caused by infectious complications and occurred
during the further chemotherapy given after comple-
tion of participation in this study, one patient died
because of stroke during the follow-up period, and
two deaths were caused by circulatory failure; one
patient had a myocardial infarction and left ventricular
failure after the 1st cycle, and the second patient had
left ventricular failure during further chemotherapy
given due to disease progression. Among 25 deaths,
three were recorded as early deaths before completing
two CMC cycles; one patient died due to septic shock
after the 1st cycle, a second suffered a myocardial
infarction and left ventricular failure after the 1st
cycle, and the third patient died because of disease
progression. These three patients were not considered
for response assessment.
Toxicity
The major toxicity was myelosuppression. Severe
neutropenia (Grade 3 – 4 according to the WHO
classification) was observed in 14 patients (39%) and
in total 32 episodes (31%) were seen during all 104
CMC courses. Sixteen episodes (15%) of Grade 3 – 4
infections were observed, including nine cases of
severe pneumonia, two herpes zoster infections, one
case of influenza-like syndrome, and three episodes
of fever of unknown origin (FUO). Four cases of
pneumonia were microbiologically documented and
were caused by Gram-positive micro-organisms,
mainly Streptococci. Pneumonia caused by Pneumo-
cystis carinii or other opportunistic micro-organisms
were not documented. The intervals between CMC
courses due to myelosuppression and/or infections
were prolonged from 2 to 8 weeks in 15 (45%)
patients. There were three treatment related deaths.
These patients died from severe pneumonia compli-
cated by septic shock and agranulocytosis; one
patient died after the first cycle, and two patients
after the third cycle. Grade 3 – 4 thrombocytopenia
or anaemia was observed in nine patients (25%) and
10 patients (28%), respectively. Vomiting of Grade 3
was observed in four patients (11%) and alopecia in
five patients (14%). Toxicity of the CMC therapy is
summarised in Table IV.
Late haematological and non-haematological toxi-
cities were also observed in the study group. Four
weeks after the completion of the CMC therapy,
Grade 3 – 4 neutropenia was observed in six patients
(18%) with the median value of 2.36 109 l71 (range
0.4 – 10.0). Grade 3 – 4 thrombocytopenia or anae-
mia was observed in six patients (18%) and two
patients (6%), respectively. The median platelets
count was 1196 109 l71 (range 11 – 3986 109 l71),
and the median haemoglobin level was 11.3 g/dl
(range 6.6 – 14.7 g/dl). Late Grade 3 – 4 infections,
Table II. Response rate and response duration of 33 NHL patients.
Type of lymphoma No. of patients OR (%) CR (%)
No. of CMC courses,
median (range)
Median response duration
in months (range)
Mantle cell lymphoma 13 7 (54) 1 (8) 3 (2 – 6) 6 (2 – 16)
Diffuse large B-cell lymphoma 8 5 (62.5) 2 (25) 2 (2 – 6) 4 (2 – 17)
Follicular lymphoma 5 2 (40) 1 (20) 3 (2 – 4) 8 (3 – 13)
Small lymphocytic lymphoma 3 3 (100) 2 (67) 4 (2 – 4) 6 (4 – 27)
T-cell lymphoma* 4 2 (50) 1 (25) 2.5 (2 – 4) 3.5 (2 – 5)
Total 33 19 (58) 7 (21) 3 (2 – 6) 4 (2 – 27)
*T-cell lymphomas included anaplastic large T-cell lymphoma, Sezary syndrome, angioimmunoblastic lymphoma, T-cell lymphoblastic
lymphoma. OR, overall response; CR, complete response.
Cladribine, cyclophosphamide, and mitoxantrone in NHL 1095
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f M
inne
sota
on
05/1
5/13
For
pers
onal
use
onl
y.

Tab
leII
I.C
har
acte
rist
ics
of
pat
ien
tsw
ho
resp
on
ded
toC
MC
ther
apy.
Pat
ien
tn
o.
Dia
gn
osi
s
An
nA
rbo
rst
age
bef
ore
CM
C
Dis
ease
stat
us
bef
ore
CM
C
Pri
or
trea
tmen
t
(No
.o
fco
urs
es)
No
.of
CM
Cco
urs
es
Tim
eb
etw
een
firs
t
and
last
CM
C(m
on
ths)
Res
po
nse
toC
MC
Du
rati
on
of
resp
on
se(m
on
ths)
1M
CL
IVre
curr
ent
CH
OP
(4)
65
PR
16
2M
CL
IVre
frac
tory
CH
OP
(5)
33
CR*
3{
3M
CL
IVre
frac
tory
CH
OP
(6)
33
PR
4
4M
CL
IVre
curr
ent
CO
P(4
)C
HO
P(3
)4
5P
R*
6{
5M
CL
III
refr
acto
ryC
HO
P(6
)2
1P
R*
2{
6M
CL
IVre
frac
tory
CO
P(6
)3
3P
R9
7M
CL
III
refr
acto
ryC
OP
(6)
34
PR
12
8D
LB
CL
IVre
curr
ent
CH
OP
(9)
22
PR*
2{
9D
LB
CL
IVre
curr
ent
CH
OP
(4)
CH
OP
-Ble
o(6
)2
1C
R*
17{
10
DL
BC
LIV
recu
rren
tC
HO
P(3
)C
HO
P-B
leo
(3)
DH
AP
(2)
21
PR*
3{
11
DL
BC
LIV
recu
rren
tC
HO
P(4
)C
HO
P-B
leo
(6)
IMV
PIG
(6)
65
CR
11
12
DL
BC
LIV
refr
acto
ryC
HO
P(4
)D
HA
P(1
)3
3P
R3
13
FL
IIre
curr
ent
CH
OP
(6)
Rit
(2)
43
PR
3{
14
FL
III
recu
rren
tC
HO
P(1
2)
Rit
ux
(4)
45
CR
13{
15
SL
LII
Ire
frac
tory
CO
P(5
)C
HO
P(4
)Id
aþ
2-C
DA
(2)
43
PR
6
16
SL
LIV
refr
acto
ryC
OP
(4)
CH
OP
(6)
2-C
DA
(2)
21
CR
4
17
SL
LII
Ire
curr
ent
CO
P(1
2)
Idaþ
2C
DA
(3)
44
CR
16
18
AIL
DII
Ire
frac
tory
CH
OP
(4)
33
PR
2
19
T-L
LII
refr
acto
ryC
HO
P(5
)2
1C
R*
5{
*P
atie
nts
aliv
e,in
CR
/PR
.{ P
atie
nts
aliv
e.
MC
L,
man
tle
cell
lym
ph
om
a;D
LB
CL
,d
iffu
sela
rge
B-c
ell
lym
ph
om
a;F
L,
follic
ula
rly
mp
ho
ma;
SL
L,
smal
lly
mp
ho
cyti
cly
mp
ho
ma;
AIL
D,
angio
imm
un
ob
last
icly
mp
ho
ma;
T-L
L,
T-c
ell
lym
ph
ob
last
icly
mp
ho
ma;
CH
OP
,cy
clo
ph
osp
ham
ide,
do
xoru
bic
in,
vin
cris
tin
e,p
red
nis
on
e;B
leo
,b
leo
myc
in;
Ida,
idar
ub
icin
;R
it,
ritu
xim
ab;
2-C
dA
,cl
adri
bin
e;D
HA
P,
dex
amet
has
on
e,
do
xo
rub
icin
,cy
tara
bin
e,p
red
nis
on
e.
1096 T. Robak et al.
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f M
inne
sota
on
05/1
5/13
For
pers
onal
use
onl
y.

which occurred beyond 4 weeks after the last CMC
cycle and before the beginning of subsequent
chemotherapy, were observed in six patients (18%).
During the follow-up period, secondary cancers or
acute myeloid leukaemia (AML) were not observed
in any of the patients.
Discussion
In this study we report on the efficacy and toxicity of
the CMC regimen in patients with relapsed or
refractory NHL. We evaluated here a heterogeneous
group of 36 patients, most of whom were diagnosed
with MCL (14/36) and DLBCL (10/36). The results
suggest a good level of anti-tumour activity and an
acceptable tolerance of the CMC regimen. Among
33 evaluated patients, an overall response rate was
58%, including 21% of patients who achieved a CR.
The results are comparable to those previously
reported by us, with an overall response rate of
48.6% and a CR rate of 12.1% in the group of heavily
pre-treated patients with indolent lymphoid malig-
nancies (19 patients with CLL and 14 with LG-
NHL) [27].
Cladribine has been reported to be active as the
first-line therapy or in the first relapse among
patients with MCL achieving a response rate of
58% [9,10]. It is noteworthy that patients refractory
to 2-CDA did not respond to other salvage
therapies like CHOP or Dexa-BEAM. Rummel
et al. [23] reported later on increased efficacy of
the combination treatment with reduced-dose of
2-CdA and mitoxantrone in previously untreated
or relapsed patients with MCL. They achieved a
response rate of 100% with a CR rate of 44%.
2-CdA is a potent inhibitor of DNA repair and
mitoxantrone acts as a DNA-damaging agent. Thus,
simultaneous use of these drugs enhances their anti-
tumour activity [22]. High response rates to the
combined chemotherapy observed by Rummel et al.
in MCL patients confirm its superiority to mono-
therapy. Another purine analog, fludarabine, has
been also shown to be effective in the treatment of
low-grade lymphomas, and in particular of MCL
[32,33]. Similar to 2-CdA, fludarabine seems to be
more active if it is combined with cyclophospha-
mide or cyclophosphamide and mitoxantrone
[32,33]. The German Low-Grade Lymphoma
Study Group obtained an overall response rate of
46% in relapsed or refractory MCL patients who
received combination therapy with fludarabine,
cyclophosphamide and mitoxantrone [34]. Recent
studies have indicated that the addition of mono-
clonal antibody, rituximab, may increase the clinical
effectiveness of standard chemotherapy [34 – 37].
Forstpointner et al. [34] achieved a higher overall
Figure 1. Kaplan – Meier overall survival (OS) curve for responders and non-responders to CMC treatment.
Cladribine, cyclophosphamide, and mitoxantrone in NHL 1097
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f M
inne
sota
on
05/1
5/13
For
pers
onal
use
onl
y.

response rate (79% vs. 58%), a higher complete
remission rate (33% vs. 13%), and a superior
overall survival at 2 years (90% vs. 70%) in
relapsed/refractory LG-NHL patients treated with
rituximab combined with chemotherapy (R-FMC)
compared with that of those who received che-
motherapy alone (FCM). It may be therefore
speculated that the addition of rituximab to the
Figure 2. Kaplan – Meier failure-free survival (FFS) (A) and overall survival (OS) (B) curves for NHL patients refractory or recurrent to prior
CMC treatment.
1098 T. Robak et al.
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f M
inne
sota
on
05/1
5/13
For
pers
onal
use
onl
y.

CMC therapy could also improve the prognosis of
heavily pre-treated NHL patients. The addition of
rituximab may render tumour cells susceptible to
apoptosis and enhance the effect of subsequent
chemotherapy.
One of the most interesting observations in our
study is the results obtained for DLBCL patients.
Five patients (62.5%) responded to the CMC
treatment, and two of them achieved a CR despite
refractoriness to previous treatment regimens. In our
study, one patient with a CR after the CMC
treatment received subsequently high dose therapy
followed by autologous stem cell transplantation
(autoSCT) and remained in remission for 15 months.
Although purine analogs in monotherapy were
reported to be ineffective against high grade lympho-
mas [38], promising results have been obtained for
combination chemotherapy. Fludarabine combined
with dexamethasone, cytosine arabinoside and cis-
platinum (FluDAP) showed high activity in relapsed/
refractory aggressive NHL patients [39], while the
combination of fludarabine with cyclophosphamide
was effective in the treatment of refractory peripheral
T-cell lymphoma concurrent with DLBCL [40]. Our
results suggest that CMC therapy could be used in
the treatment of refractory or relapsed patients with
high grade lymphomas. Moreover, patients who
respond to CMC treatment could then be considered
for autologous haematopoietic stem cell transplanta-
tion [41 – 43].
An additional aim of our study was the evaluation
of the treatment-related toxicity of the CMC therapy.
We have shown that the major toxicity of this
regimen was myelosuppression. It was manifested
with 39% of Grade 3 – 4 neutropenia, complicated
with 16 episodes (15%) of Grade 3 – 4 infections.
Grade 3 – 4 thrombocytopenia was observed in 25%
and anaemia in 28% of patients. However, it has
been reported that cladribine alone induces Grade
3 – 4 neutropenia in 17%, and Grade 3 – 4 thrombo-
cytopenia in 2% of patients [9,10]. The main reason
for myelotoxicity was the use of the CMC regimen in
heavily pre-treated patients. Additionally, the dose of
mitoxantrone (10 mg/m2) we used was high and
higher than the dose (8 mg/m2) used by Forstpoint-
ner et al. [34,37]. They also observed neutropenia in
40% of the pre-treated patients; however, the
incidence of Grade 3 – 4 neutropenia and thrombo-
cytopenia was significantly lower [34,37]. Late
toxicity was also mainly manifested by Grade 3 – 4
neutropenia and infections observed in 18% of
patients. Further reduction of myelosuppression
and infections may be most likely achieved with the
prophylactic use of growth factors following che-
motherapy cycle as well as antibacterial and antiviral
agents. Additionally, myelosuppression could be
diminished by reducing the dose of mitoxantrone to
8 mg/m2.
Based on these results, it can be concluded that the
combination of 2-CdA, mitoxantrone and cyclophos-
phamide is a highly effective salvage therapy for
relapsed or refractory NHL patients, in particular, for
those with MCL and DLBCL. However, the toxicity
of the CMC treatment is significant, although it is
restricted mainly to myelosuppression and infections.
The CMC regimen can be considered a valuable
treatment choice for heavily pre-treated NHL pa-
tients; however, a prospective, randomized study
comparing the efficacy of the CMC regimen with
cladribine alone should be undertaken.
References
1. Robak T, Korycka A, Kasznicki M, Wrzesien-Kus A,
Smolewski P. Purine nucleoside analogues for the treatment
of hematological malignancies: pharmacology and clinical
applications. Curr Cancer Drug Targets 2005;5:424 – 444.
2. Tallman MS, Hakimian D. Purine nucleoside analogs:
emerging roles in indolent lymphoproliferative disorders.
Blood 1995;86:2463 – 2474.
3. Kay AC, Saven A, Carrera CJ, Carson DA, Thurston D,
Beutler E, et al. 2-chlorodeoxyadenosine treatment of low-
grade non-Hodgkin’s lymphomas. J Clin Oncol 1992;10:371 –
377.
4. Betticher DC, von Rohr A, Ratschiller D, Schmitz SF,
Egger T, Sonderegger T, et al. Fewer infections but
maintained antitumor activity with lower-dose versus standard
dose caldribine in pretreated low grade non-Hodgkin’s
lymphoma. J Clin Oncol 1998;16:850 – 859.
5. Liliemark J, Porwit A, Juliusson G. Intermittent infusion
cladribine (CdA) in previously treated patients with low-grade
non-Hodkin’s lymphoma. Leuk Lymphoma 1997;25:313 –
318.
Table IV. Severe toxicity of CMC treatment.
Toxicity (Grade 3 – 4 according to WHO) Number of patients, N¼36 (%) Number of cycles, N¼104 (%)
Neutropenia 14 (39) 32 (31)
Thrombocytopenia 9 (25) 15 (14)
Anaemia 10 (28) 17 (16)
Infections and FUO* 10 (25) 16 (15)
Vomiting 4 (11) 5 (5)
Alopecia 5 (14) 6 (6)
*FUO, fever of unknown origin.
Cladribine, cyclophosphamide, and mitoxantrone in NHL 1099
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f M
inne
sota
on
05/1
5/13
For
pers
onal
use
onl
y.

6. Robak T, Gora-Tybor J, Krykowski E, Walewski JA,
Borawska A, Płu_zanska A, et al. Activity of 2-chlorodeox-
yadenosine (Cladribine) in 2-hour intravenous infusion in 94
previously treated patients with low-grade non-Hodgkin’s
lymphoma. Leuk Lymphoma 1997;26:99 – 105.
7. Tulpule A, Schiller G, Harvey-Buchanan LA, Lee M,
Espina BM, Khan AU, et al. Cladribine in the treatment of
advanced relapsed or refractory low and intermediate grade
non-Hodgkin’s lymphoma. Cancer 1998;83:370 – 376.
8. Ogura M, Morishima Y, Kobayashi Y, Uike N, Sugai S,
Chou T, et al. Durable response but prolonged cytopenia after
cladribine treatment in relapsed patients with indolent non-
Hodgkin’s lymphomas: results of Japanese phase II study. Int J
Haematol 2004;80:267 – 277.
9. Rummel MJ, Chow KU, Jager E, Leimer L, Hossteld DK,
Bergmann L, et al. Intermittent 2-hour infusion of cladribine
as first-line therapy or in first relapse of progressive advanced
low-grade and mantle cell lymphomas. Leuk Lymphoma
1999;82:957 – 964.
10. Rummel MJ, Chow KU, Jager E, Hossfeld DK, Bergmann L,
Peters HD, et al. Treatment of mantle-cell lymphomas with
intermittent two-hour infusion of cladribine as first-line
therapy or in first relapse. Ann Oncol 1999;10:115 – 117.
11. Kong LR, Huang CF, Hakimian D, Variakojis D, Klein L,
Kuzel TM, et al. Long term follow-up and late complications of
2-chlorodeoxyadenosine in previously treated, advanced in-
dolent non-Hodgkin’s lymphoma. Cancer 1998;82:957 – 964.
12. Saven A, Emanuele S, Kosty M, Kozioł J, Ellison D, Piro L.
2-chlorodeoxyadenosine activity in patients with utreated in-
dolent non-Hodgkin’s lymphoma. Blood 1995;86:1710 – 1716.
13. Fridrik M, Jager G, Kienzer HR, Hausmaninger H, Oppitz P,
Krieger O, et al. Efficacy and toxicity of 2-chlorodeoxyade-
nosine (Cladribine)– 2 h infusion for 5 days – as first-line
treatment for advanced low-grade non-Hodgkin’s lymphoma.
Eur J Cancer 1998;34:1560 – 1564.
14. Van Den Neste E, Bontemps F, Delacauw A, Cardoen S,
Louviaux I, Scheiff JM, et al. Potentiation of antitumor effects
of cyclophosphamide derivatives in B-chronic lymphocytic
leukemia cells by 2-chloro-20-deoxyadenosine. Leukemia
1999;13:918 – 925.
15. Gora-Tybor J, Robak T. Synergistic action of 2-chlorodeox-
yadenosine and cyclophosphamide on murine leukemia L1210
and P388. Acta Haematol Pol 1993;24:177 – 182.
16. Hoffman M, Xu JC, Lesser M, Rai K. Cytotoxicity of 2-
chlorodeoxyadeosine (cladribine – 2-CdA) in combination
with other chemotherapy drugs against two lymphoma cell
lines. Leuk Lymphoma 1999;33:141 – 145.
17. Szmigielska-Kapłon A, Ciesielska E, Smigiero L, Robak T.
Anthracyclines potentiate activity against murine leukemias
L1210 and P388 in vivo and in vitro. Eur J Haematol
2002;68:370 – 375.
18. Laurencet FM, Ballabeni P, Rufener B, Hess U, Cerny T,
Fey M, et al. The multicenter trial SAKK 37/95 of cladribine,
cyclophosphamide and prednisone in the treatment of
chronic lymphocytic leukemias and low-grade non-Hodgkin’s
lymphomas. Acta Haematol 2007;117:40 – 47.
19. Van den Neste E, Louviaux I, Michaux JL, Delnnoy A,
Michaux L, Sonet A, et al. Phase I/II study of 2-chloro-2-
deoxyadenosine with cyclophosphamide in patients with
pretreated B-cell chronic lymphocytic leukemia and indolent
non-Hodgkin’s lymphoma. Leukemia 2000;14:1136 – 1142.
20. Kalinka E, Wajs JJ, Sułek KS, Blasinska-Morawiec M,
Centkowski P, Ceglarek B, et al. Randomized comparison of
cladribine single (C) or in combination with cyclophospha-
mide (CC) and COP in previously untreated low-grade B-cell
non-Hodgkin lymphoma patients. Blood 2006;108 (Suppl
1):703a (abstract 2481).
21. Robak T, Gora-Tybor J, Urbanska-Rys H, Krykowski E.
Combination regimen of 2-chlorodeoxyadenosine (cladri-
bine), mitoxantrone and dexamethasone (CMD) in the
treatment of refractory and recurrent low-grade non Hodg-
kin’s lymphoma. Leuk Lymphoma 1999;32:359 – 368.
22. Armitage JO, Tobinai K, Hoelzer D, Rummel MJ. Treatment
of indolent non-Hodgkin’s lymphoma with cladribine as
single-agent therapy and in combination with mitoxantrone.
Int J Hematol 2004;79:311 – 321.
23. Rummel MJ, Chow KU, Karakas T, Jager E, Mezger J, von
Grunhagen U, et al. Reduced dose cladribine (2-CdA) plus
mitoxantrone is effective in the treatment of mantle cell and
low-grade non-Hodgkin’s lymphoma. Eur J Cancer
2002;38:1739 – 1746.
24. Robak T, Gora-Tybor J, Chojnowski K. Cladribine as
monotherapy or combined with dexamethasone and idarubi-
cin or mitoxantrone in previously treated patients with low
grade lymphoid malignancies. Haematologica 2000;85:215 –
216.
25. Robak T, Błonski JZ, Kasznicki M, Gora-Tybor J, Dwilewicz-
Trojaczek J, Boguradzki P, et al. Cladribine combined with
cyclophosphamide and mitoxantrone as front-line therapy
in chronic lymphocytic leukemia. Leukemia 2001;15:1510 –
1516.
26. Robak T, Błonski JZ, Gora-Tybor J, Jamroziak K, Dwilewicz-
Trojaczek J, Tomaszewska A, et al. Cladribine alone and in
combination with cyclophosphamide or cyclophosphamide
plus mitoxantrone in the treatment of progressive chronic
lymphocytic leukemia: report of a prospective, multicenter
randomized trial of the Polish Adults Leukemia Group (PALG
CLL 2). Blood 2006;108:473 – 479.
27. Robak T, Gora-Tybor J, Lech-Maranda E, Błonski JZ,
Kasznicki M. Cladribine in combination with mitoxantrone
and cyclophsophamide (CMC) in the treatment of heavily
pretreated patients with advanced indolent lymphoid malig-
nancies. Eur J Haematol 2000;66:188 – 194.
28. Cheson BD, Horning SJ, Coiffier B, Shipp MS, Fisher RI,
Connors JM, et al. Report of an international workshop to
standardize response criteria for non-Hodgkin’s lymphomas. J
Clin Oncol 1999;17:1244 – 1253.
29. Miller AB, Hoogstraten B, Staquet M, Winkler A. Reporting
results of cancer treatment. Cancer 1981;47:207 – 214.
30. Duffy DR, Santner TJ. Confidence intervals binomial para-
meter based on multistage tests. Biometrics 1987;47:207 –
214.
31. Kaplan EL, Meier P. Nonparametric estimation from in-
complete observations. J Am Stat Assoc 1958;53:457 –
481.
32. Cohen BJ, Moskowitz C, Straus D, Noy A, Mednick E,
Zelenetz A. Cyclophosphamide fludarabine (CCF) is active in
the treatment of mantle cell lymphoma. Leuk Lymphoma
2001;42:1015 – 1022.
33. Thomas DW, Owen RG, Johnson SAN, Hillmen P,
Seymour JF, Wolf MM, Rule SAJ. Superior quality and
duration of response among patients with mantle cell
lymphoma treated with fludarabine and cyclophosphamide
with or without rituximab compared with prior responses to
CHOP. Leuk Lymphoma 2005;46:549 – 552.
34. Forspointer R, Dreyling M, Repp R, Hermann S, Hanel A,
Metzner B, et al. The addition of rituximab to a combination
of fludarabine, cyclophosphamide, mitoxantrone (FCM)
significantly increases the response rate and prolongs
survival as compared with FCM alone in patients with
relapsed and refractory follicular and mantle cell lymphomas:
results of a prospective randomized study of the German
Low-Grade Lymphoma Study Group. Blood 2004;104:
3064 – 3071.
1100 T. Robak et al.
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f M
inne
sota
on
05/1
5/13
For
pers
onal
use
onl
y.

35. Robak T, Smolewski P, Cebula B, Blonski JZ. Rituximab
combined with cladribine or with cladribine and cyclopho-
sphamide in heavily pretreated patients with indolent lympho-
proliferative disorders and mantle cell lymphoma. Cancer
2006;107:1542 – 1550.
36. Robak T. Rituximab plus purine nucleoside analogs in the
treatment of indolent lymphoid malignancies. Am J Cancer
2005;4:279 – 292.
37. Forspointner R, Unterhalt M, Dreyling M, Bock HP, Repp R,
Wandt H, et al. Maintenance therapy with rituximab leads to a
significant prolongation of response duration after salvage
therapy with a combination of rituximab, fludarabine,
cyclophosphmide and mitoxantrone (R-FCM) in patients
with recurring and refractory follicular and mantle cell
lymphomas: results of a prospective randomized study of the
German Low Grade Lymphoma Study Group (GLSG). Blood
2006;108:4003 – 4008.
38. Redman JR, Cabanillas F, Velasquez WS, Mc Laughlin P,
Hagemeister FB, Swan F Jr, et al. Phase II trial of fludarabine
phosphate in lymphoma an effective new agent in low-grade
lymphoma. J Clin Oncol 1992;10:790 – 794.
39. Child JA, Johnson SA, Rule S, Smith GM, Morgan GJ,
Johnson PW, et al. FLUDAP: salvage chemotherapy for
relapsed/refractory aggressive non-Hodgkin’s lymphoma.
Leuk Lymphoma 2000;37:309 – 317.
40. Yamaguchi M, Kotani T, Nkamura Y, Ueda M. Successful
treatment of refractory peripheral T-cell lymphoma with a
combination of fludarabine and cyclophosphamide. Int J
Hematol 2006;83:450 – 453.
41. Villanueva ML, Vose JM. The role of hematopoietic stem cell
transplantation in non-Hodgkin lymphoma. Clin Adv Hema-
tol Oncol 2006;4:521 – 530.
42. Van Besien K. The evolving role of autologous and allogeneic
stem cell transplantation in follicular lymphoma. Blood Rev
2006;20:235 – 244.
43. Laudi N, Arora M, Burns L, McGlave P, Miller J, Bohac G,
et al. Efficacy of high-dose therapy and hematopoietic stem
cell transplantation for mantle cell lymphoma. Am J Hematol
2006;81:519 – 524.
Cladribine, cyclophosphamide, and mitoxantrone in NHL 1101
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f M
inne
sota
on
05/1
5/13
For
pers
onal
use
onl
y.